
Abstract
OBJECTIVE:
To report a case of sulfhemoglobinemia in a patient receiving phenazopyridine for a urinary tract infection.
CASE SUMMARY:
A 63-year-old white woman presented to the emergency department with complaints of fatigue and bluish discoloration of her body that had gradually progressed over the previous 6–8 weeks. About 4 months prior to presenting to the emergency department, she had started taking phenazopyridine, an over-the-counter medication for symptoms of dysuria. Because the cyanosis did not improve after the patient received oxygen and methylene blue, sulfhemoglobinemia was suspected and confirmed by spectrophotometer analysis.
DISCUSSION:
Sulfhemoglobin is a green-pigmented molecule containing a sulfur atom in one or more of the porphyrin rings. It is a rare cause of cyanosis, which is usually drug induced. Sulfhemoglobinemia is suspected when a cyanotic patient has normal to near-normal oxygen tension, laboratory reports of elevated methemoglobin, and does not respond to methylene blue therapy. Sulfhemoglobinemia is relatively rare, despite the widespread use of drugs that have been reported to cause it. Predisposing factors, such as chronic constipation, present in our patient, have been suggested as a source of hydrogen sulfide.
CONCLUSIONS:
This case of sulfhemoglobinemia, which occurred after the patient took phenazopyridine, is considered a probable adverse event according to the Naranjo probability scale.
Sulfhemoglobin is a green-pigmented molecule containing a sulfur atom in one or more of the porphyrin rings. It is a rare cause of cyanosis, which is usually drug induced. 1 Evaluation of a patient with cyanosis normally includes assessment of cardiac and pulmonary conditions; however, dyshemoglobinemic states, such as methemoglobinemia and sulfhemoglobinemia, can be responsible for bluish discoloration of skin and should be considered in the differential. Dyshemoglobinemia results in a bluish discoloration of skin due to the hemoglobin altered visible spectra. These altered hemes have reduced oxygen affinity, resulting in physiologic effects of anemia. Most of the chemical agents that cause methemoglobinemia can also cause sulfhemoglobinemia. In addition, medications have been associated with both of these conditions, although much more rarely with sulfhemoglobinemia. Sulfhemoglobinemia is suspected when a cyanotic patient has normal to near-normal oxygen tension, laboratory reports of elevated methemoglobin, and does not respond to methylene blue therapy. 2
We report the case of a patient with sulfhemoglobinemia caused by the commonly used over-the-counter medication phenazopyridine. This patient had severe symptomatic anemia due to oxidant chemical stress and hemolysis. Clinical aspects in the evaluation of sulfhemoglobinemia are reviewed briefly.
Case Report
A 63-year-old white woman presented to the emergency department with complaints of fatigue and bluish discoloration of her body that had gradually progressed over the previous 6–8 weeks. She reported additional symptoms of lightheadedness, dyspnea with minimal exertion, epigastric discomfort, and constipation. Her medical history included peptic ulcer disease and anxiety disorder for which she took, respectively, ranitidine 150 mg at bedtime and alprazolam 1 mg 3 times a day for the last 10 years. About 4 months prior to presenting to the emergency department, she had started taking phenazopyridine 100 mg 3 times a day for symptoms of dysuria. The patient denied experiencing fever or blood in the urine.
On examination, she appeared cyanotic, most prominently on her lips and extremities. Her vital signs were T 36.5 °C, HR 104 beats/min, BP 98/60 mm Hg, and RR 16 breaths/min. Cardiorespiratory examination was unremarkable. She had epigastric tenderness with hemoccult-negative stools. She was somnolent, with a nonfocal neurologic examination. Significant laboratory values included hemoglobin 8.6 g/dL, PaO2 75.4 mm Hg, pH 7.42, and O2 saturation 80% while breathing room air. No improvement in cyanosis was noted with addition of 100% oxygen. She was treated with 2 doses of methylene blue 1 mg/kg intravenously, with no improvement. Blood oximetry (Radiometer ABL520) revealed a methemoglobin concentration of 17.1%. Repeat analysis 3 hours following methylene blue administration showed no change in methemoglobin levels. Possible causes of failure of methylene blue therapy were discussed.
The peripheral blood smear showed anisocytosis, polychromasia, eosinophilia, and no identifiable Heinz bodies or fragmented cells. The patient's blood sample was sent to an outside laboratory for sulfhemoglobin analysis. In addition, serum glucose-6-phosphate dehydrogenase and NADPH methemoglobin reductase levels were measured. Results of analysis by spectrophotometer (DU 7500) showed sulfhemoglobin levels to be 17.9%. Methemoglobin reductase level was 12.8 IU/g of hemoglobin and glucose-6-phosphate dehydrogenase level was 6.9 units/g of hemoglobin, both within normal limits. The patient's hemoglobin dropped to 7.6 g/dL, with worsening fatigue and abdominal discomfort following methylene blue administration. She received a transfusion of 2 units of packed red blood cells. The patient reported clinical improvement of her symptoms. Eight weeks later, her cyanosis had improved and sulfhemoglobin levels had decreased to 4%, with no further drop in hemoglobin. Her anemia was determined to be due to hemolysis, with a corrected reticulocyte count of 298.2 × 103/mm3 (6.6%) and reduced haptoglobin (12 mg/dL).
Discussion
Our patient was cyanotic, with near-normal arterial oxygen tension, and the pulse-oximetry desaturation suggesting the possibility of an abnormal hemoglobin species as the cause. Furthermore, the lack of response to methylene blue administration raised the suspicion of sulfhemoglobinemia.
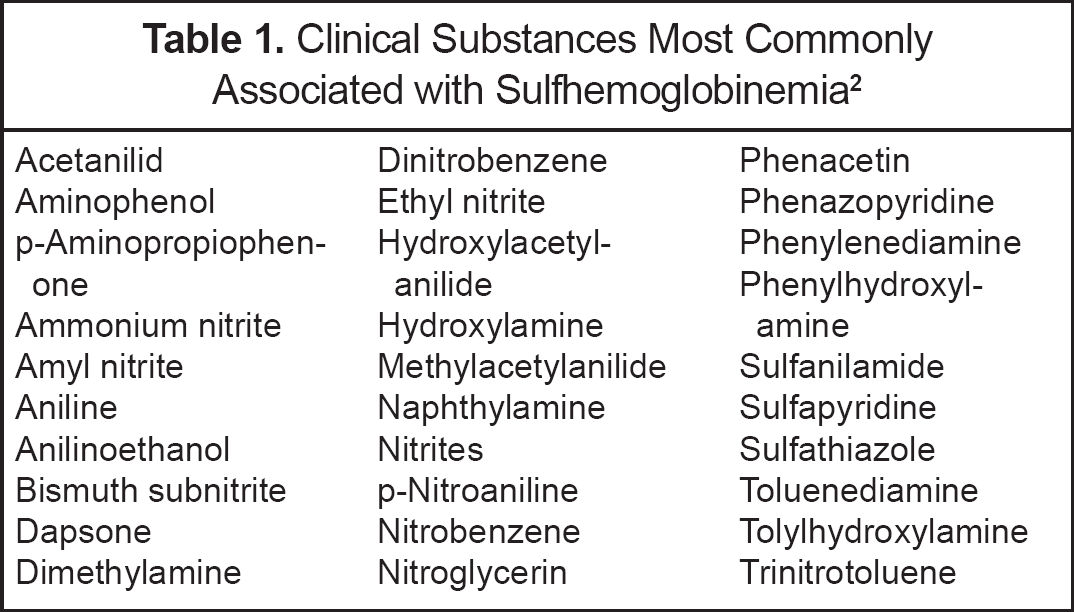
Sulfhemoglobinemia is a rare cause of cyanosis, often drug induced. Many of the responsible drugs are similar to those that induce methemoglobinemia (Table 1) 2 ; it is important to note that these agents do not need to contain sulfur. The reason why drugs with oxidant potential produce methemoglobin in some individuals and sulfhemoglobin in others is unknown. Because sulfhemoglobinemia is relatively uncommon despite the widespread use of drugs with which it is associated, predisposing factors such as chronic constipation, which was seen in our patient, have been suggested as sources of hydrogen sulfide. 1
Clinical Substances Most Commonly Associated with Sulfhemoglobinemia 2
Clinically, sulfhemoglobinemia is usually a benign disorder despite often being associated with intense cyanosis. Only 0.5 g/dL of sulfhemoglobin is sufficient to produce cyanosis equivalent to that produced by 1.5 g/dL of methemoglobin. 3 Symptoms related to hypoxia in a patient with sulfhemoglobinemia are rare. This is explained by a decrease in the oxygen affinity of heme that is not sulfinated. This change facilitates tissue oxygenation by functional hemoglobin units. Thus, patients take medications for longer periods of time without significant symptomatology. The coexistence of anemia may also alter the severity of symptoms. 2
Phenazopyridine is an azo dye agent that has phenazopyridine as its active ingredient. When prescribed, it is frequently used as an adjunct to antibacterial therapy and helps to relieve the pain and discomfort associated with urinary tract infections. The exact mechanism of action is unknown; however, phenazopyridine exerts its analgesic effects primarily topically on the urinary tract mucosa. 4 This topical effect results in the symptomatic relief of burning, urgency, frequency, and pain that commonly accompanies a urinary tract infection. The usual adult dose is 200 mg 3 times a day orally after meals, for a maximum of 2 days following onset of symptoms. Our patient took the medication for approximately 4 months without medical supervision. Some of the adverse effects can be hematologic (eg, anemia, methemoglobinemia, neutropenia, sulfhemoglobinemia, thrombocytopenia), central nervous system—related (eg, headache), gastrointestinal (eg, nausea, vomiting, diarrhea), renal (eg, nephrotoxicity, discoloration of the urine, nephrolithiasis), and hepatic (eg, hepatitis, abnormal liver function tests). 4 The majority of the unwarranted adverse effects are rare, but they still have the potential to occur. Phenazopyridine is more commonly associated with methemoglobinemia; however, the aniline metabolites of phenazopyridine can cause sulfhemoglobinemia. Hemolytic anemia caused by both normal and high doses of phenazopyridine has also been reported. 3
The co-oximeters used can measure the presence of 4 different hemoglobin species—carboxyhemoglobin, methemoglobin, deoxyhemoglobin, and oxyhemoglobin. Having a fifth hemoglobin species present, such as sulfhemoglobin, may cause a false-positive result for methemoglobin. This occurs due to similar spectral absorbances of methemoglobin and sulfhemoglobin. 5 Significant absorbances at a wavelength of 660 nm have been associated with spurious pulse-oximetry readings. 6 In our patient, hemolysis and the resultant anemia may have affected readings of pulse oximetry.
Diagnosis is confirmed by hemoglobin electrophoresis with isoelectric focusing. 7 It is more challenging to quantify sulfhemoglobin, as its measurement requires spectrophotometry analysis or gas chromatography that may not be readily available. 8 Treatment of sulfhemoglobinemia includes supportive care, although blood/exchange transfusions may be required for severe toxicity. 7 It is not reduced by treatment with methylene blue and remains in the red blood cell for the duration of its life span. 9
To date, only 2 other cases of sulfhemoglobinemia caused by phenazopyridine have been published. In another similar clinical setting, phenazopyridine was prescribed to an 84-year-old woman for a recent urinary tract infection. 10 The patient reported receiving a normal dose of 100 mg 4 times a day. The patient was diagnosed with sulfhemoglobinemia and was discharged from the hospital 9 days later. She was diagnosed with bacteruria 9 months after her previous urinary tract infection and inadvertently received phenazopyridine again. The patient was admitted to the hospital after taking this medication for one week and was diagnosed with sulfhemoglobinemia resulting from the inadvertent rechallenge of phenazopyridine. She was discharged from the hospital 13 days later. A second case of phenazopyridine-induced sulfhemoglobinemia involved a 57-year-old woman who reported taking phenazopyridine for several years. 11 The patient improved after 7 days and was discharged with no further sequelae.
Conclusions
Sulfhemoglobinemia is a rare cause of cyanosis and is most commonly drug induced. In our patient, none of the other medications were known to be associated with this complication. According to the Naranjo probability scale, this unwarranted sulfhemoglobinemia reaction ranked as a probable adverse event. 12 It should be reiterated that phenazopyridine is a widely used over-the-counter medication, and it is important to educate patients about the adverse effects of using such drugs over unusually long periods of time, especially without medical supervision.