
Abstract
OBJECTIVE:
To report a case of concomitant warfarin therapy with consecutive cycles of capecitabine therapy, providing time of onset, magnitude, and assessment of the interaction.
CASE SUMMARY:
A 59-year-old man receiving chronic warfarin therapy for a mechanical mitral valve replacement was diagnosed with stage IV metastatic colon cancer. He was started on capecitabine/irinotecan after his cancer progressed with fluorouracil/leucovorin and the FOLFOX 6 regimen (oxaliplatin, leucovorin, and continuous fluorouracil infusion). He received 3 consecutive cycles of capecitabine/irinotecan with concomitant oral anticoagulation and, with each cycle, the warfarin dose was reduced. Over the course of these 3 cycles, the total weekly dose of warfarin was reduced by >85%.
DISCUSSION:
The capecitabine–warfarin interaction is clinically significant, requiring a black box warning in the package insert. The mechanism of action for the interaction is not clear, but may be related to down-regulation of CYP2C9 by capecitabine or its metabolites or a pharmacodynamic interaction with warfarin. A common response to this interaction, as discussed in previously published case reports, is the discontinuation of warfarin, capecitabine, or both. In this case, the Naranjo probability scale indicates a highly probable drug interaction between warfarin and capecitabine.
CONCLUSIONS:
As more patients require anticoagulation, and as chemotherapy agents such as capecitabine become available, the likelihood for these drug interactions increases. In our patient, close monitoring of therapy allowed successful use of warfarin and capecitabine.
Capecitabine, a fluoropyrimidine carbamate with antineoplastic activity, is an orally administered systemic prodrug that is converted to fluorouracil. Capecitabine is indicated for treatment of colorectal cancer and breast cancer. The recommended dose is 1250 mg/m 2 administered orally twice daily (2500 mg/m 2 total daily dose) for 2 weeks followed by a one-week rest period given in 3-week cycles. Postmarketing reports identified a significant interaction between warfarin and capecitabine necessitating a black box warning in the package insert. 1 Clinically relevant increases in prothrombin time/international normalized ratio (INR), major bleeding events, and 2 deaths have been reported in the literature and to the Food and Drug Administration (FDA).
Bleeding events secondary to the interaction between capecitabine and oral anticoagulants have occurred within several days to several months after initiation of capecitabine therapy and, in one case, several months after discontinuation of the drug. In each case, the elevated prothrombin time and/or bleeding event resulted in discontinuation of warfarin, capecitabine, or both. These reports are limited in describing the time of onset and management of the drug interaction (other than discontinuation of one of the offending agents).
We present a case of anticoagulation therapy given concomitantly with 3 concurrent cycles of capecitabine.
Case Report
A 59-year-old man receiving chronic warfarin therapy with a goal INR of 2.5–3.5 for a mechanical mitral valve replacement was diagnosed with stage IV colon cancer with hepatic metastasis. The patient's past medical history was significant for gastroesophageal reflux disease, right hemisphere cardioembolic stroke (secondary to discontinuation of warfarin for dental procedure), anemia, hemorrhoids, and rheumatic heart disease. His outpatient medications at the start of chemotherapy included prochlorperazine 10 mg as needed for nausea, senna 8.6 mg daily, and warfarin daily as directed by the anticoagulation clinic. Prior to initiating chemotherapy, the patient was stable, and therapeutic INRs were maintained with an average warfarin dose of 10.35 mg/day. His height and weight were 165 cm and 51 kg, respectively. His calculated body surface area was 1.53 m 2 .
Following lower wedge resection of the sigmoid colon and liver mass resection, the patient received 3 cycles over 6 months of fluorouracil/leucovorin (leucovorin 500 mg/m 2 over 2 h with fluorouracil 500 mg/m 2 bolus 1 h after start of leucovorin). During this 6-month course, recombinant epoetin alfa 40 000 units weekly, rabeprazole 20 mg daily, potassium chloride 20 mEq daily, and hydromorphone 2 mg every 3 hours as needed were added to his regimen; senna was discontinued.
After completion of the chemotherapy regimen, a restaging computed tomography (CT) scan showed new pulmonary nodules and liver metastasis. Following right lower lobe resection of the lung, the patient was started on the FOLFOX 6 regimen given every 2 weeks (oxaliplatin 100 mg/m 2 over 2 h with leucovorin 400 mg/m 2 over 2 h, fluorouracil 400 mg/m 2 intravenous bolus, followed by fluorouracil continuous infusion 2.25 g/m 2 /day given over 46 h). 2 After 4 cycles, a restaging CT scan revealed progression of the lung and liver metastases. The patient then received 2 weeks off chemotherapy prior to initiating capecitabine/irinotecan (capecitabine 1000 mg/m 2 twice daily on days 2–15, irinotecan 120 mg/m 2 on days 1 and 8 given every 3 wk). 3 Atropine 0.025/diphenoxylate 2.5 mg every 4 hours as needed was added to his drug regimen while receiving capecitabine/irinotecan. No medications were discontinued during this time.
The patient completed 3 consecutive cycles of capecitabine/irinotecan. He remained on warfarin throughout the duration of his chemotherapy. He experienced some nausea but no vomiting, and his weight remained stable. Laboratory tests were performed on a routine basis. The albumin level, platelet count, and liver function test results (except alkaline phosphatase) remained within normal limits throughout treatment with capecitabine/irinotecan. The alkaline phosphatase level was 117 U/L (reference range 30–115%) at the start of cycle 1 and progressed to 134 U/L by the end of cycle 3.
Our management of the warfarin—capecitabine interaction is illustrated in Figures 1–3. The patient's INR was initially low (1.3%) on day 0, cycle 1 ((Figure 1)). His average warfarin dose was 3.6 mg/day following resolution of the fluorouracil interaction 2 weeks earlier. He refused the use of low-molecular-weight heparin, so the dose of warfarin was increased significantly over the next 5 days to decrease the risk of thromboembolism. Sixteen days after initiation of chemotherapy (day 16, cycle 1%), the patient's INR was supratherapeutic (5.83%) while he received 5.7 mg/day of warfarin. Warfarin was withheld for 2 days, and the total weekly dose was reduced. On day 21, cycle 1, a goal INR was achieved (3.3%) with 3 mg/day. On day 7 of cycle 2 ((Figure 2)), the INR was elevated (7.09%) despite a dose reduction to 2.8 mg/day initiated the week before. No signs of bleeding or bruising were reported.
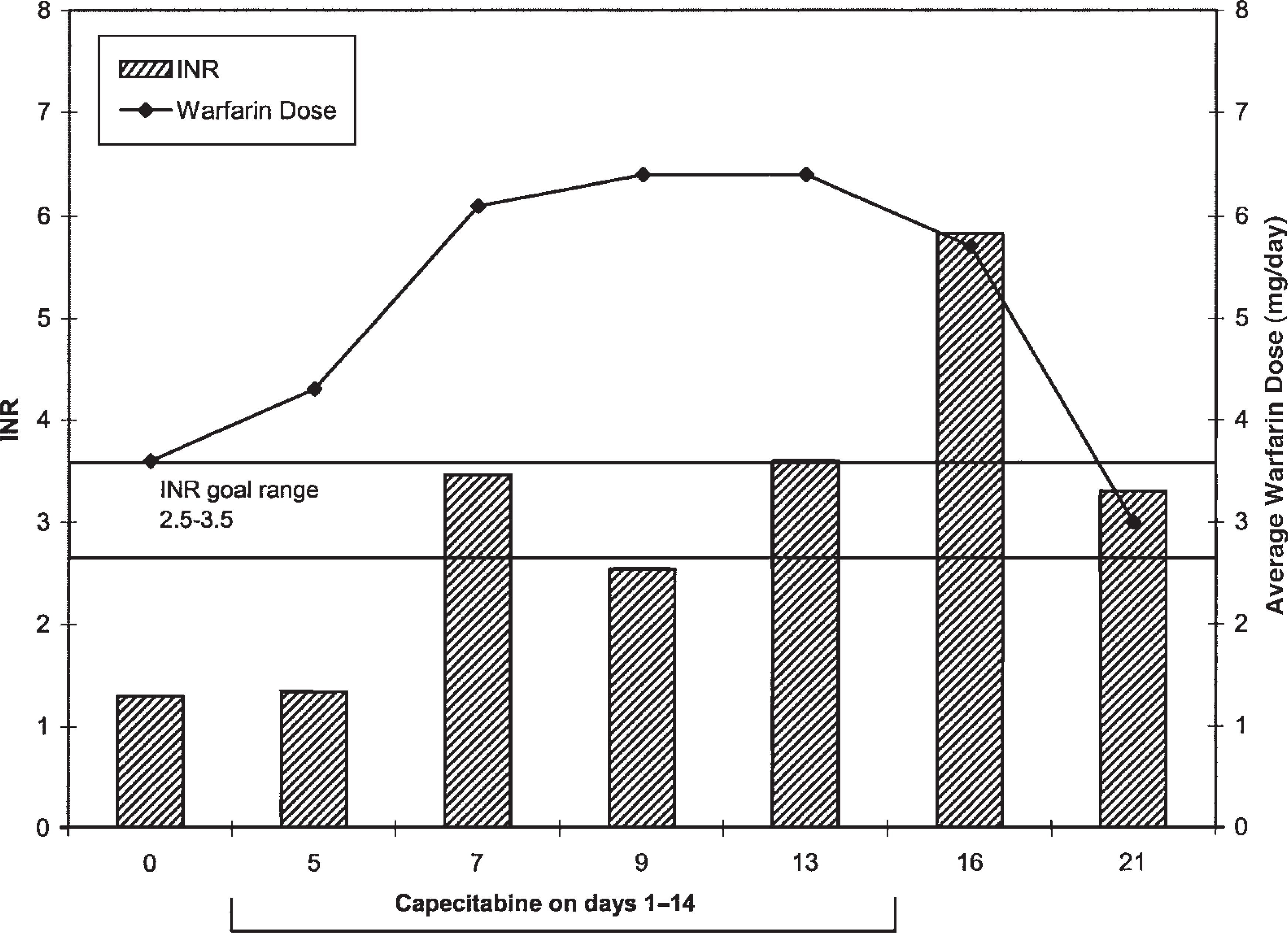
Management of warfarin therapy and INR response during cycle 1.
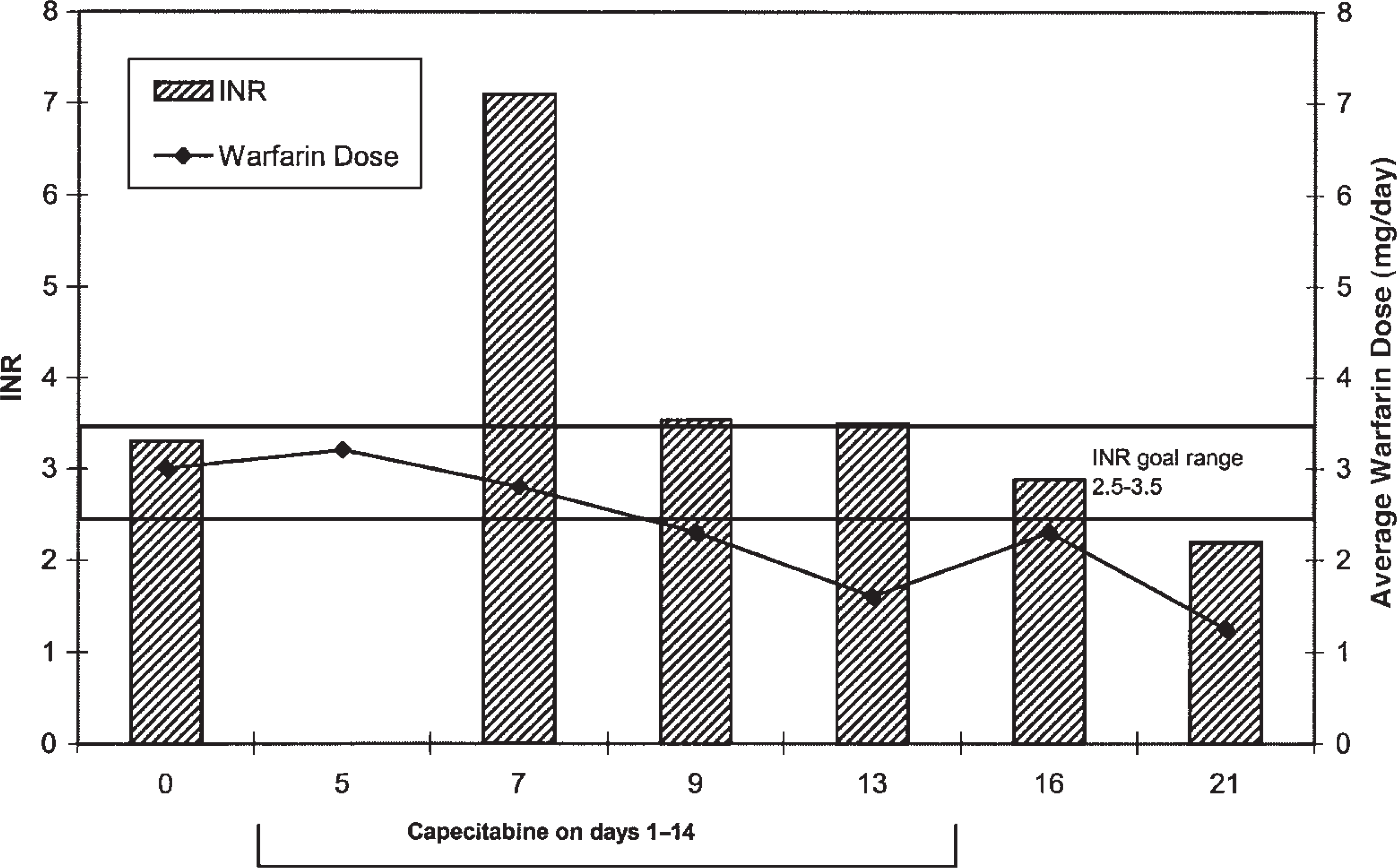
Management of warfarin therapy and INR response during cycle 2.
Warfarin was again withheld for 2 days and, on day 9, the INR was 3.53. The patient's dose was further reduced to 1.25 mg/day over the remaining 12 days, achieving an INR of 2.19 at the beginning of cycle 3. After reviewing the INR trends in cycles 1 and 2, clinicians checked the INR on day 5 of cycle 3 ((Figure 3)). The INR was elevated (4.33%), and the warfarin dose was lowered on 3 occasions to obtain a therapeutic INR (2.57%) on day 21 with a dose of 0.78 mg/day. After completion of 3 cycles of capecitabine/irinotecan, the average daily dose of warfarin was reduced by >85% to achieve a therapeutic INR.
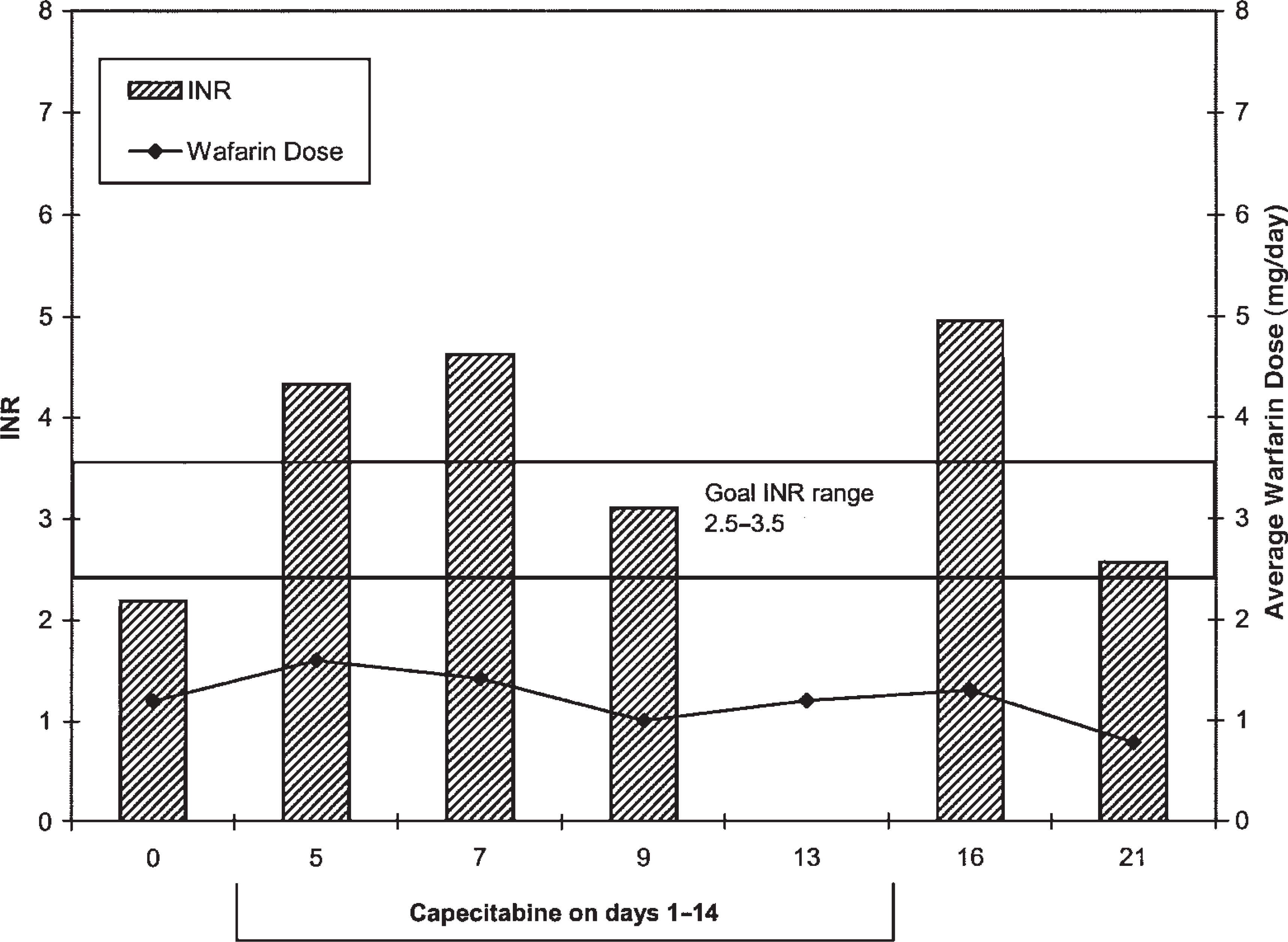
Management of warfarin therapy and INR response during cycle 3.
A restaging CT recently revealed progression of cancer in the liver and lungs, and the patient chose not to continue chemotherapy. After discontinuation of capecitabine/irinotecan, his warfarin dosage was increased to 4 mg/day to achieve a therapeutic INR over the next 3 weeks.
Discussion
Based on an objective causality assessment, it is highly probable that an interaction between warfarin and capecitabine exists. 4 Our case illustrates the management problems that can occur with concomitant use of warfarin and capecitabine during consecutive cycles of chemotherapy. During the first cycle, the INR most likely became elevated due to the rapid dosage escalation of warfarin required after the patient refused enoxaparin bridge therapy. However, at the end of cycle 1, he was taking 16% less warfarin than at the beginning of that cycle. Subsequent cycles also required further warfarin dosage reductions with no other identifiable causes for the increased INR such as additional drug interactions, vomiting, or weight loss. Worsening liver disease may be considered; however, once chemotherapy was stopped, the patient's warfarin requirements did increase. Over this period, he did not experience an adverseevent; however, maintaining INRs within the therapeutic range was challenging. We were fortunate to have a patient who was able to adhere to our monitoring requirements. This may not be feasible with other patients.
The significance of the interaction is illustrated by a black box warning in the package insert, although literature support of the interaction and potential management is limited. In our attempt to develop a monitoring plan, we reviewed the pharmacokinetic and pharmacodynamic profiles of capecitabine, the case series that prompted the FDA to require the black box warning, and 4 additional published cases.
Reigner et al. 5 reviewed the pharmacokinetics of capecitabine and the potential mechanisms of the interaction between capecitabine and warfarin. Capecitabine, a prodrug, is enzymatically converted in 3 metabolic steps to fluorouracil. Concentrations of fluorouracil are 3 times higher in colorectal tumor tissue and liver metastasis due to differences in the enzymatic activity of cytidine deaminase and thymidine phosphorylase. Interpatient variability in the pharmacokinetic profile of fluorouracil is >85% due to differences in the activity of these metabolic enzymes. 1 In vitro drug interaction studies investigated the inhibition potential of cytochrome P450 isoenzymes (1A2, 2C9, 3A4%) by capecitabine and its metabolites, including fluorouracil, and no significant interactions were identified.
A small pharmacokinetic and pharmacodynamic study in adults with advanced solid tumors was performed to assess the potential for a capecitabine—warfarin interaction. 6 Administration of capecitabine 1250 mg/m 2 twice daily starting on day 8 in 3-week cycles (2 weeks on, 1 week off) was given with a single 20-mg dose of warfarin on days 1 and 61. Pharmacokinetic and pharmacodynamic data were available on all sampling days (1, 20, 61%) for 4 of 6 patients. Results on day 61 (end of cycle 3%) showed an increase in both the AUC (57%) and half-life (51%) of the S-enantiomer of warfarin from baseline. The AUC and half-life of the R-enantiomer increased by 13% and 15%, respectively. Pharmacodynamically, a 2.8-fold increase in the baseline-corrected AUC of the INR was reported on day 61. The highest observed INR increase was 91% from baseline. Three of the 4 patients had an INR >3 and subsequently received vitamin K. Twelve patients were initially planned for the study, but enrollment ceased when results of a drug interaction were apparent.
R-warfarin is primarily metabolized by CYP1A2 and 3A4, and S-warfarin is metabolized by CYP2C9. Due to the lack of a direct interaction between CYP2C9 and capecitabine (or its metabolites), it has been hypothesized that the interaction may be related to down-regulation of CYP2C9. This would better explain the length of time after the drugs are administered for the interaction to become apparent. Another possible explanation is that fluorouracil, not capecitabine, is the cause. The interaction between fluorouracil and warfarin is well documented and likely relates to inhibition of CYP3A4 and 2C9. Unfortunately, the pharmacokinetic interaction between capecitabine and warfarin is not as well documented, and a pharmacodynamic increase in the INR is the most likely mechanism.
Labeling changes to the package insert identifying a potential interaction between capecitabine and warfarin were initially implemented in April 1999. 7 Eighteen cases were selected from the adverse events reporting system by the FDA for a case series review, resulting in the addition of a black box warning in June 2001. Three cases involved patients on phenprocoumon and 15 cases involved patients on warfarin. Seven of the cases involving warfarin occurred after the initial label change in 1999. Outcomes included 3 deaths, 9 hospitalizations, 1 patient requiring intervention, 1 life-threatening case, and 4 others that were considered medically relevant. 6 The majority of the cases involved females with breast cancer and patients >60 years of age; all deaths occurred in patients >75 years of age. None of the deaths occurred after the initial change in labeling. Average time to reported elevated INR was 30.5 days (range 6–61%), with an average INR of 12.4 (range 5.2–28.7%). Warfarin was discontinued in 9 cases, both warfarin and capecitabine were discontinued in 6 patients, and capecitabine was discontinued in 1 case; management in the final 2 cases was not reported. 7
Four cases have been published (Table 1): 2 in 2001 8 and 2 in 2003. 9 One of the cases from 2001 was also in the FDA case series. These reports emphasize that the interaction is most likely to occur in an older population and is associated with significant INR elevations, which increases the potential for life-threatening bleeding events. Unfortunately, the time of onset of the interaction remains poorly differentiated and most likely is due to individual variation in capecitabine metabolism.
Review of Cases of Capecitabine-Warfarin Interaction
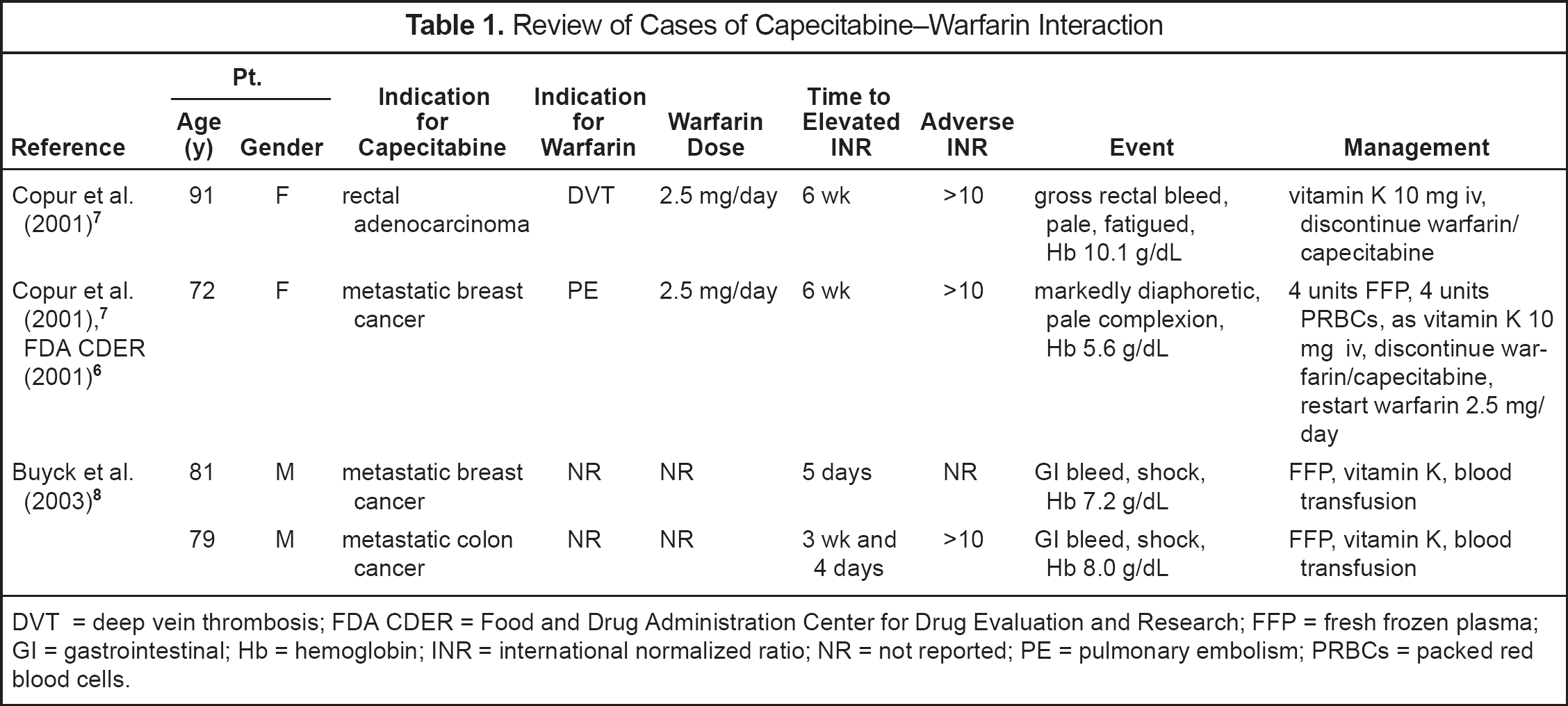
DVT = deep vein thrombosis; FDA CDER = Food and Drug Administration Center for Drug Evaluation and Research; FFP = fresh frozen plasma; GI = gastrointestinal; Hb = hemoglobin; INR = international normalized ratio; NR = not reported; PE = pulmonary embolism; PRBCs = packed red blood cells.
In our patient, the interaction between warfarin and capecitabine occurred within the first 2 weeks of each cycle, typically on days 7–16. His highest INR (7.09%) was consistent with other reported cases and occurred 28 days after initiation of capecitabine/irinotecan. Over the course of 9 weeks, the patient's warfarin dose was subsequently reduced over each cycle between 16% and 58%, illustrating capecitabine's cumulative effect. The established monitoring plan required follow-up INRs several times per week in an effort to avoid complications such as thromboembolism and bleeding. Adherence to blood draws and dosing recommendations was outstanding, and our patient did not experience any of the potential adverse events from chemotherapy that may have complicated the situation. Our experience and our patient's willingness to follow our recommendations have been invaluable in managing this critical drug—drug interaction. We recommend a minimum of weekly INR monitoring while capecitabine chemotherapy is administered, with more frequent (twice weekly) checks when INRs do not reflect dosage adjustments. Dosage reductions were significant in our patient and not consistent with many algorithms found in the literature. Dosage reductions up to 50% were required for each dosing cycle to maintain INRs near the therapeutic range. This can be done only with very close monitoring.
Conclusions
As more patients require anticoagulation and as chemotherapy agents, such as capecitabine, become available, the likelihood for these drug interactions increases. Alternatives such as low-molecular-weight heparins may be a more viable option in some patients; however, our patient refused its use even as bridge therapy, thus necessitating the close monitoring of the interaction. It is our desire that this report will be useful for clinicians for whom no alternatives are available to manage capecitabine and warfarin without adverse effect to the patient.