Abstract
BACKGROUND:
Substitution of generic warfarin for imprint warfarin (Coumadin; DuPont/Bristol-Myers Squibb) has been a controversial issue due to bioavailability and bioequivalence concerns.
OBJECTIVE:
To assess the risk of thrombotic and hemorrhagic events following substitution of warfarin formulations in patients with atrial fibrillation (AF).
METHODS:
Historical cohort analysis was performed using a commercial insurance claims database. Adults with a diagnosis of AF between January 2003 and December 2007, with 16 or more months of continuous eligibility, a warfarin prescription within 30 days after index AF diagnosis, and at least 3 warfarin prescription fills during the follow-up period were included. Individuals with AF diagnosis or warfarin prescription during the pre-index period were excluded. Cox proportional hazard regression models controlling for sex and baseline comorbidities (Charlson comorbidity index, CCI) were used to evaluate the risks of thrombotic and hemorrhagic events following warfarin formulation switches.
RESULTS:
Of 37,756 subjects included in the analysis (mean age 70.96 years, 42.3% females), 12,996 (34.4%) switched warfarin formulations, 20,292 (53.7%) used only 1 generic product, and 4468 (11.8%) used only Coumadin during follow-up. Compared with continued use of Coumadin, switching from that product to the generic formulation was associated with a significantly higher risk of thrombotic events (HR = 1.81; 95% CI 1.42 to 2.31). Similar findings were observed for switching from generic warfarin to Coumadin (HR = 1.76; 95% CI 1.35 to 2.30), and from 1 generic to another generic product (HR = 1.89; 95% CI 1.57 to 2.29). Similarly, switching from Coumadin to generic warfarin (HR = 1.51; 95% CI 1.17 to 1.93), generic warfarin to Coumadin (HR = 1.60; 95% CI 1.23 to 2.1), and from 1 generic to another generic product (HR = 1.74; 95% CI 1.45 to 2.11) were associated with significantly higher risk of hemorrhage than remaining on Coumadin.
CONCLUSIONS:
Switching warfarin formulations exposed patients with AF to a higher risk of bleeding events compared to remaining on a single product. Maintaining patients on a product with consistent bioavailability may optimize the risk-benefit balance of anticoagulation therapy.
The clinical efficacy of warfarin in reducing the risk of ischemic stroke and other systemic thromboembolism in patients with atrial fibrillation (AF) has long been established in clinical trials.1–5 Due to warfarin' narrow therapeutic index, frequent monitoring of prothrombin time and the more standardized international normalized ratio (INR) is required in patients taking warfarin to balance the clinical benefit of ischemic stroke prevention with the risk of bleeding. 6 Extensive data have demonstrated that the risk-benefit balance of warfarin therapy is optimized by maintaining an INR between 2.0 and 3.0.7,8 Warfarin is also highly protein-bound; approximately 99% is bound to plasma proteins. 9 Several factors affect the bioavailability and biouptake of warfarin. Drug interactions may result in variations in the amount of unbound warfarin in systemic circulation, therefore affecting antithrombotic activity.9,10 The most common mechanism for drug-drug interactions with warfarin occurs via altered metabolism in the liver involving CYP2C9, CYP3A4, and CYP1A2 isoenzymes. Other mechanisms also influence the anticoagulant activity of warfarin. Warfarin is highly dependent on vitamin K, an essential cofactor for the clotting cascade. Vitamin K is prevalent in many foods, nutritional shakes, and multivitamins. Inconsistent dietary consumption of vitamin K can result in significant fluctuation in the INR. In addition, an individual' genetics, specifically variations in CYP2C9 and VKORC1 isoenzymes, significantly alters a patient' response to warfarin. 11
For more than 40 years, warfarin sodium was a single-source product marketed by DuPont Pharmaceuticals in the US as Coumadin. Generic formulations have been available in the US since 1997. Presently there are 7 warfarin products available in the US: the reference listed drug (Coumadin; Bristol-Myers Squibb) and 6 generics by other manufacturers (Zydus, USL Pharma, Taro, Pliva, Mylan, and Barr). 12 The Food and Drug Administration (FDA) does not require generic manufacturers to replicate the extensive clinical trials to establish safety and efficacy, but they do require manufacturers to demonstrate bioequivalence to the pioneer drug to receive a bioequivalence (AB) rating. 13 Coumadin and the generic warfarin products, having a narrow therapeutic index, have not been subject to regulatory requirement modifications. This has resulted in variations in bioavailability and a lack of bioequivalence among warfarin formulations, and concerns about the clinical consequences remain.14–16
Several published studies have assessed INR levels before and after treatment is switched from Coumadin to a generic warfarin formulation. Many of these studies, with prospective observational or randomized, single- or doubleblind crossover design and relatively small sample sizes (N = 210 or less), have consistently shown that substitution with either the Barr or Apothecon generic warfarin formulation for Coumadin did not significantly affect INR.17–22 Studies with larger sample sizes yielded somewhat different results.23,24 For example, retrospective analysis was conducted using computerized records of 975 patients from an Israeli health maintenance organization (HMO). 23 The study found that the average warfarin dosage was significantly higher (p < 0.001) and INR level was significantly lower (p < 0.001) during 6 months after a nationwide switch from Coumadin to the Taro generic warfarin formulation. Even among patients whose dose was unchanged (n = 94, 9.6%), there was a significant reduction in median INR level from therapeutic to subtherapeutic level (from 2.2 to 1.7, p < 0.001). 23 Another retrospective analysis was conducted on data from 2299 patients stabilized on Coumadin who regularly visited an anticoagulation clinic affiliated with an HMO in the US. 24 This study found that during the 90 days after switching from Coumadin to the Barr generic warfarin formulation, the INR levels in more patients who had the ratios determined fell below therapeutic range. More than one third (38.9%) of patients had an INR decrease of more than 10% (p < 0.001), 33% of patients had an improvement in INR by 10%, and 28% of patients had a change of less than 10%. The authors concluded that the difference was not clinically significant because the overall numerical difference in the amount of time that INR values were within therapeutic range was small.
Most of the studies published to date have been conducted in anticoagulation clinics, where warfarin therapy is monitored on a regular basis. To our knowledge, all published studies have been limited to assessing outcomes after switching from Coumadin to a single generic formulation and have excluded other types of switching (eg, from 1 generic formulation to another generic formulation). Considering warfarin' narrow therapeutic index and the growing trend of generic drug use, it is important to understand how substituting/switching among the various generic warfarin formulations may affect patient outcomes, when patients may or may not have been under close INR monitoring. The objective of this study was to assess the risk for thrombotic and hemorrhagic events following the switching of warfarin formulations, including switching from 1 generic product to another, within 1 year after diagnosis of AF.
Methods
DATA SOURCE
A historical cohort analysis was performed using the Thomson Reuters Medstat Market Scan Commercial Claims & Encounters and Medicare Supplemental & Coordination of Benefits database (Thomson Reuters, Chicago, IL). The database is Health Insurance Portability and Accountability Act-compliant and consists of integrated enrollment history and medical and pharmacy claims data for more than 94 million patients receiving commercial health insurance benefits through employers. The database has been used for research projects aimed at understanding the costs and patterns of medication utilization in AF.25–29 The study was reviewed and approved by the institutional review board at the University of Utah.
STUDY POPULATION
The study sample comprised adults (≥18 years old) with an index diagnosis of AF as identified by having a medical claim associated with an ICD-9 CM (International Classification of Diseases, 9th Revision, Clinical Modification) code of 427.31 between January 1, 2003, and December 31, 2007. The index date was defined as the date of first diagnosis of AF. Patients were required to be continuously eligible for medical and pharmacy services for at least 16 months (4 months prior to and 12 months after index date). Those who had a medical claim associated with AF diagnosis or had filled a prescription of warfarin during the 4 months before the index AF date were excluded from the analysis to maximize the probability of including individuals who were newly diagnosed with AF. To further confirm that study subjects were receiving ongoing warfarin therapy for stroke prevention in AF, only those who had at least 3 prescription fills for warfarin during the 12-month follow-up period (with the first warfarin prescription filled within 30 days of index AF diagnosis) were eligible for inclusion in this study. The switching pattern of warfarin formulation fills and the risks of thrombotic and hemorrhagic events during the 12-month follow-up period after the index AF diagnosis date were evaluated.
PERIOD OF RISK ASSESSMENT
Figure 1 is a schematic representation of the risk period during which warfarin formulation switching patterns and the occurrence of adverse events were assessed. The 12-month follow-up period began from the index AF diagnosis date. Subjects who filled their first warfarin prescription within 30 days of the index AF diagnosis date were eligible for the analysis. A 30-day warfarin stabilization period was applied after the first warfarin prescription fill to allow for any dosage adjustment/titration that may be required to achieve a stable, initial warfarin treatment regimen. The risk period for the assessment of warfarin formulation switching and occurrence of thrombotic and hemorrhagic events began at the end of the stabilization period and stopped at the end of the 12-month follow-up period. Any thrombotic or hemorrhagic events that occurred during the stabilization period were excluded from the analysis.
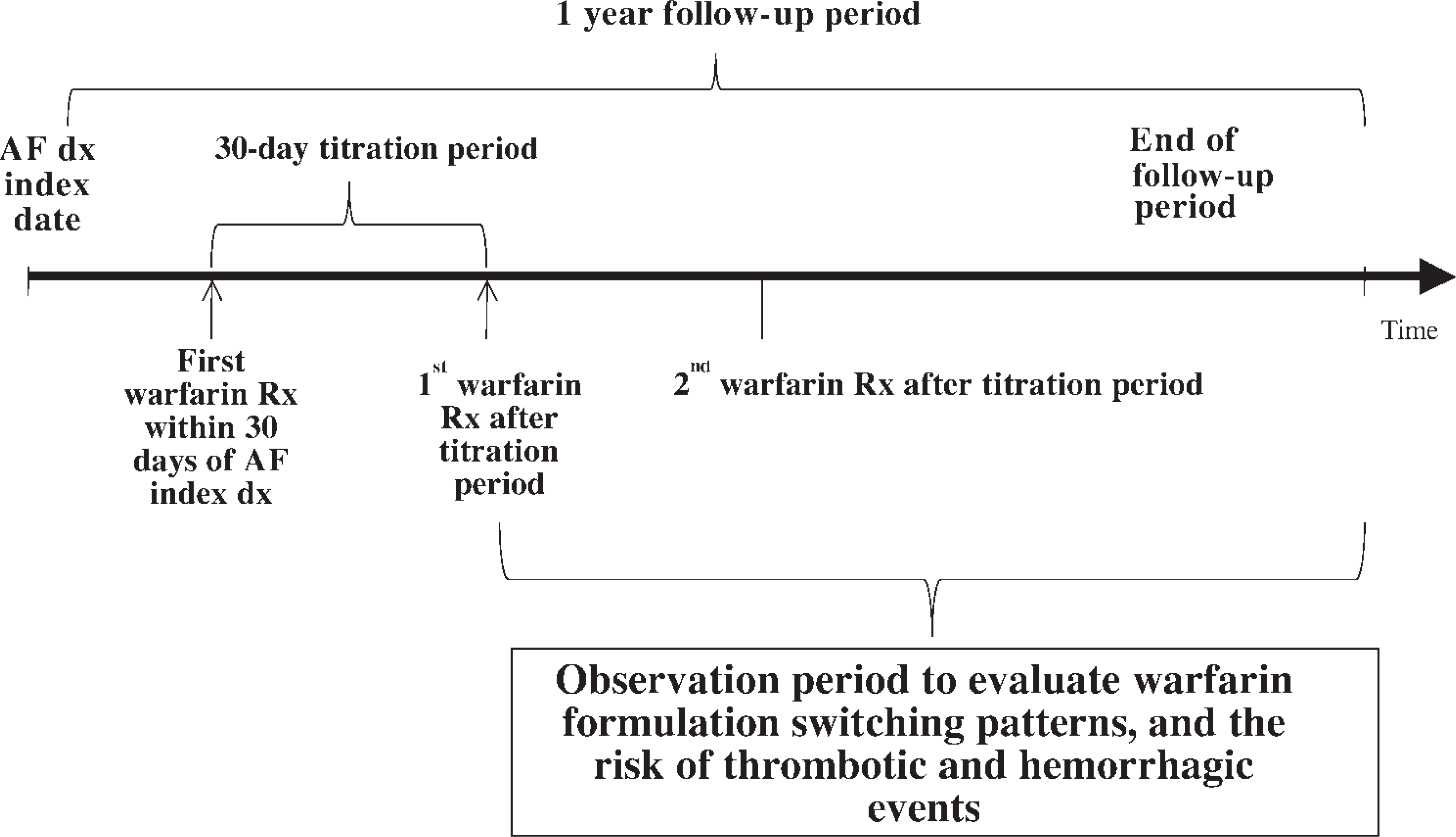
Schematic representation of risk period and identification of adverse events. Not to scale.
KEY VARIABLES
Each warfarin prescription fill during the risk period was categorized as Coumadin or generic warfarin, based on National Drug Code (NDC) code. The Red Book (2008) was used to identify the generic name, brand name, and the manufacturer' name associated with the NDC code of each warfarin prescription fill. 30 Subjects who received Coumadin for all warfarin prescriptions during the follow-up period were classified as Coumadin-only users. Those who received generic warfarin formulations from a single manufacturer consistently during the follow-up period were classified as 1 generic product user. Subjects who received warfarin formulations from multiple manufacturers during the follow-up period were classified as warfarin formulation switchers. Warfarin formulation switchers were further categorized to 3 groups: (1) Coumadin to generic warfarin, (2) generic warfarin to Coumadin, or (3) 1 generic warfarin formulation to another generic formulation, based on the type of warfarin formulation prescription fills observed during the follow-up period. Therefore, there were a total of 5 groups of interest in this study: (1) Coumadin only, (2) only 1 generic warfarin product, (3) Coumadin to generic warfarin, (4) generic warfarin to Coumadin, and (5) 1 generic to another generic warfarin product.
Hemorrhagic adverse events—including major and minor gastrointestinal (GI) bleeding and intracranial (IC) bleeding, as well as thrombotic adverse events including ischemic stroke, pulmonary embolism (PE), and deep vein thrombosis (DVT)—occurring during the risk period were assessed. Major GI bleeding events were defined as GI bleeding that required hospitalization, identified based on inpatient claims associated with an ICD-9 code for GI bleed (Table 131–35). Minor GI bleeding events were defined as GI bleeding that did not require hospitalization, identified by an outpatient claim associated with a GI bleed ICD-9 code in the absence of any inpatient GI bleed claim. A 7-day time period between minor GI outpatient claim and major GI medical inpatient bleeding claim was imposed to differentiate minor GI and major GI as 2 separate events. IC bleeding events were identified by inpatient claims associated with an ICD-9 code for IC bleeding. PE, DVT, and ischemic stroke events were identified by the presence of an inpatient or outpatient claim associated with the corresponding ICD-9 codes shown in Table 1.
ICD-9 Codes to Identify Hemorrhagic and Thrombotic Events
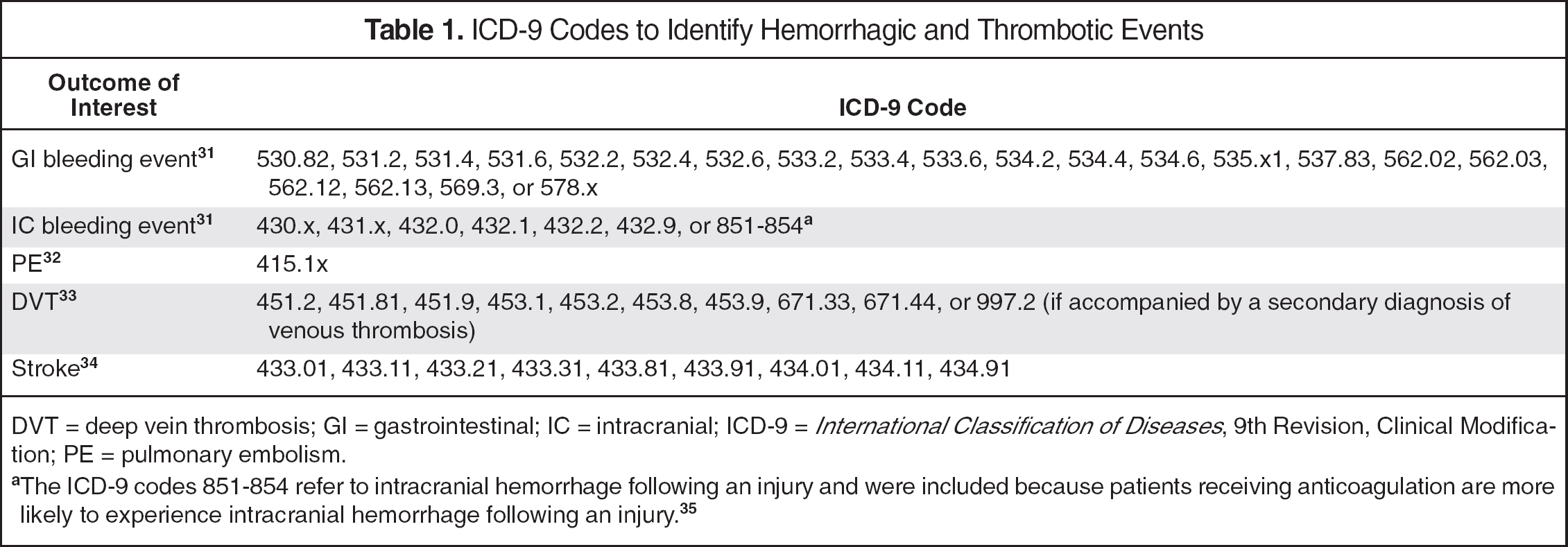
DVT = deep vein thrombosis; GI = gastrointestinal; IC = intracranial; ICD-9 = International Classification of Diseases, 9th Revision, Clinical Modification; PE = pulmonary embolism.
The ICD-9 codes 851-854 refer to intracranial hemorrhage following an injury and were included because patients receiving anticoagulation are more likely to experience intracranial hemorrhage following an injury. 35
STATISTICAL ANALYSIS
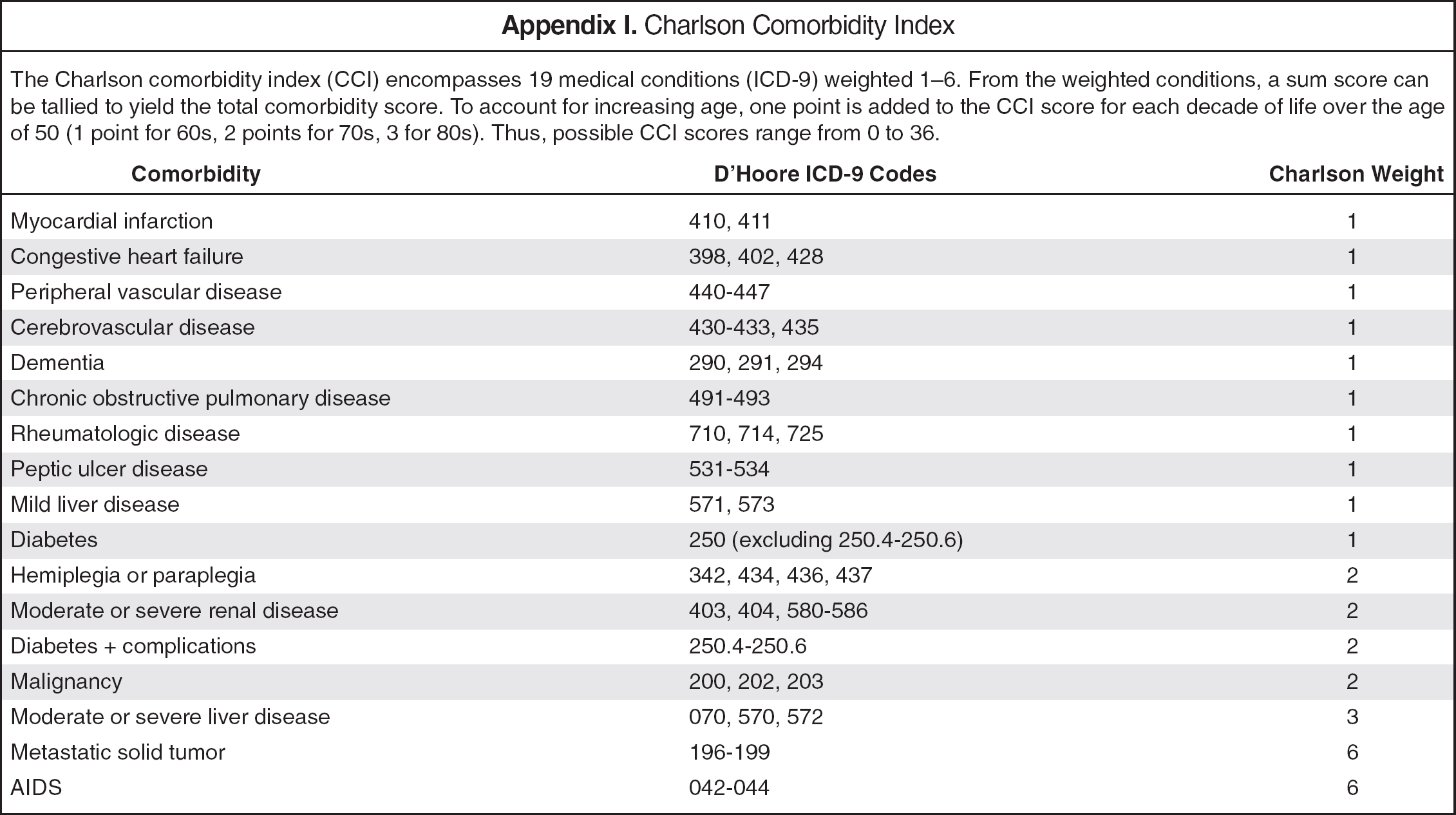
For the purpose of baseline characteristics assessment, subjects were categorized into 3 mutually exclusive groups (Coumadin-only users, 1 generic product users, and warfarin formulation switchers) based on the types of warfarin formulations received during the risk assessment period. Pearson' χ2 test was used to compare demographic characteristics and comorbidities betweens switchers and brand-only users, and between generic-only users, and brand-only users. Baseline comorbidities were assessed using the D'Hoore adaptation of the Charlson comorbidity index (CCI), which assigns a comorbidity score based on a person' age and the ICD-9 codes associated with his or her medical claims during the 4-month preindex period. 36 The CCI score was used in this study because it controlled for preexisting conditions such as prior stroke and peptic ulcer disease that may affect the risk of thrombotic and hemorrhagic adverse events. Baseline characteristics of each group were summarized by descriptive statistics. Appendix I provides details of medical conditions and corresponding ICD-9 codes included in CCI.
Cox proportional hazard regression models, controlling for baseline comorbidities and sex, were used to estimate the risk of having a thrombotic or hemorrhagic adverse event during periods of exposure to a single generic warfarin formulation following switching of warfarin formulations (ie, from Coumadin to a generic warfarin formulation, from a generic warfarin formulation to Coumadin, or from 1 generic warfarin formulation to another generic formulation), relative to staying on Coumadin only. Separate regressions were run for thrombotic and hemorrhagic adverse events. Cox proportional hazard regressions were performed at the level of warfarin exposure, and data were censored at the first occurrence of an adverse event or at the end of the follow-up period, whichever occurred first. Because days of supply information may not consistently reflect the duration of warfarin therapy, person-years of warfarin exposure were calculated by counting the number of days between 2 prescription fills. Time to first adverse event among Coumadin only and 1 generic product users was calculated as the number of days from date of index warfarin prescription to the date of first adverse event. The time to no event in Coumadin and 1 generic product users without adverse event was incorporated into the model as the number of days from date of index warfarin prescription fill to end of follow-up period. Warfarin formulation switchers contributed data to more than one cohort in the regression analysis, depending on the type of warfarin formulations received prior to the first occurrence of adverse event of interest. Switchers were followed after their index warfarin prescription fill through their switch to another warfarin formulation, other than the index warfarin formulation, until they experienced the first adverse event or until the end of the follow-up period, whichever occurred first. If switchers switched formulations with no adverse event prior to the switch, the number of days from index warfarin prescription fill to the date of switch was categorized as time to no event and was classified as belonging to its corresponding warfarin exposure group (Coumadin to a generic warfarin formulation, generic warfarin formulation to Coumadin, or 1 generic warfarin formulation to another generic formulation) depending on the type of switch. Switchers were followed and any subsequent switches were similarly classified to different warfarin exposure groups until an adverse event occurred. The time to first adverse event among switchers was calculated as number of days from the date of the subject' latest switch to the date of the adverse event. The Cox regression analysis was conducted using the robust sandwich estimator of variance (COVSANDWICH option, SAS Institute, Cary, NC) to account for possible correlation between multiple observations contributed by the same subject.
Because age was already part of the CCI score calculation, it was not included as a covariate in the Cox proportional hazard regressions. Unadjusted rates of thrombotic and hemorrhagic events per 100 years of person-years of warfarin exposure were also assessed.
Results
A total of 222,405 adults with AF were identified between January 1, 2003, and December 31, 2007, who did not have prior AF diagnosis or warfarin prescription during the 4 months pre-index period and provided medical and prescription data for at least 12 months following the index AF diagnosis in the Marketscan database. Among these subjects, 37,756 who filled at least 3 warfarin prescriptions during the 12-month follow-up period and received the first warfarin prescription within 30 days of AF index diagnosis were eligible for analysis. Among these subjects, 4468 (11.8%) used Coumadin only, 12,996 (34.4%) switched warfarin formulations (either from Coumadin to generic, from generic to Coumadin, or from 1 generic warfarin product to another) and 20,292 (53.7%) subjects used only 1 generic product during the follow-up period. Among subjects who switched warfarin formulations, 2575 (19.8%) switched from Coumadin to generic warfarin, 1785 (13.7%) switched from generic to Coumadin, and 8636 (66.4%) subjects substituted 1 generic warfarin product for another generic product at least once during the study. Some subjects had multiple warfarin formulation switches during the study.
Demographic characteristics and comorbidities of Coumadin-only users, 1 generic product users, and warfarin formulation switchers are summarized in Table 2. Compared to Coumadin-only users, warfarin formulation switchers and 1 generic product users were older and had a significantly higher proportion of subjects older than 65 years old (p < 0.05). Sex distribution was similar across the 3 groups. There was a significantly higher proportion of fee-for-service insurance subjects among warfarin formulation switchers (57.9%, p < 0.01) compared to Coumadin-only users (49.6%), but the proportion of 1 generic product users with fee-for-service insurance (43.9%, p < 0.01) was significantly lower than Coumadin-only users. Compared to Coumadin-only users (46.6%), the proportion of subjects with managed health plans was significantly lower among warfarin formulation switchers (39.2%, p < 0.01), but the proportion of subjects with managed health plans was significantly higher among 1 generic product users (51.8%, p < 0.01). Both the switching (50.3%) and 1 generic warfarin product cohorts (48%) had a significantly higher proportion of subjects with 3 or more comorbidities (50.3%) than the Coumadin-only cohort (42.9%) (p < 0.01).
Baseline Characteristics and Comorbidities a
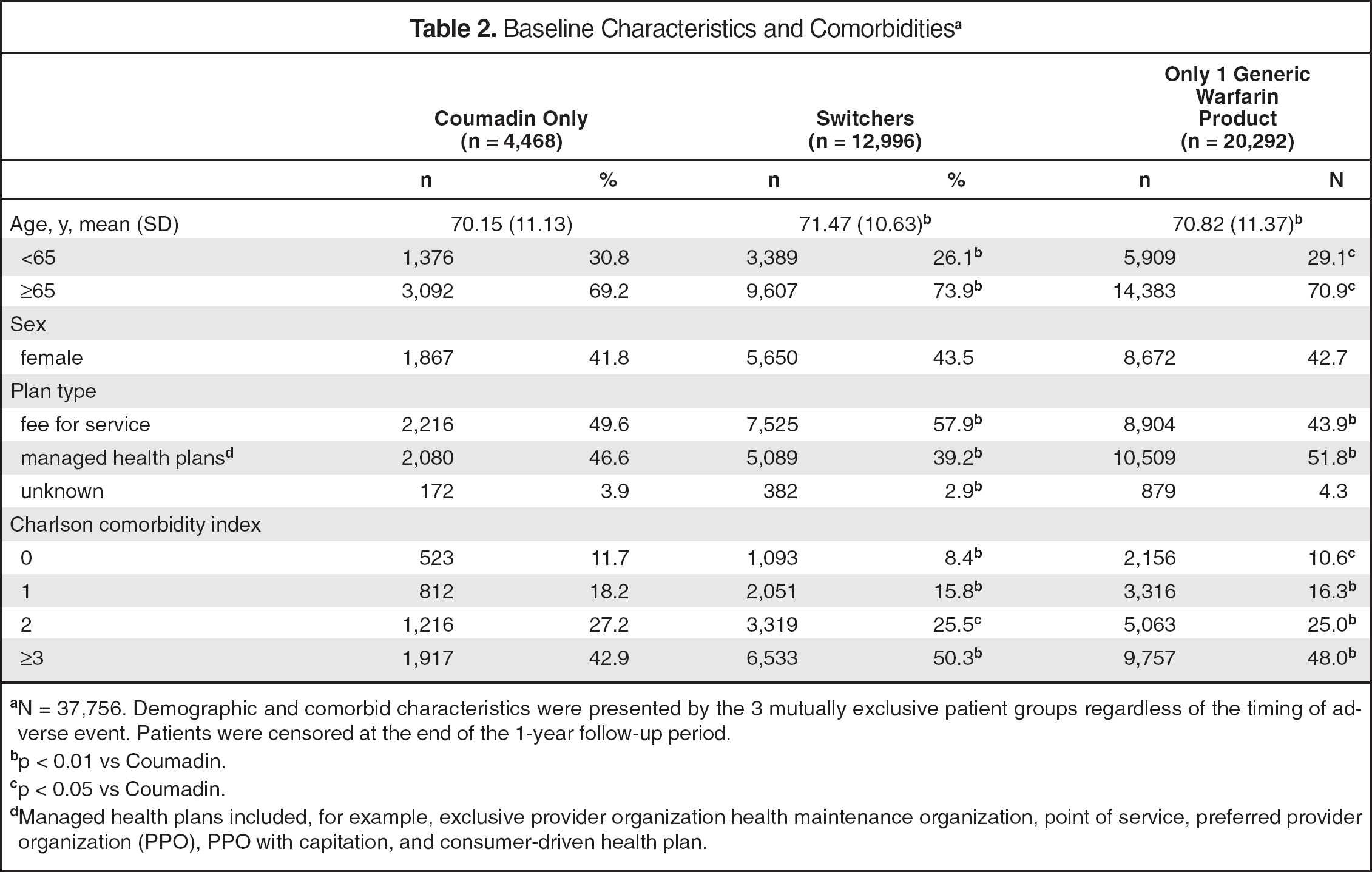
N = 37,756. Demographic and comorbid characteristics were presented by the 3 mutually exclusive patient groups regardless of the timing of adverse event. Patients were censored at the end of the 1-year follow-up period.
p < 0.01 vs Coumadin.
p < 0.05 vs Coumadin.
Managed health plans included, for example, exclusive provider organization health maintenance organization, point of service, preferred provider organization (PPO), PPO with capitation, and consumer-driven health plan.
The number of person-years and unadjusted rate of adverse events are summarized in Table 3. The number of person-years varied by type of adverse event because patients were censored at the occurrence of first adverse event and the time of censoring might be different between thrombotic and hemorrhagic adverse events. The overall unadjusted hemorrhagic event rate across all warfarin formulations was 7.53 events per 100 person-years (1614 events/21,423 person-years of warfarin exposure). The unadjusted rate of hemorrhagic events was numerically highest after switching from generic warfarin to Coumadin (9.3 events per 100 person-years), followed by switching from 1 generic product to another (8.4 events per 100 person-years), switching from Coumadin to generic (8.0 events per 100 person-years), staying on 1 generic warfarin product (7.2 events per 100 person-years), and staying on Coumadin (6.8 events per 100 person-years). Across all warfarin formulations, the overall unadjusted thrombotic event rate was 8.6 events per 100 person-years (1689 events/19,713 person-years of exposure). Switching from Coumadin to a generic warfarin formulation had the highest unadjusted thrombotic event rates (12.2 events per 100 person-years), followed by switching from 1 generic product to another (11.7 events per 100 person-years), switching from generic to Coumadin (10.5 events per 100 person-years), staying with 1 generic warfarin (7.9 events per 100 person-years) and staying with Coumadin (6.3 events per 100 person-years). Staying with Coumadin had longer mean time to first hemorrhagic or thrombotic event than switching between warfarin formulations. The mean time to first hemorrhagic or thrombotic event for staying with 1 generic only was similar to remaining on Coumadin.
Unadjusted Rate and Mean Time a to First Hemorrhagic Event or Thrombotic Event During Follow-Up Period
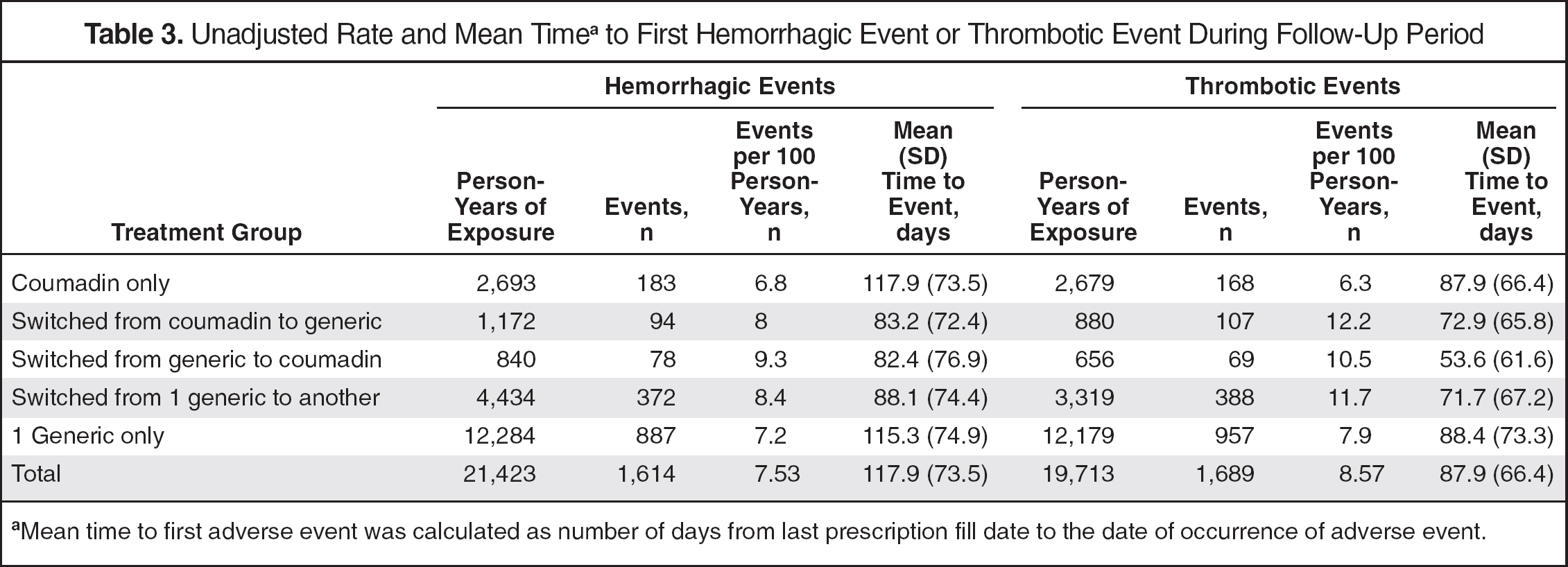
Mean time to first adverse event was calculated as number of days from last prescription fill date to the date of occurrence of adverse event.
COX REGRESSION MODEL RESULTS
Cox proportional hazard regression models were used to estimate the likelihood of adverse events following switching of warfarin formulations (from 1 generic to another, from generic warfarin to Coumadin and from Coumadin to generic warfarin) and staying on 1 generic warfarin product, relative to staying on Coumadin, while controlling for sex and baseline CCI (Table 4). Figure 2 provides a forest plot of the estimated hazard ratios associated with hemorrhagic and thrombotic events. Compared to remaining on Coumadin, switching warfarin formulations was associated with a significantly higher risk of thrombotic events. The highest increase in the risk for thrombotic events (including stroke, DVT, or PE) was observed after switching from 1 generic to another generic (HR = 1.89, p < 0.001), followed by Coumadin to generic warfarin switch (HR = 1.81, p < 0.001), and generic warfarin to Coumadin switch (HR = 1.76, p < 0.001) compared to remaining on Coumadin. Similarly, switching warfarin formulations was associated with a significantly higher risk of hemorrhagic events. Switching from Coumadin to a generic warfarin product, from generic warfarin to Coumadin, or from 1 generic warfarin product to another was associated with a 51% (p = 0.001), 60% (p = 0.001), and 74% (p < 0.001) higher risk, respectively, for hemorrhagic events compared to remaining on Coumadin only. Staying with the same generic product was also associated with a significant but smaller increase in the risk of thrombotic events (HR = 1.23, p = 0.015) relative to remaining on Coumadin. Notably, the risk of hemorrhage when staying with 1 generic product was not significantly different than remaining on Coumadin only.
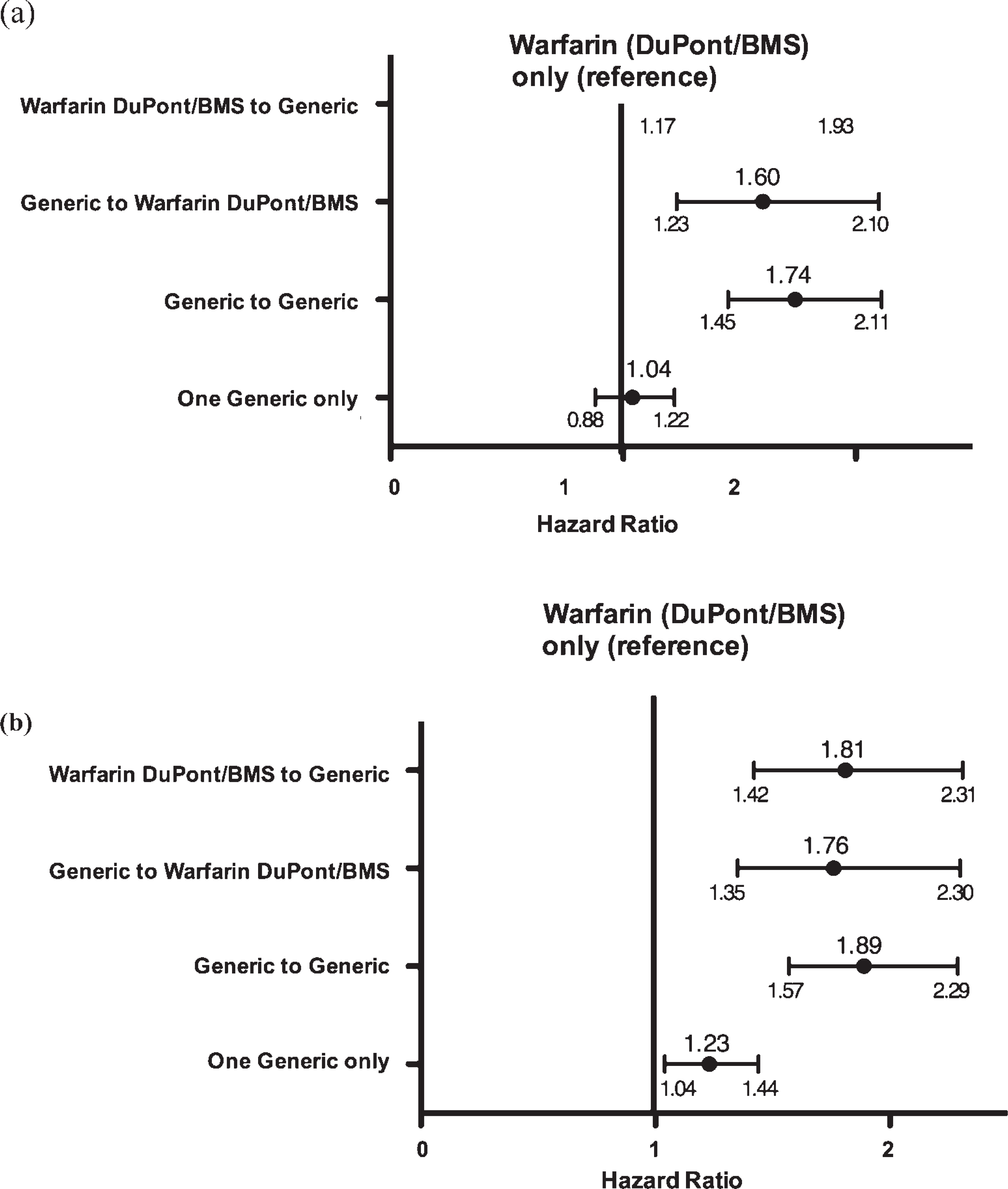
Forest plot of hazard ratios for (a) hemorrhagic and (b) thrombotic adverse events in patients who switch or remain on generic compared to those who remain on warfarin (DuPont/BMS).
Hazard Ratios for Adverse Events in Patients Who Switch or Remain on Generic, Compared to Those Who Remain on Brand Warfarin
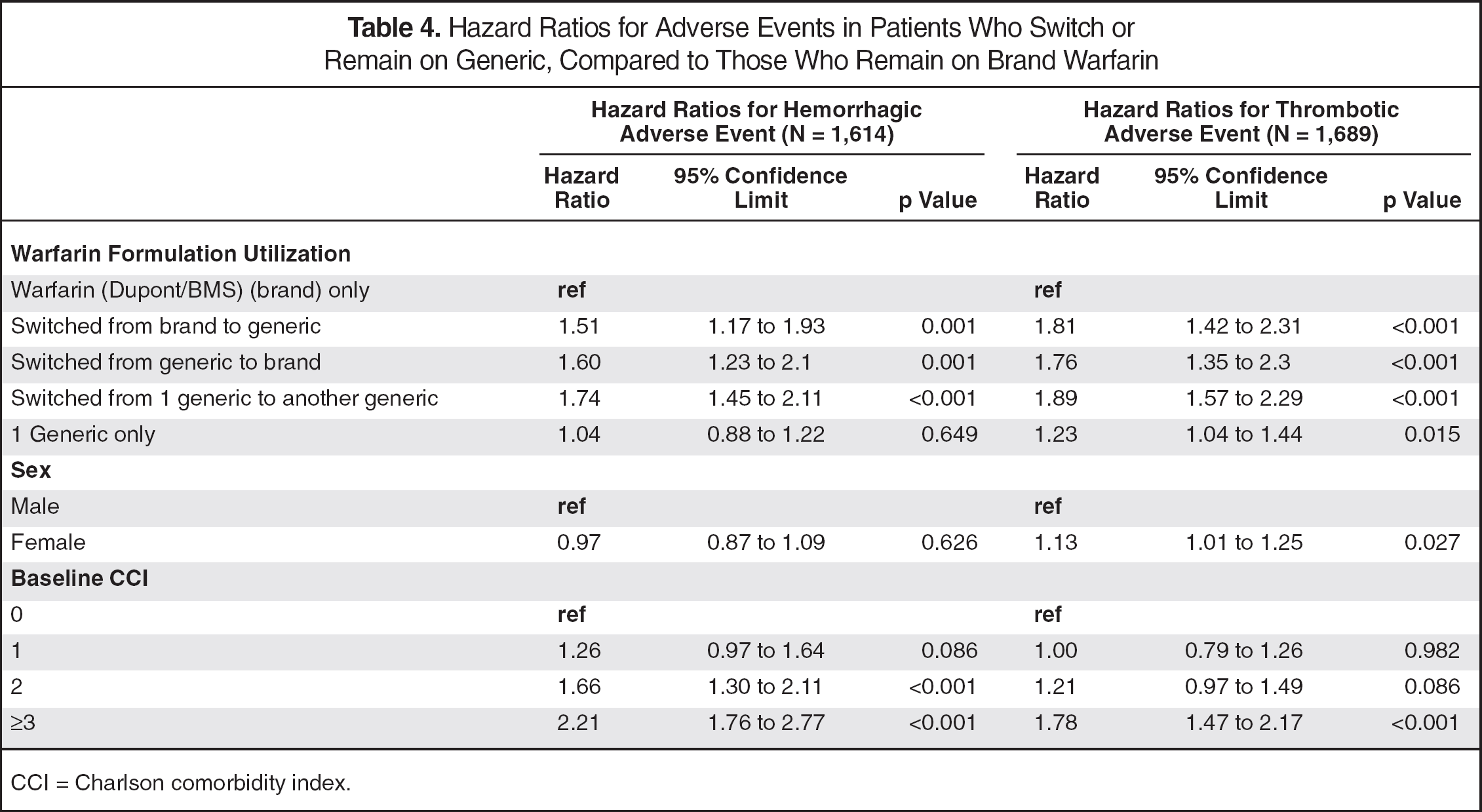
CCI = Charlson comorbidity index.
Women were found to have an increased risk of a thrombotic event compared to men (HR = 1.13, p = 0.027; Table 4). Compared to subjects with no comorbidities (CCI = 0) at baseline, those with a baseline CCI score of 1 did not have a statistically significant difference in the risk of hemorrhagic event (HR = 1.26, p = 0.086) or thrombotic event (HR = 1.00, p = 0.982). However, subjects who had a baseline CCI score of 2 (HR = 1.66, p < 0.001) or 3 or more (HR = 2.21, p < 0.001) had significantly higher risk of hemorrhagic event compared to subjects with no comorbidities. Subjects with a baseline CCI score of 3 or more also had significantly higher risk of thrombotic events (HR = 1.78, p < 0.001) compared to subjects with a baseline CCI score of zero. The risk of thrombotic events for subjects with a CCI score of 2 (HR = 1.21, p = 0.086) was similar to the risk in those with no comorbidities at baseline.
Discussion
Generic warfarin utilization and switching between warfarin formulations were common in AF patients. Among generic warfarin users in this study, at least 1 in 4 subjects substituted 1 generic product with another generic during the 1-year follow-up period. Substituting 1 generic warfarin product with another was associated with the highest increase in the risk of thrombotic and hemorrhagic events relative to staying on Coumadin among the different types of switching. To our surprise, staying with a single generic product was also associated with a significant but smaller increase in the risk of thrombotic events relative to staying on Coumadin, although no difference in bleeding risk was observed. The results suggest that switching warfarin formulations, including the substitution of 1 generic for another, may expose patients with AF to a higher risk of thrombotic and bleeding events compared to remaining on Coumadin and underscore the challenges associated with the availability and use of warfarin from multiple manufacturers.
A key strength of this study was the use of a large-scale, administrative claims database representative of the US general population covered by commercial insurance. However, the retrospective nature of the claims analysis posed several challenges. First, although we attempted to control for comorbidities, analysis of claims data cannot rule out other causes of the increased risks of adverse events observed in this study. We limited our analysis to include only patients who had at least 3 warfarin prescription fills during the follow-up period to increase the likelihood of including patients on continuous warfarin therapy, and we assumed these patients to be continuously using warfarin between consecutive prescription fills. However, this assumption could not be validated in the absence of additional clinical information. Neither medical records nor INR values, including the frequency of INR monitoring, were available for this study. Therefore, we were unable to confidently attribute adverse events identified using diagnosis codes to warfarin therapy or a formulation-switching event. Data on missing follow-up appointments that may impact the rate of hemorrhagic and thrombotic events were also unavailable for retrospective analysis. Medications such as proton pump inhibitors, histamine H2 receptor blockers, aspirin, or nonsteroidal antiinflammatory drugs that may influence the risk of hemorrhagic or thrombotic events are available over the counter and are also not captured in the Medstat database. (The CCI encompasses peptic ulcer disease, and the analysis may have controlled for the concomitant medication use of proton pump inhibitors or H2 receptor blockers in subjects diagnosed with peptic ulcer disease). Concomitant use of other prescription drugs and antithrombotic agents was not controlled for in this analysis. Also, data on adherence to warfarin treatment were not collected, which may influence the risk of hemorrhagic or thrombotic events. Further research is needed to corroborate and further strengthen the evidence of this retrospective study.
Second, the study may be subject to selection bias. The study required subjects to provide at least 12 months of follow-up data after the index AF diagnosis date. Therefore, individuals who discontinued health plan coverage or died during the follow-up period were not included. Excluding subjects who died likely underestimated the event rate. Subjects who died within 12 months of AF diagnosis may have been sicker and the event rate may have been higher in this population. Any adverse events that occurred during the 30-day stabilization period immediately after the index warfarin prescriptions were also excluded. These requirements may have led to an underestimation of the adverse event rate. Nevertheless, we found that the overall rates of major GI bleeding (2.48 per 100 person-years), IC hemorrhage (0.66 per 100 person-years), and ischemic stroke (2.98 per 100 person-years) observed in our study were similar to those reported in other published clinical trials 37 and higher than those reported in published retrospective analyses of data from integrated health-care systems. 38 It is possible that a more intense INR monitoring of warfarin therapy in the integrated health-care system may be accountable for the difference in event rates. Another limitation of the study is the potential for hidden product switching, which may have resulted in misclassification bias. It was not possible to validate that the warfarin product dispensed by the pharmacy was actually the product consumed by the subject. A relatively small but unknown percentage of subjects may have consumed a product different from the one observed in claims.
Notwithstanding these limitations, the study addresses an important question that has been raised by many clinicians for more than a decade. Each generic formulation is tested for bioequivalence relative to Coumadin, but the individual generic formulations are not tested for bioequivalence among each other. Despite the regulatory definition of bioequivalence, due to the narrow therapeutic window of warfarin, skepticism remains regarding the impact of variation in bioavailability on the outcomes of patients. Our results are somewhat different from those of previously published studies. Milligan and colleagues conducted an observational study in patients taking Coumadin who were switched to the Barr generic warfarin in an HMO setting in the US. 18 These patients exhibited no significant difference in INR control (based on the % INR values within target therapeutic range) or rates of thrombotic and hemorrhagic events after the switch. 18 All patients included in that study were managed by a telephone-based anticoagulation service. In contrast, Halkin et al. showed, in an observational study, that among patients whose warfarin dosage remained the same, median INR levels dropped from therapeutic to subtherapeutic levels after generic substitution of Coumadin. 23 Patients in the study were managed by their primary care physicians, and INRs were monitored every 2-3 weeks. The Halkin et al. study did not evaluate the risk of any adverse events, but found no significant difference in the number of hospital admissions occurring during periods of Coumadin and generic warfarin formulation use. Patients in both studies appeared to be under close INR monitoring on a regular basis, whereas subjects in the current study may or may not have been monitored on a regular basis. Further research is needed to determine whether the level of INR monitoring or other reasons could explain the difference in study findings.
Warfarin formulation switches likely occur at the pharmacy level, without a physician' knowledge, except in Oklahoma, where a prescriber' or provider' consent is required before substitution. The Kentucky, Pennsylvania, South Carolina, and North Carolina boards of pharmacy either have restrictions on generic substitution or maintain a list of narrow therapeutic index drugs, including warfarin anticoagulants, that cannot be generically substituted.39–42 However, most of these regulations focus on generic substitution of brand products but do not necessarily address the risk associated with substituting 1 generic product for another. Unlike previous studies that compared switching from Coumadin to a single generic formulation, this study evaluated switching among the various generic formulations. Given that there are currently 7 manufacturers of generic warfarin and an even larger number of repackagers of generic warfarin, this type of switching probably occurs frequently in the retail pharmacy setting unbeknownst to patients or their physicians. As our retrospective study has demonstrated, this type of switching among generic warfarin products, in addition to generic substitution of Coumadin, appears to be associated with the highest risk of adverse events. Studies have shown that supplemental monitoring of INR is required after brand to generic warfarin switches and patients must be closely monitored to allow detection of changes in anticoagulation response. 24 As generic warfarin formulation substitution/switching done at the pharmacy level could predispose AF patients to a higher risk of adverse events, there is a need to improve communication among pharmacies, physicians, and patients to ensure that patients are monitored closely after intergeneric warfarin product substitutions. Nevertheless, there are suggestions in the literature that maintaining an optimal INR level during warfarin therapy is challenging in the real-world setting. 43
Evident from the descriptive results of the study (Table 2), subjects with managed health plans were likely to stay with a generic formulation or Coumadin, while subjects with fee-for-service insurance were likely to switch among different warfarin formulations. Current health plan drug formularies tend to regulate access to branded warfarin therapy and encourage the free use of generic products. Nevertheless, it is possible that managed care members were encouraged to use the same pharmacy so that they were less likely to experience inadvertent warfarin formulation substitution. Studies are needed to further explore this relationship. This study also found that elderly subjects were more likely to switch between multiple warfarin formulations than to stay with Coumadin. However, to what extent that this higher propensity to switch is related to price sensitivity and affordability of medication to the elderly or the implementation of Medicare Part D benefits in recent years remains unclear and warrants further investigation.
In conclusion, generic warfarin utilization and switching among warfarin formulations, including substituting 1 generic for another generic, are common among patients with AF. This study suggests that switching warfarin formulations may expose AF patients to a higher risk of thrombotic and bleeding events than remaining on Coumadin. Further studies should prospectively evaluate whether switching between warfarin formulations increases the risk of thrombotic and bleeding events. The consequences of warfarin formulation switching need to be adequately considered in health policy decisions pertaining to the appropriate anticoagulation in patients diagnosed with AF.
Footnotes
Authors reported none. This study was funded, in part, by a research grant from Daiichi Sankyo, Inc., Parsippany, NJ
Acknowledgements
We acknowledge the input of Daniel Singer MD, Massachusetts General Hospital and the Harvard Medical School, in our study design and the contribution of Dusica Tasic, graduate student in our Department of Pharmacotherapy, University of Utah, in organizing the content for the manuscript.
Charlson Comorbidity Index
| The Charlson comorbidity index (CCI) encompasses 19 medical conditions (ICD-9) weighted 1-6. From the weighted conditions, a sum score can be tallied to yield the total comorbidity score. To account for increasing age, one point is added to the CCI score for each decade of life over the age of 50 (1 point for 60s, 2 points for 70s, 3 for 80s). Thus, possible CCI scores range from 0 to 36. | ||
|---|---|---|
| Comorbidity | D'Hoore ICD-9 Codes | Charlson Weight |
| Myocardial infarction | 410, 411 | 1 |
| Congestive heart failure | 398, 402, 428 | 1 |
| Peripheral vascular disease | 440-447 | 1 |
| Cerebrovascular disease | 430-433, 435 | 1 |
| Dementia | 290, 291, 294 | 1 |
| Chronic obstructive pulmonary disease | 491-493 | 1 |
| Rheumatologic disease | 710, 714, 725 | 1 |
| Peptic ulcer disease | 531-534 | 1 |
| Mild liver disease | 571, 573 | 1 |
| Diabetes | 250 (excluding 250.4-250.6) | 1 |
| Hemiplegia or paraplegia | 342, 434, 436, 437 | 2 |
| Moderate or severe renal disease | 403, 404, 580-586 | 2 |
| Diabetes + complications | 250.4-250.6 | 2 |
| Malignancy | 200, 202, 203 | 2 |
| Moderate or severe liver disease | 070, 570, 572 | 3 |
| Metastatic solid tumor | 196-199 | 6 |
| AIDS | 042-044 | 6 |