
Abstract
BACKGROUND:
Acetaminophen overdose is the most common pharmaceutical poisoning in the US. The labeled dosing regimen for Acetadote, the only intravenous N-acetylcysteine (IV-NAC) product approved by the Food and Drug Administration (FDA) for treatment of acetaminophen toxicity, is a complex 3-step process that produces frequent medication errors. We have been using an off-label, uncomplicated dosing regimen consisting of a standard preparation of IV-NAC 30 g in 1 L of 5% dextrose in water, with a 150-mg/kg loading dose administered over 1 hour followed by an infusion of 14 mg/kg/h for 20 hours.
OBJECTIVE:
To evaluate the frequency of medication errors, resolution of hepatotoxicity, and tolerability of the protocol used in our institution for treatment of acetaminophen toxicity.
METHODS:
This single-center, retrospective chart review evaluated patients receiving IV-NAC for acetaminophen toxicity from August 2006 to August 2008. Charts were reviewed for prescribing practices, dosing errors, and clinical outcomes.
RESULTS:
Among 70 patients who met inclusion criteria, 35 medication errors occurred, including 22 administration errors and 13 protocol initiation errors. The frequency of administration errors was 13.5 errors per 100 administration interventions. Loading dose errors were most common with 11 rate-related and 8 dose-related errors. Interruptions longer than 60 minutes occurred in only 3 patients. No adverse outcomes were associated with medication errors. The mean (SD) duration of therapy was 25.6 hours (n = 60 pts. [17.8], range 1-76.5), and mean length of stay was 2.99 days ([3.82], range 0.1-25.7). All patients with hepatotoxicity (aspartate aminotransferase >1000 units/L) due to acute acetaminophen toxicity had resolution of the toxicity and were successfully discharged.
CONCLUSIONS:
This single intravenous bag protocol is effective and well tolerated, and there is infrequent interruption of therapy. The overall rate of administration errors is similar to that in reports on the FDA regimen; thus, our protocol may be an acceptable alternative.
Acetaminophen overdose is one of the most common toxic exposures treated in the US. Acetaminophen accounts for approximately 0.5% of human exposures but approximately 20% of fatal poisonings reported to the American Association of Poison Control Centers annually. 1 N-acetylcysteine is the drug of choice for treating acetaminophen overdose and preventing hepatotoxicity.
Acetadote, the only intravenous N-acetylcysteine (IV-NAC) product approved by the Food and Drug Administration (FDA) for treatment of acetaminophen toxicity, was approved in 2004. The labeled dosing regimen of this product consists of a complex 3-step process using 3 custom-prepared bags of 2 different sizes with 3 different concentrations and 3 different infusion rates. 2 The first step of the FDA-labeled regimen consists of a 150-mg/kg loading dose (LD) placed in 200 mL of 5% dextrose in water for injection (D5W). The maintenance dose is given in 2 stages. First, a 50-mg/kg dose in 500 mL of D5W is given over 4 hours, followed by the last phase, a 100-mg/kg dose in 1000 mL of D5W administered over 16 hours. The complexity of the dosing process has been associated with frequent dosing and administration errors.3–5 In a 2008 retrospective poison control center chart review by the Maryland Poison Control Center, Hayes et al. identified 84 medication errors in 74 patients. The most common dosing error was interruption of the infusion for more than 60 minutes. 4
Our institution has been using an alternative, off-label IV-NAC dosing regimen that originated prior to the availability of Acetadote. Because of the labor intensity of compounding the inhalational acetylcysteine into an intravenous product, a single-bag method was chosen. 6 The hospital began using the FDA-approved IV-NAC product in 2004. However, the standard concentration infusion prepared by placing 30 g of IV-NAC (Acetadote) in 1000 mL of D5W (total volume) was continued (Figure 1). The dosing regimen was modeled after work by Prescott and colleagues. 7 Slight modifications in maintenance infusions were made to facilitate bedside drip calculations prior to availability of “smart” infusion pumps. The same LD of 150 mg/kg is given to the patient over 1 hour with 1 dose reduction to 14 mg/kg/h as the maintenance rate for 20 hours. The dosing regimen requires only 1 compounding step with a standardized concentration into a single bag with fewer administration interventions by caregivers. The patient still receives the total required dose of 300 mg/kg of IV-NAC. This potentially reduces the number of opportunities for medication errors. The purpose of this was to evaluate the error rate, safety, and efficacy of our institution's regimen.
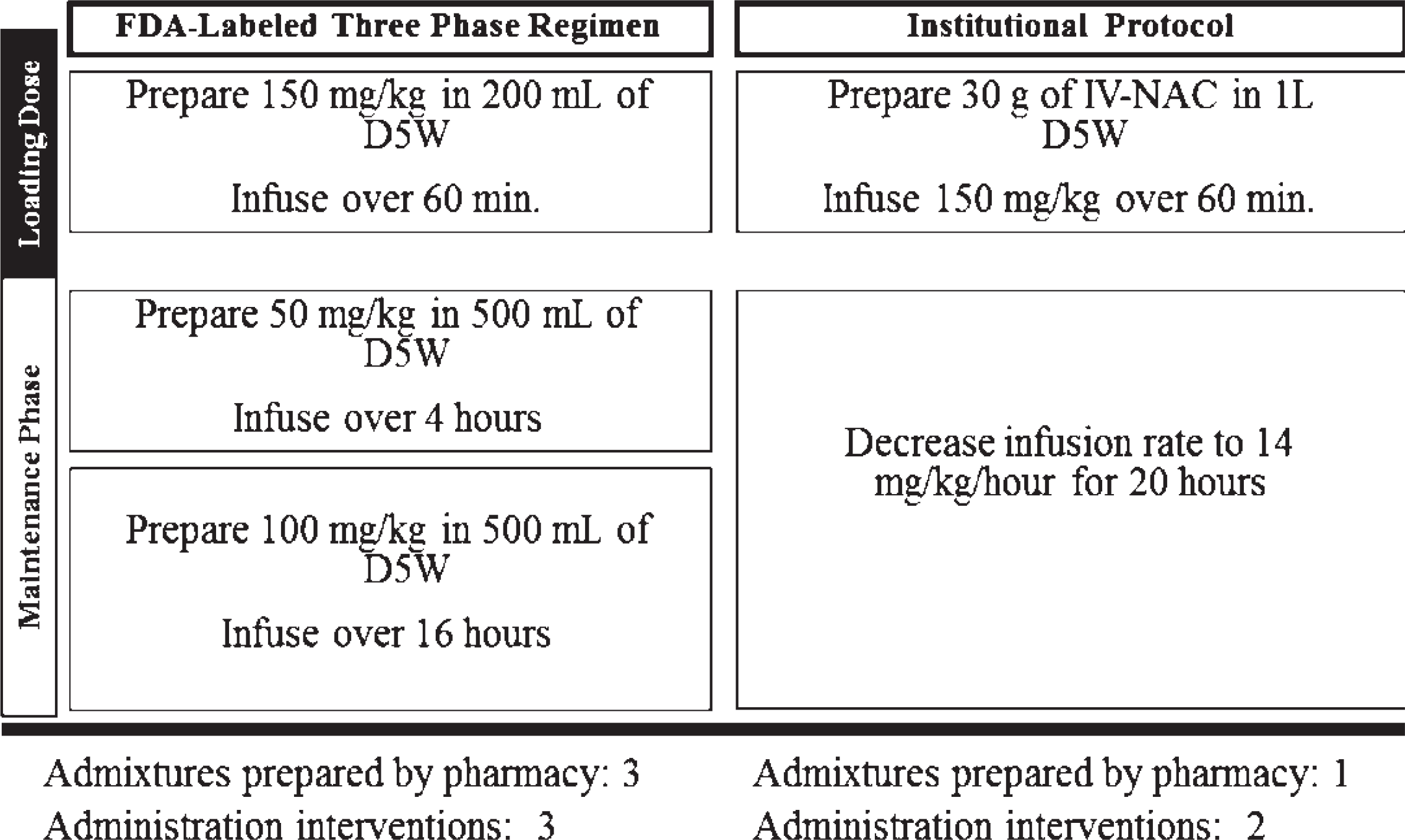
Comparison of N-acetylcysteine dosing protocols. D5W = 5% dextrose in water; FDA = Food and Drug Administration.; IV-NAC = intravenous N-acetylcysteine.
Methods
STUDY LOCATION AND PATIENTS
This study was conducted at Barnes-Jewish Hospital, a 1200-bed university-affiliated, urban teaching hospital.
During a 2-year period (August 30, 2006-August 28, 2008), all hospitalized patients to whom IV-NAC was dispensed were eligible for this investigation. This study was approved by the Washington University School of Medicine Human Studies Committee.
STUDY DESIGN AND DATA COLLECTION
A single-center, retrospective cohort methodology was used to conduct this study. We identified cases with reported acetaminophen concentrations and IV-NAC treatment using our institution's medical informatics database. Patients were included in the primary analysis if receiving IV-NAC for the treatment of acute or chronic acetaminophen toxicity. Patients were excluded if they received IV-NAC for any other indication, had a history of chronic liver disease, had received treatment at another health-care facility, or had received oral NAC therapy at any time. To ensure consistency during data extraction, the electronic medication administration record, laboratory results, and patient's chart were reviewed by a single investigator (MTJ).
We recorded baseline characteristics including age, sex, race, type of ingestion (acute vs chronic), time from ingestion, initial acetaminophen concentration, and baseline aspartate aminotransferase (AST), alanine aminotransferase (ALT), and international normalized ratio (INR). The following processes of care variables were also collected: department of hospital where the patient received treatment (emergency department vs intensive care unit [ICU]), time of initiation of IV-NAC, duration of IV-NAC therapy, frequency of medication administration errors, adverse effects attributed to IV-NAC therapy, length of stay (LOS), maximum AST, ALT, INR values, and discharge status of the patient.
The primary objective of this study was to characterize the frequency of medication errors with the institution's standardized IV-NAC regimen. The secondary objectives were to describe the frequency of inappropriate prescribing of IV-NAC, estimate the cost of IV-NAC misuse, identify the adverse reactions associated with this regimen, and report the clinical outcomes of patients treated with this regimen.
DEFINITIONS
All definitions were selected as part of the original study design. Basic error categories were modeled after the report by Hayes et al. to include LD, LD rate, maintenance dose rate, interruptions of infusion, and initiation errors. 4 The error criteria were further refined to account for the institutional protocol and medical chart review. An administration error was defined as violation of 1 of the following criteria: (1) a total amount of LD deviation of 10% (±15 mg/kg); (2) a rate of LD deviation by 10% (±6 minutes from 1 hour); (3) a rate of maintenance dose infusion deviation of 10% (±1.4 mg/kg/h); and (4) an interruption of infusion longer than 60 minutes. It was possible for each case to have more than 1 medication error during treatment. For patients treated longer than the institutional protocol, medication errors occurring after the initial 20 hours of therapy were included in the analysis. If the investigator deemed the clinical documentation insufficient to accurately allow retrospective assessment, the case was classified as not evaluable for the particular outcome. Administration intervention was defined as an evaluable point in medication administration during which an error could have occurred. Cases of acetaminophen toxicity were classified into groups based on presentation. Ingestions were classified as acute if physicians noted the time of ingestion of an amount of acetaminophen larger than 6 g. Ingestions were classified as chronic if indicated so by the treating physician. Finally, in patients from whom no history could be obtained, ingestions were classified as unknown. Inappropriate prescribing of IV-NAC was analyzed only in patients with acute ingestion with a serum acetaminophen concentration that could be compared to the Rumack-Matthew nomogram. 8 Therapy that was started prior to obtaining the results of acetaminophen concentration 4 hours postingestion or when serum acetaminophen concentration was below the Rumack-Matthew nomogram treatment line (ie, 150 μ/mL 4 hours postingestion) was classified as an initiation error. Patients deemed to have a compelling indication for early initiation of therapy (ie, pregnancy, alcoholism, or concomitant ingestion of an enzyme inducer) were excluded from this outcome. Initiation errors of IV-NAC were considered a medication error in this study. However, patients with inappropriate initiation were analyzed for administration errors if a full course of IV-NAC was given. Hepatotoxicity was defined as any AST concentration greater than 1000 units/L. 9 Resolution of hepatotoxicity was defined as a greater than 50% reduction in AST concentration and no coagulopathy (INR <2). Adverse effects attributed to IV-NAC therapy must have been documented by a treating physician to be included in this study.
Data Analysis
Continuous variables are reported as mean (SD). Nominal data are presented as frequency distribution. Analysis of variance was used to compare duration of treatment and LOS for each presentation type. Administration error frequencies were compared between groups using Fisher exact test (SPSS version 11.0.1 for Windows; SPSS, Inc.; Chicago, IL).
Results
PATIENT CHARACTERISTICS
The database identified 115 patients who received IV-NAC at the institution over a 24-month period (August 2006-August 2008) (Figure 2). Of these patients, 45 were excluded for the following reasons: treatment at another institution (n = 31); unknown substance or polysubstance ingestion (6); ischemic, infectious, or other hepatitis (6); and received oral N-acetylcysteine therapy (2). For the 70 patients who met inclusion criteria, the mean age was 34.7 (3.77) years (range 18-67) with 29 (41%) males and 41 (59%) females. The mean dosing weight was 76.1 (21.7) kg (range 21-127). Twenty-nine patients presented with acute ingestion (41%), 19 with chronic toxicity (27%), and 22 (32%) had an unknown time of ingestion and/or unknown amount of ingestion (Table 1).
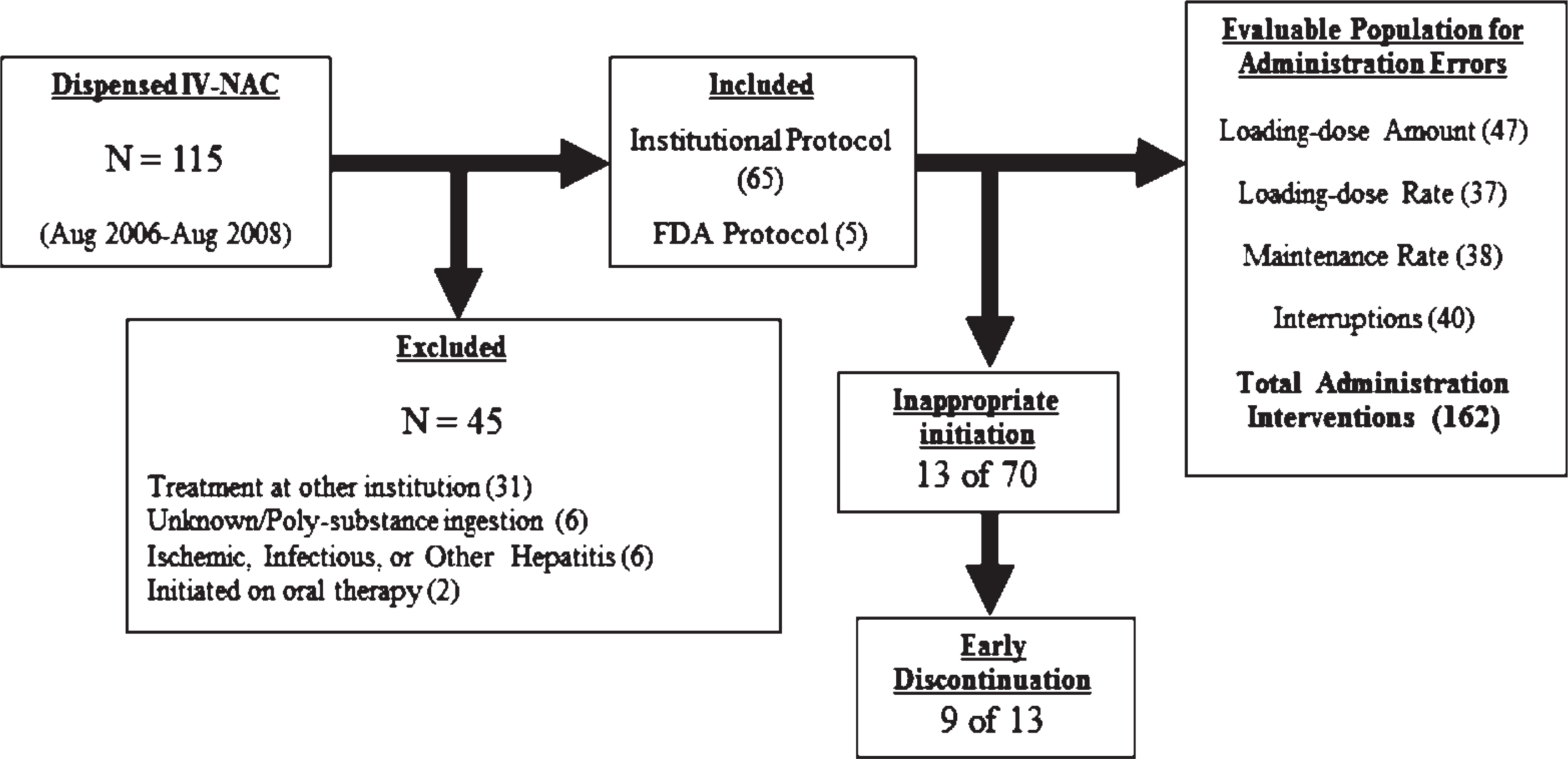
Study flow diagram. FDA = Food and Drug Administration; IV-NAC = intravenous N-acetylcysteine.
Baseline Patient Characteristics a
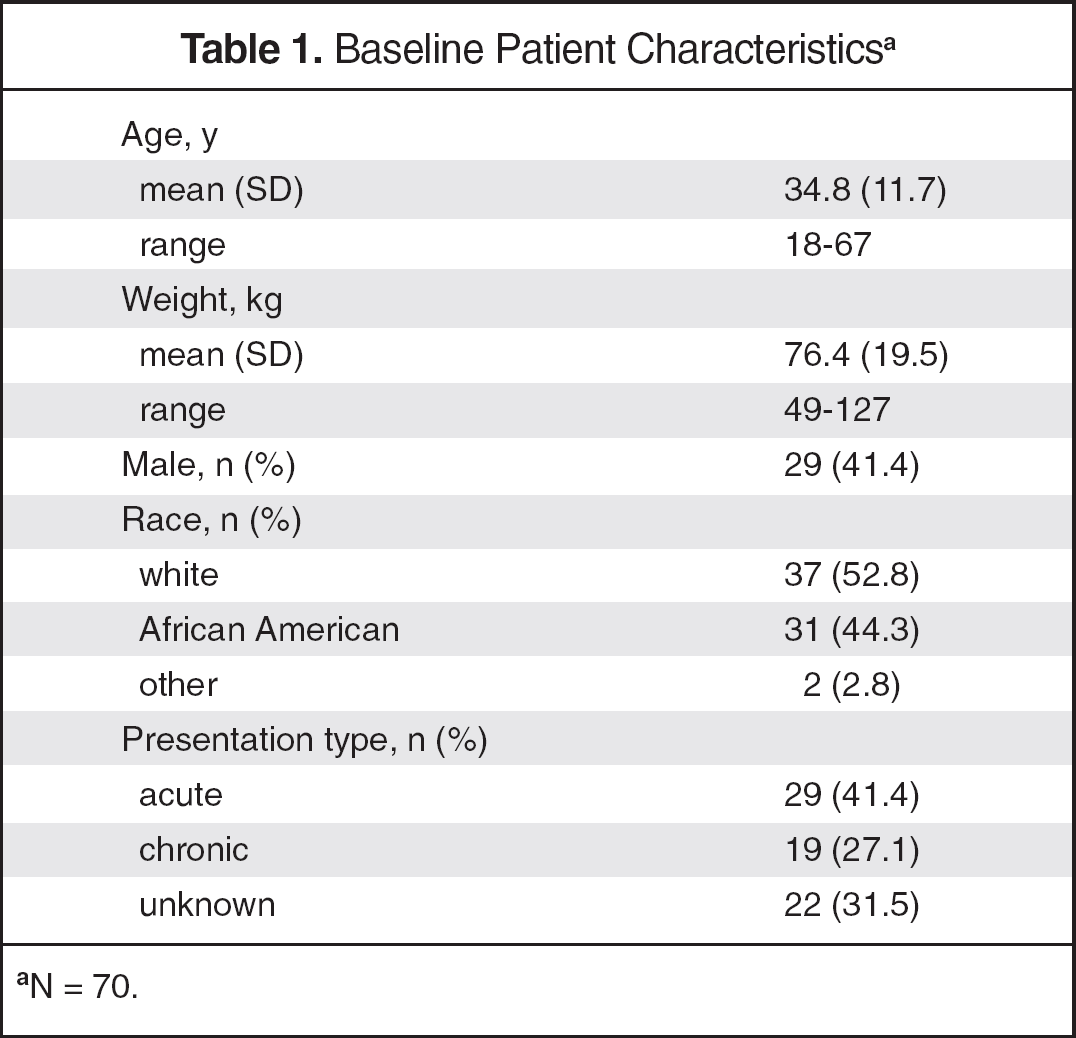
N = 70.
OVERALL ERRORS
A total of 35 errors occurred in 28 patients from our sample (Table 2), with 13 initiation errors and 22 administration errors. When directly comparing rates of cases with at least 1 error between the FDA-labeled regimen (3 of 5 cases, 60%) and the institutional regimen (25 of 65 cases, 38%) no significant difference was observed (p = 0.383, OR = 1.53, 95% CI 0.52 to 4.57; Table 3).
Medication Errors by Type
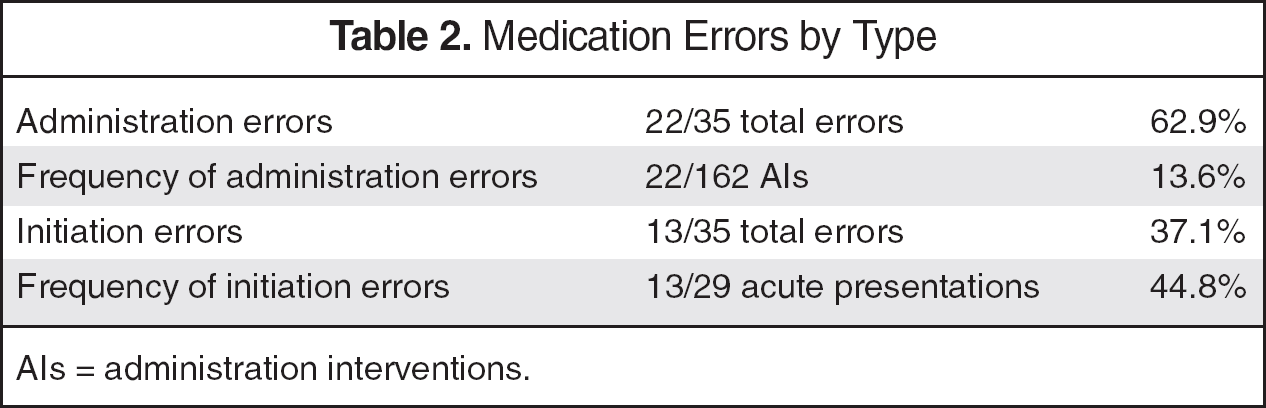
AIs = administration interventions.
Comparison of FDA and Institutional Protocol a
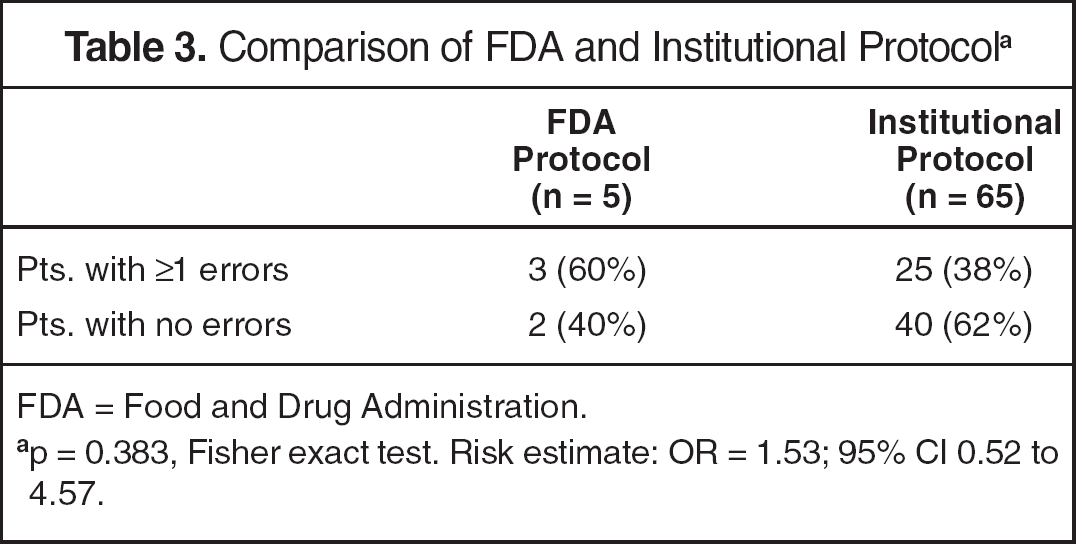
FDA = Food and Drug Administration.
p = 0.383, Fisher exact test. Risk estimate: OR = 1.53; 95% CI 0.52 to 4.57.
PRESCRIBING PRACTICES AND INITIATION ERRORS
The majority of patients (70) were followed by the toxicology service (n = 48, 69%) when IV-NAC therapy was initiated. The remaining patients were managed by the emergency department (n = 19, 27%), hepatology service (n = 2, 3%), and medical ICU/ward (n = 1, 2%). Sixty-five of 70 patients received IV-NAC according to the institutional protocol; the remaining 5 patients received the FDA-labeled regimen. Patients who presented with acute ingestion had inappropriate initiation in 13 of 29 (45%) cases of IV-NAC therapy. Nine of the 13 patients had early discontinuation of IV-NAC therapy (Table 2). The reasons for inappropriate administration were therapy was started prior to identification of the serum concentration (6 of 13, 46%), blood sample for acetaminophen concentration was drawn prior to 4 hours postingestion with initiation of IV-NAC (5 of 13, 39%), and acetaminophen serum concentration was below the nomogram treatment line (2 of 13, 15%). The emergency department was treating 10 of 13 patients and the toxicology service was following the remaining 3 patients. The mean duration of therapy in 60 patients, excluding initiation errors with early termination and fatal cases, was 25.6 (17.8) hours (range 1-76.5). The duration of treatment did not differ significantly by presentation type and was 24.9, 21.7, and 24.5 hours for acute, chronic, and unknown presentations, respectively (p > 0.05).
ADMINISTRATION ERRORS
Sixty-five patients received the institutional protocol, with 20 administration errors occurring in 19 (29%) patients. Of the 5 patients who received the FDA-labeled regimen, 2 administration errors occurred in 2 patients (40%, 1 error in each patient). Overall, there were 22 (13%) administration errors in 162 medication administration interventions evaluated (Figure 1 for evaluated administration interventions). Administration errors occurred most often during the LD phase of the regimen (19 of 22, 86%). The LD infusion rate was the most frequent administration error, occurring in 11 of 37 (30%) evaluable patients. All but 2 of these cases were classified as excessive rates of infusion, with the LD infused in less than 54 minutes. Deviation from the expected 150 mg/kg LD was observed in 7 of 47 (15%) evaluable patients. The average LD in cases classified as administration errors was 169.5 mg/kg; no patients were underdosed, as the LDs ranged from 150 to 212 mg/kg. In all patients evaluated in the study, the mean LD was 155.8 (65.6) mg/kg (range 138.2-212.4). There was 1 deviation in the rate of the maintenance infusion (1 of 38 evaluable cases) during the maintenance phase of the FDA protocol. In the 40 evaluable patients, there were 3 (8%) interruptions of infusion longer than 60 minutes. The interruptions occurred in patients weighing more than 69 kg (77.1 kg, 86.6 kg, 106 kg), requiring pharmacy to compound a second infusion to complete the regimen. Forty patients in the sample weighed more than 69 kg.
CLINICAL OUTCOMES AND SAFETY
Sixty-nine (99%) of the 70 patients were ultimately discharged home; 13 patients were transferred to an acute psychiatric care facility after medication stabilization. The average LOS was 2.99 (3.82) days (range 0.1-25.7). LOS did not differ significantly by presentation type and was 2.39, 2.48, and 4.27 days for acute, unknown, and chronic presentations, respectively (p > 0.05). Sixteen patients developed hepatotoxicity (AST >1000 units/L), with acetaminophen concentrations above the nomogram treatment line in 6 patients at presentation; 5 chronic acetaminophen intoxications; and 5 patients with an unknown time of ingestion. There was 1 death attributed to chronic acetaminophen toxicity. Upon presentation, that patient had fulminant hepatic failure: the initial serum acetaminophen concentration was 25.6 μ/mL; other laboratory values were prothrombin time 109 seconds, ALT 1019 units/L, AST 1246 units/L, and total bilirubin 1.1 mg/dL. There were no medication errors in this patient's IV-NAC therapy. All other patients had successful resolution of hepatotoxicity. No medication errors led to patient harm. There was a single adverse reaction attributed to IV-NAC therapy. The patient developed respiratory difficulty, with facial and truncal flushing approximately 1 hour after completing the loading dose of IV-NAC. The treating physician decreased the infusion rate and administered oral diphenhydramine, leading to symptom resolution; the rest of the treatment course was well tolerated.
DISCUSSION
The institutional protocol that used a fixed concentration of 30 g IV-NAC placed in 1 liter of D5W (fluid adjusted) was adopted due to the perceived benefits of uncomplicated compounding, as well as having a complete antidote regimen contained in a single dosing form, and decreased number of nursing interventions to administer the regimen. Overall, there were 13 initiation errors and 22 administration errors in the 70 patients included in this study. Interruptions of infusions longer than 1 hour occurred at a much lower frequency (8%) than reported with the FDA-labeled regimen (19%). 4 Interruptions in our study occurred only in patients with an actual body weight greater than 69 kg, which required preparation of a second admixture. This finding is consistent with the hypothesis that increasing the number of admixtures in an intravenous medication regimen furthers the potential for medication error. Inappropriate initiation occurred in 13 of 70 patients (19%). Based upon an average wholesale price (AWP) of $31.47 per gram, these 13 cases represent a potential excess medication expenditure of $12,273 over 24 months. 10
Administration errors were by far the most common medication error in this study, as they made up 63% of all errors. The frequency of administration errors was 13.5 errors per 100 administration interventions. The rates of administration errors were similar in FDA-labeled regimen versus institutional protocol. Due to high compliance with the institutional protocol, we were unable to demonstrate a difference in error rates between these 2 regimens. The wide 95% confidence interval of the odds ratio of cases with errors illustrates this fact. The average LD provided to our patients was within acceptable limits (155.8 mg/kg). No errors led to underdosing. The patient who received a loading- dose of 212 mg/kg received this excessive dose due to a prescribing error. A quarter of all errors were due to the LD being administered in less than 54 minutes, which is not clinically relevant, as safety data suggest that infusion of the IV-NAC 150-mg/kg LD over 15 minutes is acceptable. 11 This practice is not part of the institutional protocol and thus was deemed a medication error. Kerr et al. 11 found adverse event rates of 45% and 38% in the 15- and 60-minute LD groups, respectively. We reported only 1 adverse drug event in our sample (1 case in 70 patients, 1%).
Hayes and colleagues reported data from the Maryland Poison Control Center using the FDA-labeled regimen as the cohort. 4 Their evaluation of 221 cases revealed that 84 errors occurred in 74 patients (33%). The breakdown of error types from this cohort is reported in Table 4. These data confirm the complexity of administering the 3-bag regimen. Approximately 19% of the interruptions of therapy occurred between the LD and the first maintenance dose. These lapses in antidote therapy are concerning. Unnecessary drug therapy resulted in excessive medication expenditures of approximately $12,064 per year (AWP). The authors concluded that education regarding appropriate use of IV-NAC and investigating simpler dosing regimens should take place to decrease medication errors with this agent.
Medication Errors: Comparison to MPCC Data 4 Using MPCC Definitions
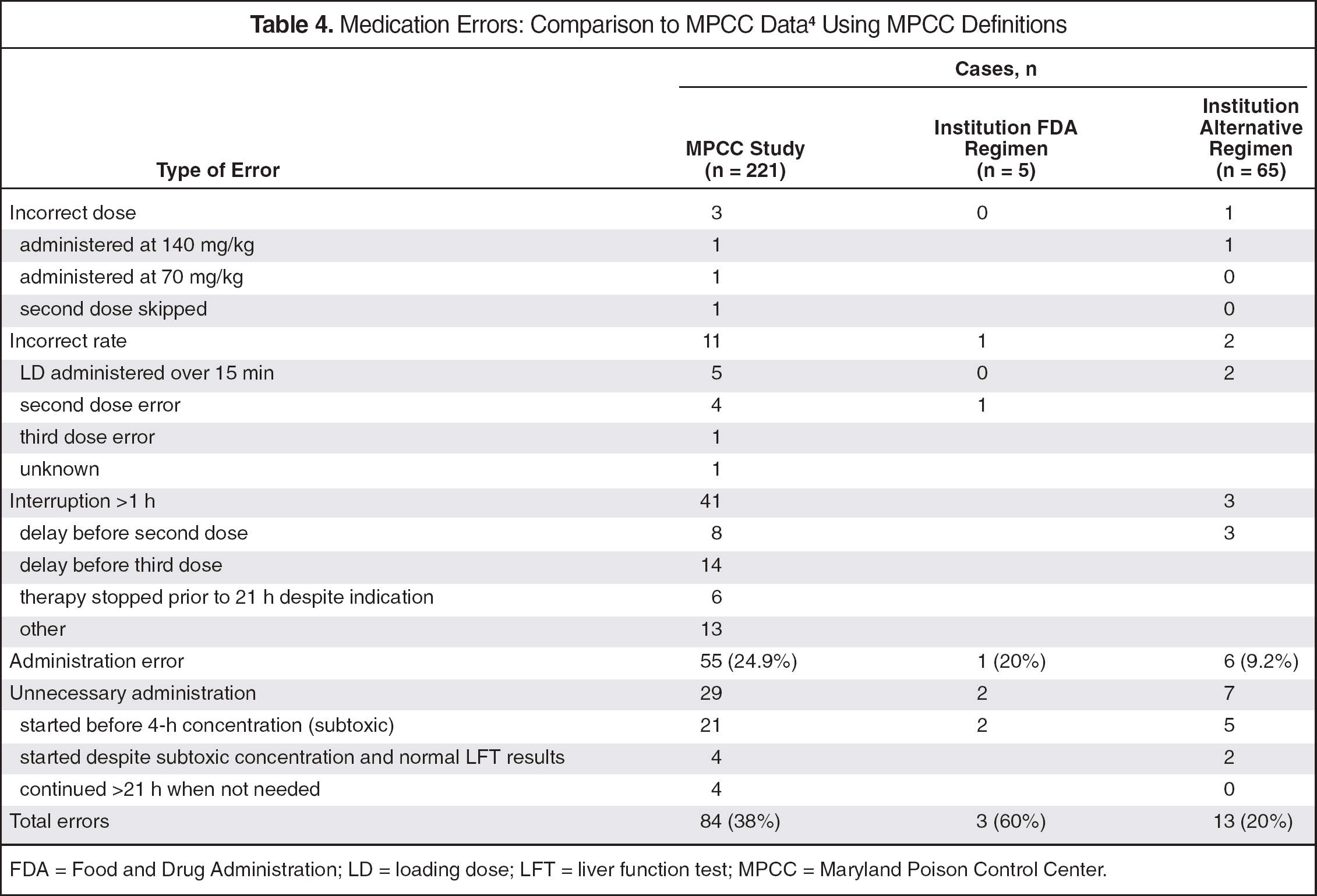
FDA = Food and Drug Administration; LD = loading dose; LFT = liver function test; MPCC = Maryland Poison Control Center.
Direct comparison of our protocol with the results described by Hayes and colleagues is difficult due to methodologic differences between the studies. The primary difference is data collection source; in our study, the patients' medical records were reviewed for pertinent documentation; Hayes et al. reviewed the Maryland Poison Control Center's database. Due to the difference in data source, we were able to collect detailed information directly from the medical record and apply more robust error definitions. By applying the less-stringent definitions used in the Hayes study (Table 4), our novel regimen error rate drops to 20% (13 errors in 65 cases), the inappropriate initiation error rate drops to 11%, and the administration error rate is 9%. A comparison of the data using our more rigorous study definitions can be found in Table 5.
Medication Errors: Comparison to MPCC Data 4 Using Current Study Definitions
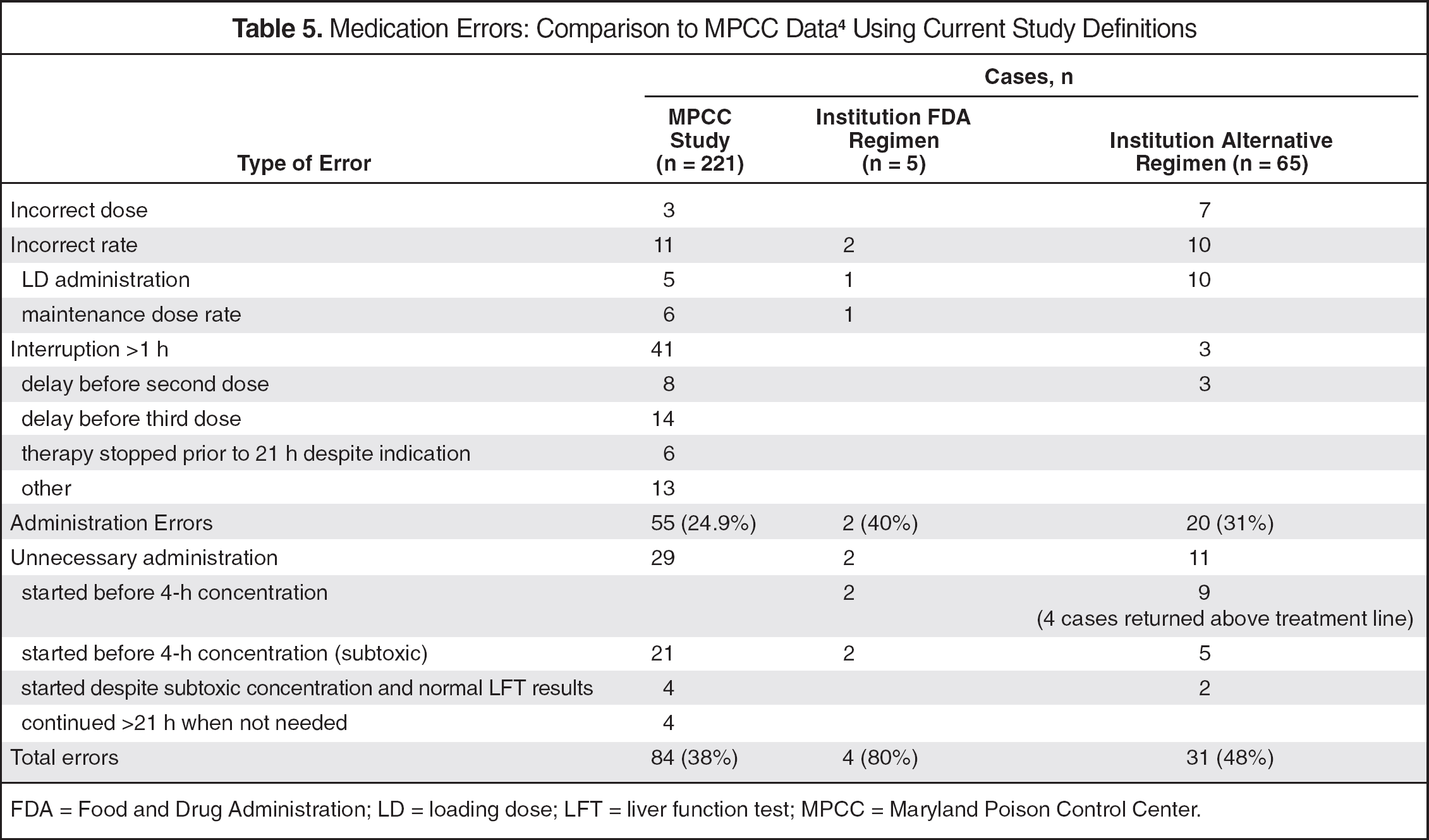
FDA = Food and Drug Administration; LD = loading dose; LFT = liver function test; MPCC = Maryland Poison Control Center.
The complexity of preparing the FDA-labeled IV-NAC regimen was reported by Ferner and colleagues. A multicenter trial evaluating the preparation of IV-NAC by measuring the concentration of the individualized infusions being administered was performed. 5 The investigators reported that only one third of the patients received the correct regimen (with a 10% margin of error). In total, two thirds of the infusions tested were within a 20% error margin. Seventeen (9%) infusions had greater than 50% deviation from expected concentration. The process steps at which the errors occurred in major deviations were in calculation (5%), compounding (3%), and inadequate mixing of the intravenous solution (9%). The presence of these complications supports the standardization of the IV-NAC preparation.
The results of the current study must be taken within the context of the limitations of the design. First, the single-center, retrospective structure did not allow for adequately powered comparisons of the institutional protocol and FDA-labeled regimen in error rate, interruptions of infusions, adverse effects, and clinical outcomes. Second, the study was conducted at a single institution with unique medical care characteristics, such as on-site toxicology consults, established IV-NAC protocol for several years, and high frequency of acetaminophen toxic ingestion. Additionally, our institution does use “smart” infusion pump technology. The standard concentration and dosing limits for IV-NAC are included in the medication library. The bedside nurse still must enter multiple variables into the pump at the time of administration. The value of standard concentration IV-NAC will rise as pump technology advances and more fully integrates into electronic medical record systems.
The results of this study suggest that this regimen may reduce the frequency of interruptions of infusions, limit the potential for underdosing IV-NAC, and be well tolerated. All patients who developed hepatotoxicity had normalizing AST levels and INR at the time of discharge. All but 1 patient with chronic toxicity was successfully discharged. Therapy was not discontinued in any case due to adverse effects. Inappropriate initiation as per previous studies is a potential target for the reduction of health-care expenses and avoidance of unnecessary medication administration. This regimen may be considered as a medication error mitigation strategy in health-care settings in which acetaminophen ingestion is rarely treated and health-care providers are unfamiliar with the complex 3-admixture FDA-labeled regimen. An additional consideration may be given in situations whereby providing a complete course of IV-NAC in a single admixture may be preferable to eliminate the potential for antidote interruptions. In conclusion, this regimen represents an acceptable alternative to the FDA-labeled regimen as it was effective, well tolerated, and medication errors associated with underdosing and interruptions of therapy were less frequent.