
Abstract
OBJECTIVE:
To review the pharmacology, safety, and efficacy of the prokinetic agents metoclopramide and erythromycin in children.
DATA SOURCES:
English-language literature was accessed using MEDLINE (1970–June 2004) with metoclopramide, erythromycin, macrolides, gastroesophageal reflux, and gastrointestinal motility as the search terms.
STUDY SELECTION AND DATA EXTRACTION:
Abstracts and original research articles were included. Preference was given to published controlled trials. Articles providing descriptions of pharmacology, safety, and effectiveness of metoclopramide and erythromycin for the treatment of gastroesophageal reflux (GER) were also used in this review.
DATA SYNTHESIS:
Some authors advocate using a prokinetic agent along with acid suppression for treatment of GER in children. The 2 prokinetic agents most commonly used are erythromycin and metoclopramide. Erythromycin has numerous observational reports and controlled trials demonstrating its efficacy in improving feeding tolerance in children. Adverse drug reactions associated with its use were uncommon in prospective controlled trials. Few data support the use of metoclopramide for management of GER, and the potential adverse effects associated with its use need to be considered before prescribing.
CONCLUSIONS:
The literature supports the use of erythromycin as a prokinetic agent. Many children with GER are adequately controlled with acid suppression alone; however, if use of a prokinetic agent is warranted, erythromycin in combination with acid suppression should be considered. Given the lack of prospective controlled studies demonstrating metoclopramide's efficacy and safety in the treatment of GER in children, metoclopramide should not be considered a treatment option.
Gastroesophageal reflux (GER) has been estimated to occur in 18% of children, and may occur more frequently in patients with comorbidities. 1 It is often an uncomplicated and self-limited condition that spontaneously resolves by 12–15 months of age. However, GER has also been associated with chronic respiratory problems, failure to thrive, and sudden infant death syndrome. 2 While many nonpharmacologic and pharmacologic options exist for the treatment of GER, historically, a gastric acid suppressant has been the treatment of choice. The use of acid suppression for GER in children has been well studied and is beyond the scope of this review. Furthermore, some authors advocate using a prokinetic agent along with the acid suppression for the treatment of GER in children. Two of the most common prokinetic agents used in children are metoclopramide and erythromycin. The purpose of this article is to review the use of these 2 agents in the treatment of GER in the pediatric population.
Data Sources
A systematic search of the MEDLINE database (1970–June 2004) was performed to identify studies pertaining to the use of prokinetic agents in children. The following MeSH search terms were used: metoclopramide, erythromycin, macrolides, gastroesophageal reflux, and gastrointestinal motility. The search was limited to studies published in English and to those involving human subjects. It was then further limited to studies focusing on patients aged birth to 18 years of age. Both abstracts and original research articles were included; however, preference was given to published, controlled clinical trials. Literature providing descriptions of pharmacology, safety, and effectiveness of metoclopramide and erythromycin for the treatment of GER was also used in this review. Dr. Chicella evaluated all articles for inclusion. Additionally, the bibliographies of relevant articles were reviewed to identify additional references.
The 12 articles summarized in Table 1 make up the core group of articles evaluated regarding the use of metoclopramide in the treatment of GER in children.3–14 The 9 articles in Table 2 make up the core group used for the evaluation of erythromycin.15–23
Summary of Metoclopramide Studies in Children
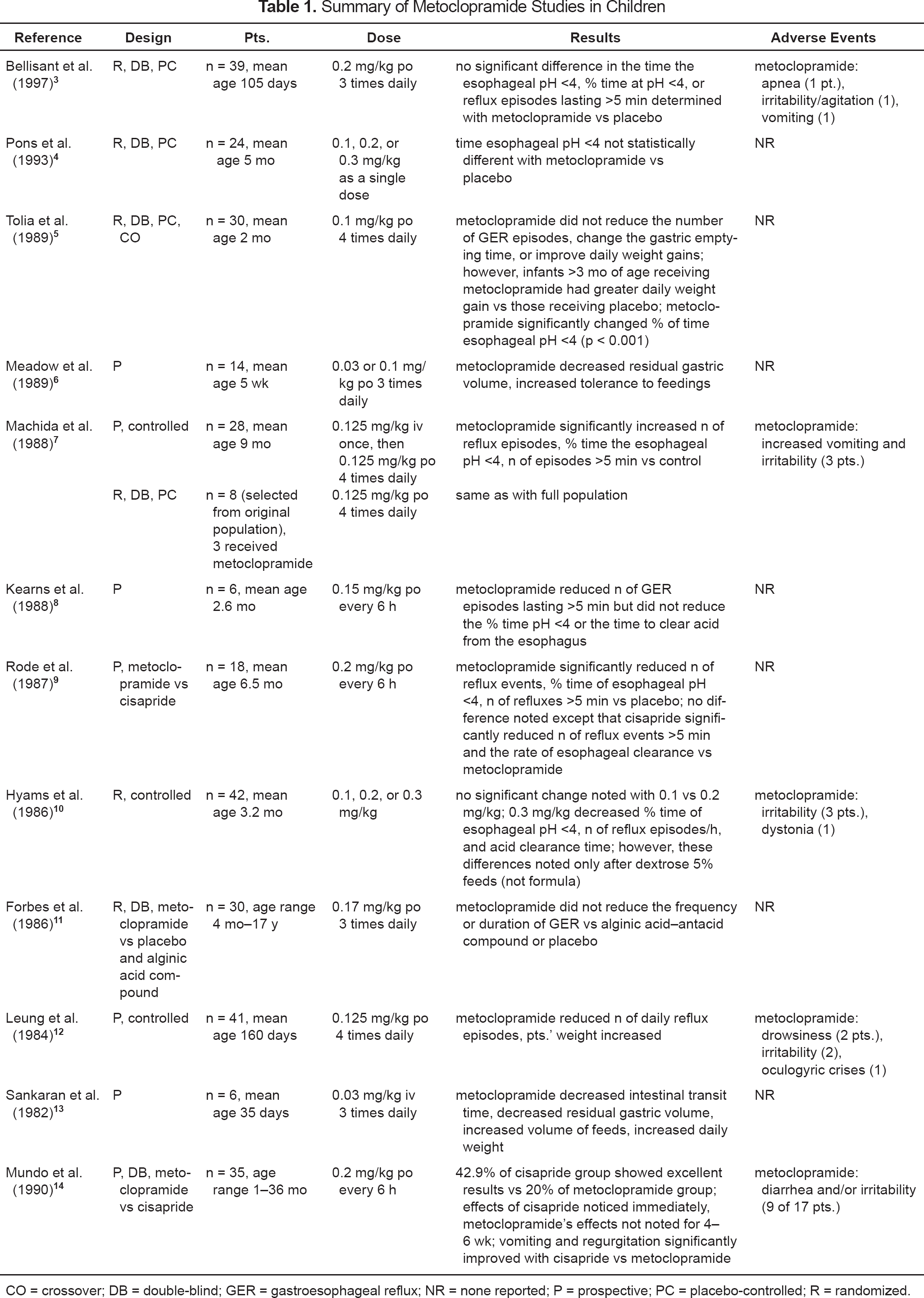
CO = crossover; DB = double-blind; GER = gastroesophageal reflux; NR = none reported; P = prospective; PC = placebo-controlled; R = randomized.
Summary of Erythromycin Studies in Preterm Infants
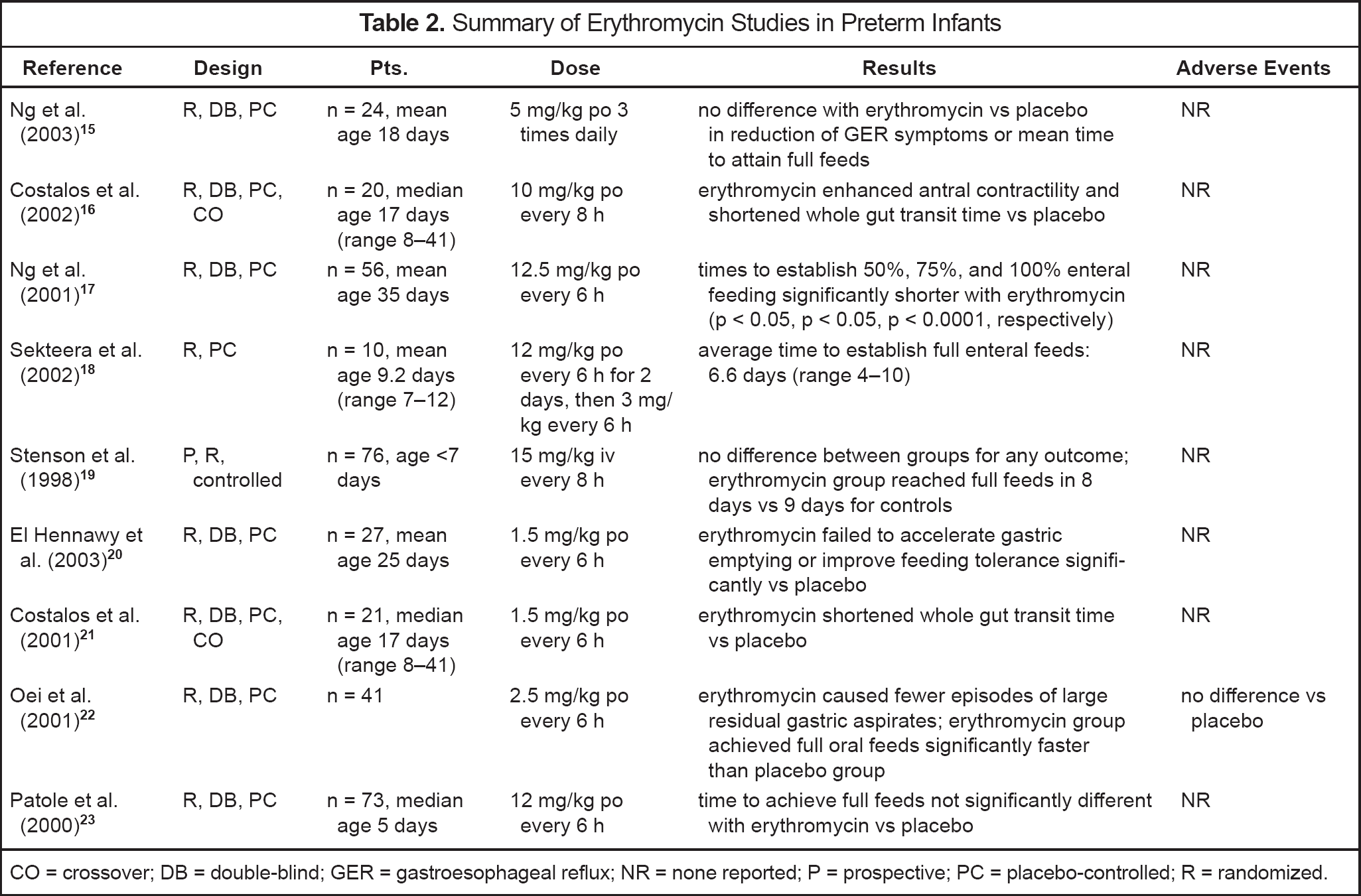
CO = crossover; DB = double-blind; GER = gastroesophageal reflux; NR = none reported; P = prospective; PC = placebo-controlled; R = randomized.
Gastroesophageal Reflux and Feeding Intolerance
GER is defined as the effortless retrograde movement of gastric contents into the esophagus and, at times, into the mouth. 24 GER has several proposed mechanisms including inappropriate relaxation of the lower esophageal sphincter, reduced lower esophageal sphincter pressure, anatomic abnormalities, delayed gastric emptying, and immature esophageal peristalsis. 25 However, delayed gastric emptying and decreased lower esophageal sphincter pressure are commonly cited in the pathophysiology of GER in pediatrics, especially in infants <4 months of age.26–29
Metoclopramide as a Prokinetic Agent in Pediatrics
Metoclopramide is a dopamine antagonist that enhances the response of the upper gastrointestinal (GI) tract to acetylcholine. It thereby increases motility and accelerates gastric emptying. Metoclopramide has also been shown to increase lower esophageal sphincter tone.28,29 Therefore, metoclopramide functions in a dual role and, in theory, it would appear to be the ideal medication for the treatment of GER. Table 1 summarizes the pediatric studies that have evaluated metoclopramide's role in the treatment of GER.3–14 Unfortunately, many of these studies have demonstrated that metoclopramide is no more effective at improving GER symptoms than placebo. Nine of the studies were either placebo-controlled or a head-to-head comparison with another prokinetic agent. Of these 9, 7 (78%) demonstrated no significant improvement of GER symptoms while the child was on metoclopramide. The dose of oral metoclopramide in these studies ranged from 0.03 mg/kg every 8 hours to 0.25 mg/kg every 6 hours. In clinical practice, a starting dose of 0.1 mg/kg every 6–8 hours is commonly prescribed. Dose—response studies have not demonstrated that increasing the dose improves the patient's response4,10; furthermore, doing so may put the patient at greater risk of experiencing an adverse drug reaction.
Safety is also a concern with metoclopramide. Metoclopramide has a number of adverse effects associated with its use in children including diarrhea, drowsiness, restlessness, gynecomastia, and galactorrhea. 30 More significantly, patients taking metoclopramide can experience extrapyramidal reactions, including dystonia and tardive dysknesia. 31 While the manufacturer of metoclopramide reports the incidence of extrapyramidal reactions as 1 in 500 patients, the incidence of these reactions appears to be substantially higher in children. 31 Furthermore, while a higher dose is more likely to result in the patient experiencing an adverse effect, many of the cases reported occur in children receiving metoclopramide at commonly prescribed doses.31–36 A misconception is that these types of reactions are easily treated with diphenhydramine and will resolve once metoclopramide is discontinued. Putnam et al. 31 reported a case of prolonged tardive dyskinesia in an 8-year-old boy who was receiving metoclopramide for GER. In this case, the patient received a single 0.4-mg/kg dose of metoclopramide and experienced torticollis, oculogyric spasms, and facial grimacing. The metoclopramide dose was decreased to 0.1 mg/kg 4 times a day for the next 3 months; however, the patient continued to have movement disorders and mental status changes. Finally, metoclopramide was discontinued, but the child continued to have uncontrollable facial spasms for 15 months after the drug was stopped.
Erythromycin as a Prokinetic Agent
Erythromycin is a macrolide antibiotic that has been shown to increase GI motility by acting as a motilin agonist. 37 Motilin is a hormone secreted in the GI tract during fasting and plays a role in smooth muscle contractions.
Numerous observational studies have reported that erythromycin is safe and effective in improving feeding tolerance for pediatric patients.38–41 The controlled trials that have evaluated erythromycin in the treatment of feeding intolerance in neonates and infants are summarized in Table 2.15–23 Nine studies have been performed to date, and 8 (89%) of these demonstrated improvement in feeding with erythromycin compared with placebo. Four of the 8 showed that erythromycin shortened whole-gut transit time, and 5 showed that infants who received erythromycin achieved goal feeds sooner than infants who did not. Both the intravenous and oral forms of erythromycin have demonstrated improvement in GI motility and feeding tolerance. The dose of oral erythromycin in these studies ranged from 1.5 mg/kg every 6 hours to 12.5 mg/kg every 6 hours. While erythromycin's effects are dose dependent, lower doses, initially 1–3 mg/kg, may increase GI motility without increasing undesired effects. 37
Adverse effects associated with erythromycin are uncommon, especially in children, but they can be severe. These include GI upset, hepatotoxicity, ototoxicity, and anaphylaxis. None of the studies listed in Table 2 demonstrated an increase in adverse reactions associated with erythromycin. Two concerning adverse effects associated with the use of erythromycin that warrant further discussion are infantile hypertrophic pyloric stenosis and arrhythmias.
Hypertrophy of the pylorus causes obstruction of gastric outlet, resulting in repetitive vomiting, metabolic alkalosis, and failure to thrive. While the exact mechanism of action is unclear, a link between the use of erythromycin in infants and the development of pyloric stenosis has been suggested. A case series of 5 infants who received systemic erythromycin and subsequently developed infantile hypertrophic pyloric stenosis was first reported in 1976. 42 Since that time, others have reported similar observations. Honein et al. 43 compared the incidence of infantile hypertrophic pyloric stenosis among infants who received erythromycin for pertussis prophylaxis with the incidence in infants who did not. They found that pyloric stenosis occurred in 4.5% of the erythromycin-treated infants and in no untreated infants. Mahon et al. 44 retrospectively reviewed the association between erythromycin exposure and infantile pyloric stenosis in infants who had either received erythromycin or who had been exposed to erythromycin in utero. Of 14 876 infants, 45 (0.3%) developed pyloric stenosis. Infants who received systemic erythromycin during the first 2 weeks of life appeared to be at greatest risk for developing pyloric stenosis. Additionally, maternal macrolide use within 10 weeks of delivery was also identified as a possible risk factor. These authors concluded that erythromycin should be used with caution during the first 2 weeks of life.
Cardiovascular toxicity associated with the use of erythromycin has also been described.45,46 Two cases of acute cardiac and pulmonary deterioration occurred in infants receiving intravenous erythromycin lactobionate. 45 Both were preterm infants, one born at 26 weeks of gestation and the other at 25 weeks. Both patients were empirically receiving erythromycin for possible Ureaplasma infection. Within minutes of receiving the first dose, both infants developed bradycardia and hypotension unresponsive to cardiopulmonary resuscitation. Two similar cases were associated with erythromycin lactobionate. 46 Both patients were preterm infants, 29 and 34 weeks' gestational age. Both were empirically receiving intravenous erythromycin for possible infection. After 4 days of therapy, the first infant developed QT interval prolongation and, subsequently, atrioventricular block that was unresponsive to resuscitation efforts. The second infant developed fatal ventricular tachycardia on day 8 of erythromycin therapy. Both authors urged caution when using intravenous erythromycin lactobionate in preterm infants. However, as of December 2004, there have been no reports of arrhythmias when enteral erythromycin has been given at a prokinetic dose. 47
There are limitations to the reports that need to be addressed before erythromycin can be recommended for the treatment of GER. First, most of the studies evaluating its use in children with GER have been performed primarily in preterm and full-term infants. There is evidence showing that erythromycin can be an effective prokinetic agent in older children with motility disorders48–50; however, there are no data in prospective, controlled clinical trials establishing efficacy in older pediatric patients with GER. Another limitation to these studies is the lack of standardized endpoints to determine efficacy. Some of the studies used clinically significant endpoints, like the time to establish full feeds and the number of reflux episodes experienced, to determine efficacy. Other studies used less clinically significant endpoints to determine efficacy, such as increased antral motility index, induction of migrating motor complexes, or induction of antro-duodenal contractions. Using these types of endpoints makes it more difficult to extrapolate these effects to GER symptom improvement and/or better patient outcomes.
The potential for increased bacterial resistance to the macrolides also needs to be considered. While, as of December 2004, no studies establishing a relationship between the use of erythromycin in GER and a change in antimicrobial resistance patterns have been published, it is prudent that this relationship be considered before any antibiotic is used for a noninfectious indication. On the other hand, other macrolides, for example azithromycin, have been used in diseases such as cystic fibrosis for noninfectious indications without an increase in bacterial resistance being described.
Conclusions
Based on this review, the literature supports the use of erythromycin as a prokinetic agent. Many children with GER are adequately controlled with acid suppression alone; however, if use of a prokinetic agent is warranted, erythromycin in combination with acid suppression should be considered. Erythromycin has numerous observational reports and controlled trials demonstrating its efficacy in children, especially preterm and full-term infants. Additionally, while some clinicians have expressed concerns over using erythromycin in infants <2 weeks of age or using the intravenous preparation in preterm infants, prospective controlled trials have demonstrated that erythromycin, in lower doses, is a safe option. Limited data are available to support the use of metoclopramide for GER. Additionally, the potential adverse effects associated with its use need to be strongly considered before prescribing metoclopramide.