
Abstract
OBJECTIVE:
To report a case of hypotension and bradyarrhythmia caused by verapamil toxicity in a patient prescribed telithromycin.
CASE SUMMARY:
A 76-year-old white woman receiving verapamil 180 mg/day for hypertension experienced a sudden onset of shortness of breath and weakness and was found to be profoundly hypotensive and bradycardic, with a systolic blood pressure of 50–60 mm Hg and a heart rate of 30 beats/min. She had been taking telithromycin 800 mg/day for 2 days previously for acute sinusitis. The patient was treated with crystalloids, vasopressors, and transvenous pacing. Approximately 72 hours after admission, her blood pressure and heart rate rapidly returned to normal, and she was discharged several days later.
DISCUSSION:
Telithromycin is a known substrate of the CYP3A4 system, and several pharmacokinetic interactions can occur by displacement of other drugs from this system. Verapamil is metabolized through several cytochrome P450 isoenzyme systems. Although there are no previous reports of an interaction between these drugs, other possible causes for the patient's symptoms were excluded and the diagnosis of a probable interaction between verapamil and telithromycin leading to verapamil toxicity was made.
CONCLUSIONS:
Telithromycin is a ketolide antibiotic approved for treatment of respiratory tract infections and acute sinusitis. The potential for clinically significant drug interactions should be considered before using this agent, especially in patients taking other drugs that are metabolized through the CYP3A system. Caution should be exercised when considering the use of this antibiotic in patients receiving verapamil.
Telithromycin was the first of the ketolide class of antibiotics to gain approval in the US. 1 A derivative of macrolide antibiotics, telithromycin has clinical activity against bacterial pathogens associated with community-acquired respiratory infections including Streptococcus pneumoniae, Hemophilus influenza, Mycobacterium catarrhalis, and atypical organisms such as Legionella pneumophila.1–3 Telithromycin exerts its antibacterial effects by blocking protein synthesis at domains II and V of 23S rRNA of the 50S ribosomal subunit. As with its macrolide counterparts, telithromycin is hepatically metabolized by the cytochrome P450 mixed oxidase system, primarily through the 3A4 (about 50% of its total metabolism) and 1A isoenzyme pathways.3,4 In vitro studies have not demonstrated a propensity for induction or inhibition of these enzyme systems.1,5 However, clinically significant drug interactions may occur by potential displacement of one drug at enzyme binding sites by another drug. We report a case of verapamil toxicity caused by a probable interaction between verapamil and telithromycin.
Case Report
A 76-year-old white female was brought to the emergency department (ED) of a large community teaching hospital after experiencing a sudden onset of shortness of breath and weakness while at home. Upon arrival in the ED, the patient was found to be profoundly hypotensive and bradycardic, with systolic BP 50–60 mm Hg and HR 30 beats/min. Her past medical history was significant for breast cancer, hypertension, chronic obstructive pulmonary disease, gastroesophageal reflux disease, and hyperlipidemia.
Chronic medications included sustained-release verapamil 180 mg/day, esomeprazole 40 mg/day, telmisartan 80 mg/day, furosemide 40 mg/day, montelukast 10 mg/day, colesevelem 1875 mg/day, oxaprozin 600 mg/day, fluticasone 0.05% nasal spray 2 squirts per nostril daily, albuterol 90 μg/ipratropium 18 μg meter-dosed inhaler 2 puffs 4 times daily, and budesonide 200 μg dry powder inhaler 2 puffs daily. She had been taking all these medications for at least a year. She denied significant over-the-counter or herbal drug use. She also denied any significant changes in her diet, specifically an increase in grapefruit consumption.
Physical examination revealed the patient to be lethargic and slightly confused. Her heart rate was slow but regular. Lungs were coarse and without wheezes or crackles. Neck veins revealed no distension, and her extremities revealed no cyanosis or edema. An electrocardiogram (ECG) revealed the patient to be in a junctional rhythm (Figure 1). Of note, 2 days prior to her presentation in the ED, the patient had been seen by her primary care physician for nasal congestion and malaise. She was diagnosed with a sinus infection and started on telithromycin 800 mg/day. She reported that, until the current episode, she had been feeling better since starting the antibiotic.
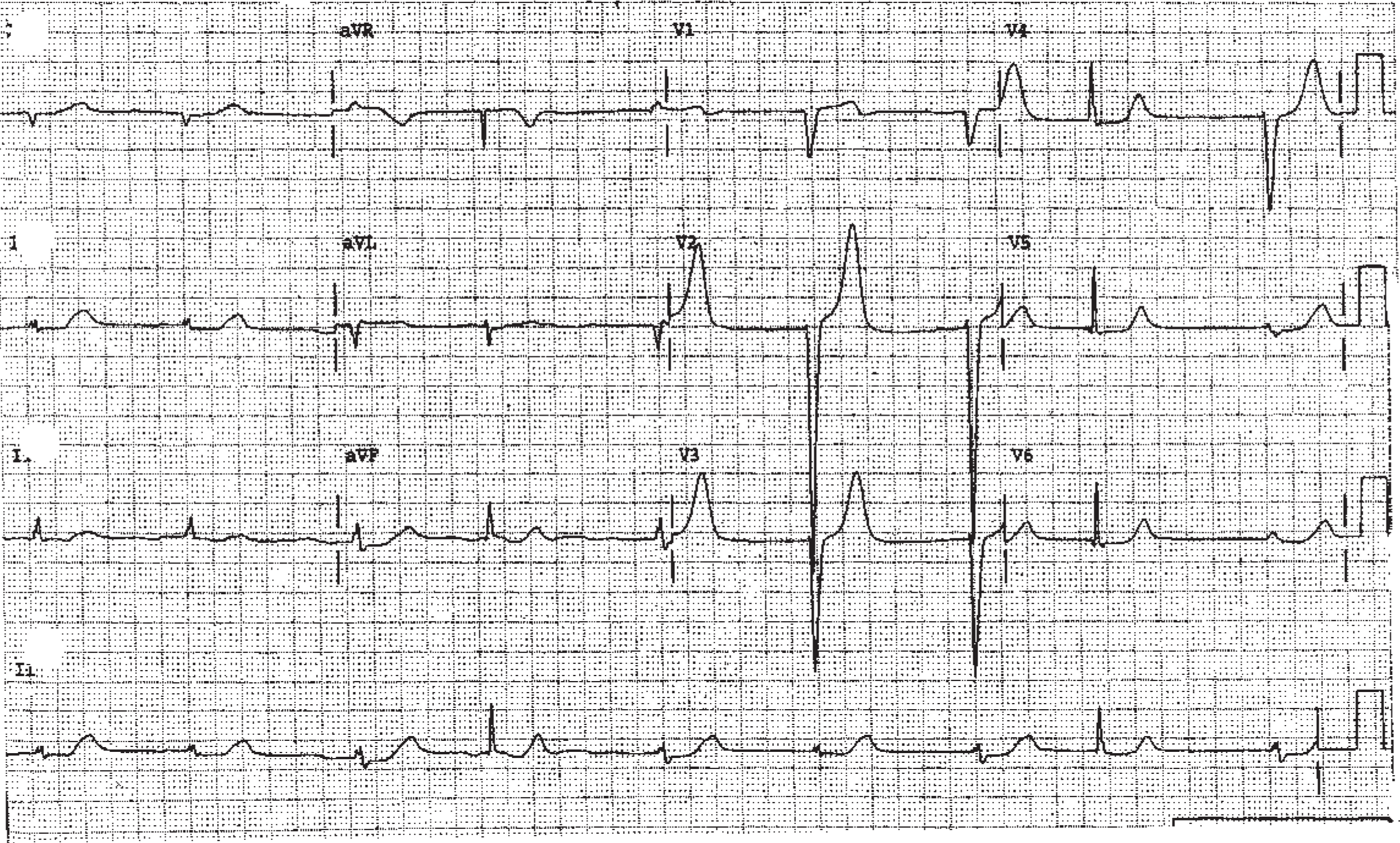
Twelve-lead electroardiogram showing junctional rhythm on admission.
Once in the ED, the patient was administered 2 L of NaCl 0.9% through rapid intravenous infusion, with no improvement in her blood pressure. All oral medications were discontinued. She was then started on intravenous infusions of dopamine followed by norepinephrine, with her systolic BP rising to 80–90 mm Hg with dopamine 17 μg/kg/min and norepinephrine 3 μg/kg/min. The cardiology service was consulted for the junctional bradycardia, and a transvenous pacemaker was placed through the left internal jugular vein. The heart was paced at 100 beats/min with only minimal improvement in BP.
Initial laboratory results revealed serum sodium 120 mEq/L, potassium 4.8 mEq/L, bicarbonate 22 mEq/L, creatinine 1.5 mg/dL, creatine kinase 235 U/L, troponin-I <0.3 ng/mL, lactic acid 3.3 mEq/L, hemoglobin 10.5 g/dL, white blood cell count 10.5 × 103/mm3, and quantitative d-dimer >20 ng/mL. An echocardiogram performed at the bedside revealed normal ejection fraction, with no ventricular wall motion abnormalities. The echocardiogram did, however, reveal dilatation of the right ventricular chambers and an elevated central venous pressure. Based on this finding, in conjunction with the patient's clinical presentation and elevated d-dimer, the diagnosis of pulmonary embolism was considered. The patient underwent a spiral computed tomography scan that was negative for pulmonary embolism.
At this time the patient remained clinically stable on the dopamine and norepinephrine infusions and was in a fully paced rhythm. She was transferred to the intensive care unit for close observation. On the morning of hospital day 2, the patient was fully alert and oriented. She was questioned about her medications and reported that she had been faithfully using her prescribed pill box. She felt that it was highly unlikely that she had inappropriately dosed her medications. An inquiry to her community pharmacy confirmed her drug history and that she had been receiving refills at appropriate intervals. She reiterated that the only recent change in her medications was the addition of telithromycin.
By midday, the patient's BP rapidly improved, and her pressors were steadily decreased and discontinued. That evening, her pacemaker was turned off and telemetry strips revealed an underlying junctional rhythm at 60–70 beats/min. The pacemaker was restarted at a back-up rate of 40 beats/min. The patient remained stable and, on the morning of hospital day 3, converted to normal sinus rhythm with a rate of 80–90 beats/min. The transvenous pacemaker was discontinued, and the patient was transferred out of the intensive care unit in stable condition. The remainder of her hospitalization was unremarkable, and she remained stable until discharge.
Discussion
We attributed our patient's symptoms to verapamil toxicity. Although the Naranjo probability scale is not specifically designed to be used in evaluating drug—drug interactions, we did use the scale to determine the probability that the patient's symptoms were caused by verapamil. 6 Our calculations indicate that her symptoms were probably due to verapamil. At toxic serum concentrations, verapamil can completely occupy and block the myocardial L-type channel, leading to conduction abnormalities. Verapamil also decreases calcium concentrations in arterial smooth muscle cells, leading to hypotension. In fact, our patient's presentation is similar to accounts of verapamil overdoses reported in the literature. 7 Verapamil toxicity causes more conduction abnormalities than do other calcium-channel blockers. ECG findings can include bradycardia with primary, secondary, or complete atrioventricular block. Additionally, verapamil toxicity can lead to sinus node arrest, with the ECG showing a junctional or ventricular escape rhythm with no atrial activity. 8 Other possible ECG manifestations can include QT prolongation, ST depression, T wave flattening, prominent U waves, and, occasionally, atrial fibrillation. Hypotension associated with verapamil toxicity can be severe, and the decreased perfusion to tissues can lead to subsequent lactic acidosis. Other effects associated with verapamil toxicity include pulmonary edema, confusion, coma, nausea, ileus formation, and, occasionally, hyperglycemia. 8 Our patient presented with several symptoms suggestive of calcium-channel antagonist toxicity, including severe hypotension and bradycardia. Her initial ECG showed sinus arrest, which was also suggestive of verapamil toxicity, as was her lactic acidosis.
We feel that, based on our questioning of the patient, her long adherence to verapamil therapy, and information from her pharmacy, we were able to rule out an accidental overdose of the drug. As telithromycin has the potential for drug—drug interactions, we attributed the patient's signs and symptoms to a probable interaction between this drug and verapamil. This diagnosis, we feel, is further corroborated by the relative rapidity in which the patient recovered. Verapamil is extensively metabolized hepatically, with the parent drug and norverapamil primarily metabolized through the CYP2C8, 3A4, and 3A5 pathways. 9 As noted above, telithromycin has not been shown to be a CYP450 inhibitor in vitro. However, because approximately 50% of the drug is metabolized through CYP3A4, the possibility of displacement of another substrate for this pathway is possible. The manufacturer of telithromycin warns against prescribing the drug concomitantly in patients receiving cisapride and midazolam and cautions that CYP3A4-metabolized drugs with a narrow therapeutic index (eg, tacrolimus) may need dosage adjustment. 1 Our patient had been taking her other medications listed at the same doses for at least a year, making an interaction with any of these agents unlikely. Additionally, esomeprazole, telmisartan, and oxaprozin are not appreciably metabolized through the CYP2C or 3A pathways.10–12 Montelukast is extensively metabolized in vitro by CYP3A4 and 2C9, yet few clinically relevant interactions with this drug have been reported.13,14 Interestingly, a recent report found an increased risk of sudden cardiac death (attributed to ventricular tachyarrhythmias) with erythromycin. 15 The rate of sudden death was significantly increased when erythromycin was coprescribed with a drug known to inhibit the CYP3A. Although telithromycin is not a macrolide, our report does highlight the risk of cardiovascular adverse events in a related class of antibacterials and the increased risk of these events when interacting drugs are coprescribed.
Although relatively new to the US market, telithromycin has been available in other countries for several years. A number of randomized controlled studies have shown the drug to be at least as efficacious as comparator antibiotics for community-acquired pneumonia, bacterial sinusitis, and exacerbations of chronic obstructive pulmonary disease. 16 However, many of these trials excluded patients taking medications that may be likely to interact with telithromycin or did not list any drug interactions found in study patients.16,17 It has been noted that formal phenotyping or drug—drug interaction studies could help clinicians determine the potential for serious interactions with telithromycin. 3 Certainly, premarketing studies do not always fully determine the interaction potential for a medication. Standardization of in vitro methods for determining CYP450 metabolic interactions is needed, and this may translate into the discovery of clinically significant interactions from postmarketing reports. 18 For example, although telithromycin product information states that no pharmacokinetic or pharmacodynamic interactions between the drug and warfarin were found, 1 a recent report suggests that such an interaction may in fact exist. 19
Conclusions
Verapamil toxicity was probably the result of an interaction with telithromycin in our patient. We suggest that clinicians use caution in prescribing telithromycin for patients receiving verapamil until other evidence either confirming or refuting our observation is found.