
Abstract
OBJECTIVE
To review the safety and efficacy of a once-daily dosage regimen for abacavir, a nucleoside reverse transcriptase inhibitor.
DATA SOURCES
English-language MEDLINE and Iowa Drug Information Service database reports were accessed from 1966 to March 2005. International Pharmaceutical Abstracts was searched from 1970 to March 2005. The key words used in all searches were abacavir and Ziagen. Article bibliographies were used to identify additional relevant articles. The Internet was searched to identify abstracts of poster and oral presentations that have not yet been published. The manufacturer was also contacted to obtain unpublished information.
STUDY SELECTION AND DATA EXTRACTION
Publications were included that provided information related to the safety and efficacy of abacavir when used once daily. Preference was given to randomized, double-blind, controlled trials comparing once-daily abacavir regimens with other antiretroviral regimens. Abstracts from professional meetings were included for unpublished studies, and conference coverage reviews were included if the abstracts were not available.
DATA SYNTHESIS
In trials directly comparing once- and twice-daily abacavir, little difference was shown in the efficacy of the 2 regimens. Despite similar adverse effect profiles, significantly more severe hypersensitivity reactions and severe diarrhea were seen with once-daily abacavir in one trial.
CONCLUSIONS
Once-daily administration of abacavir has not been shown to be inferior to twice-daily dosing, but it may put patients at increased risk for severe hypersensitivity reactions and diarrhea. More data are needed to confirm this risk.
Abacavir is a synthetic carbocyclic nucleoside reverse transcriptase inhibitor (NRTI) that is converted intracellularly to carbovir triphosphate (CBV-TP). 1 CBV-TP inhibits reverse transcriptase by acting as a competing substrate that is incorporated into viral DNA. This prohibits growth of the DNA chain and suppresses viral replication.
Because some HIV strains are unresponsive to certain drugs and HIV has the potential to mutate into resistant strains, it is necessary to use at least 3 antiretrovirals concurrently. 2 The Panel on Clinical Practices for Treatment of HIV Infection periodically updates its treatment guidelines for adults. 3 Despite its initial acclaim as a potent antiretroviral, abacavir remains an alternative therapy as part of a nucleoside backbone. 4 Triple nucleoside regimens are not recommended by the panel unless preferred therapies cannot or should not be used. 3 If one must be used, abacavir plus tenofovir and lamivudine should be avoided because of high potential for early virologic failure. However, there is still a triple nucleoside option that includes abacavir, so it has not been excluded completely from this use.
Adherence to HIV therapy is important 5 ; however, multiple daily dosing and substantial pill burden of antiretroviral therapy make adherence difficult. Experience with other chronic conditions has shown that simplified dosing regimens improve adherence, contributing to the growing popularity of once-daily antiretroviral regimens. Abacavir was approved by the Food and Drug Administration (FDA) for twice-daily use >6 years ago, but in August 2004, the FDA approved once-daily abacavir for adults. 6 A combination tablet of abacavir 600 mg and lamivudine 300 mg was approved the same day. 7 Nevertheless, once-daily abacavir must prove it is not inferior to twice-daily administration. The purpose of this review is to examine the literature comparing the efficacy and safety of once- versus twice-daily abacavir.
Data Sources
English-language literature was retrieved from MEDLINE, Iowa Drug Information Service (IDIS)/Web, and International Pharmaceutical Abstracts. MEDLINE and IDIS/Web were searched from 1966 to March 2005; International Pharmaceutical Abstracts was searched from 1970 to March 2005. The key words used in all searches were abacavir and Ziagen. Bibliographies of the relevant articles were also searched. Unpublished data from abstracts presented at professional meetings were included, and the manufacturer was contacted to obtain unpublished information regarding once-daily dosing of abacavir.
Articles were included that provided information related to the safety, efficacy, and pharmacokinetics of abacavir when used once daily. Literature that dealt solely with twice-daily dosing was not included. Preference was given to randomized controlled trials comparing the once- and twice-daily regimens. Uncontrolled studies were included if no comparative trials existed.
The criteria for assessing efficacy included achieving treatment goals and avoiding treatment failure. The goals of treatment in antiretroviral-naïve HIV-infected patients are to (1) maximize viral suppression, (2) restore and preserve immune function, (3) reduce HIV morbidity and mortality, and (4) improve quality of life. Viral load and CD4+ cell count are surrogate markers of treatment efficacy. A major goal of therapy is suppression of HIV-RNA to undetectable levels (<50 copies/mL) in 16–24 weeks. Adequate viral suppression causes the CD4+ cell count to rise 100–150 cells/mm 3 from baseline during the first year of treatment and 100 cells/mm3 per year after that to a threshold level. 3 Treatment failure is a suboptimal response to therapy. Virologic failure is characterized as (1) HIV-RNA >400 copies/mL after 24 weeks of treatment, (2) HIV-RNA >50 copies/mL after 48 weeks of treatment, or (3) detection of HIV-RNA after suppression to undetectable levels. Immune failure is characterized as a CD4+ cell count increase <25–50 cells/mm3 from baseline after one year of treatment or CD4+ cell count below baseline. Clinical progression is characterized by the occurrence of HIV-related events after at least 3 months of treatment.
Pharmacokinetics
Abacavir 300 and 600 mg have a bioavailability of 83%. 8 A study of twice-daily abacavir showed the mean terminal half-life to be 2.6 hours (95% CI 2.0 to 3.3).9,10 However, the half-life values of its CBV-TP metabolite in peripheral blood mononuclear cells were 20.6 hours (95% CI 16.34 to 26.0)9,10 and 12–19 hours. 11 Intracellular CBV-TP levels were detectable for at least 48 hours, suggesting a potential for once-daily administration. The only study comparing once- and twice-daily abacavir was done in pediatric patients (median age 5.6 y) in the Paediatric European Network for Treatment of AIDS 13. 12 Once-daily abacavir administration increased the AUC by 35% (90% CI 19% to 54%) and decreased clearance by 27% (90% CI 16% to 36%). The authors did not speculate as to why there may be a delayed clearance with a greater exposure to the drug, but concluded that once-daily use is feasible. Based on this and other 12-week efficacy studies, it is suggested that therapeutic equivalency trials be conducted. Analysis by age (2–6 and 6–13 y) was unable to detect a difference between the pharmacokinetics of the drug in these subgroups. No pharmacokinetic studies of once- or twice-daily dosing have been conducted in patients >65 years old.
Clinical Studies
The failure of once-daily administration of tenofovir, abacavir, and lamivudine in clinical trials raised suspicion that this dosing of abacavir might be inadequate. 4 Three studies compared the safety and efficacy of once- and twice-daily abacavir. CNA300211,13–19 and ESS3000820–22 assessed once-daily abacavir's fitness as part of a nucleoside backbone, and EPV4000114,23 evaluated once-daily abacavir as the foundation for a triple nucleoside regimen. Other studies investigated new roles for abacavir while comparing the dosing regimens. CAL3000124,25 and Ruane et al. 26 compared once- and twice-daily abacavir in 4-drug regimens for which there are no current recommendations (Table 1).
Efficacy Trials of Once- Compared with Twice-Daily Abacavir
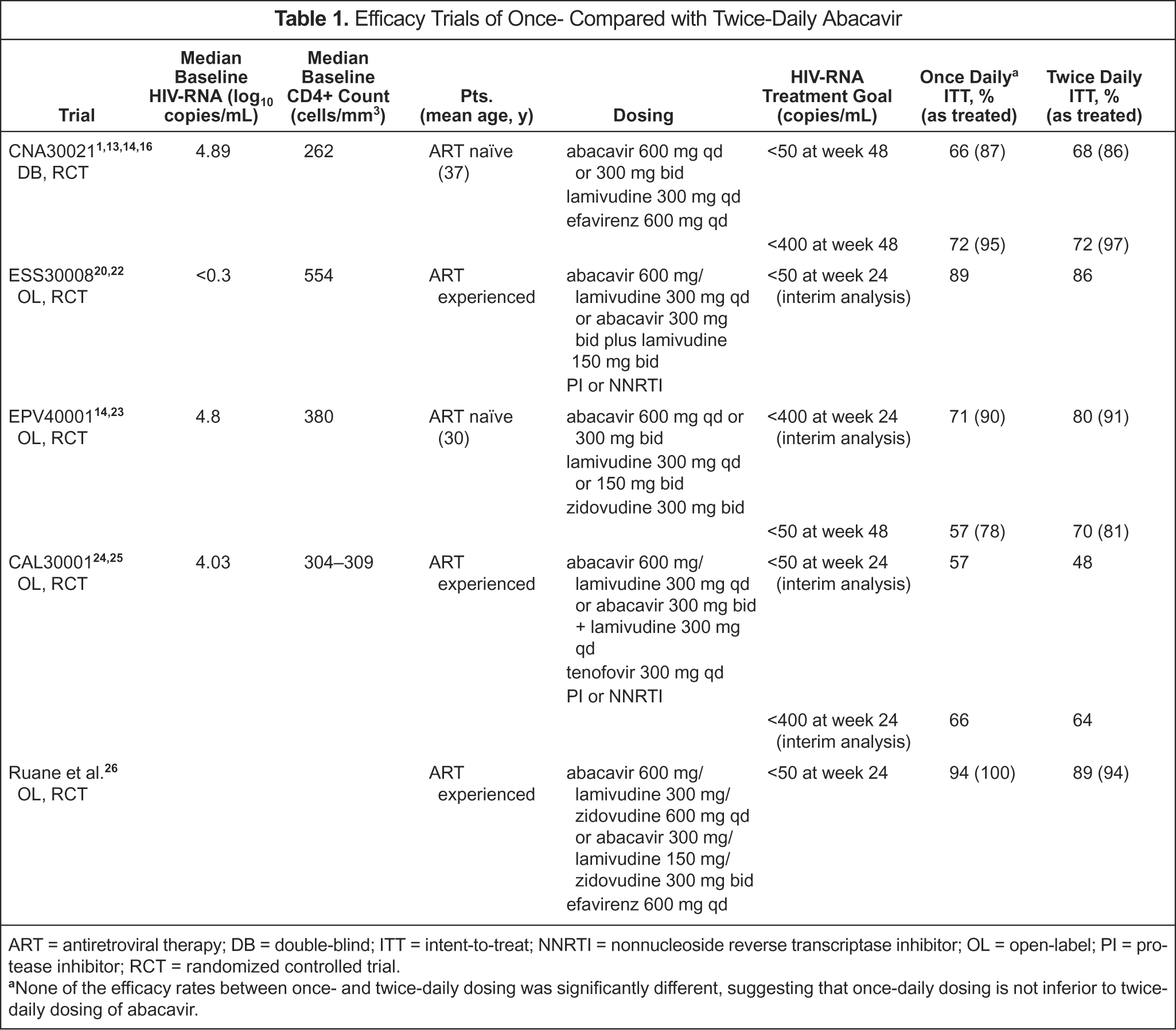
ART = antiretroviral therapy; DB = double-blind; ITT = intent-to-treat; NNRTI = nonnucleoside reverse transcriptase inhibitor; OL = open-label; PI = protease inhibitor; RCT = randomized controlled trial.
None of the efficacy rates between once- and twice-daily dosing was significantly different, suggesting that once-daily dosing is not inferior to twice-daily dosing of abacavir.
NUCLEOSIDE BACKBONE
Abacavir is an option as an alternative component of the nucleoside backbone in therapy. However, it is not preferred because of its potential to cause hypersensitivity reactions. 3
CNA30021
The results of CNA30021, also known as the ZODIAC (Ziagen Once Daily in Antiretroviral Combination) study, were submitted to the FDA for approval of once-daily abacavir.1,13–16 This trial compared virologic response to the differing dosing schedules of abacavir in 770 HIV-infected adults for at least 48 weeks. The primary endpoint was defined as suppression of HIV-RNA viral load to a level undetected by ultrasensitive assay (<50 copies/mL) at week 48. Virologic response was similar in both groups. The investigators used intent-to-treat (ITT) analysis of only patients who had actually initiated therapy (ITT exposed). In this analysis, the 95% confidence interval for the difference between once- and twice-daily abacavir was −8.4% to 4.9%. Based on a noninferiority margin of 12%, the authors concluded that the efficacy of once-daily dosing was not inferior to that of twice-daily dosing. The median increase in CD4+ cell count from baseline was similar in the 2 arms (188 vs 200 cells/mm3, respectively).
Virologic failure, defined as failure to achieve or rebound above undetectable levels, occurred in 10% of patients on once-daily treatment and 8% on twice-daily abacavir in the ITT exposed analysis. Fewer than half of these patients were examined for HIV mutations. Baseline mutations were higher in the once-daily arm (18% vs 6%), but the incidence of emergent mutations was similar between the 2 groups. The M184V mutation, which has been associated with abacavir use, developed in 10 once-daily patients and 5 twice-daily patients, but this was not significantly different. 4
ESS30008
The ESS30008 trial enrolled HIV-infected adults who had been on abacavir and lamivudine twice daily plus a protease inhibitor (PI) or nonnucleoside reverse transcriptase inhibitor (NNRTI) for at least 6 months and had an HIV-RNA level <400 copies/mL for at least 3 months.20–22 The subjects continued their treatment (n = 130) or switched to combination abacavir/lamivudine once daily (n = 130). At baseline, the patients had been on abacavir plus lamivudine twice daily for a median of 22 months. One objective of this open-label study was to compare the efficacy of the 2 regimens. The primary endpoint was the proportion of patients who did not meet criteria for virologic failure (confirmed HIV-RNA ≥1265 copies/mL).
In a planned interim analysis at 24 weeks, the once-daily regimen was reported to be non-inferior to the twice-daily regimen based on viral suppression (90% CI–8% to 1.8%).20,21 However, the predetermined limit for non-inferiority was not disclosed. Virologic failure occurred in 1.5% of the subjects in each group. Overall, the median adherence determined by pill count was found to be 94%. The percentage of patients in the once-daily group that took at least 95% of their doses was higher than in the twice-daily group (44% vs 36%, respectively).
The final analysis after 48 weeks yielded results similar to those of the interim analysis. 22 The percentage of patients whose HIV-RNA measured <1265 copies/mL was 95% in the once-daily group, compared with 93% in the twice-daily group. The 1.5% difference (90% CI −3.4% to 6.4%) fell above the non-inferiority limit of −12%. Median adherence in both groups was 93%. The percentage of patients who took at least 95% of their doses remained slightly higher in the once-daily group (39% vs 31%).
The other objective of this study was to compare patient satisfaction with the 2 regimens.20,21 At baseline, subjects completed the HIV Treatment Satisfaction Questionnaire (HIVTSQ), and no significant difference was detected between the groups. The HIVTSQ change version (HIVTSQc) assesses satisfaction in relation to baseline. When scores on the HIVTSQc were compared during the interim analysis at 24 weeks, no significant difference was detected, despite greater increased satisfaction overall with the once-daily regimen.
Triple Nucleoside Regimen
Abacavir can be part of a triple nucleoside regimen, but these regimens are to be used only if PI- or NNRTI-based therapies have been ruled out. This is because of reduced potency and potential for virologic failure. 3
EPV40001
Study EPV40001 compared the safety and efficacy of once- and twice-daily abacavir administration in a triple nucleoside regimen over 48 weeks.14,23 The researchers also wanted to compare once- and twice-daily lamivudine. They randomized 151 HIV-1 infected adults to 1 of 3 arms: abacavir, lamivudine, and zidovudine twice daily; abacavir once daily plus lamivudine and zidovudine twice daily; or lamivudine once daily plus abacavir and zidovudine twice daily. The primary objective was to compare the median HIV-RNA change from baseline between groups. In this trial, once-daily abacavir therapy would not be considered inferior to twice-daily dosing if the upper limit of the 95% confidence interval for the difference between treatments was <0.4 log
The investigators assessed the results in a planned 24-week interim analysis and at the end of the study using an ITT exposed analysis.14,23 Switching from randomized therapy to another therapy meant the patient would be considered a treatment failure in this analysis. The difference between treatments at 48 weeks was 0.14 log
The results after 24 and 48 weeks suggested that abacavir administered once daily was not inferior to twice daily, but the power calculation for the primary endpoint was not given.14,23 Therefore, it cannot be said with certainty that once-daily treatment is not inferior. The study may not have had the power to detect a difference between the 2 therapies.
EMERGING THERAPIES
Current recommendations from the panel do not include 4-drug regimens because there is not yet enough evidence to support these combinations. 3 The 4-drug abacavir regimens that have been studied contain 3 NRTIs plus a PI or NNRTI.
CAL30001
CAL30001 compared the safety, efficacy, and virology of combination abacavir/lamivudine once daily in 94 adults with abacavir twice daily plus lamivudine once daily in 88 adults.24,25 All patients received tenofovir and a new PI or NNRTI. To be included, patients had to have received 2 NRTIs and a PI, NNRTI, or NRTI, not including tenofovir, prior to enrollment. An HIV-RNA >1000 copies/mL and no K65R, L74V, or MDR NRTI-associated mutations were also required.
Non-inferiority was assessed using viral load reduction based on the starting viral load level.24,25 Baseline HIV-RNA was significantly greater in the twice-daily arm (3.92 vs 4.22 log
More subjects in the once-daily group were prescribed an NNRTI as their fourth drug (45% vs 34%), but more NNRTI subjects experienced virologic failure.24,25 Virologic failure, defined as failure to achieve or loss of viral suppression <400 copies/mL, occurred in 16% (15/94) subjects on once-daily and 15% (13/88) on twice-daily treatment. Baseline presence of M184V/I in virologic failures was 73% and 54%, respectively. Most subjects were analyzed for new HIV mutations, and the rates of emergent mutations, including the K65R mutation also associated with abacavir, were similar between the groups. 4 Four subjects in each group developed reduced susceptibility to abacavir.
The authors reported that once-daily abacavir/lamivudine was not inferior to abacavir twice daily plus lamivudine once daily at the 24-week interim analysis. However, they did not identify the predetermined limit for non-inferiority. Virologic failure and resistance were similar in both groups.
Ruane et al.
Ruane et al. 26 undertook a small trial to assess the feasibility of dosing combination abacavir/lamivudine/zidovudine once daily in addition to efavirenz once daily. Patients already receiving the triple combination twice daily with efavirenz once daily were randomized to either continue treatment or switch to the entire regimen once daily. To be included in the study, patients were required to have an HIV-RNA count <50 copies/mL for at least 3 months. When the 24-week study ended, 36 subjects had been randomized. No significant difference was detected between the percentage of patients who maintained undetectable levels in either group (p = 1.0). One subject in the once-daily arm had a confirmed viral load ≥120 copies/mL, meeting the definition for treatment failure. In this pilot study, a difference in efficacy between abacavir/lamivudine/zidovudine once or twice daily was not detected. A larger trial is required to support this finding.
Adverse Effects
Abacavir is known to be responsible for hypersensitivity reactions. These reactions have occurred in a small proportion (8%) of patients in clinical trials, but can become severe and life threatening. An abacavir hypersensitivity reaction is typically characterized by ≥2 of the following symptoms: (1) fever, (2) rash, (3) nausea, vomiting, or diarrhea, (4) malaise or fatigue, and (5) cough or sore throat. If these symptoms occur, abacavir should be discontinued. It should not be used again because, if restarted, the symptoms will recur and become life threatening rapidly.
It is important to identify whether patients taking abacavir once daily are at greater risk of hypersensitivity than those on twice-daily dosing. It is also important to determine whether the adverse effects commonly seen with twice-daily abacavir occur at a higher frequency with once-daily administration. Patients should be advised on the signs and symptoms of abacavir hypersensitivity and encouraged to see their physician immediately if such a reaction develops. They also should be counseled that the more common adverse effects of abacavir will generally improve over the initial weeks and months of treatment.
Adverse effects, such as nausea, dizziness, insomnia, and diarrhea, were similar in the abacavir once- and twice-daily arms of trial CNA30021.1,16,18,19 Subjects in the twice-daily group reported more fatigue (20% vs 15%); however, severe (grade 3 or 4) hypersensitivity reactions were seen with greater frequency in the once-daily arm. Severe diarrhea also occurred significantly more often in the abacavir once-daily group. Nonetheless, discontinuation rates due to adverse effects were similar between the 2 regimens. The differences in adverse effects are summarized in Table 2. For patients who remained in the study for >48 weeks, the incidence of grade 2–4 adverse effects after week 48 was 16% with once-daily and 17% with twice-daily dosing. 17 Serious adverse events occurred at the same rate (1%) in both groups.
Adverse Effects Through Week 48 in Trial CNA30021
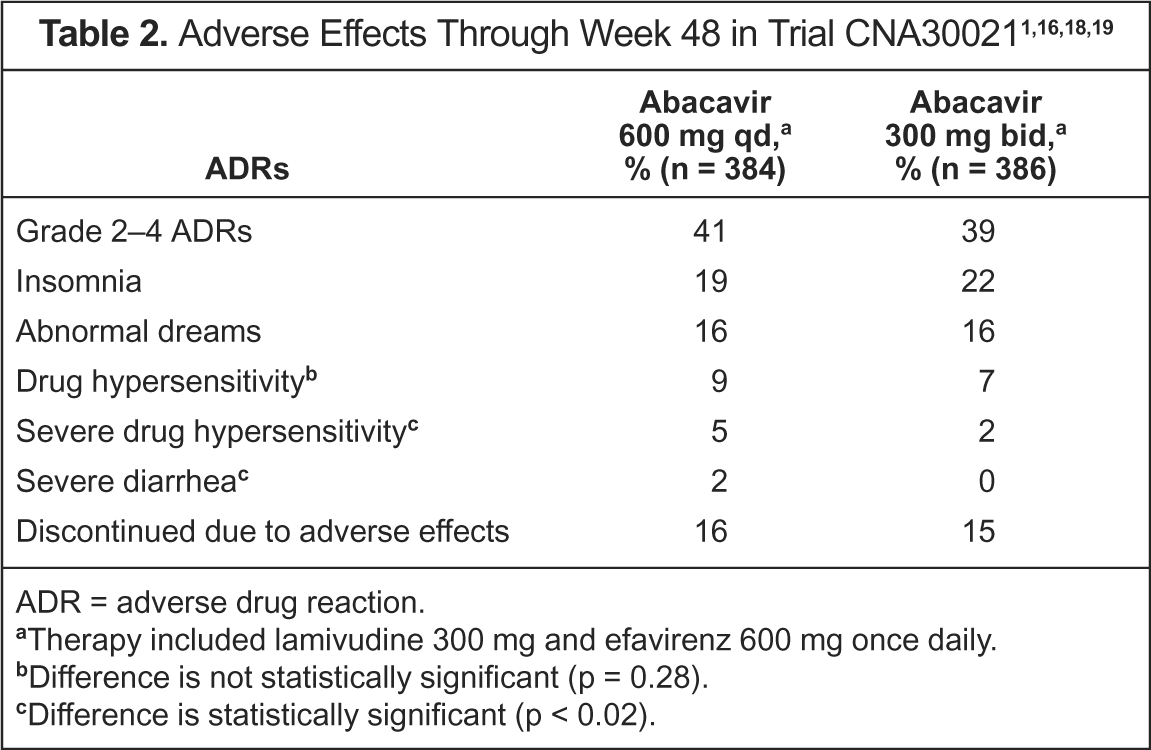
ADR = adverse drug reaction.
Therapy included lamivudine 300 mg and efavirenz 600 mg once daily.
Difference is not statistically significant (p = 0.28).
Difference is statistically significant (p < 0.02).
Grade 2–4 adverse effects in patients taking abacavir once daily were similar to those in patients on twice-daily regimens in study ESS30008.20,22 The most common adverse effects reported were upper respiratory infection, nasopharyngitis, nausea, and headache. No serious drug-related adverse events or hypersensitivity reactions occurred. EPV40001 reported more serious fatigue in the abacavir once-daily arm (4% vs 0%). 14 However, anemia was identified only in the abacavir twice-daily group (10% vs 0%). Other serious adverse effects, such as nausea, vomiting, and neutropenia, were similar between the groups. The rate of abacavir hypersensitivity was 8% in both groups.
The incidence of hypersensitivity reactions in CAL30001 was twice as high (9% vs 4%) in the once-daily group, but the difference was not statistically significant.24,25 Discontinuations due to adverse effects were also higher in the once-daily group (63% vs 24%). In the Ruane et al. 26 study, adverse effects were similar whether patients received once- or twice-daily dosing. None of the patients in that study withdrew due to adverse effects, nor were there any hypersensitivity reactions.
Brothers et al. 27 retrospectively compiled data on abacavir hypersensitivity reactions from 37 clinical trials enrolling 9330 patients. A subanalysis compared reactions in 1027 patients exposed to abacavir twice daily in 4 trials with those in 940 patients receiving the drug once daily in 4 trials. The difference between dosing in terms of grade 3/4 hypersensitivity reactions was not statistically significant. Limiting the usefulness of this study is the lack of blinded trials directly comparing the regimens. Only one of the trials was a double-blind, randomized comparison of once- and twice-daily abacavir (CNA30021). A second trial compared dosing but was open-label (CAL30001), and the other 4 did not compare the regimens.
Summary
Abacavir is approved for once-daily administration in adults and does not appear to be inferior to twice-daily dosing. The risk of severe hypersensitivity reactions and severe diarrhea was significantly greater with once-daily abacavir in the only double-blind, randomized, controlled trial comparing the 2 regimens. However, this risk was not seen in open-label comparison trials, so more evidence is needed to determine whether such a risk exists. In addition, there is no definitive way to identify patients at risk of hypersensitivity reactions short of administering the drug. Although once-daily regimens can improve adherence in HIV-infected individuals, as of May 24, 2005, there have been no conclusive data showing that patients are more adherent to once-daily abacavir therapy. At this time, the convenience of using once-daily abacavir is an advantage that must be weighed carefully against the potential risks.