
Abstract
OBJECTIVE:
To report a case of multidrug-resistant osteomyelitis successfully treated with telavancin, rifampin, and meropenem.
CASE SUMMARY:
An 18-year-old male with spina bifida was treated primarily in the outpatient setting over the course of 133 days with multiple antimicrobials for a recurrent right calcaneal wound and osteomyelitis infection. Initial cultures were positive for methicillin-resistant Staphylococcus aureus and coagulase-negative Staphylococcus, which were treated with intravenous vancomycin 1 g every 12 hours, increased after 13 days to 1.5 g every 12 hours with addition of rifampin 300 mg twice daily, both of which were discontinued on day 22 due to leukopenia (white blood cell count 3.0 × 103/μL) and neutropenia (absolute neutrophil count 0.2 × 103/μL). Daptomycin 8 mg/kg/day was then initiated with rifampin 300 mg twice daily; treatment was discontinued after 49 days due to an elevated creatine kinase level of 1831 U/L (baseline 86). Intravenous meropenem 1 g every 8 hours was again initiated on day 83 following additional identification of quinolone-resistant Pseudomonas aeruginosa from the soft tissue of the right foot. Intravenous vancomycin 1 g every 12 hours was also restarted at this time for persistent coagulase-negative Staphylococcus and oral rifampin 300 mg twice daily was again added. Adverse events again required the discontinuation of vancomycin on day 91. The eventual drug therapy regimen consisted of telavancin 750 mg/day for 42 days, meropenem for 50 days, and oral rifampin for 50 days. At the end of treatment, the patient's right heel wound had almost completely closed. He was without recurrence or treatment-related adverse events at follow-up 1 year later.
DISCUSSION:
Antimicrobial selection for osteomyelitis infections presents a challenge to the clinician due to patient intolerance, increasing antimicrobial resistance, and variable antimicrobial penetration at the site of infection. To our knowledge, this is the first case report of the successful use of a regimen including telavancin for the treatment of a recurrent, coagulase-negative Staphylococcus osteomyelitis infection.
CONCLUSIONS:
In this complex case involving a polymicrobial infection of the right calcaneal bone and surrounding soft tissue, eventual drug therapy including telavancin, meropenem, and rifampin resulted in a successful clinical response.
Patients with chronic osteomyelitis typically experience a painful and prolonged course of infection, as well as the potential for amputation if treatment is not successful. While appropriate treatment regimens are determined by culture and susceptibility results, therapy decisions are also influenced by the properties of antimicrobials such as spectrum, rate and extent of penetration into the bone tissue, safety, and the potential for administration of therapy in an outpatient setting.1,2 In most patients, antimicrobial therapy is coupled with surgical debridement. 3 Surgical debridement improves antimicrobial efficacy by removing the nidus of infection, improving granulation, enhancing the immunologic status of the wound, and removing necrotic tissue. 4
Patients with multidrug-resistant infections and/or intolerance to one or more drug classes can present a special challenge when considering antimicrobial therapy. The incidence of multidrug-resistant nosocomial infections continues to rise in the US. Increasing prevalence of methicillin resistance in Staphylococcus spp. has been observed over the past decade and, similarly, other organisms such as Pseudomonas aeruginosa have demonstrated resistance to antimicrobials. 5 Pathogens commonly identified in chronic osteomyelitis infections include methicillin-resistant Staphylococcus aureus (MRSA), coagulase-negative Staphylococcus, and quinolone-resistant P. aeruginosa. 6
We report the extensive clinical course of a patient with polymicrobial osteomyelitis who had an inadequate clinical response and developed intolerance to several antimicrobial regimens. The calcaneal osteomyelitis was eventually successfully treated with a combination of telavancin, rifampin, meropenem, and hyperbaric oxygen treatments.
Case Report
An 18-year-old male with L4 myelomeningocele, neurogenic bladder, and a gait resulting in abnormal heel pressure presented with a complex history involving recurrent right heel infections with chronic calcaneus osteomyelitis. Three months prior to this presentation, he had undergone multiple courses of antimicrobial therapy, including ciprofloxacin, amoxicillin/clavulanate, minocycline, ertapenem, vancomycin, and daptomycin for osteomyelitis with abscess formation in the right calcaneus. On previous discharge, he was placed on oral minocycline for suppressive therapy, and the heel was well healed, with no erythema, warmth, or tenderness.
At this presentation, the patient described a 1-month history of induration of the right heel; magnetic resonance imaging demonstrated a large fluid collection. The patient exhibited decreased lower leg muscle tone, bilateral lower leg weakness, and limited bilateral ankle flexion. The patient was ambulatory on crutches. Abscess cultures grew coagulase-negative Staphylococcus resistant to tetracycline and trimethoprim/sulfamethoxazole, eliminating these 2 agents as possible oral suppressive therapy. Debridement of the wound was performed in the hospital and vancomycin 1 g (13 mg/kg) intravenously every 12 hours was started. This was continued upon discharge to the physician outpatient infusion center and pharmacy. Trough concentrations of 15-20 μg/mL were targeted for vancomycin, with dosing performed by the pharmacy. At the time of therapy initiation, the patient's serum creatinine was 0.8 mg/dL and creatinine clearance, calculated using his ideal body weight and the Cockcroft-Gault method, was 155 mL/min. 7 Intravenous medications were prepared in the on-site pharmacy and the patient was taught to self-administer the medications via a peripherally inserted central catheter (PICC) in his left arm, which was inserted during hospitalization. Weekly laboratory indices included a complete metabolic panel, erythrocyte sedimentation rate, and vancomycin trough concentrations. Cultures of bone and soft tissue taken intraoperatively were returned, also indicating infection with coagulase-negative Staphylococcus. Due to patient availability on day 13, a random vancomycin concentration was measured instead of a trough concentration. The concentration obtained 4 hours after dose administration was 21.3 μg/mL, and the dose was increased to 1.5 g (19 mg/kg) every 12 hours. Oral rifampin 300 mg every 12 hours was also added to the regimen for potential synergy. 8
On day 22 the patient experienced leukopenia (white blood cell [WBC] count 3.0 × 10 3 /μL) and severe neutropenia (absolute neutrophil count [ANC] 0.2 × 10 3 /μL). The vancomycin trough concentration was 7.4 μg/mL. Neutropenia was determined to be related to vancomycin therapy (probable causality according to the Naranjo probability scale 9 ), and both vancomycin and rifampin were discontinued. Due to the severity of the neutropenia and the serious nature of the infection, granulocyte colony-stimulating factor (G-CSF) 300 μg was also started at this time (Figure 1). 10
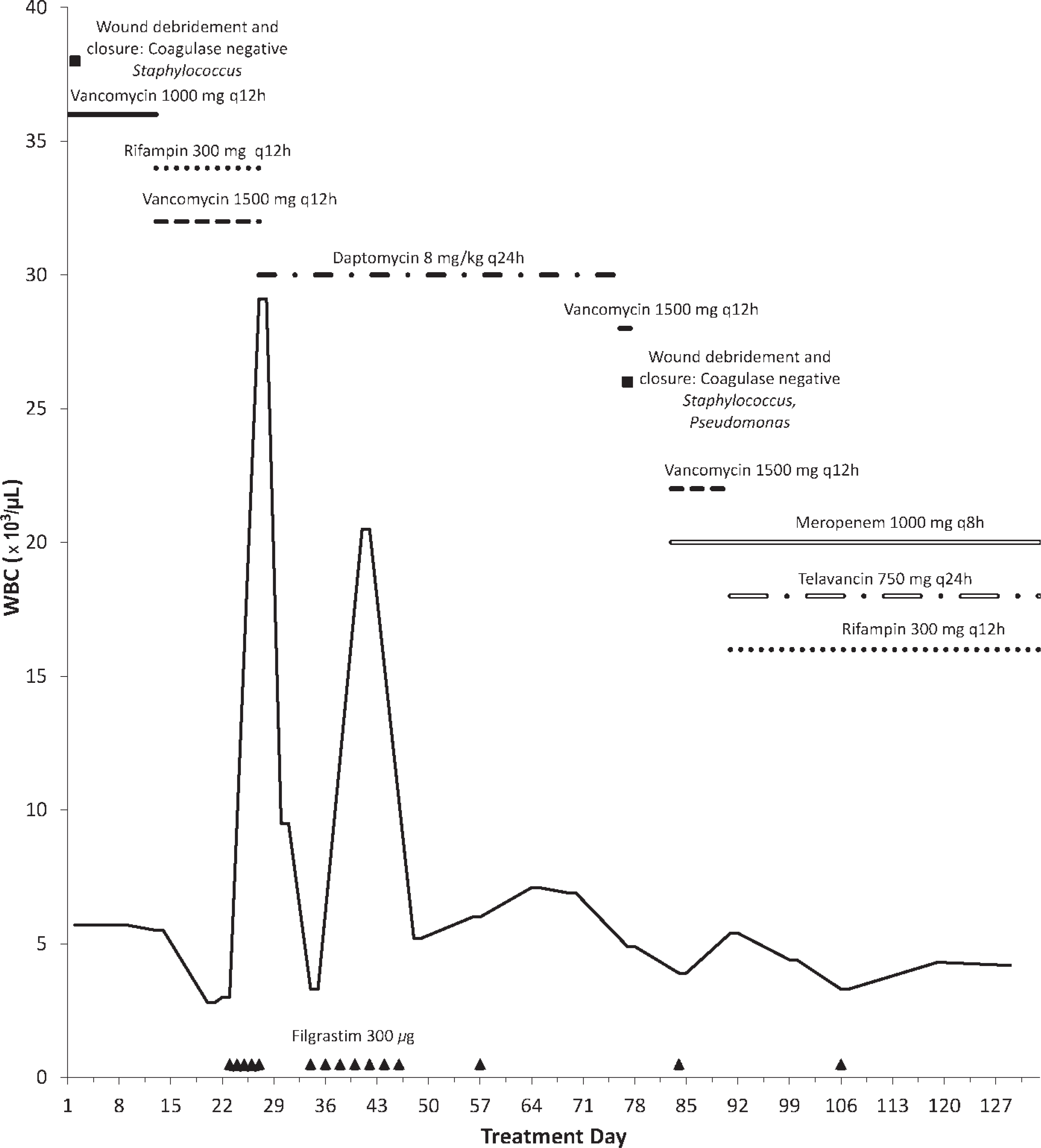
Relationship of white blood cell (WBC) count to therapy regimen by treatment day.
Daptomycin was then initiated at 8 mg/kg/day and the oral rifampin was restarted. The potential for bone marrow suppression was concerning; G-CSF dosing was continued on an as-needed basis as indicated by WBC count and ANC. By day 34, the wound was smaller, with healthy granulation tissue and no exudates.
On day 76, after 49 days of daptomycin, therapy was discontinued due to creatine kinase elevation of 1831 U/L from a baseline of 86 U/L (probable causality according to the Naranjo probability scale 9 ). Additionally, the patient had developed greenish, yellow drainage from the right heel wound. Oral ciprofloxacin was started and debridement was performed in the hospital the following day, with vancomycin given perioperatively. Both tissue and bone cultures taken intraoperatively grew quinolone-resistant, carbapenem-susceptible P. aeruginosa, and coagulase-negative Staphylococcus. Although the patient was continuing to experience some bone marrow suppression, results of bone cultures taken intraoperatively indicated the organism was susceptible to vancomycin and a trial of vancomycin was initiated in the inpatient facility. On day 83, therapy was reinitiated with intravenous vancomycin 1.5 g every 12 hours with the addition of intravenous meropenem 1 g every 8 hours, and oral rifampin 300 mg twice daily. Hyperbaric oxygen treatments were also added. He was then discharged from the hospital 7 days after debridement, with vancomycin and meropenem again provided through the physician outpatient infusion center and pharmacy for self-administration at home. Evaluations by the physician, changes to the PICC dressing, and drawing of blood for laboratory tests were performed in the physician's office.
On day 91 of therapy, vancomycin was discontinued due to continued bone marrow suppression and generalized pruritus. Telavancin 750 mg/day (approximately 10 mg/kg/day) was added to the meropenem/rifampin regimen to provide coverage for the coagulase-negative Staphylococcus.
On day 98 of antimicrobial therapy, the patient returned to the physician outpatient infusion center for a follow-up visit. The patient had received 2 hyperbaric oxygen treatments and the wound was dry. The patient reported taste disturbance, lasting for about an hour after the telavancin infusion, but resolving spontaneously. The patient indicated to the physician and pharmacist that this did not result in missed doses and he confirmed adherence to the entire antimicrobial regimen. On day 101, the patient developed chills, followed by a fever of up to 38.9 °C, which was associated with fatigue and malaise after the antimicrobial infusions. In accordance with the Centers for Disease Control and Prevention guidelines for the prevention of intravascular catheter–related infections, the PICC inserted into his left arm was removed and replaced with a PICC in his right arm. 11 The patient returned home to resume antimicrobial therapy, and fever and associated symptoms were completely resolved upon his return visit on day 105. The results of the PICC tip and blood cultures obtained during removal were negative.
On day 106 of antimicrobial treatment, the physician noted during evaluation that the surgical wound had healed well with no signs of acute inflammation and the patient was afebrile. The patient did note some continued dysgeusia and slightly diminished appetite after administration of telavancin. A WBC count of 3.3 × 10 3 /μL and ANC of 1.3 × 10 3 /μL indicated mild leukopenia and neutropenia and the patient was given 1 dose of G-CSF 300 μg. The relationship of WBC count to therapy regimen is noted in Figure 1.
During the visit on day 119, the wound on the patient's right heel was almost closed, although he was still not placing weight on the foot. Hyperbaric oxygen treatments were continued. On day 126, during the physician visit, the surgical wound was noted as well healed with no signs of acute inflammation of the right heel. Laboratory indices were stable, but WBC count and ANC continued to be closely monitored. No other adverse reactions were seen with antimicrobial therapy. Intravenous antimicrobial treatment was extended for 1 more week along with continued hyperbaric oxygen treatments.
On day 133, meropenem, telavancin, and rifampin were discontinued after completing 42 days of telavancin, 50 days of meropenem and rifampin therapy, and 20 hyperbaric oxygen treatments. At this time, the patient's right heel wound had almost completely closed. The PICC was removed and the patient was discharged from the physician outpatient infusion clinic and pharmacy. He was without recurrence or treatment-related adverse events at follow-up 1 year later.
Discussion
Chronic osteomyelitis is an infection of the bone generally lasting longer than 10 days and is associated with inflammation and necrosis of the bone. 6 Infection of healthy bone is uncommon and is usually a result of trauma, the presence of a foreign body, or vascular insufficiency. 12 Calcaneal osteomyelitis may initially be mistaken for a more benign condition such as a sprain; this, combined with a more subtle onset, may lead to a delay in diagnosis and result in a more complicated clinical course. 13 Osteomyelitis infections are commonly treated with parenteral administration of antimicrobials and surgical debridement. 14
Chronic osteomyelitis due to Staphylococcus, including Staphylococcus-infected surgically implanted devices and foreign bodies, has been well studied. 15 Multidrug-resistant strains of S. aureus, such as MRSA and others, present an ever-increasing challenge to clinicians designing antimicrobial therapy regimens.5,16 The emergence of community-acquired MRSA coincided with an increase in the diagnosis of osteomyelitis in children (from 2.6 to 6 per 1000 admissions between 2000 and 2004), an increase in the length of hospitalizations, and an increase in the length of recorded fevers; this indicates an increase in both incidence and severity of community-acquired MRSA. 17
Coagulase-negative Staphylococcus has been long regarded as an organism with low pathogenicity. Awareness of the virulence of coagulase-negative Staphylococcus infections has steadily increased over the last decade. Although most commonly reported as a causative agent in bone infections due to prosthetic joint infections, coagulase-negative Staphylococcus is also prevalent in osteomyelitis. 18 Treatment can be challenging due to a high rate of resistance to a number of antimicrobial agents.19,20 The optimal route of administration has not been established, but parenteral therapy is often used initially. 21
Glycopeptides, primarily intravenous vancomycin, are common first-line agents due to the adequate bone concentration achieved, although increased failures may be seen as vancomycin resistance increases.22–24 Vancomycin was clinically effective in our patient, but consistently caused severe neutropenia and leukopenia, as well as pruritus during the second course, resulting in discontinuation. Vancomycin-related neutropenia is estimated to occur at rates between 2% and 12%, and generally necessitates discontinuation of the drug. While no current guidelines are available for the use of G-CSF for vancomycin-induced neutropenia, treatment of vancomycin-induced neutropenia with G-CSF has been previously reported.10,25
Daptomycin, a cyclic lipopeptide effective against Staphylococcus strains, is another option, particularly suitable for outpatient use. Daptomycin was discontinued in our patient due to the development of asymptomatic elevation of creatine kinase to 1831 U/L. 26 Wound improvement was also not seen with daptomycin, but susceptibility tests were not performed to rule out potential nonsusceptibility, which has also been reported.27,28
Telavancin is a novel lipoglycopeptide that received Food and Drug Administration approval in late 2009 for the treatment of complicated skin and skin structure infections. 29 Although telavancin has not been studied for osteomyelitis in humans, it is structurally similar to the glycopeptide vancomycin, which is currently the parenteral drug of choice for complicated skin and skin structure infections as well as resistant osteomyelitis infections.23,30 Telavancin was developed as an alternative therapy for gram-positive infections to alleviate concerns over limited treatment options and the development of vancomycin-resistant S. aureus and vancomycin-intermediate S. aureus. Although structurally similar to vancomycin, telavancin contains additional hydrophobic and hydrophilic functional groups. 31 Telavancin has 2 proposed mechanisms of action, including inhibition of bacterial cell wall synthesis and depolarization of the bacterial cell membrane. 31 For skin and soft tissue infections, telavancin has the same clinical efficacy as vancomycin, but with the advantage of once-daily administration and a different adverse effect profile. A study comparing telavancin and vancomycin demonstrated equivalent efficacy for treatment of complicated skin and skin structure infections, with trends favoring telavancin for clinical cure and microbiologic eradication. 32 In a comparative surveillance study of telavancin activity against gram-positive clinical isolates in the US, telavancin had activity against vancomycin-susceptible enterococci (MIC90 1 μg/mL), vancomycin-intermediate S. aureus (MIC90 0.5-1.0 μg/mL), and vancomycin-resistant S. aureus strains (MIC90 1.0-4.0 μg/mL). In an international surveillance study of staphylococcal clinical isolates from 2007-2008, including 5726 S. aureus and 1808 coagulase-negative staphylococci with multidrug-resistant isolates, telavancin showed 2- to 8fold lower MIC90 results than comparators (daptomycin, quinupristin/dalfopristin, vancomycin, and linezolid). 33 The only published study concerning the efficacy of telavancin for treatment of bone infections is on a rabbit model. In rabbit bone, telavancin displayed comparable efficacy to vancomycin and linezolid for osteomyelitis due to MRSA. 34 Landersdorfer et al. reported ratios of 0.1-0.6 mean bone:serum concentration for glycopeptides based on studies using vancomycin and teicoplainin. 35 The known bone penetration of similar glycopeptides combined with the studies of telavancin in the rabbit model suggest telavancin is likely to penetrate into bone. One recent case report published by Twilla et al. noted the successful use of telavancin in 4 patients for treatment of methicillin-resistant Staphylococcus aureus osteomyelitis, reinforcing our use of telavancin. 36 Thus, in our patient with a multidrug-resistant infection who was unable to tolerate prior vancomycin and daptomycin therapies, telavancin was selected to provide gram-positive coverage and combined with oral rifampin for synergy. 8 Renal dysfunction with telavancin was reported in 3% of patients treated for skin and soft tissue infections, although the prevalence has been noted to be higher in patients with risk factors. Risk factors for renal dysfunction associated with telavancin include preexisting renal dysfunction and the concomitant use of medications known to affect renal function. 37 Our patient was young with no risk factors. His creatinine clearance remained normal throughout therapy (204 mL/min upon discharge) and no renal adverse events were observed.
Quinolone-resistant P. aeruginosa occurs most often in hospitals and nursing homes, and typically in patients who are immunosuppressed or have other significant comorbidities.38,39 When susceptible, ciprofloxacin or levofloxacin are suggested as the primary treatment for P. aeruginosa osteomyelitis. Recommended alternatives are ceftazidime or cefepime for treatment of quinolone-resistant Pseudomonas. Meropenem is a broad-spectrum carbapenem antimicrobial also commonly used for resistant Pseudomonas spp. infections. 40 Although it is not suggested as a first-line therapy for the treatment of osteomyelitis, detectable concentrations of meropenem in bone, as well as the successful use of meropenem in chronic osteomyelitis, have been reported.35,41 In our patient, P. aeruginosa was resistant to fluoroquinolones; therefore, meropenem was selected to provide P. aeruginosa coverage.
The lack of clinical data on alternative therapies for osteomyelitis can result in severely limited options for patients with multidrug-resistant infections. Here, we report a case of a recurrent multidrug-resistant calcaneal infection successfully treated with a regimen including telavancin, meropenem, rifampin, surgical debridement, and hyperbaric oxygen. These data, along with a positive patient outcome, indicate the effectiveness of meropenem for the treatment of multidrug-resistant P. aeruginosa osteomyelitis and telavancin for treatment of recurrent coagulase-negative staphylococcal osteomyelitis.