
Abstract
BACKGROUND:
Toxicology screens obtained on patients who have overdosed on drugs frequently include tricyclic antidepressants (TCAs) as part of the evaluation. Quetiapine is an antipsychotic agent with structural similarity to the TCAs.
OBJECTIVE:
To determine whether quetiapine may cross-react with plasma TCA immunoassays in vitro using commonly available autoanalyzers.
METHODS:
Quetiapine stock solution was added to 9 separate samples of pooled drug-free human plasma to produce concentrations ranging from 1 to 640 ng/mL that were verified by gas chromatography. No quetiapine metabolites were present. Each spiked plasma sample was tested in a blinded fashion using the Abbott Tricyclic Antidepressant TDx Assay on the TDxFLx autoanalyzer in 2 separate laboratories, the Syva Emit tox Serum Tricyclic Antidepressant Assay on the AU400 autoanalyzer and the S TAD Serum Tricyclic Antidepressant Screen on the ACA-Star 300 autoanalyzer. The TDx assay is quantitative, while Emit and S TAD are qualitative screening assays with a threshold of 300 ng/mL for TCA positivity. The outcome of interest was a positive TCA result.
RESULTS:
The quantitative assay showed concentration-related TCA cross-reactivity beginning at quetiapine concentrations of 5 ng/mL. The 640-ng/mL spiked sample produced TCA results of 379 and 385 ng/mL in labs 1 and 2, respectively. The qualitative assays were screened as TCA positive at quetiapine concentrations of 160 and 320 ng/mL for the S TAD and Emit assays, respectively.
CONCLUSIONS:
Quetiapine cross-reacts with quantitative and qualitative plasma TCA immunoassays in a concentration-dependent fashion. Therapeutic use or overdose of quetiapine may result in a false-positive TCA immunoassay result.
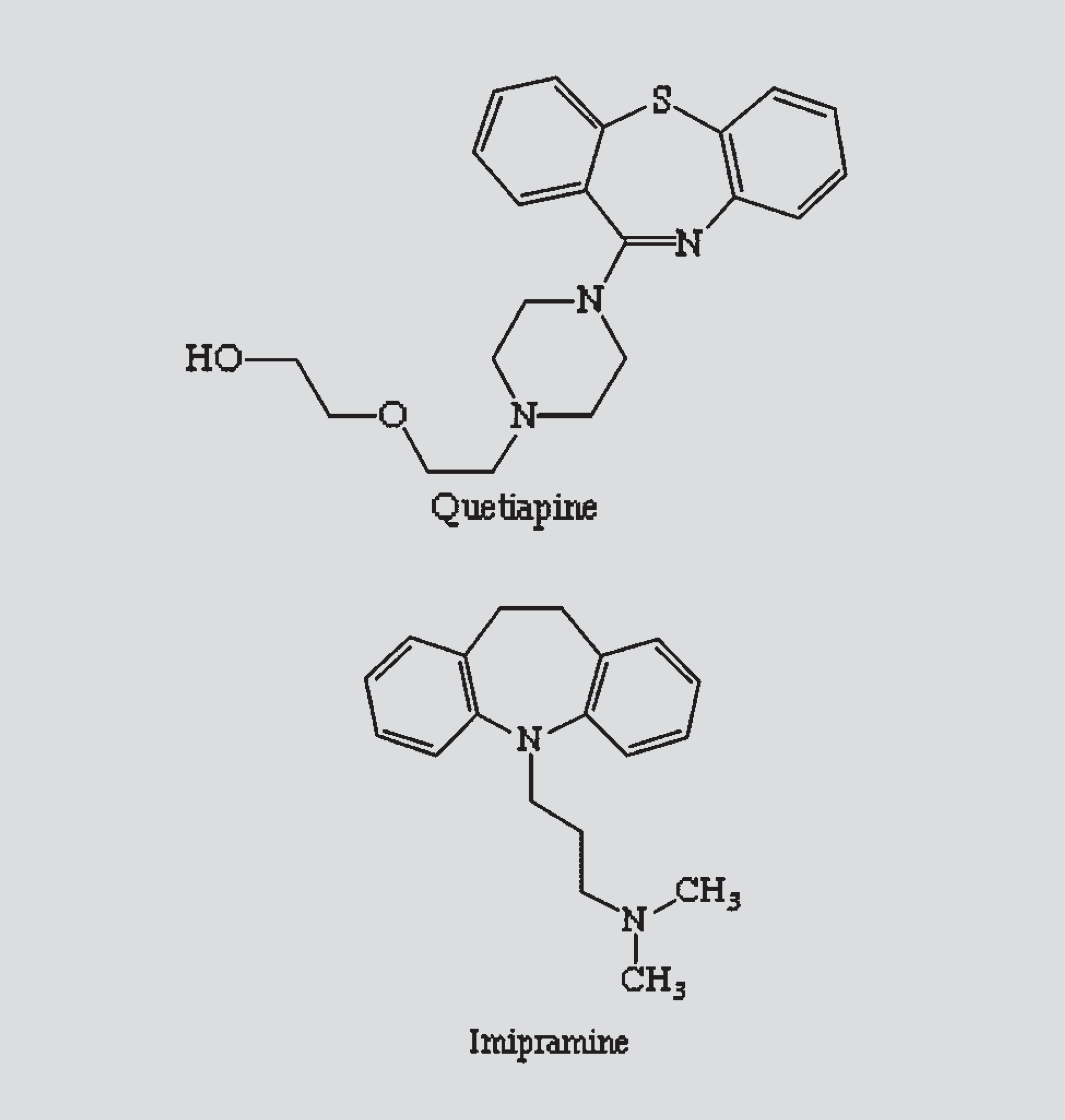
Chemical structures of quetiapine and imipramine
We investigated the potential for quetiapine to yield a false-positive result by plasma TCA immunoassay. The objective was to determine the degree to which quetiapine in therapeutic and supratherapeutic plasma concentrations may cross-react with quantitative and qualitative plasma TCA immunoassays in vitro using commonly available autoanalyzers.
Methods
This was a blinded, in vitro laboratory investigation using pooled, drug-free human plasma samples spiked with known quetiapine concentrations and a control sample without quetiapine. The study took place at university medical center—affiliated toxicology laboratories.
PROTOCOL AND MEASUREMENTS
Pooled drug-free human plasma was obtained from the blood bank on samples about to expire. The plasma was verified to be drug-free prior to use by gas chromatography (GC)—mass spectrometry (MS) and high-performance liquid chromatography (HPLC)—MS screening analysis for >70 therapeutic drugs and all common drugs of abuse. A quetiapine stock solution was made by one of the investigators (JMJ) by crushing a 25—g quetiapine tablet and dissolving it in HPLC-grade methanol to yield a quetiapine concentration of 1 μg/μL. The appropriate volume of quetiapine solution was added to 9 separate 10-mL samples of plasma to yield quetiapine concentrations ranging from 1 to 640 ng/mL. The spiked samples were allowed to rock for 2 hours. All quetiapine sample concentrations were independently verified by GC using the 1-μg/μL methanolic stock standard. No quetiapine metabolites were present. Pooled drug-free plasma without quetiapine were used as a control.
Each spiked sample and the control were labeled with a code number and analyzed by laboratory technicians according to standard laboratory testing procedures for patient samples. The technicians were blinded to the study hypothesis and sample contents. Each spiked sample was tested twice using the Tricyclic Antidepressant TDx Assay (Abbott Laboratories, Abbott Park, IL), a fluorescence polarization immunoassay, on the TDxFLx autoanalyzer (Abbott Laboratories) in 2 separate laboratories (lab 1 and lab 2%) for quantitative results. The analyzer reports the average of the 2 measurements as the final result. Imipramine is used as the calibrator drug, and the TCA results are reported as imipramine equivalents. The detection range of TCAs for the TDx assay was 20–1000 ng/mL.
The 9 samples were also tested once each using the Syva Emit tox Serum Tricyclic Antidepressant Assay (Dade Behring, Deerfield, IL) on the AU400 (Olympus, Hamburg, Germany) and the S TAD Serum Tricyclic Antidepressant Screen (Dupont, Wilmington, DE) on the ACA-Star 300 (Dupont) autoanalyzers for qualitative results. The Emit and S TAD assays are qualitative TCA screening assays with a threshold of 300 ng/mL for positivity. Values <300 ng/mL are deemed negative outcomes.
DATA ANALYSIS
The primary analysis of data was descriptive, with the outcomes of interest being the number of spiked samples that tested positive with each qualitative assay and the numerical TCA results from the quantitative assay. Linear regression analysis was performed on the quantitative results to determine whether there was a concentration-related cross-reactivity.
This in vitro laboratory investigation did not involve human subjects and was deemed exempt by the investigational review board.
Results
The quantitative immunoassay (TDx) showed concentration-related TCA cross-reactivity beginning at quetiapine concentrations of 5 ng/mL and increased with each subsequent sample (Table 1, Figure 2). This concentration-related cross-reactivity was demonstrated in both labs (lab 1, y = 0.56X + 47.8, r 2 = 0.961; lab 2, y = 0.55X + 58.1, r 2 = 0.955%). The quantitative values were slightly higher for each sample analyzed in lab 2 compared with lab 1, but did not differ by a clinically relevant amount (Table 1). The 640-ng/mL spiked quetiapine sample produced TCA results of 379 and 385 ng/mL in labs 1 and 2, respectively.
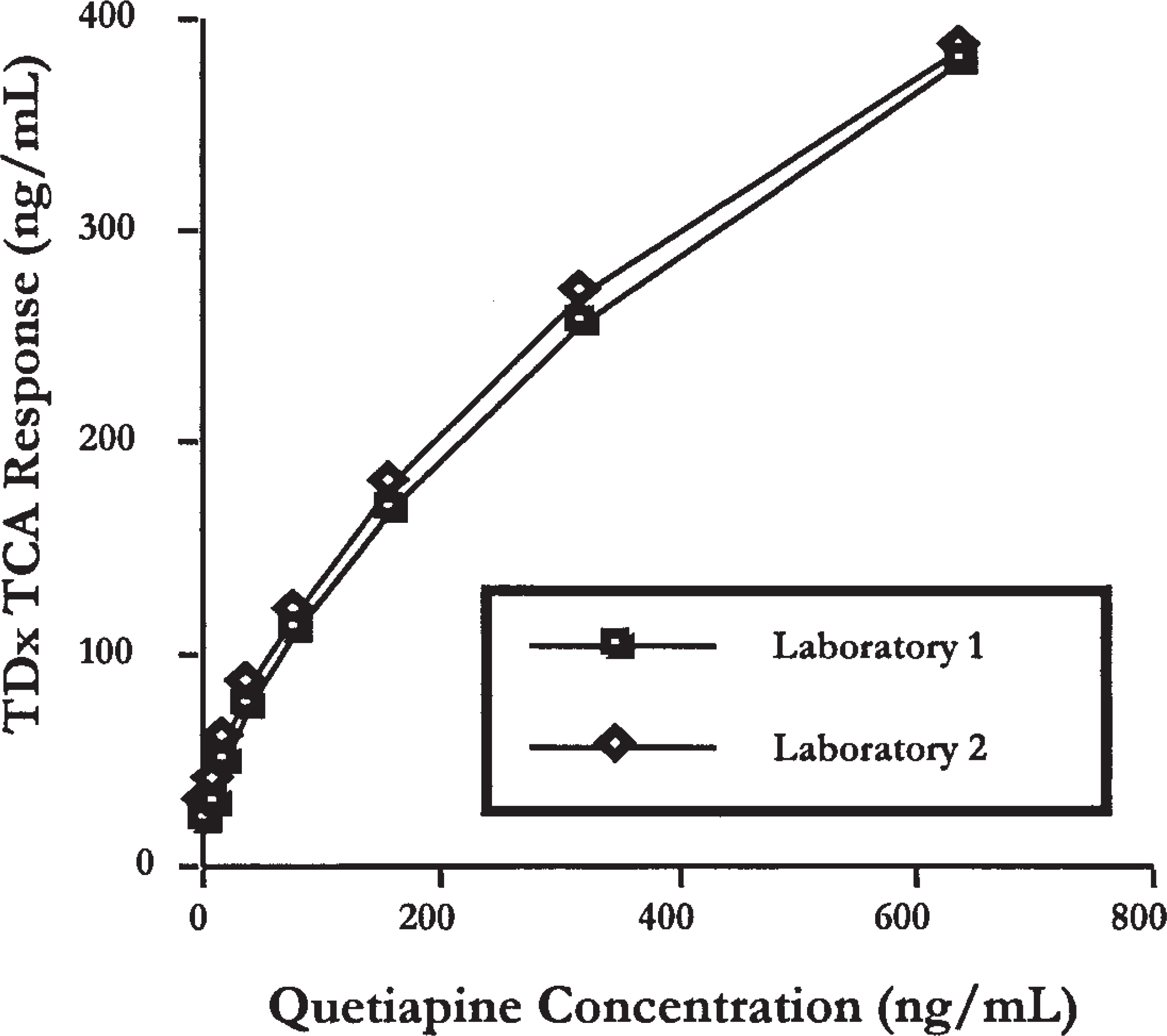
Comparison of quetiapine concentrations and tricyclic antidepressant (TCA) TDx Response
Cross-Reactivity of Quetiapine-Spiked Plasma Samples with TCA Assays
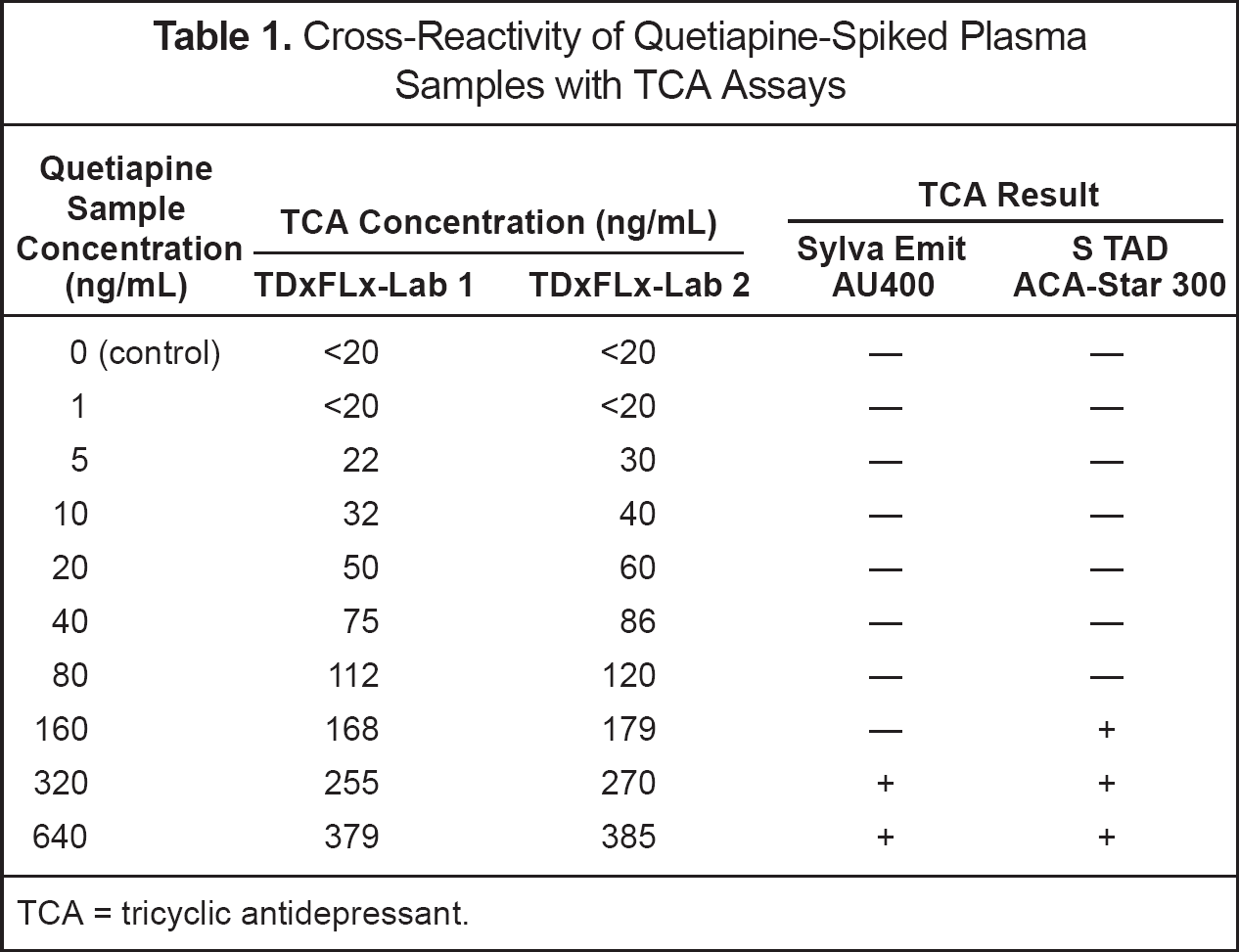
TCA = tricyclic antidepressant.
The qualitative TCA immunoassays screened as positive at quetiapine concentrations of ≥160 ng/mL and ≥320 ng/mL for the S TAD and Emit assays, respectively.
Discussion
This in vitro controlled study demonstrates that quetiapine cross-reacts with plasma TCA immunoassays in a concentration-dependent fashion. The quantitative TCA assay began to show cross-reactivity at a relatively low plasma quetiapine concentration of 5 ng/mL. Samples were analyzed on separate TDxFLx analyzers in 2 separate labs to evaluate potential laboratory bias. The TCA concentration results of the spiked samples from both laboratories were very similar. Due to the 300-ng/mL threshold of the 2 qualitative assays for a positive result, cross-reactivity was not observed until the 160- and 320-ng/mL spikes for the S TAD and Emit assays, respectively.
Immunoassay screening tests are commonly used in clinical laboratories because they are inexpensive, easy to use, and have a rapid turnaround time. However, they lack the specificity of more sophisticated tests such as GC and HPLC. Immunoassay technology uses a polyclonal antibody directed at a certain parent drug or its metabolite in a class. The antibody reacts variably with active and inactive metabolites, as well as other drugs in the therapeutic class.2,3 Although the antibody is directed at a target drug, it often has affinity for other drugs and their metabolites that have similar chemical structures. The degree of cross-reactivity to alternate drugs or metabolites varies.
Quetiapine is structurally similar to imipramine (Figure 1). Commercially available instrumented TCA immunoassays use imipramine as the target drug. Drugs previously known to cause interference or false-positives on TCA immunoassays include carbamazepine, 4 diphenhydramine, 5 cyclobenzaprine, 6 cyproheptadine, 7 and phenothiazines. 8 Urine spiked with quetiapine has tested qualitatively positive using Syva RapidTest d.a.u. and Microgenics Tricyclic Serum Tox EIA Assay at concentrations of 1000 and 10 μg/mL, respectively. 9 Patient samples with urine quetiapine concentrations of 0.2 and 7.5 μg/mL also tested positive using both tests, suggesting that a metabolite of quetiapine may also cross-react with the assay. Quantitative analysis was not performed on the urine samples and, unlike our study, a dose—response trend was not established. 9 We used plasma samples rather than urine for several reasons. These immunoassays are intended for use with plasma, immediate quantitative TCA measurements are usually performed on plasma, and many hospitals use plasma TCA screens rather than urine.
CLINICAL RELEVANCE
Quetiapine is an atypical antipsychotic used in the treatment of schizophrenia. The mean plasma concentration of quetiapine in schizophrenic patients on a multidose schedule of 250 mg every 8 hours ranges from 400 to 600 ng/mL. 10 The median peak blood concentration in a series of patients with quetiapine overdose was 2590 ng/mL (range 220–20 480%). 11 These concentrations exceed the threshold for positive results for the qualitative plasma assays in our study. In addition, a quantitative plasma assay for TCA may produce a result suggestive of a toxic TCA plasma concentration (eg, >300 ng/mL) at these therapeutic and toxic quetiapine concentrations.
The clinical presentation of quetiapine toxicity includes central nervous system depression, seizures, prolonged QTc interval, sinus tachycardia, and hypotension. 5 This presentation can be similar to that with TCA toxicity and, in combination with a positive TCA immunoassay, can lead to a misdiagnosis of the intoxication. A few case reports have described patients on therapeutic doses of quetiapine12,13 or presenting with symptoms of quetiapine overdose who tested positive for TCAs by immunoassay.9,14 Our study provides in vitro evidence that confirms the potential for the false-positive results reported in these case reports.
LIMITATIONS
This study was performed with pooled human plasma. The samples were not obtained from patients taking quetiapine therapeutically or as an overdose. Therefore, the immunoassay cross-reactivity quantitative results and positive qualitative thresholds may differ in the clinical setting. Only the parent compound, quetiapine, was tested. Possible cross-reactivity with the major metabolites of quetiapine was not investigated. It is unknown how the presence of metabolites may affect the cross-reactivity of the assays. This study was performed on a single day in 2 labs for the quantitative and 1 lab for the qualitative assays with a limited number of samples.
Conclusions
In this in vitro study, quetiapine cross-reacted with quantitative and qualitative plasma TCA immunoassays in a concentration-dependent fashion. Therapeutic use or overdose of quetiapine may result in a false-positive plasma TCA immunoassay result. This cross-reactivity has been reported in isolated case reports, but the extent to which it occurs in clinical practice is not yet known. Quetiapine should be added to the list of drugs that may cross-react with plasma TCA immunoassays. Future research should investigate the incidence of false-positive TCA immunoassays in patients with quetiapine overdose and the impact on patient care.
Footnotes
This material was presented as a poster at the North American Congress of Clinical Toxicology, Chicago, September 2003.