
Abstract
Objective:
To review the efficacy and safety of vasopressin in cardiac arrest.
Data Sources:
MEDLINE, EMBASE, and PubMed were searched (all to June 2005) for full-text English-language publications describing trials in humans. Search terms were vasopressin, epinephrine, adrenaline, heart arrest, cardiac arrest, and clinical trial.
Study Selection and Data Extraction:
Prospective, randomized, controlled trials that evaluated efficacy or safety endpoints of vasopressin in the management of cardiac arrest were included. Efficacy outcomes included return of spontaneous circulation, successful resuscitation, survival to hospital admission, 2hour survival, and survival to hospital discharge. Safety outcomes were as defined by each trial.
Data Synthesis:
Three prospective trials were identified and included in this review. Vasopressin does not appear to offer any therapeutic advantage compared with epinephrine in the treatment of both in-hospital and out-of-hospital cardiac arrest, regardless of the presenting arrest rhythm. Although there is a suggestion that vasopressin may be effective in treatment of asystole, the evidence for this arises from a subgroup analysis that should be viewed as hypothesis generating. There are limited data describing the safety of vasopressin in cardiac arrest.
CONCLUSIONS:
The current evidence for the use of vasopressin in cardiac arrest is indeterminate. Given the similarly equivocal evidence of efficacy for epinephrine, either drug could be considered the first-line agent in cardiac arrest. Placebo-controlled studies with appropriate statistical power are warranted to evaluate meaningful clinical outcomes, such as survival to hospital discharge. Further evaluation of the role of vasopressin in asystolic cardiac arrest and its use in combination with epinephrine is also justified.
Overall, patients experiencing VF have the best prognosis, with survival rates of 4–33%. 3 However, only 1–4% of patents with PEA survive, and those presenting with asystole rarely survive. 3
Reported overall survival from out-of-hospital cardiac arrest varies with location. A recent Canadian study of 5 centers found a range of 4.3–9.0%; however, regional differences in data collection may be a factor in the observed differences. 4 Survival rates as high as 42% have been reported in US centers for the subgroup of patients presenting with VF. 5 It is clear that in-hospital cardiac arrest patients are a different population from the out-of-hospital group, although again a great range exists in the reported survival rates, from a low of 0% to a high of 29%. 6 A recent Italian study suggests that, analogous to the out-of-hospital situation, survival from in-hospital cardiac arrest varies with the rapidity of advanced life support arrival (with survival rates in nonmonitored units 34% vs 10% when the delay to advanced life support was less than vs more than 3 min, respectively). 7
The management of specific cardiac arrest rhythms is based on recommendations from the International Liaison Committee on Resuscitation (ILCOR) and the American Heart Association (AHA). 8 Initial treatment for VF includes cardiopulmonary resuscitation (CPR) and defibrillation followed by the administration of vasopressors and antiarrhythmic agents. Asystole and PEA are initially treated with CPR, epinephrine, and atropine. In all rhythms, but particularly in PEA, there is an emphasis on diagnosing and treating the underlying cause of the arrest.
Despite the lack of human evidence that epinephrine improves outcome in cardiac arrest, it has remained the vasopressor of choice for several decades. Although historically and currently recommended for use in cardiac arrest, epinephrine, either in high or low doses, has not been shown to be effective in cardiac arrest.9–14 In addition to its lack of efficacy, concerns regarding adverse effects such as severe hypertension, myocardial ischemia, and intractable ventricular tachydysrhythmias have prompted the search for new vasopressors to be used in cardiac arrest.9,10
One of the most promising alternative vasopressor agents is vasopressin. Vasopressin is an endogenous hormone that causes profound vasoconstriction when given in supraphysiologic doses. It has the theoretical advantage over epinephrine of increasing oxygen delivery to vital organs without increasing oxygen consumption and worsening ischemia.15–19 In cardiac arrest, lack of perfusion quickly results in acidosis due to anaerobic metabolism and lactate accumulation. In this hypoxic and acidotic state, adrenergic receptors become less sensitive to the vasoconstrictive effects of epinephrine and other catecholamines.9,10 Vasopressin continues to cause vasoconstriction in the presence of acidosis.15–19 Additionally, studies have shown that increased epinephrine concentrations following cardiac arrest are associated with increased mortality, while increased concentrations of vasopressin are associated with improved survival. 20 To date, numerous animal studies have suggested benefits from vasopressin in cardiac arrest in improving return of spontaneous circulation (ROSC, defined as the return of a palpable pulse of any duration), increasing coronary perfusion pressure (CPP), and improving neurologic outcomes. 19 The purpose of this paper is to systematically review the efficacy and safety of vasopressin in cardiac arrest.
Data Sources
A systematic search of MEDLINE, EMBASE, and PubMed (all to June 2005) was performed to identify full-text English-language publications evaluating the use of vasopressin in cardiac arrest. Search terms were vasopressin, epinephrine, adrenaline, heart arrest, cardiac arrest, and clinical trial. Additional published reports were identified through a manual search of references from retrieved articles.
Study Selection
Citations identified following literature review were evaluated independently by all 3 authors for inclusion using title and abstract. If questions remained regarding eligibility for inclusion, the full-text article was reviewed. Only prospective, randomized, controlled trials that evaluated efficacy or safety endpoints in humans were included. Abstracts, case reports, and animal studies were excluded.
Data Extraction
Data elements were evaluated for all trials independently by each author. Primary data elements extracted included study design, patient population, vasopressor and comparator regimens, and clinical outcomes (efficacy and safety). Efficacy outcomes included ROSC, successful resuscitation (as defined by each study), survival to hospital admission, 2hour survival, and survival to hospital discharge. Safety outcomes were also as defined by each trial.
Clinical Trials
The systematic search identified 5 papers,21–25 2 of which were meta-analyses and were excluded.24,25 Thus, 3 randomized controlled trials were included in this review, all of which compared vasopressin with epinephrine (Table 1).21–23
Review of Clinical Trials Evaluating Vasopressin in Cardiac Arrest
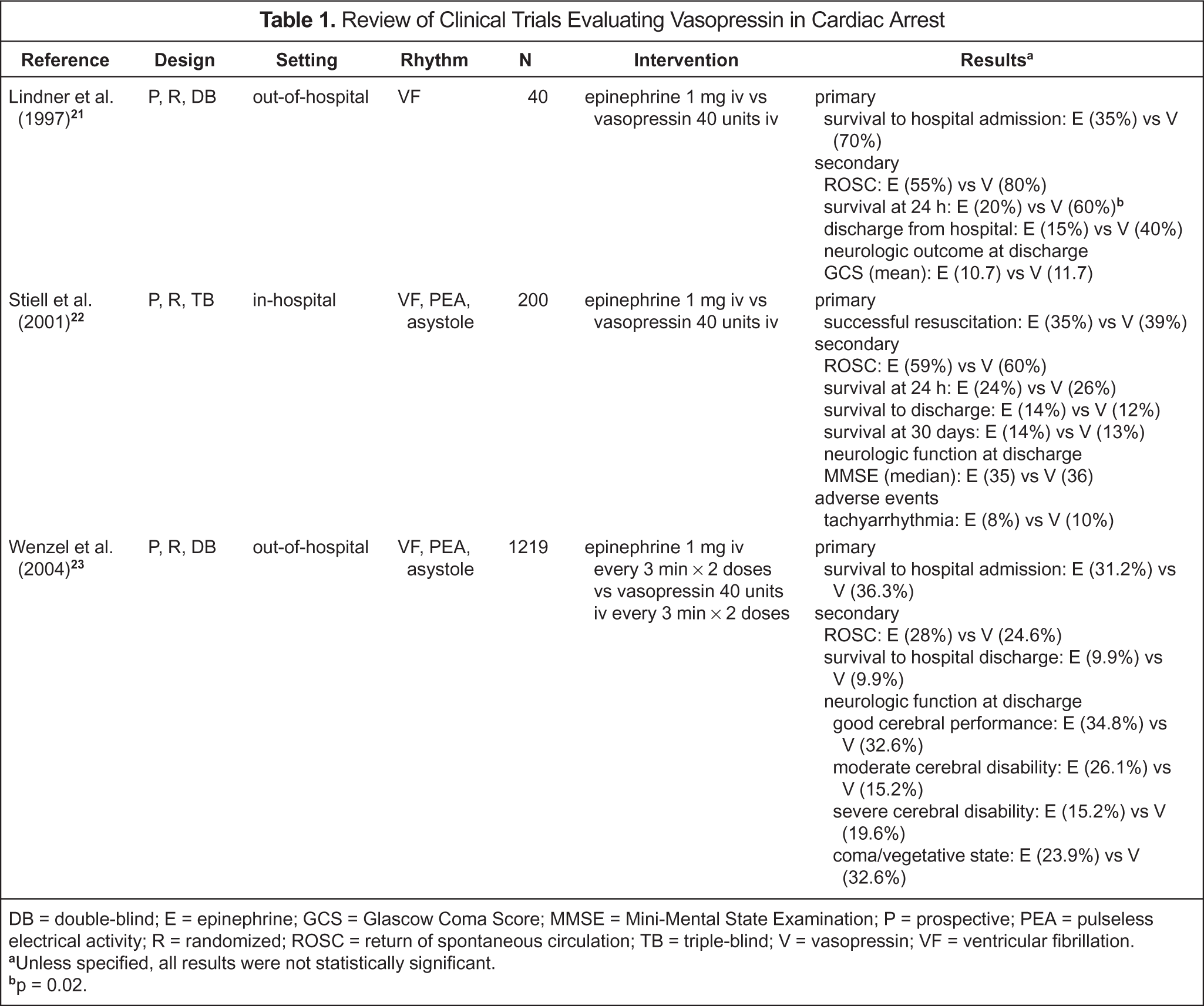
DB = double-blind; E = epinephrine; GCS = Glascow Coma Score; MMSE = Mini-Mental State Examination; P = prospective; PEA = pulseless electrical activity; R = randomized; ROSC = return of spontaneous circulation; TB = triple-blind; V = vasopressin; VF = ventricular fibrillation.
Unless specified, all results were not statistically significant.
p = 0.02.
Lindner et al. 21 evaluated vasopressin in 40 out-of-hospital cardiac arrest patients with shock-refractory VF. Patients were randomized to receive either epinephrine 1 mg or a single dose of vasopressin 40 units intravenously. If cardiac arrest persisted following the administration of study drug and an additional defibrillation, resuscitation was continued according to standard advanced cardiac life support (ACLS) guidelines.26,27 The primary outcome was successful resuscitation, defined as survival to intensive care unit admission without the need for closed chest CPR after ROSC. Other outcomes are shown in Table 1.
Successful resuscitation was achieved in 70% of patients in the vasopressin group compared with 35% of those receiving epinephrine. Survival at 24 hours was achieved in 60% of patients receiving vasopressin compared with 20% of those receiving epinephrine. There were no differences in any other endpoints (Table 1). Adverse effects did not appear to be systematically evaluated; however, a comment in the text of the paper indicated that there were no observed adverse effects. 21
Vasopressin treatment was also evaluated in hospitalized patients with cardiac arrest. 22 Patients experiencing VF, PEA, or asystole were randomized to receive a single intravenous dose of either epinephrine 1 mg or vasopressin 40 units. If treatment failed, resuscitation was continued as per ACLS guidelines, which included additional open-label administration of epinephrine if indicated. 27 The primary outcome was successful resuscitation defined as the continuous presence of a measurable pulse and blood pressure for at least one hour following ROSC. Secondary outcomes are presented in Table 1. Evaluation of adverse events included presence of tachyarrhythmias, uncontrolled hypertension, and mesenteric infarction. Twenty-seven percent of patients randomized were excluded from the analysis as they were subsequently found not to meet inclusion criteria.
Successful resuscitation was achieved in 39% of the vasopressin group and 35% of the epinephrine group. Survival to hospital discharge was 12% in the vasopressin group and 14% in the epinephrine group. There were no clinically or statistically significant differences in any other endpoint or subgroup. The only reported adverse effect was tachyarrhythmias. 22
The largest trial to date, conducted by Wenzel et al., 23 evaluated patients with out-of-hospital VF, PEA, or asystolic cardiac arrest. Patients were randomly assigned to receive epinephrine 1 mg or vasopressin 40 units intravenously. If spontaneous circulation was not restored within 3 minutes, a second dose of the same agent was administered. Additional interventions were at the discretion of the physician managing the cardiac arrest. The primary outcome was survival to hospital admission, while survival to hospital discharge was defined a priori as a secondary outcome.
Overall, there was no significant difference in survival to hospital admission or survival to hospital discharge. There was also no significant difference in either endpoint in the subgroup populations of VF and PEA; however, a difference was found in those presenting with asystole. Asystolic patients treated with vasopressin had a survival to hospital admission of 29% compared with 20.3% in those treated with epinephrine (p = 0.02). There was also a significant difference found in this group in survival to hospital discharge, which occurred in 4.7% and 1.5% in the vasopressin- and epinephrine-treated patients, respectively (p = 0.04). 23
Discussion
Despite numerous pharmacologic and nonpharmacologic interventions since the first description of closed-chest CPR over 4 decades ago, overall survival from cardiac arrest remains low. 3 There is little evidence to support the use of vasopressors in cardiac arrest; however, to date, epinephrine has remained the vasopressor of choice.9,10,21–23 Various doses of epinephrine have been evaluated in a number of placebo-controlled cardiac arrest trials. Unfortunately, despite demonstrating improvements of surrogate endpoints, such as cerebral and myocardial blood flow and ROSC, epinephrine has never demonstrated an improvement in overall survival at any dose studied.9–14 Vasopressin has been studied in both in-hospital and out-of-hospital cardiac arrest and, based on the 3 studies included in this review, there is little evidence to support its use in either location.21–23
Preliminary data in both animals and humans suggested additional benefits of vasopressin over epinephrine in the setting of cardiac arrest. Numerous animal studies found that vasopressin had better outcomes in terms of both ROSC and neurologic outcomes when compared with epinephrine. It was also found to improve CPP and cerebral oxygen delivery compared with epinephrine. The first published report of vasopressin's use in humans was a case series of 8 patients with refractory cardiac arrest. 28 Multiple doses of vasopressin were used at different intervals, and ROSC was achieved in all patients. Three patients were discharged from the hospital with intact neurologic function, while the remaining 5 patients survived for 0.5–82 hours. A prospective, open-label clinical trial of 10 patients evaluated hemodynamic parameters in refractory cardiac arrest. 29 Four of the patients had a significant increase in CPP (mean ± SD, 28.2 ± 16.4 mm Hg); however, no patient achieved ROSC.
In 2000, the AHA/ILCOR ACLS guidelines added vasopressin to the ACLS algorithm for VF. 8 It was given a class IIb recommendation, defined as “safe, acceptable, clinically useful, and considered optional or alternative treatment.” Due to the absence of evidence, epinephrine was classified as class indeterminate. At the time the current ACLS guidelines were developed, only the trial by Lindner et al. 21 had been published. The unpublished results of the study by Stiell et al. 22 were reviewed by the committee, and it was concluded that these data, in combination with animal data and human case reports, were sufficient to merit a class IIb recommendation for use of vasopressin in the ACLS VF guidelines.
Subsequent publication of the studies by Stiell et al. 22 and Wenzel et al. 23 and a recently published meta-analysis 25 have further defined the utility of vasopressin in cardiac arrest. The meta-analysis incorporated the 3 trials presented here in addition to one study published in Chinese with 83 subjects and another with 10 patients published only in abstract form. This meta-analysis concluded that there was no difference between epinephrine and vasopressin in any of the outcomes studied (ROSC, death before hospital admission, death within 24 h, death before hospital discharge, the combination of number of deaths and neurologically impaired survivors).
The meta-analysis had a number of limitations that restricted its usefulness. The analysis was both clinically and statistically heterogeneous, combining both in-hospital and out-of-hospital cardiac arrests. A significant amount of data was missing, which excluded trials from numerous analyses, limiting the interpretation of the results. Although the studies were weighted, the largest trial 23 influenced the results, which raises questions about the utility of performing a meta-analysis.
Asystole is the most refractory cardiac arrest rhythm and usually results in death. Therefore, the positive results reported by Wenzel et al. 23 in the subgroup of 528 asystole patients receiving vasopressin were both surprising and encouraging. These results led to the simultaneous publication of a controversial editorial in the New England Journal of Medicine 30 along with the Wenzel et al. study, which called for the immediate incorporation of vasopressin into existing asystole resuscitation guidelines. However, great caution should be used when interpreting these results, as they arose from a subgroup analysis and thus should be considered hypothesis generating. In addition, it merits noting that there were 29 statistical subgroup comparisons made in this trial, and there were no statistical adjustments for multiple comparisons. It is therefore conceivable that these results simply arose from chance.
There are several limitations to the currently available data. In all 3 trials, a consistent issue was the fact that most patients received epinephrine at some point in their arrest, even if randomized to the vasopressin group. By design, the intervention compared 1 or 2 doses of vasopressin with epinephrine and, if there was failure, treatment was to continue according to standard ACLS guidelines, which included additional doses of epinephrine every 3–5 minutes. There are animal data suggesting that the combination of vasopressin and epinephrine may increase CPP more than either drug alone. 31 Rates of epinephrine use in the vasopressin group were not reported by Lindner et al. 21 ; however, 87% of patients in the study by Stiell et al. 22 and 63% of those in the Wenzel et al. 23 study received epinephrine after receiving vasopressin. A post hoc analysis of the Wenzel et al. 23 trial suggested that there was improvement in the hospital discharge outcome when the combination was used. Overall survival was 6.2% in patients who received both vasopressin and epinephrine, but just 1.7% in patients who received only epinephrine (p = 0.002). However, 8 of 20 patients in the combination group were left in a coma or vegetative state compared with none of the 5 patients who received only epinephrine (p = NS).
Another issue surrounding the interpretation of these studies is the clinical relevance of the chosen primary outcomes. Both out-of-hospital trials used survival to hospital admission and the in-hospital trial used a successful resuscitation defined as a measurable pulse and blood pressure for at least one hour. The decision to use ROSC or short-term survival as a primary outcome in preliminary cardiac arrest studies is predicated on the assumption that there is a relationship between such outcomes (as predictors of a clinically relevant treatment effect) and survival to hospital discharge (if a survival benefit actually exists). This assumption has never been proven, and it has shown that different commonly reported ROSC definitions lead to strikingly different treatment effect estimates. 32 Survival to hospital discharge with intact neurologic function is clearly the ultimate endpoint; however, given the low baseline survival from cardiac arrest, studies powered to detect a difference in this outcome are often not feasible, as they require thousands of patients.
With the exception of the study by Wenzel et al., 23 the sample sizes of the studies were small. The initial study enrolled only 40 patients. 21 The positive findings of vasopressin in VF in this trial were subsequently refuted by the results of the larger, more definitive study. 23 Although this trial provided more definitive results for the role of vasopressin in the setting of out-of-hospital cardiac arrest, there are still limited data on vasopressin in the setting of in-hospital cardiac arrest. The only in-hospital cardiac arrest study enrolled 200 patients, and a significant percentage (27%) of patients were excluded from the analysis after randomization.
Cost and convenience also merit consideration. Epinephrine is available in a prefilled 1-mg/10-mL syringe, which makes administration during an arrest both easy and efficient. In Canada, each prefilled syringe costs $6.80 ($CAN). Vasopressin is not available as a prefilled syringe and must be drawn up from a vial. The recommended 40-unit dose costs approximately $16.12 ($CAN). The cost difference between the 2 agents is not as pronounced in the US, with each 1-mg dose of epinephrine costing $1.63 ($US) compared with $2.88 for each 40-unit dose of vasopressin.
The international ACLS guidelines (AHA/ILCOR) are being revised, with simultaneous publication in Circulation and Resuscitation scheduled for November 2005. The work sheets developed by international experts using a systematic approach are posted on the AHA Web site for review and comment (www.c2005.org). The work sheets pertaining to the use of vasopressin in cardiac arrest suggest the possibility of a recommendation that vasopressin be considered an alternative to epinephrine for VF and PEA, both with the same level of evidence. While the work sheet authors acknowledge that the evidence for vasopressin's effectiveness in asystole arose from a post hoc analysis, they generally support the use of vasopressin over epinephrine in asystolic cardiac arrest. There also seems to be support for the use of a second vasopressor if the first has failed. Despite this, it remains unclear what the new guidelines will advise.
Summary
The current evidence for the use of vasopressin in cardiac arrest is indeterminate. Given the similarly equivocal evidence of efficacy for epinephrine, either drug could be considered a first-line agent in cardiac arrest. However, epinephrine has logistical advantages and a lower acquisition cost. Although there is a suggestion that vasopressin may have a role in asystole, the evidence for this arises from a subgroup analysis that should be viewed as hypothesis generating. Placebo-controlled studies with appropriate statistical power are warranted to evaluate meaningful clinical outcomes, such as survival to hospital discharge. Further evaluation of the role of vasopressin in asystolic cardiac arrest and its use in combination with epinephrine is also justified.