
Abstract
OBJECTIVE:
To report a case of possible interaction of menthol cough drops (Halls) with warfarin in a patient awaiting cardioversion.
CASE SUMMARY:
A 57-year-old white male awaiting cardioversion for atrial fibrillation was prescribed warfarin. His dosage was adjusted to 7 mg daily to provide stable international normalized ratio (INR) values of 2.28–2.68. Approximately one week later, his INR fell to 1.45. During a follow-up interview, the patient reported that he experienced a flu-like illness during the previous week and had been using menthol cough drops. No other potential causes for the decreased INR were found. Illness will most often elevate the INR; we therefore concluded that the cough drops were the likely cause of this reaction, and the warfarin dose was increased to 53 mg/wk. After discontinuing use of menthol cough drops, the warfarin dose was returned to the previous amount and the INR remained stabilized.
DISCUSSION:
An objective causality assessment suggests that the decreased INR was possibly related to the use of menthol cough drops during warfarin therapy. The active ingredient in these cough drops is menthol. Menthol has been shown to affect the pharmacokinetics of other drugs by inducing or inhibiting cytochrome P450 isoenzymes and slowing drug absorption. It is not clear whether these mechanisms played a role in this case. As of January 5, 2005 this is the first case report documenting an interaction between warfarin and cough drops containing menthol.
CONCLUSIONS:
This case documents a significant decrease in the INR following the use of menthol cough drops. Patients who are ill have several factors that can potentially affect their INR and should be monitored closely.
Keywords
Warfarin is known to interact with numerous medications and diet.1,2 Drugs such as ketoconazole and sulfonamides inhibit CYP2C9 and increase warfarin effects, while CYP2C9 inducers, such as carbamazepine and phenytoin, will decrease warfarin effects. Oral antibiotics may increase warfarin effects, killing gut bacteria responsible for conversion of vitamin K to its active form. Aluminum hydroxide and cholestyramine decrease warfarin effects by inhibiting its absorption. Foods containing vitamin K, such as broccoli and turnip greens, will also decrease the effects of warfarin. We describe a case of an interaction between menthol cough drops (Halls) and warfarin that led to a decrease in the international normalized ratio (INR).
Case Report
A 57-year-old white male was receiving warfarin prior to cardioversion for atrial fibrillation. His past medical history, included hypertension, hyperlipidemia, benign prostatic hyperplasia, and coronary artery disease. He had a 10 pack-year smoking history, but did not currently smoke or drink alcohol. He had no known drug allergies. At the time of presentation, his daily medications were lansoprazole 30 mg, loratadine 10 mg, spironolactone 25 mg, simvastatin 20 mg, terazosin 10 mg, atenolol 50 mg, fluticasone nasal spray, lisinopril 20 mg, sustained-release nifedipine 60 mg, nefazodone 300 mg, aspirin 325 mg, and Gen-Teal ophthalmic gel; nitroglycerin 0.4 mg was used as needed.
There were no medication changes during the 3 months prior to initiating warfarin therapy at 7 mg/day (49 mg/wk). The patient's INR goal was 2–3, with a target of 2.5. Therapy was intended to continue until 4 weeks after cardioversion. Because he was awaiting cardioversion, therapy was monitored closely and INR was monitored weekly (Table 1). For 3 consecutive weeks, the INRs were within normal range. During week 4 of therapy, the INR dropped to 1.45.
Dosing and Laboratory History
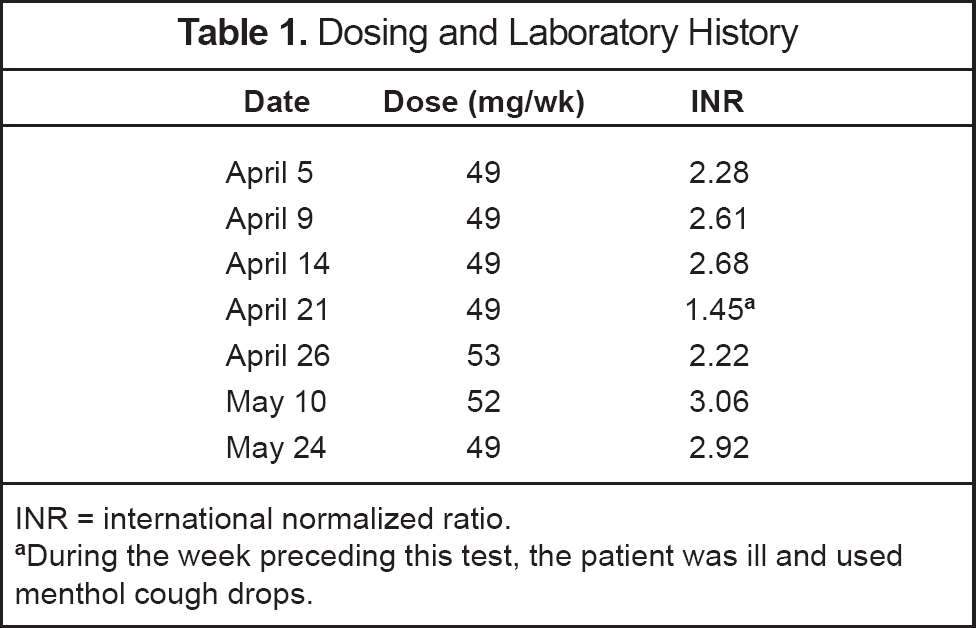
INR = international normalized ratio.
During the week preceding this test, the patient was ill and used menthol cough drops.
Following this precipitous drop in INR, the clinician called the patient, who stated that he had developed a flu-like illness over the past week and had been taking menthol cough drops but no other additional medications. He had been using about 6 cough drops per day for 4 days. He denied changes to his current medication regimen or diet. He also denied missing any warfarin doses.
Subsequently, the warfarin dose was increased to 7 mg on Monday, Wednesday, and Friday, and 8 mg on Sunday, Tuesday, Thursday, and Saturday (53 mg/wk; ∼8% increase). He also discontinued use of menthol cough drops. During week 5, the INR rose to 2.22. His dose was then decreased to 52 mg/wk. During week 7, the INR was 3.06, and the previous dose of 49 mg/week was resumed. The next week, the INR was 2.92.
Discussion
Using the Naranjo probability scale, we determined that the decreased INR was possibly due to an interaction between warfarin and menthol cough drops. 3 The only apparent changes to this patient's diet or lifestyle preceding the drop in INR were his illness and the addition of the cough drops. The effect of flu-like illness on the INR has been described. 2 Ordinarily, an elevated INR is observed. Illness can cause a decrease in appetite, leading to decreased vitamin K consumption and an elevated INR. Vitamin K—dependent clotting factors may also be metabolized more rapidly due to release of cytokines from the immune response during an illness.
The amount of menthol in Halls Cough Drops is 7 mg. Inactive ingredients are dyes, flavors, glucose syrup, sucrose, and water. Menthol is a volatile oil derived from the peppermint plant. Possible mechanisms of interactions could include decreased warfarin absorption, induction of warfarin metabolism, or decreased warfarin effect by vitamin K supplementation.
A MEDLINE search was performed to identify any documented interaction between warfarin and cough drops, menthol, or peppermint; the search returned no results. However, there have been previously documented interactions between menthol or peppermint and other drugs. In one study of healthy female volunteers, the primary effect of a single 100-mg dose of menthol on caffeine pharmacokinetics was to slow absorption, probably by decreasing gastric emptying. However, it did not affect the AUC. 4
Studies have also demonstrated menthol's potential to affect the cytochrome P450 system by inducing and inhibiting enzymes. In one report, oral administration of L-menthol to rats (800 mg/kg/day) induced CYP450 enzymes. 5 A further study of the effects of several terpenoid compounds (menthol and related compounds) on CYP450 levels found that menthol induced the CYP2B subfamily after in vivo treatment of rats with menthol 40 mg/kg/day for 3 days. 6
However, other studies have shown menthol to have the opposite effect, inhibiting CYP450 enzymes. De-Olivera et al. 7 showed inhibition of CYP2B1 and CYP1A2 enzymes by menthol in rats. Peppermint oil, the major constituent of which is menthol, was reported to inhibit CYP3A4 activity in rats and humans and enhance the oral bioavailability of felodipine.8,9
Research does not consistently show menthol to be an enzyme inhibitor or inducer, but does demonstrate that menthol has the potential to produce clinically meaningful effects on drug concentrations affected by CYP450 metabolism.
Another cause of decreased INR is increased vitamin K intake. Because menthol is derived from the peppermint plant, it is possible that it could contain vitamin K, although no documentation was found to support or refute this hypothesis.
It is not clear whether any or all of these potential mechanisms could have played a role in this case. We present them to emphasize that there are several plausible mechanisms by which menthol could affect warfarin therapy.
Conclusions
This case is the first known report of a possible interaction between warfarin and menthol cough drops. By an unknown mechanism, the cough drops seemed to decrease the anticoagulant effect of warfarin. Patients using cough drops containing menthol should be monitored closely for changes in INR. To better understand the significance of this interaction, controlled studies should be performed in animals and/or humans.