Abstract
OBJECTIVE
To review recent advances in the prevention of venous thromboembolism (VTE) in acutely ill nonsurgical inpatients.
DATA SOURCES
A MEDLINE search (1966–March 2005) was done to identify relevant articles relating to prevention of VTE in acutely ill nonsurgical inpatients.
STUDY SELECTION AND DATA EXTRACTION
Four major prophylaxis trials, one registry, one guideline, and supporting articles representative of the subject matter from the last few years were included.
DATA SYNTHESIS
Enoxaparin, dalteparin, fondaparinux, and unfractionated heparin 5000 units every 8 hours are effective in reducing the risk of VTE in acutely ill medical patients, but such prophylaxis is currently underused. Barriers to be overcome include recognition of the importance of VTE in this population, definition of the optimal strategy to assess risks, optimal timing of the risk assessment, optimal prophylactic regimen for a given level of risk or disease state, and optimal duration of prophylaxis. We recommend that acutely ill medical inpatients should be risk-stratified early in their hospitalization. At this time, the specific risk-assessment protocol should be derived from the trial(s) of the available formulary agent(s). Decisions about providing prophylaxis must also be made considering anticoagulant contraindications and renal function. Mechanical methods of prophylaxis should be considered as monotherapy only if an anticoagulant contraindication exists. The optimal duration of prophylaxis is not known, but 14 days was used in recent studies.
CONCLUSIONS
Prophylaxis of VTE in acutely ill medical inpatients is underused. Data provide some guidance for increasing awareness and optimizing patient care.
Venous thromboembolism (VTE) is a complex, potentially life-threatening disease process involving deep vein thrombosis (DVT) and/or pulmonary embolism (PE). Thrombus formation can result from venous stasis, vascular injury, or hypercoagulability. VTE contributes to >250 000 hospitalizations annually, and the mortality rate associated with the complications of PE can reach 17%. 1 In patients hospitalized for an acute medical illness, the illness can increase the risk of VTE by eightfold. 2 This risk is even more significant when one considers that approximately 20% of hospitalized medical patients have ≥3 risk factors for developing VTE.2,3
Improved care is needed for prevention of VTE.2,3 A recent survey showed that 28% of hospitalized medical patients with risk factors for VTE received appropriate prophylaxis. 3 A prospective registry of >5000 patients (DVT-FREE) from 183 sites similarly found that 42% of patients received appropriate prophylaxis within 30 days prior to developing an ultrasound-confirmed DVT. Among inpatients diagnosed with DVT in the registry, 78% were on non-intensive care floors, and 50% were nonsurgical patients. 1
These findings suggest that VTE is an important cause of morbidity and mortality in acutely ill medical patients, similar to the more extensively described surgical patient. In fact, medical and surgical patients share many characteristics, such as immobilization and underlying risk factors. The National Quality Forum and Joint Commission on Accreditation of Healthcare Organizations have announced a project to standardize performance measures for the prevention of DVT. 4 In light of the importance of VTE prevention and underutilization of appropriate preventive strategies in medical patients, this paper reviews recent data on prevention and assessment of VTE in acutely ill medical patients. For purposes of this review, the terms acutely ill medical patient or medical patient will refer to an adult hospitalized and undergoing treatment, but not undergoing surgery, for an illness unless otherwise stated.
Prevention Strategies
Pharmacologic modalities to prevent VTE include unfractionated heparin, low-molecular-weight heparins (LMWHs) (eg, enoxaparin, dalteparin), and the factor Xa inhibitor fondaparinux. Antiplatelet agents provide insufficient VTE prophylaxis. For patients maintained on long-term anticoagulation (ie, warfarin) for another indication, the anticoagulant should be continued, without need for additional prophylaxis. However, currently there is insufficient evidence evaluating nonpharmacologic strategies in medical patients. With pharmacologic agents, there is a relative lack of trials in the medical population compared with the surgical population. 2 The following recent trials are representative of a growing body of literature.
Three recent large trials compared anticoagulants with placebo: MEDENOX, 5 PREVENT, 6 and ARTEMIS, which is available only in abstract form. 7 Study inclusion criteria and additional conditions generally considered as VTE risk factors are summarized in Table 15–8; acronyms of clinical trials are shown in Appendix I.
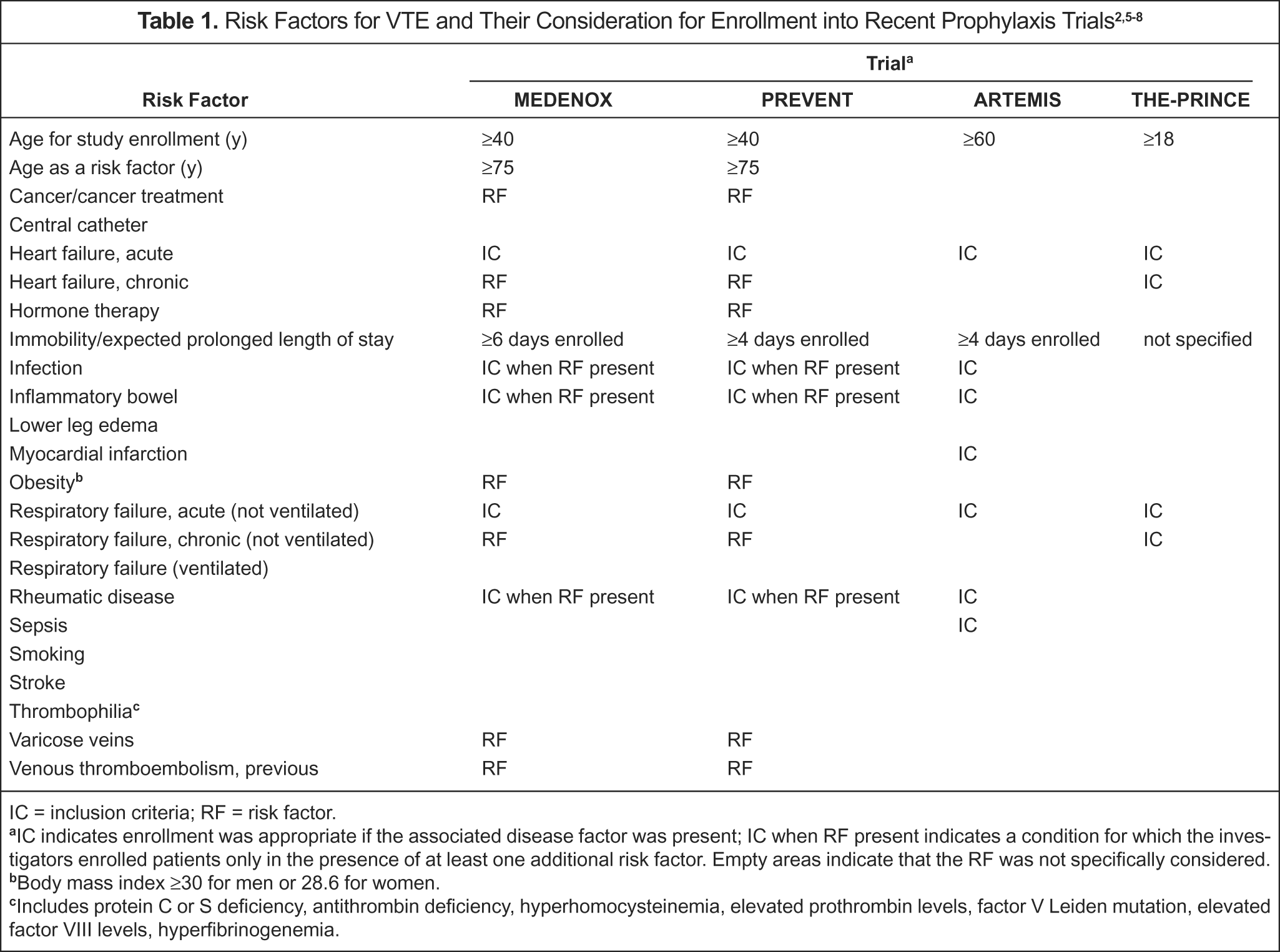
IC = inclusion criteria; RF = risk factor.
IC indicates enrollment was appropriate if the associated disease factor was present; IC when RF present indicates a condition for which the investigators enrolled patients only in the presence of at least one additional risk factor. Empty areas indicate that the RF was not specifically considered.
Body mass index ≥30 for men or 28.6 for women.
Includes protein C or S deficiency, antithrombin deficiency, hyperhomocysteinemia, elevated prothrombin levels, factor V Leiden mutation, elevated factor VIII levels, hyperfibrinogenemia.
The MEDENOX study was a double-blind, multicentered, placebo-controlled trial conducted in 866 patients. 5 The 3 groups evaluated in the trial received enoxaparin 40 mg/day subcutaneously, enoxaparin 20 mg/day subcutaneously, or placebo. The primary efficacy endpoint was the incidence of VTE (ie, DVT or PE) between days 1 and 14. DVT was defined by contrast venography or venous ultrasound, and PE was defined by high-probability lung scanning, pulmonary angiography, helical computed tomography, or autopsy. Major hemorrhage was overt and included loss of ≥2 units of packed red blood cells or whole blood with a decrease in hemoglobin of at least 2 g from baseline or if bleeding was retroperitoneal, intracranial, or fatal. Minor bleeding was any other bleeding not classified as major. The frequency of the primary endpoint was 5.5% in the enoxaparin 40–mg group, 15% in the 20-mg group, and 14.9% in the placebo group (63% RR, enoxaparin 40 mg vs placebo; p < 0.001). The frequency of hemorrhage, thrombocytopenia, and death was not statistically significantly different between the groups.
The PREVENT study compared dalteparin 5000 units/day subcutaneously with placebo. 6 It was a randomized, double-blind, placebo-controlled, multicenter trial that included 3706 patients. The primary efficacy endpoint was the incidence of VTE by day 21. VTE was defined as confirmed symptomatic DVT, fatal or symptomatic nonfatal PE, sudden death, or asymptomatic proximal DVT assessed by compression ultrasound. Bleeding was defined as major (intraocular, spinal/epidural, intracranial, or retroperitoneal, leading to death, requiring transfusion of at least 2 units of blood, or requiring surgical intervention) or minor (all not classified as major). The primary endpoint occurred in 2.77% in the dalteparin group and 4.96% in the placebo group (55% RR; p = 0.0015). The frequency of bleeding rates and other adverse events was not significantly different at day 21.
In the ARTEMIS study, a randomized trial of 849 patients given fondaparinux 2.5 mg/day subcutaneously or placebo, the primary endpoint was venogram-confirmed or symptomatically observed DVT between days 6 and 15. 7 Major bleeding included fatal bleeding, nonfatal critical organ bleeding, bleeding requiring surgical intervention, or bleeding associated with at least a 2-g fall in hemoglobin and/or ≥2 units of blood transfusion. Patients were >60 years of age and admitted with acute cardiac, respiratory, infectious, or inflammatory conditions. The primary endpoint occurred in 5.6% of patients in the fondaparinux group and 10.5% in the placebo group (49.5% RR; p = 0.029). Major bleeding was the same in both groups.
In addition to placebo-controlled trials, studies have compared LMWHs with unfractionated heparin. THE-PRINCE was a multicenter, randomized, open, parallel-group study that compared subcutaneous enoxaparin 40 mg/day and unfractionated heparin 5000 units 3 times a day in patients with heart failure or severe respiratory disease (Table 1). 8 The primary efficacy endpoint was the occurrence of thromboembolic events as confirmed by DVT-bilateral venography, suspected ventilation perfusion lung scan, chest X-ray/perfusion lung scan, and pulmonary angiography. Patients were examined for bleeding and other adverse events. The enoxaparin group contained 239 patients, and 212 patients were enrolled in the unfractionated heparin group.
The efficacy endpoint occurred in 8.4% of patients in the enoxaparin group versus 10.4% in the unfractionated heparin group, which was not significantly different. Although bleeding events were less frequent in the enoxaparin group, the difference compared with the unfractionated heparin group was not statistically significant. Other adverse events, which were not specifically reported, were significantly less common in the enoxaparin group. 8
Results of recent studies are consistent with a meta-analysis of earlier trials in which either prophylactic low-dose unfractionated heparin or LMWH was associated with a similarly lower incidence of DVT and PE (56–58% RR) relative to no prophylaxis, without an appreciable difference in effectiveness between the agents. 9 However, LMWH reduced the risk of major hemorrhage by 52% (p = 0.049) compared with unfractionated heparin.
Risk Factors and Assessment
RISK FACTORS
Recent randomized trials indicate that the use of anticoagulant prophylaxis reduces the incidence of VTE.5–8 Effective prevention requires prior identification of the at-risk population. As illustrated in Table 1, several conditions appear to predispose patients to VTE formation. However, there are inconsistent definitions of a risk factor for VTE among recent studies. Additionally, some conditions traditionally considered to be risk factors, such as intubation, thrombophilia/hypercoagulable state, and stroke, were not specifically evaluated in the recent prevention trials. Further, risk factors for upper-extremity DVT may differ from conventional lower-extremity DVT risk factors. 10 The heterogeneity of acutely ill medical patients and uncertainty regarding evaluation of risk factors have led to the development of risk assessment tools.
RISK ASSESSMENT TOOLS
Classic signs and symptoms of DVT occur in approximately one-third of individuals, and PE often occurs without warning or chance to resuscitate the patient. 2 Therefore, it is critical to identify patients who are likely to develop VTE and provide appropriate prophylaxis. The primary factor contributing to VTE risk may vary greatly from patient to patient, which underscores the need for an individualized risk assessment strategy.
Two general approaches have been taken in assessing risk for VTE and making decisions about the need for VTE prophylaxis. 2 These tools are used to classify patients as having either low or moderate risk of VTE.2,5 The first approach is to use an algorithm that scores each risk factor present in an individual patient. Patients exceeding a predetermined score are candidates for prophylaxis. 11 The second method involves use of prophylaxis in all patients with one or more major target conditions (eg, heart failure, hospital service, prolonged immobility).2,5
Unfortunately, neither assessment strategy is appropriately validated. Either may be cumbersome and time consuming. A recent study attempted to retrospectively validate 3 published risk assessment tools and found that only one successfully stratified the risk. 11 Another study evaluated the implementation of a risk assessment guideline, using ultrasound follow-up examination, and found that the incidence of DVT decreased from 9.5% in the pre-intervention sample to 3.2% (p < 0.001) in the post-intervention sample. 12 Interestingly, the use of pharmacologic prophylaxis also decreased from 48.8% to 39.7% (p = 0.02), respectively, primarily due to reduction in unnecessary anticoagulant prescribing.
An alternative strategy involves electronic computer-generated physician alerts. 13 Medical or surgical patients at least 18 years of age were randomly assigned to an intervention group (n = 1255) or a control group (n = 1251). A computer program, linked to a patient database and designed to assess individual patient risk and alert prescribers, demonstrated a reduction in the primary endpoint of clinically diagnosed, objectively confirmed DVT or PE. The 90-day incidence of the primary endpoint was 4.9% in the intervention group and 8.2% in the controls, and the respective Kaplan–Meier estimates for freedom from VTE were 94.1% and 90.6% (p < 0.001). Reduction in VTE corresponded to a respective increase in mechanical prophylaxis (10% vs 1.5%; p < 0.001) and pharmacologic prophylaxis (23.6% vs 13%; p < 0.001).
These data suggest that, in the absence of a validated gold standard risk assessment tool, a locally developed consensus protocol with active implementation can improve patient outcomes.12,13
Clinical Conundrums/Areas for Future Research
The benefit and cost-effectiveness of VTE prophylaxis in patients with acute medical illness are established. 2 Of issue among clinicians is that most DVTs are asymptomatic and confined to the calf; however, prevention of such clots is of proven benefit. 14 A number of ill-conceived perceptions, such as the relative importance of distal DVTs and the risks of bleeding with anticoagulants, encouraged underutilization of prophylaxis, and hospital education programs failed to improve the appropriate delivery of prophylactic regimens. 15 Underutilization is also due to unanswered questions about optimal use of this important therapy in the clinical setting including patient selection, optimal prophylaxis modalities, and duration of therapy.
The identification of the optimal time to assess requirements for VTE prophylaxis is critical to the optimization of patient care. It is unknown when the patient is at greatest risk for developing VTE. Enrollment criteria based on immobility was defined by several different means in recent studies. Patients immobile for <3 days with an expected length of stay of at least 6 days were admitted to one study, 5 while immobility for <3 days and expected length of stay of at least 4 days was used for inclusion into another trial. 6 Patients with an expected duration of hospitalization of at least 4 days were enrolled in another study, 7 and confinement to bed for more than two-thirds of a day was used in a fourth trial. 8 The DVT-FREE registry found that the median duration of hospitalization at the time a DVT was diagnosed in nonsurgical inpatients was 2 days—much earlier than 6 days in surgical patients (p < 0.001). 1
In acute medical illness, the risk of developing VTE is characterized as low to moderate, with VTE occurring in 5–25% of patients. 2 Available data indicate that several factors, including patient age and heart or respiratory failure, affect the rate of VTE. Studies of VTE prophylaxis have included patients with specific diagnoses and some of the recognized risk factors for VTE.5–9 THE-PRINCE study results demonstrate that VTE appears to occur more frequently in patients with heart failure compared with similarly treated patients with respiratory disease. 8 Variable rates of VTE were also observed in another trial, depending on the medical service to which the patient was admitted. 11 Therefore, it appears that the risk of VTE varies considerably. Additional information on the differing rates of VTE for various medical illnesses could result in different appropriate VTE prophylaxis based on illness severity and risk factor characteristics, similar to what is accepted for the surgical population. For example, it is currently uncertain whether a patient with 7 risk factors is at the same risk and has the same prophylaxis requirements as one with heart failure and one other risk factor.
Early ambulation is recommended only for low-risk surgical or medical patients. 2 For the moderate-risk surgical patient, methods including mechanical modalities (compression stockings or intermittent pneumatic compression) or unfractionated heparin 5000 units given subcutaneously twice daily are recommended as appropriate prophylaxis. For the moderate-risk medical patient, unfractionated heparin 5000 units twice daily has been inadequately studied, and mechanical modalities have not been studied. Currently, the American College of Chest Physicians (ACCP) guideline recommends the use of low-dose unfractionated heparin (5000 units every 8 or 12 h) or an LMWH for VTE prophylaxis in acutely ill medical patients and the option to use mechanical methods if anticoagulants are contraindicated. 2 This obvious discrepancy between recommended VTE prophylaxis for moderate-risk medically ill and surgical patients needs to be addressed in future research.
Major bleeding is rare at the dosages of anticoagulants used for VTE prophylaxis, but it does represent a well-appreciated adverse event that influences prescribing behavior in the clinical setting. Of particular importance are chronic kidney disease (CKD) and obesity, frequently encountered comorbidities in hospitalized patients. Acute care pharmacists are frequently consulted for guidance regarding the most appropriate VTE prophylaxis strategy in these 2 populations.
CKD may create a hypocoagulable or hypercoagulable state. 16 Moreover, patients with CKD or end-stage renal disease often have concomitant conditions such as hyperhomocysteinemia, endothelial dysfunction, and inflammatory states. 16 Despite the relatively common occurrence of thrombosis in patients with renal dysfunction, there is a paucity of data assessing the use of LMWHs for VTE prophylaxis in these patients. Patients with CKD were excluded from large clinical trials (MEDENOX, PREVENT, THE-PRINCE).5,6,8 Hence, there are no reliable outcomes data to evaluate the incidence of VTE or the safety and efficacy of LMWH products when given at relatively low prophylactic doses in medical patients with concomitant renal dysfunction.
The absence of definitive clinical data has led clinicians to attempt to translate pharmacokinetic and pharmacodynamic data to this population. The pharmacokinetic surrogate marker of LMWH concentration in plasma, anti-factor Xa activity, is poorly correlated to efficacy and toxicity. 17 Moreover, it appears that the pharmacodynamic (anticoagulant) response in patients with renal dysfunction is enhanced at a given anti-factor Xa activity. 18 When the anti-factor Xa activity is the same between controls and patients with renal dysfunction, the renal patients have a greater anticoagulant effect as measured by thrombin generation time. 19
One pharmacokinetic study evaluated subcutaneous enoxaparin 40 mg given prophylactically over 4 days to patients with varying degrees of renal insufficiency.
20
The results demonstrated little pharmacokinetic difference in anti-factor Xa activity between controls and subjects with mild to moderate renal dysfunction (creatinine clearance [Cl
The manufacturer of enoxaparin has recently changed its prescribing information to reflect that the dose should be reduced from 40 to 30 mg once daily in patients with Cl
Obesity is an independent risk factor for the development of VTE.5,6 There are currently no prospective studies evaluating the efficacy of LMWH in preventing VTE events in obese medical patients. Current literature contains 2 pharmacokinetic/pharmacodynamic studies assessing enoxaparin disposition in obese patients receiving treatment doses24,25 and a comparison of 2 enoxaparin prophylactic regimens in combination with other prophylactic modalities in patients undergoing bariatric surgery. 26 The results of the bariatric surgery trial suggested that subcutaneous enoxaparin 40 mg twice daily was more effective than 30 mg twice daily. Drawing firm conclusions is difficult given statistically significant differences between the treatment groups in surgical duration and length of hospitalization and the uncertain implications for nonsurgical patients. 26 The pharmacokinetic/pharmacodynamic studies did not support a requirement of dose modification of treatment doses in obese patients.24,25 No studies were identified that evaluated medical prophylaxis with dalteparin or fondaparinux in obese patients.
Finally, the optimal duration of VTE prophylaxis in the medically ill patient is unknown. Durations of therapy varying between 6 and 14 days have been used.5–9 In the clinical setting, practitioners likely will continue VTE prophylaxis until patient discharge. It is uncertain whether a patient who is transferred to a subacute medical setting, such as a rehabilitation center, should continue to receive VTE prophylaxis beyond 14 days. In agreement with issues raised previously, the optimal duration in a given patient likely is influenced by the issues of diagnosis, patient risk characteristics, and perhaps most importantly, ambulation.
Recommendations
Recent advances in our understanding of VTE risk in acutely ill medical patients have led to a greater comprehension of the benefits of prophylactic anticoagulants. Table 2 summarizes our recommendations for patient assessment and VTE prophylaxis. Recommendations are graded according to established criteria. 27
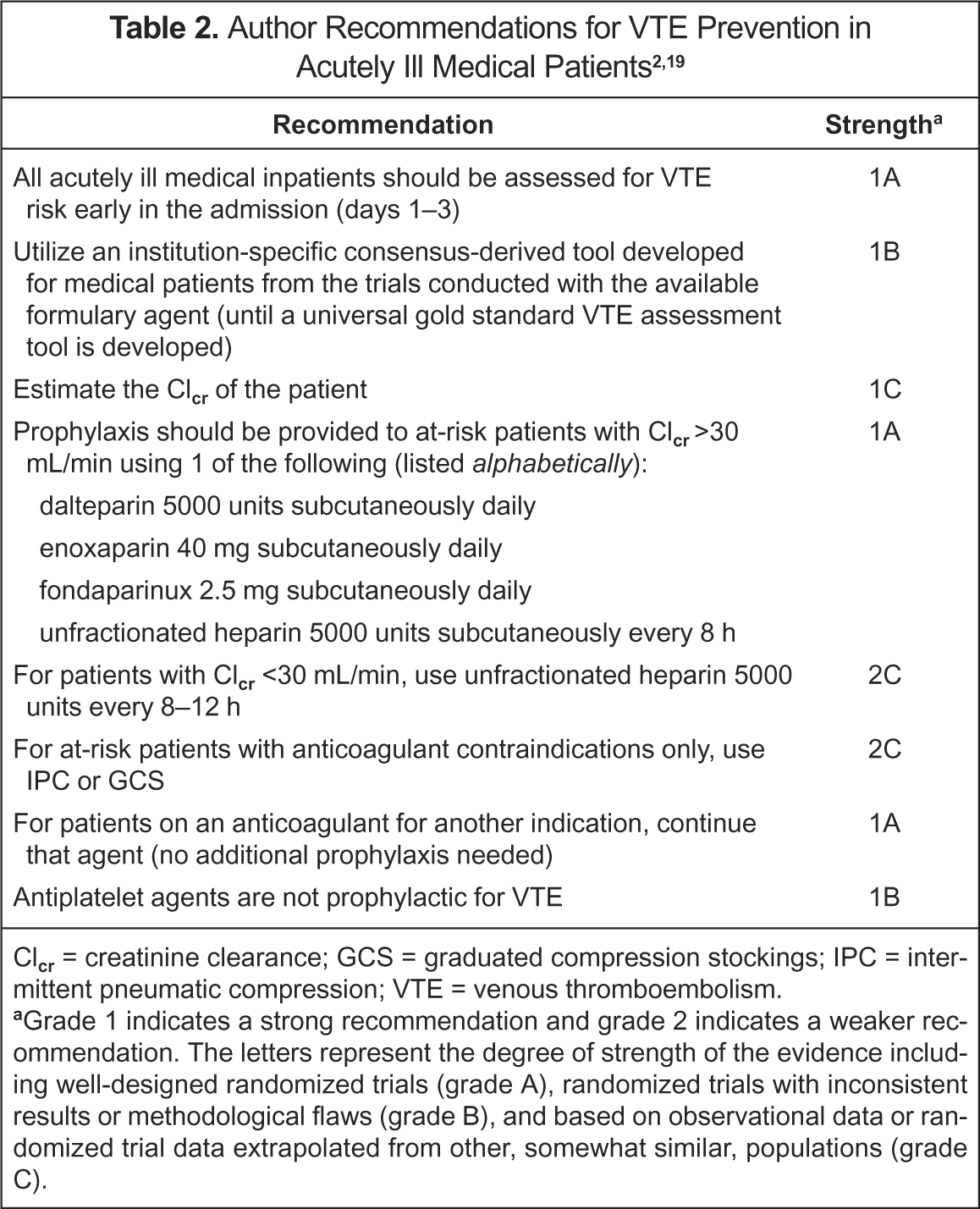
Clcr = creatinine clearance; GCS = graduated compression stockings; IPC = intermittent pneumatic compression; VTE = venous thromboembolism.
Grade 1 indicates a strong recommendation and grade 2 indicates a weaker recommendation. The letters represent the degree of strength of the evidence including well-designed randomized trials (grade A), randomized trials with inconsistent results or methodological flaws (grade B), and based on observational data or randomized trial data extrapolated from other, somewhat similar, populations (grade C).
Patients should be risk-stratified early in their hospitalization (days 1–3). The ACCP recommends the target group risk assessment method, but this still requires a healthcare practitioner to evaluate the potential need for VTE prophylaxis in each patient. 2 Prescribers can be assisted by direct notification after identification of potential VTE prophylaxis candidates by either pharmacy departments or computer-generated electronic alerts. 12 Preprinted orders may also be helpful in guiding prescribers since education alone is not very effective. 15 We recommend risk stratification by application of the inclusion criteria from the major trial(s)5–8 corresponding to the formulary agent(s) available at a given institution. A risk-assessment protocol derived from the trial(s) should be implemented by obtaining consensus among the institutional users. The users should recognize the proven risk reduction of this strategy, but should also note the possibility that some risk factors will not be taken into account.
When evaluating patients for prophylaxis, anticoagulant contraindications and renal function should be considered. Mechanical methods of prophylaxis should be considered for monotherapy only if an anticoagulant contraindication exists. Based on insufficient published evidence, LMWH or fondaparinux should be avoided in patients with Cl
Summary
Prophylaxis of VTE in acutely ill medical inpatients is effective but underutilized. Patients should be risk-stratified early in their hospitalization (days 1–3). Risk stratification by application of the inclusion criteria from major trials corresponding to the formulary agents available at a given institution is appropriate. Prescribers can be notified after identification of potential VTE prophylaxis candidates by either pharmacy departments or computer-generated electronic alerts. Anticoagulant contraindications and renal function should be considered when choosing prophylaxis strategies. Mechanical methods of prophylaxis should be considered for monotherapy only if a contraindication to use of an anticoagulant exists.
Footnotes
Appendix I. Acronyms of Clinical Trials
| ARTEMIS | Arixtra for Thromboembolism Prevention in a Medical Indications Study |
| MEDENOX | Prophylaxis in Medical Patients with Enoxaparin |
| PREVENT | Prospective Evaluation of Dalteparin Efficacy for Prevention of Venous Thromboembolism in Immobilized Patients |
| THE-PRINCE | Thromboembolism—Prevention in Cardiac or Respiratory Disease with Enoxaparin |