
Abstract
BACKGROUND
Despite significant progress in asthma drug therapy in recent years, there has been no major change in asthma morbidity and mortality. It is still important to determine whether pharmaceutical care (PC) influences health outcomes.
OBJECTIVE
To evaluate the effectiveness of PC with regard to clinical, humanistic, and economic outcomes in adults with asthma.
METHODS
An intervention study was conducted over 12 months. At baseline, 39 community/retail pharmacies, 84 primary care physicians (general practitioners, internal specialists, chest physicians), and 183 patients (aged 18–65 y) diagnosed with asthma were included. To evaluate economic outcomes, 2 German statutory health insurance funds provided 2 years of claims data for their insured patients (n = 55). A 1:10 matching was carried out to compare the data of this intervention subgroup with those of a control group (n = 550).
RESULTS
Significant improvements were found for all humanistic outcomes (eg, asthma-specific quality of life, self-efficacy, knowledge, medication adherence). In addition, asthma severity, self-reported symptoms, peak expiratory flow, and patients’ inhalation technique improved. Increases in forced expiratory volume in 1 second and vital capacity were not significant over time. Evaluation of the insurance claims data revealed a shift toward better adherence to evidence-based therapy.
CONCLUSIONS
The study shows that PC for people with asthma has a positive impact on humanistic and, to some extent, on clinical outcomes. To determine potential economic benefits, future research should focus on patients with more severe asthma.
Asthma is one of the major health problems in industrialized countries. 1 Although new drugs and evidence-based guidelines have been developed, there has been no major change in asthma morbidity and mortality. 2 Total costs for asthma in the German statutory health insurance (Gesetzliche Krankenversicherung, GKV), including direct and indirect costs, were calculated at £2.74 billion (about $3.58 billion US) during 1999. Indirect costs (primarily sickness benefit, early retirement, premature death) amounted to 75% of the total costs, suggesting that there is room for improvement in the area of asthma control. 3
As asthma symptoms and disease progression can be controlled by appropriate treatment and the correct use of medication, current guidelines focus on the importance of teaching self-management skills to patients. 4 Some experts claim that up to 90% of hospitalizations due to asthma are preventable provided that patients are trained, supervised, and treated more consistently. 5 Nevertheless, it is known from studies that patients’ knowledge about asthma and adherence to drug therapy is poor.6,7
In recent years, several multidisciplinary education programs for people with asthma have been established.8,9 Community pharmacy–based pharmaceutical care (PC) services for these patients have been proven to enhance medication adherence, self-management, and quality of life, as well as clinical outcomes.10–16 Weinberger et al. 17 found significantly higher peak flow rates in the PC group; however, those patients also had significantly more breathing-related emergency department and hospital visits.
In 2002, disease management programs for chronic diseases were introduced for clients of the GKV. Approximately 90% of the German population is insured by the GKV, which is part of the social security system. 18 Among a variety of other conditions, disease management programs include both asthma and chronic obstructive pulmonary disease (COPD).
Based on intensified cooperation between local community pharmacists, general practitioners (GPs), and other physicians, their regulatory bodies, and GKV, we investigated the effectiveness of PC with regard to clinical, humanistic, and economic outcomes in adults with asthma. This was a pivotal study to evaluate the contributions of community pharmacies in disease management program and/or integrated care contracts with regard to outcomes. In this context, we also examined whether drug therapy shifted toward better adherence with evidence-based guidelines or a reduction of hospitalizations and absence from work, which could have positive cost implications for health insurance funds.
Methods
STUDY POPULATION
All of the 148 community/retail pharmacies in the region of Trier (part of the State of Rhineland–Palatino, population 512 000) were invited by mail to enter the study. The invitation letter was signed both by the president of the chamber of pharmacists in the State of Rhineland–Palatino and the principal investigator of the study (MS). Fifty-seven pharmacies agreed initially to participate and offer PC to their asthma patients for one year. In preparation for the study, at least one full-time pharmacist at each participating pharmacy was trained to provide asthma services. Thirteen hours of training was based on a nationally certified curriculum and a published manual/protocol 19 and comprised the following: medical, pharmaceutical, and pharmacologic knowledge; communication skills; and the use of the study protocol and PC documentation forms.
In addition to the initial training provided, all pharmacies were monitored by a pharmacist based in the city of Trier and employed for this study. This pharmacist visited all practice sites regularly to check for compliance with the study protocol and the documentation forms for PC, minimize missing data, and enhance the documentation of drug-related problems detected and solved. In addition, counseling on-site and via phone/fax was offered from the first day of recruitment until the end of the study. Thus, assistance from the distant research center was limited to supervision of the support pharmacist.
We paid a maximum of £75 (about $100 US) per patient to pharmacists and physicians when data were provided at baseline and after 6 and 12 months.
To be eligible for the study, patients had to be 18–65 years old, have a physician's diagnosis of asthma (confirmed for the study), and give written informed consent. Recruitment was carried out by the participating pharmacists, as well as by the patients’ physicians (84 GPs, internal specialists, respiratory physicians). A list of participating community pharmacies was provided to all physicians’ offices. Eligible patients were asked during a regular visit to the pharmacy or physician whether they were interested in joining the program. In addition, an advertisement in the local newspaper helped with recruiting patients. The enrollment time period lasted from October 2001 until March 2002.
DATA COLLECTION AND INTERVENTIONS
In Germany, this type of research does not require an institutional review board approval. However, the work was conducted in compliance with the requirements of the data protection agencies of the health insurance funds involved.
Except for explicitly assessing readiness for change, all elements of PC, as described by Strand et al. 20 and highlighted recently by McLean and MacKeigan, 21 were included in our intervention. In cooperation with the patients’ physicians, 5 meetings between pharmacists and patients were scheduled over 12 months. These one-to-one counseling sessions took place in confidential areas or counseling rooms available within the pharmacy.
Patients were educated in asthma pathology, the use of asthma medication, inhalation technique, and self-management skills. Drug-related problems were detected and solved. At the beginning of the study, each patient was instructed to use a peak flow meter (Mini-Wright, Clement Clarke Int. Ltd., Essex, UK) and a well-recognized asthma diary (Atemwegsliga, Germany) twice daily.
At baseline and after 6 and 12 months, 4 questionnaires were administered to patients during an appointment in the pharmacy. The questionnaires covered the following areas: disease-specific quality of life, generic self-efficacy, asthma knowledge, and adherence. All questionnaires were completed by the patients without the help of the pharmacist. At the same time, patients had to visit their physician to have their lung-function (forced expiratory volume in 1 second [FEV1] and vital capacity [VC]) tested and for reassessment of asthma and dyspnea severity.
In addition to these study data, 2 German statutory health insurance funds (Allgemeine Ortskrankenkasse (AOK) in Rhineland-Palatino, and Barmer Ersatzkasse) provided 2 years of claims data for their insured patients (n = 55, 17 male) for the one-year period before the study and the study year. These patients signed a specific consent form to allow disclosure of their records. Statutory health insurance data about patients’ asthma-related hospital admissions (International Classification of Diseases [ICD] J 45 and J 46), absence from work, and drug consumption were evaluated in this subgroup. Control patients (n = 550) were identified by asthma diagnosis (ICD) and prescriptions of anti-asthmatics (Anatomical Therapeutic Chemical [ATC] code: R03) in a sample of the AOK in the Federal State of Hesse. Patients diagnosed with COPD were excluded. Control and intervention patients were matched by a ratio of 10:1 according to gender, age (± 5 y), date of recruitment, and amount (defined daily doses) of prescribed anti-asthmatics (ATC R03).
OUTCOME MEASURES
To monitor lung function, FEV1 and VC were measured by patients’ physicians at baseline and after 6 and 12 months. In case of insufficient, incorrect, or incomplete data, physicians were asked to provide flow volume curves. These data were reassessed independently by 2 experienced chest physicians. In addition, patients were asked to measure peak expiratory flow rates twice daily at home during the entire study year and on consulting dates in the pharmacy. The peak flow measures under pharmacists’ supervision were recorded in the monitoring plan. To assess dyspnea severity, physicians used the Medical Research Council Dyspnoea Scale (Medical Research Centre of Great Britain, none = 0 to severe = 4). Asthma severity was classified according to German Asthma Guidelines (from intermittent = 1 to severe, persistent = 4). 22
A 7-point checklist was used to score patients’ inhalation technique. 14 For each correct step, 1 point was assigned, and the total score of the inhalation technique was documented. The validated German version of the Living with Asthma Questionnaire was applied to measure asthma-specific quality of life.23,24 A self-constructed self-efficacy scale based in parts on a standardized generic self-efficacy questionnaire 25 and supplemented by some disease-specific items 14 was employed to investigate any changes in patients’ perceptions of their self-management skills and ability to deal with the disease.
The asthma knowledge questionnaire, which focused on basic information about the disease and drug therapy, was developed and tested in cooperation with respiratory physicians, clinical psychologists, and clinical pharmacists involved in the German PC efficacy study. 14 To measure patients’ adherence, the validated 4-item Morisky medication adherence scale was utilized. 26
GKV information about patients’ asthma-related hospital admissions (ICD J 45 and J 46), absence from work, and drug consumption (ATC R03) were evaluated in a subgroup of 55 patients of the intervention group for whom claims data were available and compared with a control group of 550 patients.
STATISTICAL ANALYSIS
Statistical computations concerning clinical and humanistic outcomes were performed using SAS version 8.2 (SAS Institute, Cary, NC). The medial trend of the intervention over time was evaluated using a pre/post/follow-up design (SAS, procedure “mixed” for repeated measure in a split-plot design). 27 This type of ANOVA outperforms the standard General Linear Model approach in terms of power and flexibility of coding single contrasts. Furthermore, it allows for explicit modeling of covariance structure over time, thus giving appropriate standard error for determining statistical significance of effects. Every analysis was replicated using its nonparametric counterpart (Friedman test), which displayed parallel results. Two-tailed a level was predetermined on a = 0.05 with power (1-β) = 0.8.
All scales and subscales derived from the repeatedly administered questionnaires (quality of life, self-efficacy, knowledge) were linearly transformed to a percentage scale ranging from 0 to 100. Low values are associated with a low characteristic of the measured construct and vice versa.
GKV (AOK and Barmer) data were evaluated using a pre/post-design (1-y periods prior to and during the study) against a control group generated from AOK data in the Federal State of Hesse. There was a need to control for the amount of drugs prescribed before baseline and avoid potential bias with regard to anti-asthmatics prescribed to patients enrolled in the study. This was achieved by analyzing individual drug consumption in time frames of 180 days before and during the study (Figure 1, Table 1) instead of analyzing the entire data set.
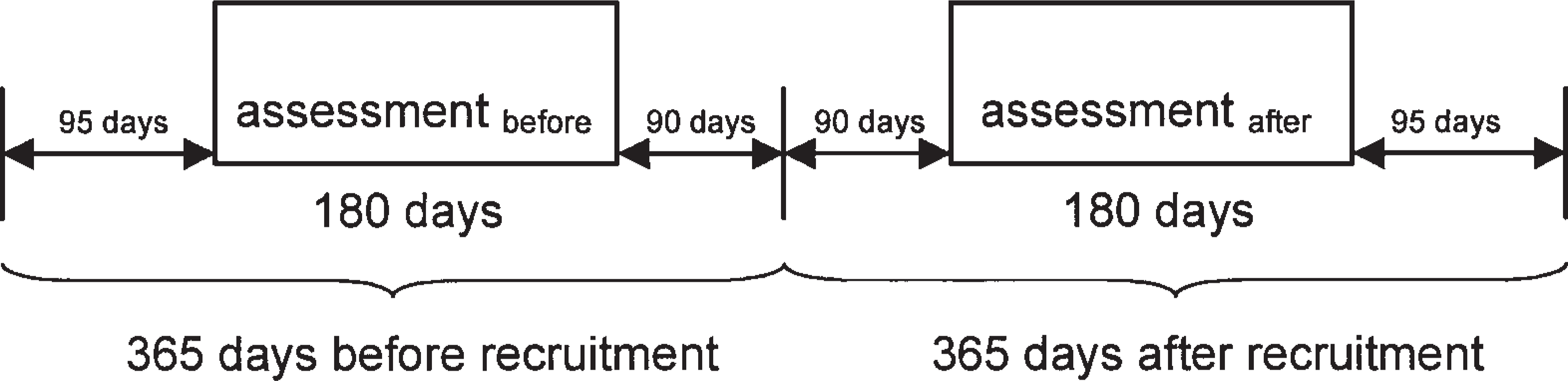
Time-frame assessment claims data.
Relative Change in Number of Receivers of Prescribed Medication a
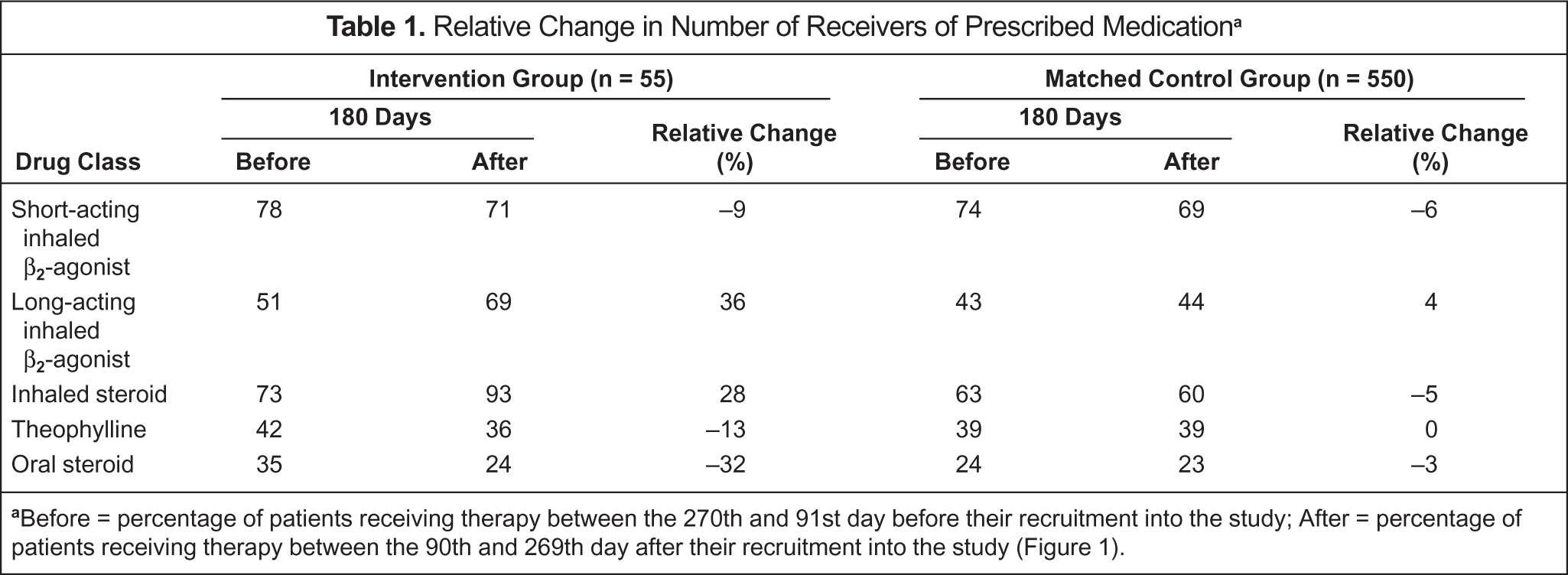
Before = percentage of patients receiving therapy between the 270th and 91st day before their recruitment into the study; After = percentage of patients receiving therapy between the 90th and 269th day after their recruitment into the study (Figure 1).
Results
Over the enrollment period of 6 months, 39 of 57 pharmacies recruited a total of 183 patients. Females were slightly older than males (44.2 vs 41.1 y). Patients’ baseline characteristics are summarized in Table 2. During the study year, 6 (15%) pharmacies and 55 (30%) patients were eventually lost to follow-up. Reasons for patients’ dropout were lack of interest/lack of time (n = 17), patients diagnosed with COPD based on lung function tests and other patient data (n = 6), relocation (n = 4), physician related (n = 2), and pharmacy related (n = 4). No specific reason was filed for 22 patients. Pharmacy dropout was mainly due to change of working place of the responsible and trained pharmacist or when all recruited patients of the pharmacy were lost to follow-up.
Baseline Data of Study Population a
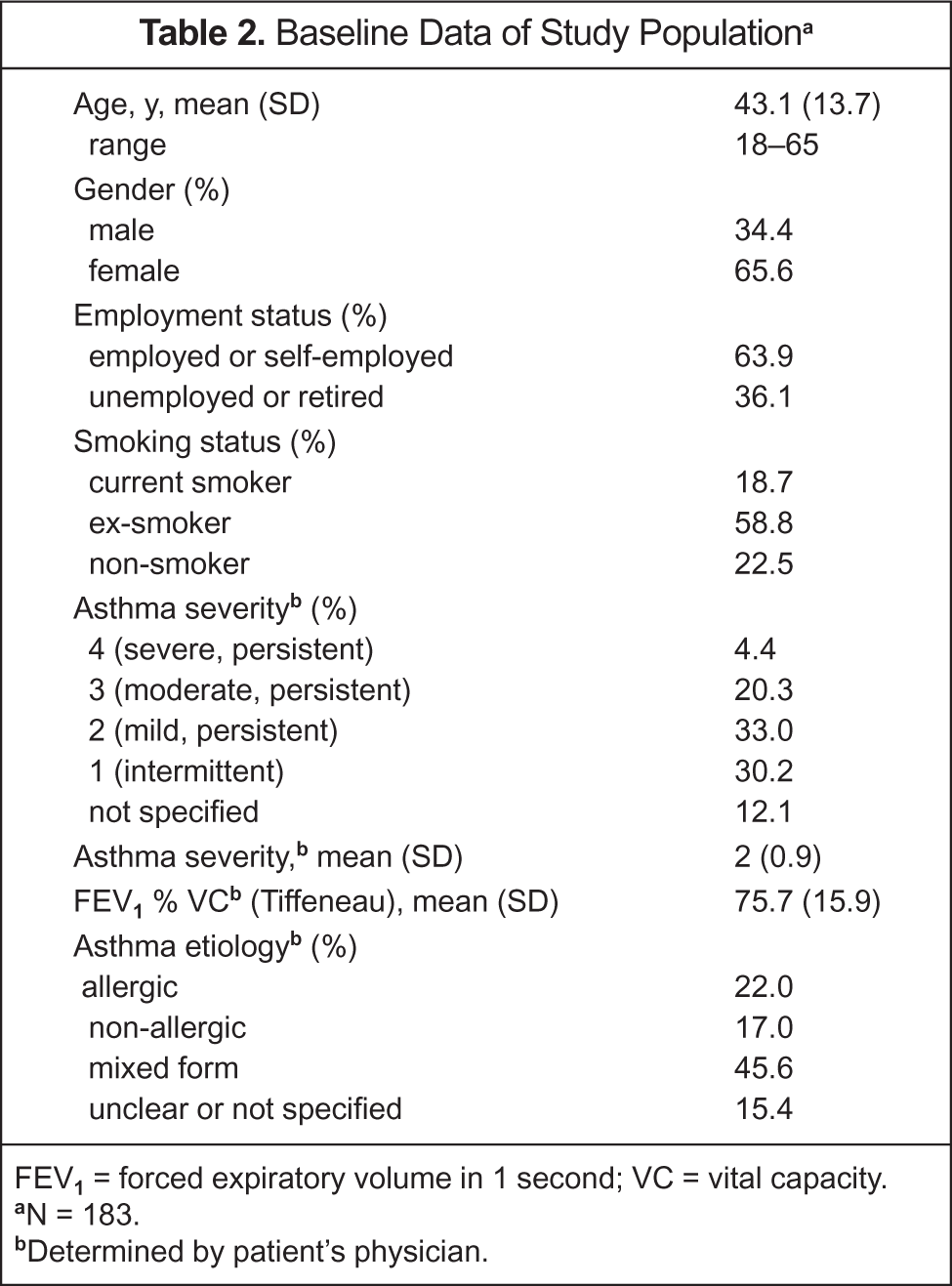
FEV1 = forced expiratory volume in 1 second; VC = vital capacity.
N = 183.
Determined by patient's physician.
CLINICAL OUTCOMES
Peak expiratory flow rates measured in the pharmacy improved significantly over time. In addition, the patients’ self-reported symptoms and asthma severity decreased significantly. Increases in lung function (FEV1 and VC) were not significant over time (Table 3).
Clinical and Humanistic Outcomes a
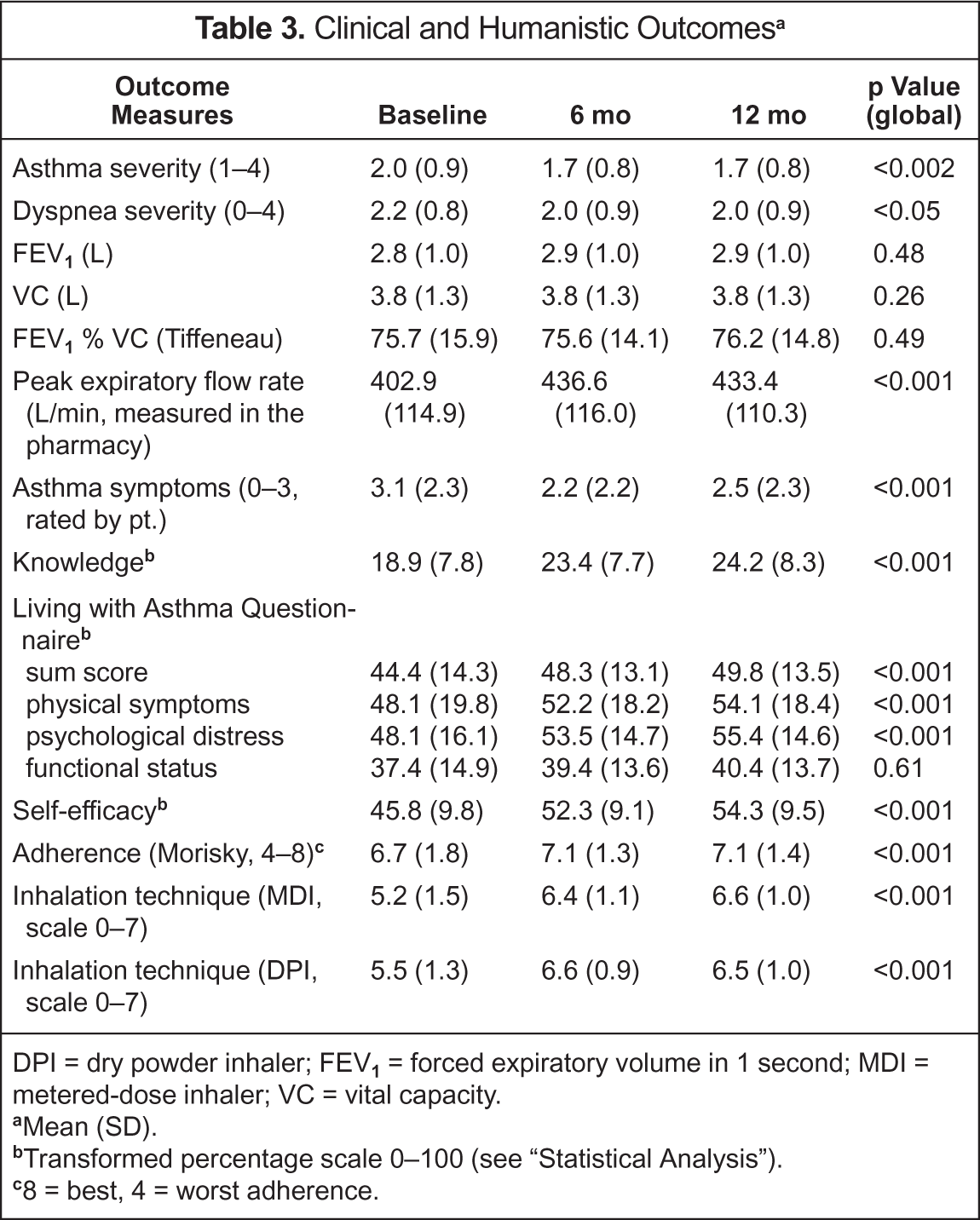
DPI = dry powder inhaler; FEV1 = forced expiratory volume in 1 second; MDI = metered-dose inhaler; VC = vital capacity.
Mean (SD).
Transformed percentage scale 0–100 (see “Statistical Analysis”).
8 = best, 4 = worst adherence.
HUMANISTIC OUTCOMES
The inhalation technique improved significantly over time. Furthermore, patients' knowledge, self-efficacy, and adherence were enhanced. Significant improvements could also be established in the summary score of the Living with Asthma Questionnaire and its 2 subscales: physical symptoms and psychological distress. The functional status subscale remained unchanged (Table 3).
ECONOMIC OUTCOMES
Equivalence tests revealed no statistically significant differences in any of the parameters of the subgroup of 55 patients for whom health insurance funds’ claims data were available compared with the entire intervention group. We therefore concluded that the subgroup is representative of the intervention group.
Evaluation of the claims data showed a higher increase in the number of recipients of long-acting β2-agonists and inhaled steroids in the subgroup compared with the control group (Table 1). Concurrently, a larger decrease in prescribed short-acting inhaled β2-agonists and oral steroids was observed. The number of prescriptions for theophylline remained unchanged in the control group and decreased in the study group.
Low overall asthma severity at/before baseline accompanied by low hospitalization rates in the preceding year and the small number of patients for whom health economic data (hospitalizations, absence from work) were available did not allow further analysis of economic outcomes.
Discussion
As the efficacy of PC has been proven before,10,11,14–16 we chose a more naturalistic pre/post-design with repeated measurement, despite known limitations in its internal validity. In contrast with other studies,10–14 this intervention focused not only on clinical and humanistic outcomes, but also on quality of medical care and economic outcomes.
The 30% patient dropout rate is comparable with the 28% rate found in our controlled study 14 and less than that in the study by McLean et al. 16 The small changes in FEV1 and VC are also consistent with the results found in other studies. 28 Obviously, the variable nature of clinical measurements, especially in multicenter studies without validation of the measurement procedure, is a limitation in evaluating clinical outcomes in a field study like this. Nevertheless, it is known that patients with asthma enrolled in a PC program perceive progress in symptoms and their well-being. This benefit of PC is also clearly supported by our findings. Self-reported symptoms and peak flow measurements (+30 L/min) under pharmacists’ supervision improved significantly over time. Most notably, the significant decrease in asthma severity rated by the patients’ physicians can be interpreted as a result of the intervention.
All humanistic parameters improved significantly. One of the most important conditions for patients’ ability to affect the course of their disease is a high level of self-efficacy and adherence.29,30 Therefore, the improved self-efficacy and adherence we noted can be regarded as the most fundamental results. The enhancement in self-management demonstrated by higher knowledge, self-efficacy, and inhalation technique might have led to the positive impact on adherence and quality of life. Patients who know more about the disease and drug therapy and perceive more control of their asthma are better prepared to cope with the burden of their disease.31,32 Given the importance of patient education in affecting the outcomes of persons with asthma, even small improvements in the knowledge score, as in our study, are relevant.
Although there is only a low correlation between increases in quality of life and lung function in patients with asthma,33,34 the subscales of the Living with Asthma Questionnaire show a clear relationship to asthma severity. 35 Consequently, it is likely that the increase in quality of life indicates a reduction in asthma symptoms. The need for education by healthcare professionals has recently been highlighted again, showing similar deficits in patients’ inhalation techniques for both pressurized metered-dose and dry powder inhalers. 36
Concerning the evaluation of economic outcomes, GKV claims data from only 55 patients insured within the 2 cooperating statutory health insurance funds (AOK and Barmer) could be analyzed. Because of the rather low asthma severity of these patients and an unexpectedly low asthma-related hospitalization rate, an interpretation of changes in hospitalization and in days of disability/absence from work was not possible. Furthermore, information on total healthcare costs was not available.
An analysis of shifts in prescribed pharmacotherapy showed promising results. The higher treatment prevalence with long-acting β2-agonists and inhaled steroids in the intervention group compared with the controls without an increase in asthma severity indicates an improvement in the quality of care.
Furthermore, the higher decrease in prescribed short-acting β2-agonists and oral steroids in the intervention group emphasizes the achieved humanistic and clinical results of the study.
In this study, patient and healthcare practitioner satisfaction was not systematically explored. Not surprisingly, patient satisfaction in PC programs is usually high.10,37 Both pharmacists and physicians reported an overall high patient satisfaction with the service. This is despite the lack of time/lack of interest to comply with all scheduled appointments, completing questionnaires, self-monitoring, and documenting peak flow and symptoms, among others.
For the first time in Germany, both physicians’ and pharmacists’ associations jointly and officially supported a PC program. Moreover, for the first time, health insurance funds provided claims data to evaluate such a program in more detail. Eventually, this cooperation was pivotal for institution of the first German integrated care contract signed in December 2004 between physicians’ and pharmacists’ associations and one of the participating health insurance funds (Barmer). This contract established the combined family pharmacy–family physician concept where patients choose and enroll in both a physician's (GP) office and a community pharmacy.
Conclusions
The findings of our study show that an intensive cooperation between pharmacists, physicians, and patients with asthma within the concept of PC has a clear positive impact on humanistic and, to some extent, on clinical outcomes. In particular, the factors that affect patients’ self-management also improved. In cooperation with the prescribing physicians, drug therapy changed toward evidence-based guidelines. To evaluate potential economic benefits, future research should focus on patients with more severe or uncontrolled asthma, such as those with a significant number of emergency department visits or hospitalizations.
Footnotes
Acknowledgements
We thank the participating patients, community pharmacists, and physicians who made this research possible. Special thanks go to Hartmut Schmall PhD, Carl-Heinz Müller MD, Bernd Krönig MD, Walter Bockemühl, Silke Klein, Klaus Richter, Juergen Tiburzy PhD, and to our monitor, Elisabeth Bläsius-Hilgers BSPharm, for their dedication, as well as to the advisory board of the data sample AOK Hessen/KV Hessen for providing their data.