
Abstract
OBJECTIVE:
To review the pharmacology, pharmacokinetics, efficacy, and safety of Exubera, a novel, dry-powder formulation of insulin for inhalation, and describe patient satisfaction and quality-of-life data.
DATA SOURCES:
A MEDLINE search (1966–November 2004) was conducted using the key words inhaled insulin and Exubera for clinical trials limited to human research published in English. BIOSIS Previews and the American Diabetes Association Scientific Abstracts were used for published abstract information.
STUDY SELECTION AND DATA EXTRACTION:
All available human studies of Exubera were selected for review. References of identified articles were used for additional citations.
DATA SYNTHESIS:
Exubera is a rapid-acting insulin administered by oral inhalation before meals with long-acting insulin administered subcutaneously once or twice daily for type 1 or 2 diabetes mellitus. Exubera provides similar efficacy and improved patient satisfaction compared with standard subcutaneous insulin therapy (ie, NPH twice daily with regular insulin before meals). Efficacy has also been demonstrated for Exubera when used as adjunctive therapy with oral medications for type 2 diabetes. The onset of Exubera is more rapid and its duration of action is similar to that of regular insulin. To date, Exubera administered before meals with a once-daily long-acting subcutaneous insulin (usually Ultralente) has been compared with standard subcutaneous NPH/regular insulin regimens. Comparison of premeal Exubera plus a basal long-acting insulin analog (eg, glargine) with a regimen of premeal subcutaneous rapid-acting insulin analog (eg, lispro or aspart) plus a basal long-acting insulin analog (eg, glargine) is needed to fully evaluate Exubera. Pulmonary safety appears to be maintained for up to 4 years, although there are no data, as of this writing, on the use of this agent in patients with pulmonary conditions.
CONCLUSIONS:
Exubera is an effective inhaled insulin for preprandial use in type 1 or 2 diabetes. Improved patient satisfaction over injected insulin increases its potential for use earlier in the treatment of type 2 diabetes.
Keywords
Diabetes mellitus affects >18 million Americans. 1 Type 1 diabetes is diagnosed most often in children, adolescents, or young adults and is characterized by failure of the pancreatic islet cells to produce insulin. 2 Individuals with type 1 diabetes (∼5–10% of those with diabetes) are reliant on the administration of exogenous insulin to replace lost physiologic insulin production. 3 Type 2 diabetes, a mixed-cause disorder affecting 90–95% of Americans with diabetes, is characterized by pancreatic dysfunction, insulin resistance, and excess hepatic glycogenolysis or gluconeogenesis. Type 2 diabetes usually occurs in adults; however, the incidence in children is on the rise. 4 This form of diabetes, whether occurring in adults or children, is highly correlated with insulin resistance and relative insulin deficiency resulting from obesity and sedentary lifestyles. 3 Treatment is aimed at reducing insulin resistance, modifying lifestyle to improve glucose utilization through activity and meal planning, and reducing associated risks. In type 2 diabetes, the metabolic syndrome (hypertension, obesity, hyperlipidemia, altered glucose metabolism) is prevalent, complicating treatment and increasing the need to reduce cardiovascular risks in addition to the potential diabetes complications. 5 The goal for patients with diabetes is to achieve a normal or near-normal blood glucose level to avoid microvascular and, potentially, macrovascular complications associated with poor glycemic control.6–9
Based on the findings of large-scale studies, significant reduction in these diabetes-related complications are achieved with every 1% decrease in hemoglobin (Hb) A1c, highlighting the importance of any improvement in glycemic control. 7 For people with type 1 diabetes, insulin is the foundation of treatment, and initiation at diagnosis is mandatory to normalize glucose levels given the pending or actual state of pancreatic insulin production failure. The prospect of relying on an injected medication is difficult for many patients and may present an adherence challenge due to factors such as fear of needles. A method of insulin delivery obviating the need for injection would be favorable.
Type 2 diabetes presents a different situation given that insulin therapy may be unnecessary or delayed because oral agents and lifestyle modification offer effective therapeutic alternatives for insulin therapy. If initiated in type 2 diabetes, insulin has the ability to potentially overcome insulin resistance, normalize blood glucose levels, and inhibit glycogenolysis and gluconeogenesis. 10 In type 2 diabetes, insulin may be used to augment oral therapy using 1 or 2 injections of long-acting insulin daily in an attempt to optimize therapeutic results. 11 Insulin is sometimes reserved as a therapeutic backup when oral drugs fail rather than introduced early in therapy to achieve control. This delay in insulin therapy for type 2 diabetes is of interest and appears related to several factors including fear of needles and injections, fear of weight gain, sense of therapeutic failure, and expense of supplies. 12 If introduced early to treat type 2 diabetes, insulin may facilitate the ability to gain more rapid glycemic control in patients resistant to oral therapies, thereby minimizing or preventing the onset of diabetes-related complications.
Recent research and development of insulin has taken 2 key directions. Development of products more closely able to mimic physiologic insulin action has been pursued to minimize insulin-related adverse effects, such as hypoglycemia, and optimize glycemic control. In addition, alternative methods of delivery, obviating the need for parenteral injections, are under investigation to facilitate convenience and use of insulin earlier in the disease process. Physiologic subcutaneous insulin dosing employs longer-acting insulins (eg, glargine, Lente, Ultralente, NPH) administered to simulate the body's daily basal insulin production with rapid-acting (lispro or aspart) or short-acting (regular) insulin given for prandial coverage of mealtime glycemic excursions. Subcutaneous insulin pump systems also offer a method for physiologic insulin dosing without the need for multiple injections throughout the day. Physiologic insulin dosing has demonstrated excellent ability to control diabetes. 13 With physiologic dosing, the potential for accumulation of insulin may be reduced when using short-acting or rapidly cleared insulins, potentially limiting related hypoglycemia.
Novel methods for insulin delivery under investigation include oral and nasal inhalation aerosols, transdermal patches, buccally administered gels, and oral dosage forms. 14 This article reviews Exubera, a dry-powder, orally inhaled form of fast-acting insulin using the Nektar Pulmonary Inhaler. Exubera is currently in extended Phase III studies to evaluate long-term pulmonary safety and efficacy. Prospective inhaled insulin products are an exciting development in diabetes care with the ability to reduce or avoid the need for parenteral injections and the ability to mimic prandial insulin action with fast-acting products. Longer-acting forms of inhaled human insulin are in the initial stages of development using a polyethylene glycol formulation to provide sustained action; these products are not discussed in this review. 15
Data Sources
A MEDLINE search (1966—November 2004) was conducted using the key words inhaled insulin and Exubera for clinical trials limited to human research published in English. Follow-up searches were performed using key author names (Cefalu, Skyler, and Inhaled Insulin Study Group). References of identified articles were used for additional citations. BIOSIS Previews and the American Diabetes Association 2004 Scientific Abstracts were evaluated for published abstract information.
Study Selection and Data Extraction
Clinical trials evaluating the safety and efficacy of inhaled insulin (Exubera) for type 1 and 2 diabetes in adults and children were selected. Studies evaluating effects on patient satisfaction or quality of life with diabetic therapy were included. Data on Exubera recently published in abstract format following presentation at scientific meetings were included. Studies evaluating drug interactions or adverse effects of any short-acting inhaled insulin formulation were evaluated where data for Exubera were limited.
Pharmacology
The investigation of inhaled insulin began in the early 1920s. In the 1970s, Wigley et al. 16 demonstrated a hypoglycemic effect in rabbits using regular insulin delivered as an inhaled aerosol via a nebulizer. Soon thereafter, they demonstrated a hypoglycemic effect in 3 healthy volunteers and 4 participants with diabetes by delivering regular pork—beef insulin as a nebulized mist. These pioneers laid the groundwork for today's advances. Several devices are being developed and show promising effects for the inhalation of insulin via liquid aerosols or dry-powder formulations into the lungs.
The lungs provide an excellent site of absorption because of the vast surface area, highly permeable membranes, and rich blood perfusion. The optimal particle size for deposition into the alveoli is 1.5–2.5 μm. Larger particles deposit in the tracheobronchial region and smaller particles are exhaled. 17 Exubera is absorbed into the alveolar capillary bloodstream via trancytosis. The insulin particles, approximately 1–5 μm in size, are transported across the cell membranes of the alveolar epithelium by billions of vesicles. The insulin-containing vesicles are transported through the alveolar capillary endothelium cells and then released into the alveolar capillary bloodstream for absorption. 18 Approximately 6–10% of the inhaled insulin is absorbed across the respiratory mucosa into the systemic circulation. Bioavailability is not improved by breath holding.18–20
Pharmacokinetics
Exubera is a dry-powder formulation of insulin (∼60%), mannitol, glycine, and sodium citrate. 17 Dry-powder formulations can deliver a higher dose per puff, are stable at room temperature, and resist microbial growth compared with liquid formulations. 18
The onset of action of Exubera reflects prandial physiologic insulin release. Using a euglycemic glucose clamp (a technique to evaluate the impact of insulin treatment on glucose and serum insulin concentrations), Heinemann et al. 19 compared inhaled insulin (delivered as an aerosol of solid insulin particles), regular subcutaneous insulin, and intravenous insulin in matched healthy nonsmoking men (N = 11). The onset of action of inhaled insulin was significantly faster than subcutaneous regular insulin (31 vs 54 min; p < 0.00001). Maximal metabolic effect was achieved in 108 minutes with inhaled insulin compared with 147 minutes with subcutaneous regular insulin (p < 0.0001). Maximum insulin serum concentrations were achieved in 24 versus 106 minutes, respectively. A more recent study compared a dry-powder inhaled insulin with subcutaneous lispro and subcutaneous regular insulin in 18 healthy, nonsmoking men using the euglycemic glucose clamp technique. 20 Inhaled insulin had a faster onset of action at 28 minutes versus subcutaneous regular insulin (48 min; p = 0.0011) and subcutaneous lispro insulin (40 min; p = 0.0704). The maximal metabolic action of inhaled insulin was comparable to that of regular insulin, but statistically significantly slower than lispro insulin (p = 0.011).
Studies have demonstrated a duration of approximately 6 hours with inhaled insulin, longer than that of subcutaneous lispro insulin but comparable to subcutaneous regular insulin.19,20 These pharmacokinetic results demonstrate a favorable prandial insulin profile due to a more rapid onset than subcutaneous injection and sustained action over 3 hours. Despite a similar duration of action, inhaled insulin has demonstrated lower rates of hypoglycemia than subcutaneous regular insulin.21–23 The mechanism of action for the lower incidence of hypoglycemia is unknown (p = 0.011).
For optimal glycemic control, it is critical to have a reproducible pharmacokinetic response after inhalation of Exubera. Gelfand et al. 24 treated 16 insulin-naïve patients in a 4-way, randomized-sequence crossover study involving 2 inhalations of Exubera and 2 subcutaneous injections of regular insulin. The patients received 5 standardized test meals (Sustacal), first with no therapy and then during the crossover period. Postprandial glucose levels and AUC at various time points were measured for all treatment groups. There were no significant intrasubject differences between the 2 same-dose route sessions in all 16 subjects. At comparable doses, the reproducibility of the pharmacokinetics of Exubera in insulin-naïve patients was equivalent to that of subcutaneous regular insulin.
Another pharmacokinetic study demonstrated similar results in elderly obese patients with type 2 diabetes. Twenty patients (10 men) were given 2 inhalations of insulin (4 mg each) and 2 subcutaneous injections (12 units each) of regular insulin in a randomized crossover sequence. 25 After an overnight fast, subjects received 1 of the 4 doses, and serum unbound insulin and fasting plasma glucose levels were measured at baseline, 2 hours, and 6 hours after administration. The insulin pharmacokinetics and postdose glucose pharmacodynamics demonstrated little within-subject variability.
The pharmacokinetics of Exubera have not been studied in individuals with pulmonary illnesses such as asthma or chronic obstructive lung disease. The use of another orally inhaled insulin solution (vs a dry powder) has been studied in nondiabetic individuals (mean age 31.0 y, healthy; 27.9 y, asthma) with mild to moderate severity asthma demonstrating reduced AUC (p = 0.013) and no significant difference (p = 0.094) in peak concentration (Cmax), although subjects with asthma consistently absorbed less insulin. 26 This study found increased intrasubject variability for AUC and Cmax for subjects with asthma compared with healthy subjects, with less reduction in blood glucose levels for the asthma group (p = 0.007). To date, there are no published trials evaluating Exubera, a dry-powder formulation, in subjects with pulmonary conditions, precluding its use in this population until further information is available.
Clinical Trials
Two Phase II proof-of-concept studies evaluating the use of Exubera for glycemic control, one in type 1 diabetes 21 and one in type 2 diabetes, 22 followed by 3 randomized clinical trials evaluating efficacy27–29 have been published. Long-term extension studies evaluating safety and efficacy were available in recent abstract form for review.30,31 Four clinical trials comparing oral and injectable treatments with Exubera were available in abstract format.30,32,34 Three randomized, open-label studies evaluating patient satisfaction with Exubera versus standard subcutaneous insulin therapy were available for review35–37 along with 3 abstracts.38–40 A summary of the information supporting short- and long-term efficacy and safety is presented in Table 1 (published trials) and Table 2 (published abstracts).
Comparison of Published Inhaled Insulin Clinical Trial Data
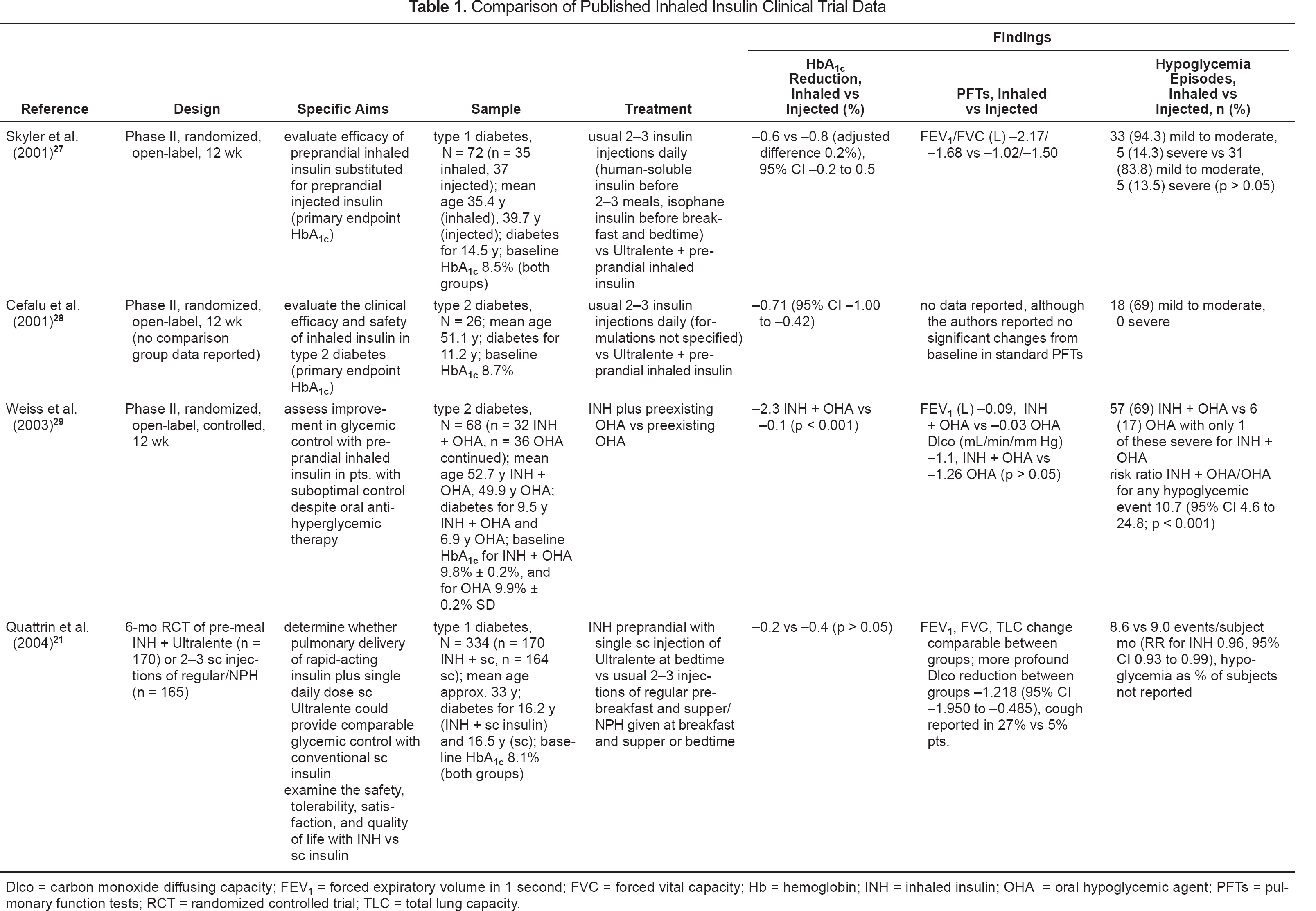
Dlco = carbon monoxide diffusing capacity; FEV1 = forced expiratory volume in 1 second; FVC = forced vital capacity; Hb = hemoglobin; INH = inhaled insulin; PFTs = pulmonary function tests; TLC = total lung capacity.
Phase III Published Abstract Information on Exubera in Adults
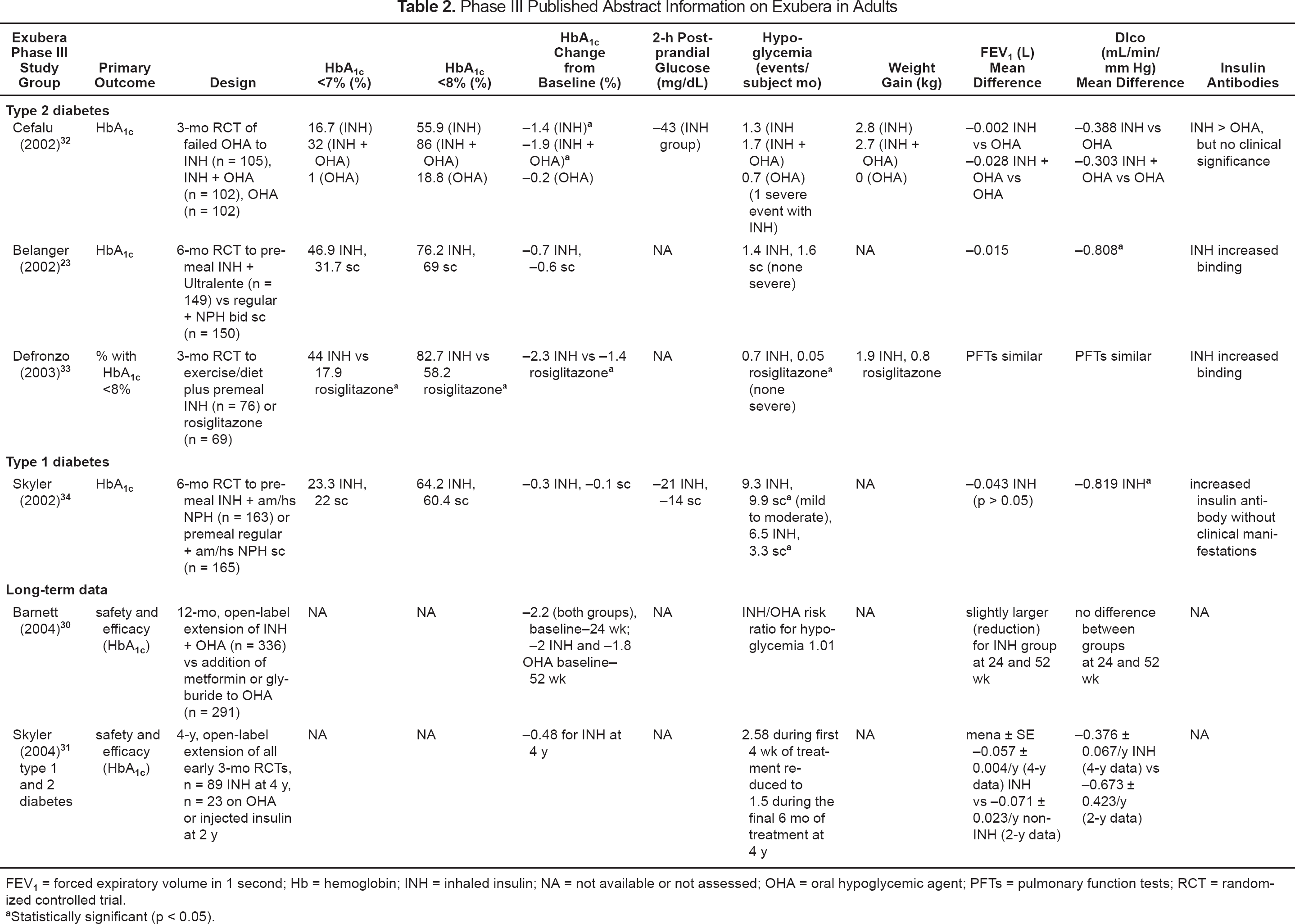
FEV1 = forced expiratory volume in 1 second; Hb = hemoglobin; INH = inhaled insulin; NA = not available or not assessed; OHA = oral hypoglycemic agent; PFTs = pulmonary function tests; RCT = randomized controlled trial.
Statistically significant (p < 0.05).
The early Phase II studies demonstrated the efficacy of Exubera in both type 1 and 2 diabetes using preprandial inhalations in addition to long-acting injected insulin (Ultralente). Efficacy of inhaled insulin plus subcutaneous bedtime Ultralente versus standard subcutaneous insulin (human-soluble insulin prior to meals and isophane insulin at breakfast and bedtime) was demonstrated for 72 subjects with type 1 diabetes (baseline mean HbA1c 8.5%) by the Inhaled Insulin Phase II Study Group using an open-label, parallel-group, randomized design. 27 In this trial, glycemic control for subjects (n = 35) randomized to receive preprandial Exubera plus Ultralente at bedtime was similar to that for the control group receiving standard subcutaneous insulin at 12 weeks.
The same group randomized 26 patients with type 2 diabetes, aged 35–65 years, to receive 1–2 inhalations (open label) of Exubera before meals along with bedtime subcutaneous Ultralente. 28 This 12-week treatment phase followed a 4-week baseline phase involving 2–3 subcutaneous injections of insulin daily (formulations not specified), meal studies, standardized glucose monitoring, pulmonary function testing, and weight education. The HbA1c decreased from a baseline mean of 8.67% by 0.71% (? 0.72%), with patients requiring less insulin than that injected (regular plus long-acting) prior to study entry. The design and adequacy of controls in this trial were unclear in this initial report. In a letter to the editor addressing this concern, Cefalu 41 explained the use of a randomized control group, not described in the initial study publication, maintained on standard subcutaneous insulin (described as “continued subcutaneous insulin” to imply the pt.'s usual 2–3-times-daily regimen) with no difference in HbA1c control between groups. This information helped to clarify the initial study report and further emphasized the comparative efficacy of inhaled insulin versus standard subcutaneous therapy. It is difficult, however, to interpret the findings of this study given the failure of the authors to fully describe the design, and confidence intervals were not clear for the change in HbA1c reported.
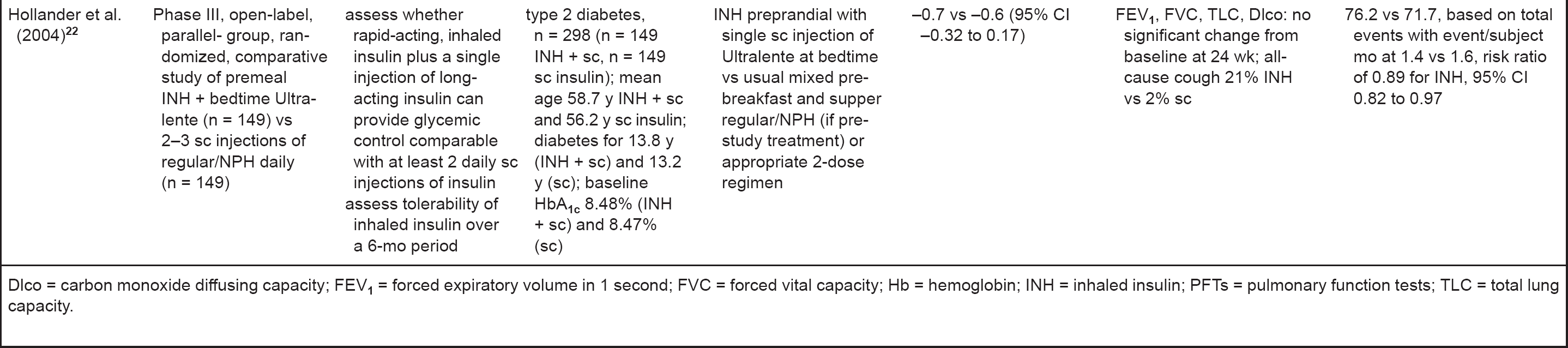
In a randomized controlled study, Exubera was efficacious in combination with oral diabetes therapies in 68 patients with type 2 diabetes not controlled with either a sulfonylurea and/or metformin. 29 After 12 weeks of treatment with preprandial Exubera plus preexisting oral hypoglycemic agents, the study group had a significantly greater reduction in HbA1c compared with the control group using oral hypoglycemic therapy only (mean −2.3% Exubera vs −0.1% control; p < 0.001). Two randomized, open-label, controlled trials of 6 months' duration comparing Exubera plus bedtime subcutaneous Ultralente with 2–3 daily injections of standard regular/NPH subcutaneous insulin therapy have recently been published, further demonstrating the efficacy of inhaled insulin.21,22 In the trial evaluating insulin use in adults with type 1 diabetes, HbA1c was reduced comparably for both the inhaled insulin treatment group and the subcutaneous insulin control (NPH and regular insulin before breakfast, regular insulin before dinner, and a second NPH insulin injection either before dinner or at bedtime) with an adjusted treatment group difference in HbA1c of 0.16% (95% CI −0.01 to 0.32). 21 A similar reduction in HbA1c was demonstrated between groups when these same regimens were compared for subjects with type 2 diabetes (adjusted treatment group difference in HbA1c −0.07%; 95% CI −0.32 to 0.17). In this study, control subjects continued the NPH and regular insulin regimen before breakfast and supper that they were on prior to the study or were placed on a 2-dose regimen (not specifically described) based on glycemic control. 22
The open-label design used for the available trials of Exubera limits the ability to make conclusions beyond the comparability of Exubera given with long-acting subcutaneous insulin versus standard insulin therapy assuming similar adherence in both groups. Although comparison regimens consisted of 2–3 injections of standard insulin therapy or regular/NPH mix, trials comparing subcutaneous rapid-acting insulin analogs (eg, lispro) with basal insulin versus Exubera with basal insulin are needed to fully evaluate the inhaled insulin product.
The safety of Exubera appears similar to that of standard subcutaneous insulin based on the findings of these preliminary investigations. Rates of severe (ie, requiring assistance of another person, coma, or seizure) and mild to moderate hypoglycemia (episodes other than those defined as severe) were not different for the treatment and control groups, with event rates for severe hypoglycemia up to 0.08 events per patient-month for inhaled insulin. 24 Weight gain was similar for both inhaled and subcutaneous insulin in early clinical trials, although this was not a primary study endpoint.27,28
Data recently presented at the 2004 American Diabetes Association Scientific Sessions, continue to support the efficacy of Exubera for control of both type 1 and 2 diabetes. Therapy extension for 1 and 4 years demonstrated sustained efficacy as well as pulmonary safety based on lack of significant change in forced expiratory volume in 1 second (FEV1) and lung diffusion capacity. The investigators reported sustained efficacy (HbA1c 7.4% at 24 wk, 7.6% at 52 wk) at one year for Exubera given with metformin or glyburide in type 2 diabetes compared with the addition of a second oral agent (HbA1c 7.8% at 52 wk). 30 In another report, ongoing efficacy at 4 years was evaluated for subjects from any of the 3-month initial studies electing to continue therapy (n = 89 of 204 electing continuation). 31 Mean ± SD HbA1c was 8.23% ± 1.21% at 4 years compared with 8.71% ± 1.49% at baseline, with the inhaled insulin dose increasing slightly from 0.15 to 0.18 mg/kg over the 4 years.
Patient satisfaction data with Exubera are better than those of subcutaneous insulin in repeated studies. Satisfaction was assessed at baseline and 12 weeks for parent clinical studies and at one year for subjects electing extension of either inhaled or subcutanous insulin. In one trial, subject preference for inhaled insulin extension treatment highlighted the desire for this therapy. 35 The majority (75.4%) of subjects who were randomized to receive subcutaneous insulin in the parent study elected to switch to inhaled insulin for the extension study, with 85% of subjects initially on the inhaled formulation preferring to continue this therapy. Efficacy was sustained at one year regardless of treatment group (reduction of 0.8% HbA1c), although there was much greater satisfaction (37.9% vs 3.1%; p < 0.01) and ease of use (43.2% vs −0.9%; p < 0.01) reported for all subjects using inhaled insulin at one year. In subgroup analyses, participants who switched from initial inhaled insulin to subcutaneous insulin extension therapy (n = 8) had reduced satisfaction from their 12-week assessment following inhaled therapy. In contrast, the cohort switching from subcutaneous to inhaled therapy (n = 40) had marked improvement in satisfaction.
Satisfaction for 51 subjects participating in a 12-week parent study was excellent for Exubera plus subcutaneous long-acting insulin (satisfaction improvement from baseline 31%; p < 0.05) over standard subcutaneous insulin therapy (13%; 95% CI 7 to 19). 37 Satisfaction, convenience or ease of use, and social comfort with therapy were all improved for Exubera over subcutaneous insulin (25%, 30%, and 10% differences in satisfaction improvement between therapies, respectively) in an analysis reported by Gerber et al. 36 Some data presented in abstract form continue to reflect improved satisfaction with Exubera therapy for patients with first exposure to any insulin following failure of oral hypoglycemic agents, although this was not a primary study endpoint. 32 Satisfaction continues to be improved and sustained for Exubera compared with standard subcutaneous insulin in short- and long-term studies.38–40
A limited number of randomized clinical trials have demonstrated the efficacy, relative safety, and satisfaction with therapy for Exubera in combination with other therapies (for type 2 diabetes) or with long-acting subcutaneous insulin (for type 1 and 2 diabetes). The efficacy of Exubera, based on these trials, appears comparable to that of regular insulin when used for prandial blood glucose control. Although abstract information is available to further support the efficacy, safety, and satisfaction with Exubera, this information is limited by the inability to fully assess study quality and design until these studies have been published. As of this writing, trials of monotherapy using Exubera have not been conducted, although the use of preprandial inhalations is logical and may provide for early use of insulin in type 2 diabetes controlled inadequately on diet and exercise alone.
Safety and Tolerability
ADVERSE EFFECTS
Hypoglycemia, cough, and bitter taste were reported in the clinical trials of Exubera. Withdrawal from clinical trials due to adverse effects was limited to only 5 of 354 subjects experiencing a problem studied in the 3 primary, open-label clinical trials (reported as cough for 1 subject, hypoglycemia for 2 subjects by Quattrin et al. 21 ; not specifically reported by other investigators21,27). Hypoglycemia is the primary adverse effect with insulin use and is expected with inhaled insulin. The risk for hypoglycemia should theoretically be lower when fast-acting, short-duration insulin is dosed appropriately to cover mealtime glucose loads and dose accumulation due to overlapping durations of action is not an issue. The overall risk of hypoglycemia for inhaled insulin appears similar to or lower than that for subcutaneous insulin, although it is difficult to evaluate this effect given the different time—action profiles of the comparator regimens (eg, Ultralente vs NPH). A recent open-label trial in patients with type 1 diabetes comparing similar doses of inhaled insulin before meals plus bedtime Ultralente insulin versus NPH insulin twice daily with regular insulin before breakfast and dinner found a lower rate of hypoglycemia for the inhaled insulin group (8.6 vs 9.0 events/subject mo) with a hypoglycemia risk ratio of 0.96. 21 In another trial comparing the same treatment, but in type 2 diabetes, a lower risk of hypoglycemia was also reported for inhaled insulin users (1.4 vs 1.6 events/subject mo). 22 In this study, doses of insulin used by each group appeared similar (23.17 vs 23.79 units short-acting insulin and 41.27 vs 41.66 units long-/intermediate-acting insulin, inhaled vs subcutaneous groups, respectively). The Exubera Phase III Study Group found the rate of hypoglycemia to be lower for Exubera than for injected insulin (1.4 events/subject mo vs 1.6 for subcutaneous insulin), although the actual doses of inhaled or injected insulin required were not reported. 23
The absorption rate of Exubera delivered through the pulmonary vasculature is similar to that of subcutaneously injected short-acting insulin analogs with duration of action similar to regular insulin.19,20 These mutual pharmacokinetic qualities may explain the similarity in prevalence of hypoglycemia between subcutaneous short-acting insulin and Exubera, an adverse effect related to peak action and duration of effect. In contrast, the risk for hypoglycemia with Exubera appears greater than for oral hypoglycemic diabetes therapies. Weiss et al. 29 identified 69% of treatment subjects reporting hypoglycemic events versus 17% of control subjects using oral hypoglycemic agents; however, the majority (56/57) of these events were mild to moderate, as opposed to severe and requiring the assistance of another person. Cefalu et al. 32 reported a higher rate of hypoglycemia with Exubera than with oral therapy, although only one severe hypoglycemia event (ie, required assistance) occurred. In a 3-month trial of Exubera versus rosiglitazone, the rate of hypoglycemia was higher for the inhaled insulin group (0.7 vs 0.05 events/subject mo) with no cases of severe hypoglycemia reported. 33 This higher risk to patients for hypoglycemia when inhaled insulin is added to an oral diabetes regimen should be expected given the reliable hypoglycemic effect demonstrated in clinical studies. Patient education when initiating inhaled insulin should highlight the prevention and management of hypoglycemia, especially for those naïve to standard subcutaneous insulin therapy.
Other adverse effect concerns for Exubera include the potential formation of insulin antibodies and effects on lung health with ongoing delivery of insulin to the pulmonary tissue and vasculature. Insulin antibody formation was initially reported to be increased with inhaled insulin possibly due to immunologic sensitivity of the pulmonary system, although this is not clear. 42 The primary concern with increased antibody formation is the potential for effects on insulin resistance. There is also the concern for circulating insulin antibody complexes able to release insulin in a time-delayed fashion, potentiating hypoglycemia and complicating dosing. Although limited studies have demonstrated increased insulin antibody formation with inhaled insulin compared with parenterally administered insulin, increased adverse effects in these short-term trials have not been demonstrated.34,43
Initial effects on pulmonary function appear limited; however, the drug is not currently recommended in patients with pulmonary disorders due to unclear influences of inflammation or disease on insulin absorption. In 2002, Pfizer completed initial Phase III studies for Exubera and has extended the clinical trial phase to allow for evaluation of longer-term use on pulmonary function and health. Recent data (Table 2) indicate continued safety to the lungs based on FEV1 and carbon monoxide lung diffusion capacity with use at 1 year 30 and up to 4 years. 31 This is consistent with lung function response in short-term studies at 3 and 6 months.
Precautions and Contraindications
The use of Exubera in individuals with pulmonary illnesses has not been studied and cannot be recommended at this time. Initial data at 4 years are demonstrating safety in pulmonary function in patients with no apparent pulmonary illness. Attempts to avoid hypoglycemia through counseling, education, appropriate dosing, and follow-up should be made to minimize the risk of severe events. Use of Exubera is not recommended in patients who smoke due to variable effects of the smoking on drug absorption. Treatment of children <18 years of age is not recommended due to lack of studies. There are no data currently available on the use of inhaled insulin in pregnant women.
DRUG INTERACTIONS
Cigarette smoking has been shown to have significant effects on total exposure (AUC) and Cmax for inhaled insulin.44–46 An increase in the AUC and Cmax appears related both to the inhalation effects of the smoke, as well as to the acute bronchoconstrictive effects of nicotine causing increased alveolar—capillary permeability. Smoking cessation also changes the pharmacokinetics of inhaled insulin. Three weeks following smoking cessation, inhaled insulin Cmax decreased to 49% and AUC decreased to 59% of the active smoking levels, with effects not completely reversed by 13 weeks' cessation. Incidence of hypoglycemic events decreased with time after smoking cessation corresponding to the reduction in Cmax and AUC. 46 The effects of other smoked products or second-hand smoke inhalation have not been studied; therefore, caution should be exercised due to the potential alteration of lung health and potential influence on insulin absorption. Exubera use in smokers or those in the early phases of smoking cessation cannot be recommended at this time due to unpredictable influences on the pharmacokinetics of inhaled insulin.
As of March 22, 2005, there are no data on the use of insulin with other inhaled medications such as albuterol or corticosteroids. Data are lacking, in part, due to the potential concern of lung diseases on insulin absorption resulting in contraindications to use of inhaled insulin in patients with pulmonary illnesses at this time.
Dosing and Administration
Exubera is packaged in single-dose blister packs of 1 or 3 mg (equivalent to 3 or 9 units of subcutaneous short-acting insulin, respectively). Each milligram of inhaled insulin delivers approximately 2–3 units of subcutaneous insulin. The dose should be titrated based on glucose response. 29
An individual blister pack is placed into the Nektar Pulmonary Inhaler (Figure 1). This device disperses the powder as an aerosol cloud into a holding chamber. The patient inhales the aerosolized powder orally by taking a slow, deep breath. Bioavailability is not improved by breath holding after inhalation of the dose. 16 As of March 22, 2005, it is unclear whether multiple doses can be dispersed into the holding chamber or whether the individual blister packs must be inhaled separately. In the available published trials, the maximum daily dose evaluated was 92 units, potentially requiring multiple inhalations. 21

Nektar Pulmonary Inhaler. Reprinted with permission from Nektar Therapeutics.
Cost
The cost of Exubera is unknown as of March 22, 2005. Pfizer and Aventis have submitted a request for marketing approval to the European Medicines Agency, the European equivalent of the Food and Drug Administration. On March 2, 2005, Pfizer and Sanofi-Aventis announced that the Food and Drug Administration had accepted for filing a new drug application to market Exubera in the US. 47
Summary
Exubera is a novel diabetes therapy. It provides comparable prandial glucose control in combination with long-acting subcutaneous insulin for type 1 or 2 diabetes compared with standard subcutaneous insulin therapy with NPH and regular insulin. Efficacy has also been proven as adjunctive therapy with oral medications for type 2 diabetes. It is similar to other available prandial insulin formulations, with onset more rapid and duration of action similar to that of regular insulin. Reported pulmonary safety appears to be maintained for up to 4 years in clinical trials. The lack of data on the use of this agent in patients with pulmonary conditions or using other inhaled medications precluded its use in these populations.
The pulmonary route of delivery for insulin Exubera offers an advantage for patients preferring an alternative to injections and is supported by positive patient satisfaction data. Exubera is an exciting addition to the treatment armamentarium for patients with diabetes reliant on standard subcutaneous insulin therapy throughout the day. Additionally, it appears to provide a safe and effective option for patients with type 2 diabetes to gain improved glycemic control while minimizing the discomfort associated with multiple daily insulin injections.