
Abstract
BACKGROUND:
The New Mexico Pharmaceutical Care Foundation received funding through the Tobacco Use Prevention and Control Program (TUPAC) to provide support for pharmacist-delivered tobacco cessation services. The goal of the program was to increase the availability of tobacco cessation services to residents of New Mexico. Program outcomes are presented, using data from the first 2 fiscal years.
OBJECTIVE:
To assess tobacco quit rates among smokers who participated in the community pharmacist–based program and identify the predictors of quitting at the end of a 6-month program.
METHODS:
Pharmacists, who had received Rx for Change training, provided tobacco cessation services. Patients were scheduled for an initial visit and then were seen at regularly scheduled follow-up visits at 1 month, 3 months, and 6 months from the initial visit. Data collected at the initial visit included demographics, smoking history, and readiness for quitting. Smoking status was collected at each of the follow-up visits. Data were analyzed using SAS (SAS Institute) and STATA (StataCorp LP) statistical software. Tobacco quit rates were calculated at 1, 3, and 6 months. Multivariate regression analysis was performed to assess predictors of quitting. Standard errors were adjusted for repeated observation.
RESULTS:
Data were available for 346 participants. The average quit rate at the end of 6 months was 25%. Significant predictors of quitting were high confidence levels in quitting at baseline, individuals who had first cigarettes at least 30 minutes after waking up, first cessation attempt, and nonwhite patients.
CONCLUSIONS:
A smoking cessation program delivered through trained community pharmacists with prescriptive authority is an effective approach to reducing smoking. Further research should be conducted to compare the effectiveness of pharmacists with that of other providers of tobacco cessation services.
Smoking is a risk factor for many chronic diseases. Smoking-related chronic diseases represent a leading cause of morbidity and mortality in the US.1,2 Tobacco use remains a leading cause of preventable death in the US, with an estimated 443,000 deaths attributable to tobacco occurring each year. 2 Tobacco use–related death and disease creates an enormous cost burden with an estimated $193 billion spent annually in direct and indirect health care costs. 3 The prevalence of smoking in the US is 17%, a rate that, although declining, remains above the goal of 12% established by the Healthy People 2010 initiative. 4 A recent Robert Wood Johnson Foundation report indicates that the prevalence of cigarette smoking in New Mexico is higher than the national average at between 19% and 24%. In addition, the report found that tobacco use is highest among economically disadvantaged individuals with low education and income. 5 To control tobacco use and prevent death, the Centers for Disease Control and Prevention (CDC) developed clinical practice guidelines that recommend intensive interventions by health care providers trained in tobacco cessation methods. 6 Intensive interventions should include the following: assessment of the tobacco user's willingness to quit; a minimum of 4 follow-up sessions that are no less than 10 minutes, and ideally around 30 minutes, in length; and use of a combination of counseling/behavior modification techniques and pharmacotherapy. Smoking cessation rates without intervention have been reported to be 3-5% at 1 year; 7-16% if the smoker undergoes behavioral intervention, and up to 24% when receiving pharmacologic treatment and behavioral support. 7 Even minimal (<3 minutes) tobacco interventions delivered by clinicians have been shown to increase the proportion of smokers who quit from 7.9% to 10.2% (OR 1.3; 95% CI 1.1 to 1.6). 8
The CDC practice guidelines identify pharmacists as one of the health care professionals who should provide these interventions. Pharmacists are ideal advocates for tobacco cessation as a result of their training in pharmacology, accessibility to the public, and availability at the time of purchasing tobacco cessation therapeutic products (over-the-counter and prescription). However, previous evaluations of pharmacist-initiated tobacco cessation clinics have identified several barriers to pharmacist-provided tobacco cessation services. 9 These barriers include pharmacists’ lack of training in behavioral modification techniques and lack of reimbursement for the time needed to provide counseling and follow-up services.
In 2004, the New Mexico Board of Pharmacy (BOP) approved pharmacist prescriptive authority for all Food and Drug Administration–approved tobacco cessation products. Pharmacists exercising prescriptive authority are required to complete a BOP-approved tobacco cessation training program. The current BOP-approved training program is the Rx for Change curriculum developed by the College of Pharmacy at the University of California–San Francisco. 10 In order to increase the number of pharmacists providing tobacco cessation services and to address previously identified barriers, the New Mexico Pharmaceutical Care Foundation received funding in 2005 through the Tobacco Use Prevention and Control Program (TUPAC) sponsored by the New Mexico Department of Health and Human Services. This funding was to provide support for pharmacist-delivered tobacco cessation services to the underserved New Mexico population. The goal of the program was to increase the availability of tobacco cessation services to residents of New Mexico and promote quitting among adults and youth who use tobacco. Through TUPAC funding support, the Rx for Change curriculum was provided to community pharmacists at various locations throughout the state of New Mexico. The training consisted of an 8-hour live workshop in which the following topics/activities were covered: epidemiology of tobacco use, including New Mexico statistics; formulations of tobacco; principles of addiction; pharmacology and therapeutics of tobacco cessation products; assisting the patient to quit (motivational interviewing and transtheoretical model of change); patient interview demonstration; pharmacist role playing exercises; patient documentation; and billing for services. In addition to the pharmacist training workshops, the TUPAC funding allowed for reimbursement to pharmacists who provided tobacco cessation services for up to 200 patients per year. Both of these interventions address the barriers identified for pharmacists providing tobacco cessation services. 9 Limited funding was provided to support the purchase of tobacco cessation products as needed for each patient.
We present the findings from the first 2 fiscal years of the TUPAC-sponsored community pharmacist–based tobacco cessation program. The primary objective of this analysis was to assess tobacco quit rates among a convenience sample of smokers who participated in this intensive intervention by community pharmacists trained in smoking cessation. The secondary objective was to identify the predictors of quitting among the program population.
Methods
Data available for analysis were derived from the fiscal years 2004-2005 and 2005-2006. In each year, a convenience sample of approximately 200 patients was enrolled across 15 pharmacies located throughout New Mexico. Participating patients were identified through one of several methods: (1) identification of current smokers by the pharmacist, (2) referral from community partner or other health care provider, or (3) local public service announcements and/or advertising. A total of 12 pharmacies participated in the program during the first 2 fiscal years for which the data are available. Pharmacists who had completed the BOP-approved Rx for Change curriculum provided the cessation program services with administrative and clerical support provided by pharmacy technicians.
The required tobacco cessation services included an initial minimum 30-minute counseling session in which the patient's current tobacco use patterns were reviewed and his/her readiness for change was assessed. At that time, a determination was made between the pharmacist and the patient as to the best use of prescription and/or over-the-counter medication to aid the patient in tobacco cessation. Based on the patient's social history and other factors, a treatment option was prescribed to patients who were in stage 2 of the transtheoretical model for change or ready to quit in the next 30 days. All pharmacists were taught the same Rx for Change curriculum. The program stresses the pharmacist's best judgment after initial consultation rather than an algorithmic approach. Available options include nicotine replacement therapy (patch, gum, lozenge, inhaler, nasal spray) and varenicline or bupropion.
At the conclusion of the initial session, a quit date was agreed upon and a follow-up visit was scheduled for 1 month after the scheduled quit date. A total of 3 follow-up visits between the pharmacist and patient were to be scheduled (1 month, 3 months, and 6 months after the initially determined quit date). The total counseling time over the course of the intervention was at least 90 minutes. In addition to counseling services, the pharmacist could provide medications without charge to the patient up to a total amount of $137.50. Pharmacists were reimbursed up to a total of $200 for counseling services. Reimbursement for pharmacist counseling time occurred after each patient visit according to the following rates: $75 for the initial visit, $25 for the 1-month follow-up visit, and $50 for each of the 3-month and 6-month follow-up visits. Patients signed a consent form for counseling and did not receive any monetary compensation for their participation; however, they did receive assistance with the cost of tobacco cessation products.
Data, including tobacco use status, were collected through self-administered patient surveys that were provided at each of the specified visits (initial, 1, 3, and 6 months). The surveys used were previously created and validated by TUPAC's antioppression model to promote tobacco cessation. Pharmacists were encouraged to maintain contact with participating patients at the determined follow-up dates even if the patient had discontinued participation in the program, the purpose being to determine smoking status. Data collected on the initial intake survey included demographic information (age, sex, ethnicity, health insurance status, and education level), smoking history, and previous quit attempts and methods (Appendix I, available at www.hwbooks.com/pdf/appendices/P146.pdf).
The patient's readiness to quit and quitting confidence were measured via a 5-point Likert scale. The questions on follow-up surveys were designed to ascertain the patient's current smoking status and tobacco cessation medication use. In addition, the 1-month follow-up survey included the patient's satisfaction with the program services on a 4-point Likert scale. The study was conducted in compliance with the requirements of the University of New Mexico's institutional review board. All available data were entered into an electronic database, using a unique subject number to maintain patient confidentiality. Data were analyzed using SAS 9.1.3 (SAS Institute) and STATA (StataCorp LP) software.
Statistical Analysis
The primary objective of this analysis was to determine tobacco quit rates associated with the community pharmacist–based program. Tobacco quit rates were calculated at 1, 3, and 6 months. Missing data on follow-up were input using the last observation carried forward method; missing values were replaced by the last observed smoking status. 11 Bivariate statistical tests using t-test and χ 2 analysis were performed to assess important demographic and behavioral predictors of quitting at the end of 6 months. Variables with significant differences (p < 0.25) were selected for inclusion in the multivariable model. 12 We used a generalized estimated equation (GEE) to estimate the probability of quitting, as this allows for modeling of binary data while accounting for repeated observations over time. In the GEE, we used a first-order autoregressive correlation structure to account for within-person correlation over time. For this analysis, we only used data from 3- and 6-month follow-up sessions. The dependent variable was whether the respondent used a tobacco product and was coded 1 if the respondent did not use tobacco products and zero otherwise. The following variables obtained at the patient's initial visit were included as covariates: age, ethnicity, sex, education level, how soon after waking the respondent uses tobacco, whether the patient's workplace allows tobacco use, whether the individual has tried quitting in the past, confidence in quitting, and perception of the importance of quitting.
Results
At the end of 2 fiscal years (2004-2005 and 2005-2006), 346 smokers had been enrolled in the program. As with any community-based participatory intervention, a large number of patients were lost to follow-up. Response rates at 1, 3, and 6 months follow-up were 48%, 47%, and 40%, respectively. Patient characteristics at the baseline visit are provided in Table 1. The average age was 46 years (range 14-100) with relatively equal proportions of male and female participants. Our study population was not representative of the New Mexico population, as most participants were non-Hispanic white (76%) and well educated, with 43% having a college degree or higher. Most participants had tried quitting in the past and reported having their first cigarettes within 5 minutes of waking up. Only 28% said that their workplace did not allow tobacco use. One half of the patients indicated that another household member currently used tobacco. At baseline, 50% of participants were confident of quitting and nearly all thought that quitting was important in their lives. In addition, 42% of patients had some form of insurance. The smoking aids most commonly chosen by pharmacists after the intake were over-the-counter products. The most commonly selected products were a nicotine patch, which was recommended approximately 30% of the time, followed by bupropion at 12% and an inhaler at 11%. Bivariate statistics among those who quit smoking and those who did not at the end of 6 months are also presented in Table 1. Individuals without a previous quit attempt and those who were confident of quitting were more likely to be tobacco free at 6 months.
Characteristics at Baseline and at 6 Months
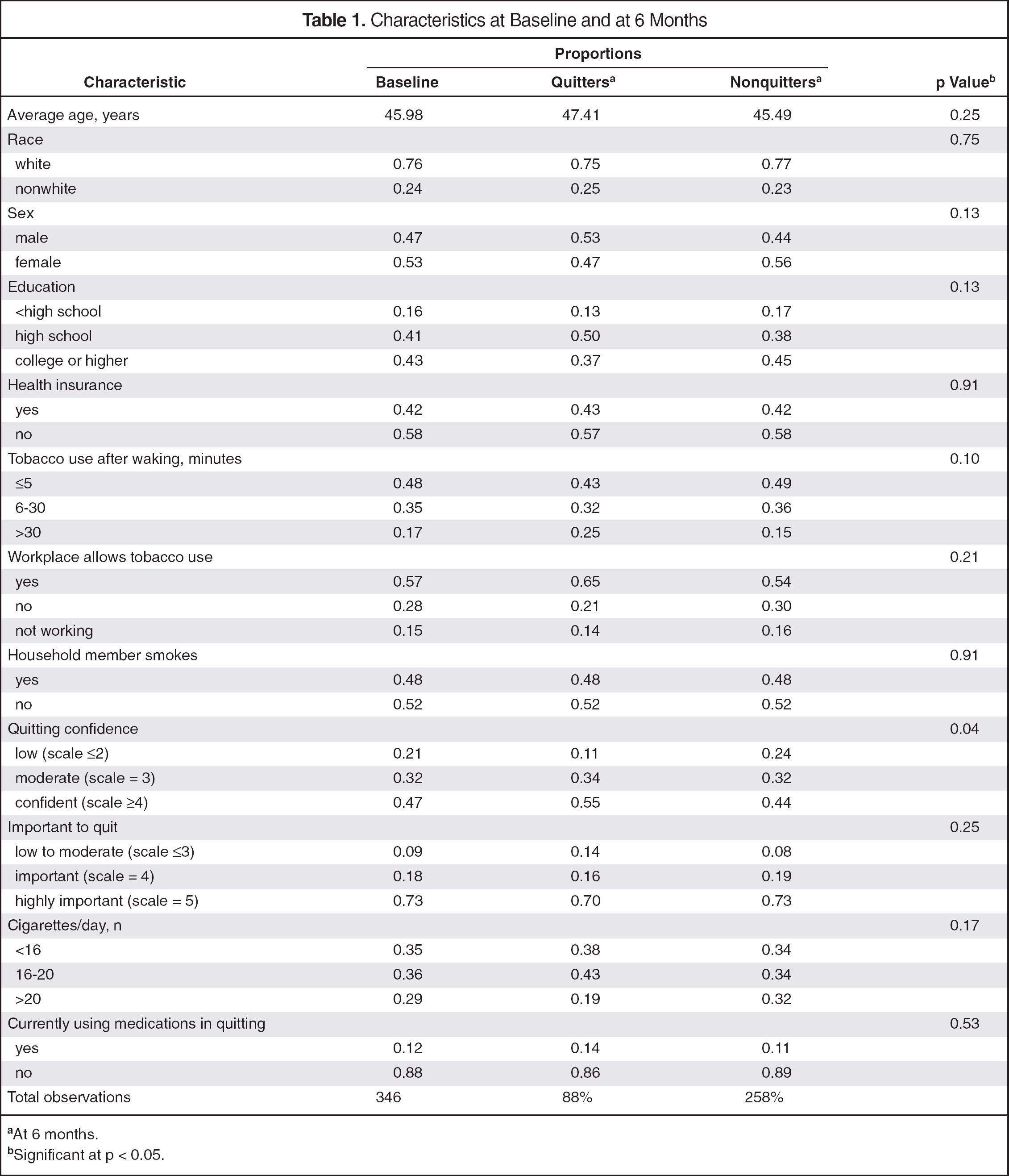
At 6 months.
Significant at p < 0.05.
Quit rates with the intensive intervention at 1, 3, and 6 months were remarkably constant at 25%, 26%, and 25%, respectively. Most participants were satisfied with the program at the 1-month follow-up. Among 146 participants with responses, 71 (49%) were very satisfied, 65 (45%) were satisfied, and 10 (7%) were somewhat satisfied. Predictors of successful tobacco cessation were identified through multivariate analysis. The results, and odds ratios (ORs) with 95% CIs, are presented in Table 2. Age, race, sex, education, workplace influence, and importance of quitting were not significant factors in determining quit rates. Patients who used tobacco within 5 minutes after waking were less likely to quit. Individuals who had previous quit attempts were less likely to quit (OR 0.52, 95% CI 0.27 to 1.00; p = 0.05). Individuals who had high confidence of quitting were more likely to quit. Specifically, the odds of quitting were 183% higher for participants with an initial confidence level of 4 or higher (ie, highly confident) compared with those with low confidence of quitting.
Predictors of Quitting Success
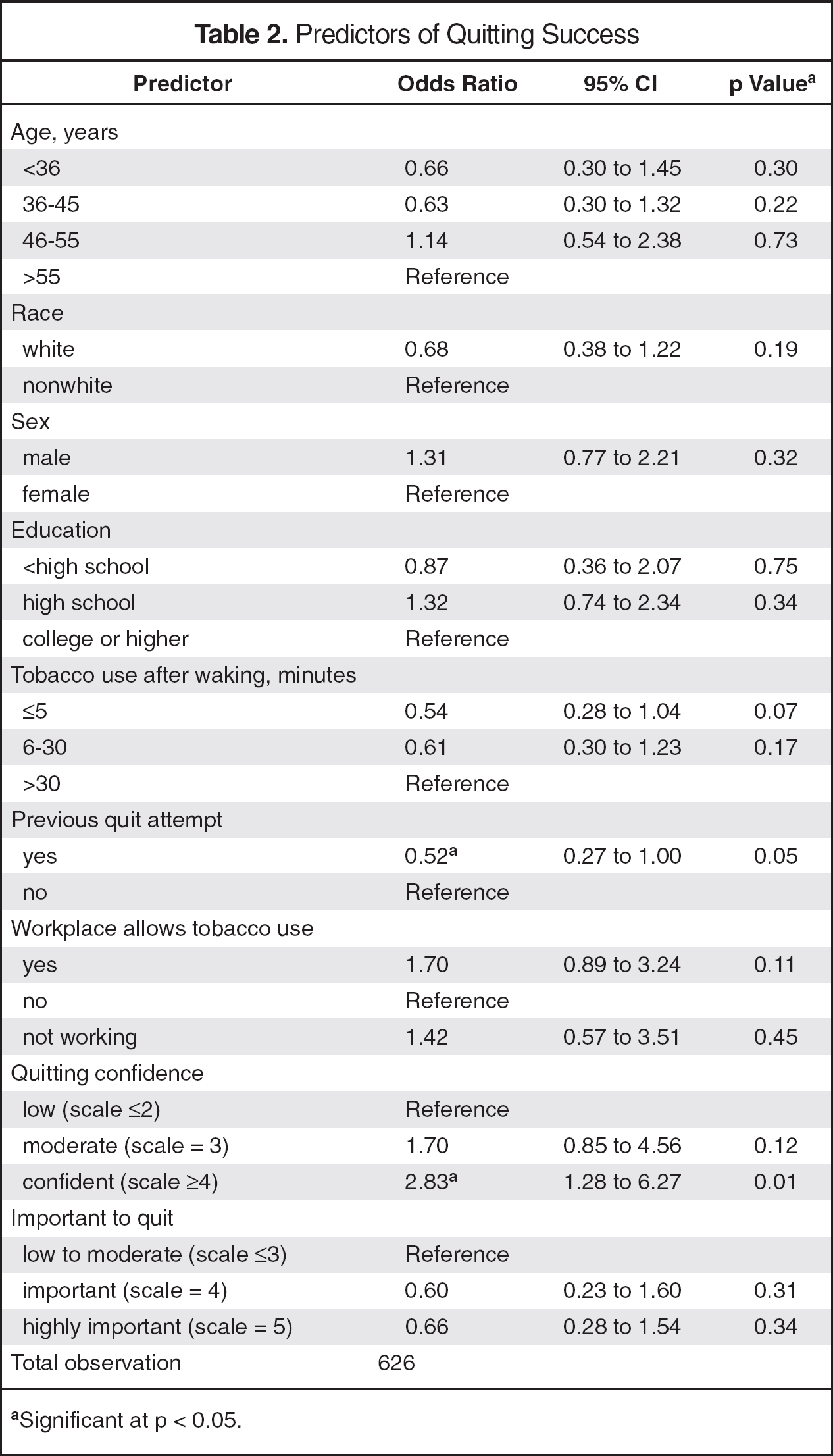
Significant at p < 0.05.
Discussion
Pharmacists are experts in drug therapy, accessible to the public, and available at the time of purchasing pharmacotherapeutic agents for smoking cessation; this makes them suitable advocates for tobacco cessation. 13 Rx for Change is an established curriculum for training pharmacists and pharmacy students in tobacco cessation services including pharmacotherapy treatment and motivation techniques. Results of our analysis indicate that a pharmacist-led smoking cessation program in New Mexico was successful. Average quit rates were 25% at the end of 6 months. These rates are very similar to those of cessation programs headed by other health care providers, including physicians, nurse practitioners, and dentists.13,14 For example, the Finnish Public Sector Study provided that 21% of baseline smokers had quit smoking at follow-up, slightly lower than our results. 15 Studies to date have not directly compared quit rates of interventions between various health care professionals. In our analysis, significant predictors of quitting were high confidence levels in quitting at baseline, first cigarettes at least 30 minutes after waking, and first cessation attempt. Our results suggest that less addicted patients with high confidence levels may have better quit rates with pharmacist guidance and counseling. In addition, patients with higher confidence levels in quitting may have been better able to make the behavioral changes necessary to quit. Patient satisfaction with pharmacist-provided tobacco cessation services was high, with 91% of participants indicating that they were either satisfied or very satisfied with the services provided.
Our study had several limitations. A comparison control group would have strengthened the validity of the success of the program. Without a control group, comparison must be based on published epidemiologic data reports of 3-5% smoking cessation rates without interventions. 7 A large number of patients had missing data on follow-up visits. A total of 346 patients were enrolled in the program; however, data were available for 146 at the 1-month follow-up visit. The last observation carried forward method was used to account for the missing data; however, this may have biased the results toward the outcome. Although patients enrolled in our program were not financially compensated, $137.50 worth of medication could be provided to the patient without charge. The financial compensation may have limited selection to less expensive options, participation in the program, and limited adherence until the funds were depleted. Adherence was not measured; however, patients were counseled by a pharmacist on how to take the medication appropriately. Pharmacists were reimbursed for counseling services, which may have been an incentive to encourage patients to meet prior to their being ready to quit. Lastly, results of our study cannot be extrapolated to rural populations because participants in our study were not representative of the New Mexico population, and many of the participating pharmacies were located in urban rather than rural areas of the state.
Although a few studies have been done to evaluate the effectiveness of pharmacist-led tobacco cessation services, ours is the only one to date evaluating smoking cessation rates with intensive intervention by pharmacists trained in smoking cessation and possessing prescriptive authority.8,16 We also evaluated the predictors of quitting among patients using a prescribing pharmacist to lead their smoking cessation program. The specialized training and a minimum of 90 minutes of counseling over the course of the intervention allowed the pharmacist more time to counsel on cognitive behavioral therapy issues. The extended counseling time also provided the pharmacist with more time to determine which medication would be most appropriate to fit the patient's needs for a more successful quit attempt. The training provided to pharmacists with prescriptive authority in New Mexico may have contributed to the increased rates of success. Because of pharmacists’ prescriptive authority, patients can go to the pharmacist when they feel they are ready to quit without the delay of waiting for an appointment. In addition, if problems or questions arise, the pharmacist is available to make immediate changes without delay or interruption to therapy. Pharmacists can oversee a patient's plan and progress for smoking cessation, and problems can be discovered and dealt with more quickly and effectively. However, an important practical issue to consider is that it is unlikely that pharmacists in the community setting would have the extended time as allowed in this program to assist patients with tobacco cessation. In rural communities such as those in New Mexico, the pharmacist may be the only—or one of a few—health care providers who can provide intervention and guidance on quitting to tobacco users visiting their local pharmacy. Future research should be conducted to compare the effectiveness of pharmacists with other providers of tobacco cessation services.