
Abstract
OBJECTIVE:
To review the current literature on the risk of venous thromboembolism (VTE) in patients with chronic liver disease (CLD).
DATA SOURCES:
Literature was accessed through MEDLINE/PubMed (1996-December 2011) using the search terms liver disease, cirrhosis, venous thromboembolism, deep vein thrombosis, and pulmonary embolism.
STUDY SELECTION AND DATA EXTRACTION:
Relevant observational and population-based studies were included to present background information. Bibliographies of all relevant articles were reviewed for additional citations.
DATA SYNTHESIS:
Liver disease affects the synthesis of procoagulants and anticoagulants, resulting in hemostatic alterations and abnormal laboratory values. Retrospective studies characterized the VTE incidence to be 0.5-6.3%. Population-based studies reported VTE relative risks of 1.74-2.10 in patients with CLD compared with population controls and VTE odds ratios of 0.9-1.39 for hospitalized patients with CLD compared with controls without liver disease. There is a paucity of data on the use of pharmacologic prophylaxis in patients with CLD.
CONCLUSIONS:
Patients with CLD should be assessed for VTE risk and given VTE prophylaxis when the benefits outweigh the risks. Diagnoses of CLD or elevated international normalized ratio do not confer protection against development of VTE and do not justify withholding pharmacologic prophylaxis based on this diagnosis.
Request
Should patients with chronic liver disease (CLD) receive venous thromboembolism (VTE) prophylaxis during hospitalization?
Response
BACKGROUND
The reported rate of VTE in hospitalized patients is 4-15%, an 8-fold increase over that in the general population.1,2 Development of VTE leads to significant morbidity and mortality. In the US, the estimated number of annual VTE-related deaths is between 100,000 and 300,000, and the associated cost for VTE is from $5 billion to $26.7 billion per year. 3 The risk of VTE is decreased by 40-60% when pharmacologic prophylaxis is used in hospitalized medical patients. 1 Guidelines recommend using pharmacologic prophylaxis (low-molecular-weight heparin [LMWH], low-dose unfractionated heparin [UFH], or fondaparinux) in patients with risk factors for VTE unless a contraindication is present. When a contraindication exists, mechanical prophylaxis should be used. 4 Ongoing research continues to explore the risks and benefits of pharmacologic and mechanical prophylaxis in hospitalized medical patients.5,6
The liver is responsible for the synthesis and elimination of multiple factors necessary for maintaining hemostasis, including those involved in coagulation, fibrinolysis, platelet production, and adhesion. Hemostatic alterations resulting in hypocoagulability have long been recognized in patients with CLD. These include decreased vitamin K clotting factors (factors II, V, VII, IX, X, and XI) and platelet production; these deficiencies are demonstrated on routine laboratory tests such as decreased platelet count and elevated prothrombin time, international normalized ratio (INR), and partial thromboplastin time (PTT) (Table 1).7,8 These tests reflect the deficiencies of procoagulants but not the alterations in concentrations of anticoagulants. It was once thought that these findings represented an endogenous coagulopathy that may confer protection against VTE development. More recent data show that these routine laboratory tests correlate poorly with clinical bleeding rates during procedures in patients with CLD, suggesting that they do not reflect the complexity of hemostatic alterations.9–11 Patients with CLD also have increased levels of procoagulants (factor VIII, von Willebrand factor) and decreased levels of anticoagulants (protein C, protein S, antithrombin, plasminogen), which lead to hypercoagulability. These procoagulant alterations are not observed on routine laboratory tests but have been demonstrated by using thrombin-generation tests to compare the thrombin activity in the presence and absence of thrombomodulin or by using snake-venom extract.7,8 Patients with CLD have a propensity to bleed during procedures or from varices but also are at increased risk to develop clots, most often observed as portal vein thromboses. To explain this duality, it has been proposed that patients with CLD have a “rebalanced” hemostasis, with reduced capacity to respond to external stressors.7,8
Hemostatic Alterations in End-Stage Liver Disease
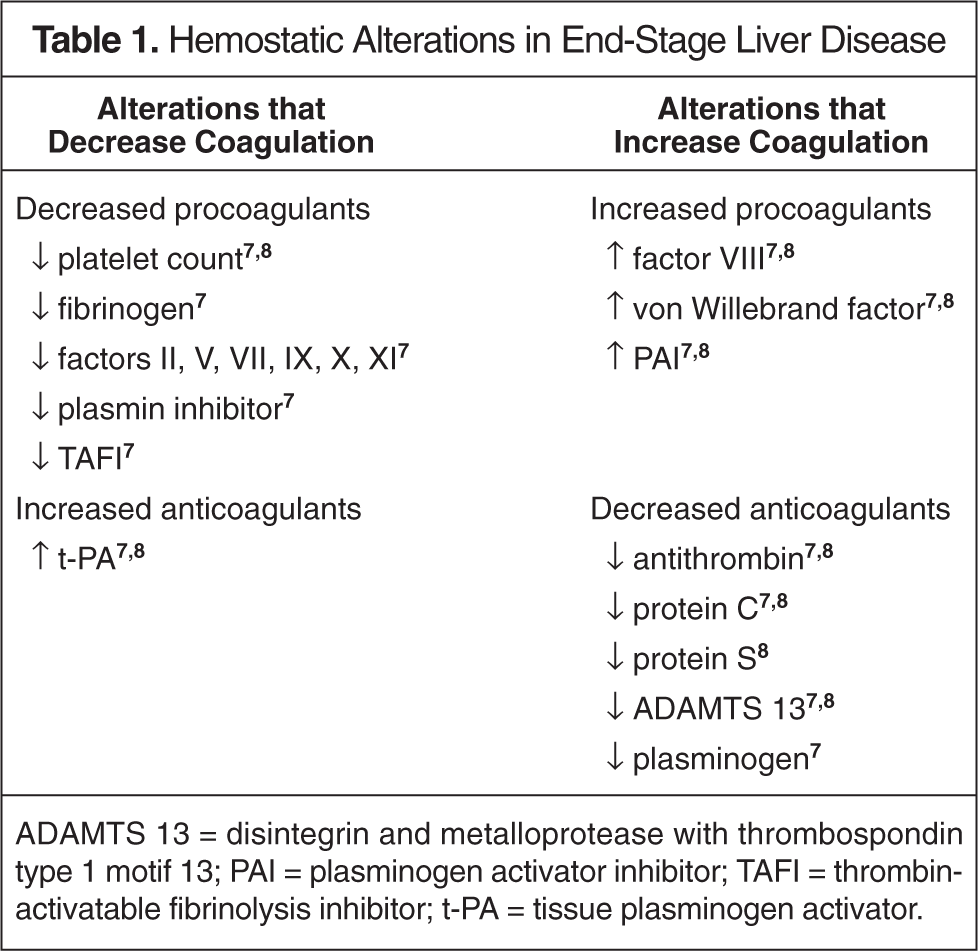
ADAMTS 13 = disintegrin and metalloprotease with thrombospondin type 1 motif 13; PAI = plasminogen activator inhibitor; TAFI = thrombin-activatable fibrinolysis inhibitor; t-PA = tissue plasminogen activator.
A subgroup analysis from a population-based, nested case-control study conducted by Heit and colleagues indicated that patients with “serious liver disease” were at a decreased risk of VTE (odds ratio [OR] 0.1; 95% CI 0.01 to 0.71). 12 Serious liver disease was not clearly defined in this study; only 5 subjects in the case group and 6 patients in the control group (<1% of total study population) were included in this subgroup. Nonetheless, these findings contributed to the question: Are patients with CLD protected from developing VTE because they are “auto-anticoagulated”?
Contrary to this evidence, a case-cohort study of similar design to that of the trial by Heit and colleagues did not find CLD (n = 68) to be protective against the development of VTE (OR 1.65; 95% CI 0.97 to 2.82), leaving clinicians to wonder about the true impact of CLD on the risk of developing VTE and the usefulness of prophylactic measures. 13
LITERATURE REVIEW
Six recent studies have characterized the incidence of VTE in patients with CLD (Table 2).14–19 The first study identified 113 new VTE events in more than 21,000 (0.5%) admissions involving patients with CLD to 1 academic medical institution over 8 years. 14 A multivariate logistic regression model revealed that serum albumin was the only independent predictor of VTE (OR 0.24; 95% CI 0.10 to 0.55; p < 0.001) in patients with CLD. The mean albumin was 2.85 g/dL in the VTE group and 3.10 g/dL in those without VTE. A small retrospective chart review from a single center had similar findings, reporting that 17 of 2074 (0.8%) patients hospitalized for CLD had a VTE diagnosis. 15 There was no comparator group in this study and no regression analysis was performed.
Retrospective Single-Center Studies
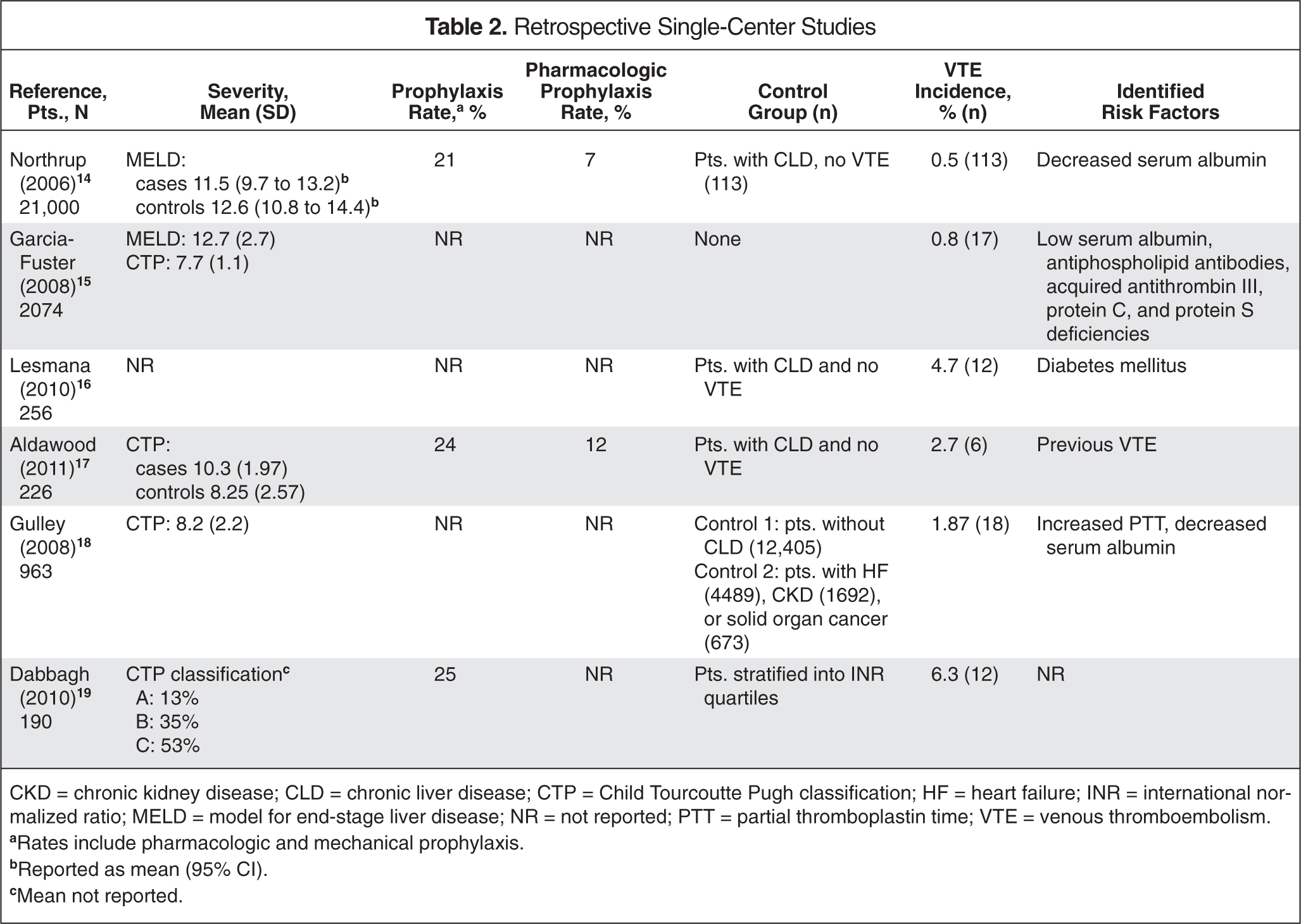
CKD = chronic kidney disease; CLD = chronic liver disease; CTP = Child Tourcoutte Pugh classification; HF = heart failure; INR = international normalized ratio; MELD = model for end-stage liver disease; NR = not reported; PTT = partial thromboplastin time; VTE = venous thromboembolism.
Rates include pharmacologic and mechanical prophylaxis.
Reported as mean (95% CI).
Mean not reported.
More recent studies with similar designs have reported higher incidences of VTE. One review of 256 admissions for CLD to a single center over 3 years reported a 4.7% incidence of deep vein thrombosis (DVT). 16 Diabetes mellitus was found to be an independent risk factor for VTE in patients with CLD (OR 3.88; 95% CI 1.135 to 13.26; p = 0.031). Another study reported a 2.7% incidence in 226 patients with CLD hospitalized over a 1-year period. 17 More patients who developed VTE during the observation period had a history of VTE; no independent risk factors for VTE were identified. These 2 studies also reported a higher proportion of patients with CLD secondary to viral hepatitis than did the previous studies.
Gulley and colleagues took a different approach to selecting control groups to estimate the risk of VTE in patients with CLD. Using a health system database, 962 patients with CLD were compared with 2 control groups: (1) those without CLD but with comorbidities that conferred an increased risk of VTE (heart failure; chronic kidney disease; and lung, breast, prostate, or colon cancer), and (2) those without CLD or any of these comorbidities. 18 The incidence of VTE over the 10-year period was higher in patients with CLD (1.87%) than in those without CLD or high-risk comorbidities (0.98%; OR 1.78; 95% CI 1.1 to 2.2; p = 0.007) but lower than in those with high-risk comorbidities (heart failure 7.75%, OR 0.23; 95% CI 0.14 to 0.37; chronic kidney disease 7%, OR 0.25; 95% CI 0.15 to 0.41; and cancer 6.1%, OR 0.29; 95% CI 0.17 to 0.52). Decreased serum albumin (OR 0.36; 95% CI 0.87 to 0.97; p = 0.001) and increased PTT (OR 0.89; 95% CI 0.87 to 0.97; p = 0.04) were found to be independent predictors of VTE in a multivariate analysis.
Dabbagh and colleagues 19 evaluated the relationship between INR and the development of VTE in patients with CLD. While INR had not been identified as a predictor of VTE risk in any of the prior studies, the observation of elevated INRs was one of the cornerstones of the “auto-anticoagulation” argument. This study stratified 190 patients with CLD into INR quartiles and compared the VTE incidence among them. 19 The overall VTE incidence was 6.3%, the highest published to date. There was no significant difference in the incidence of VTE between INR quartiles. Half of the VTE cases occurred in patients with an INR greater than 1.6 and the risk of VTE persisted in patients with an INR greater than 2.2.
These studies are all limited by their retrospective design and reliance on accurate medical coding; most of the studies did not include a comparator group. Inconsistencies in reporting of liver disease severity and VTE prophylaxis rates also make it difficult to compare results among the studies. However, the data indicate that patients with CLD are at risk for development of VTE.
The largest studies published to date on this topic are 2 population-based cohort studies (Table 3). Using the Danish registry system, Sogaard and colleagues published a population-based case-control study that included more than 99,000 patients with VTE, identified over 25 years. 20 The relative risk for VTE compared with general population controls was determined in 2 subtypes of CLD: cirrhotic liver disease (RR 1.74; 95% CI 1.54 to 1.95) and noncirrhotic liver disease (RR 1.87; 95% CI 1.54 to 1.95). When limited to unprovoked VTE, excluding diagnoses of cancer, fractures, trauma, pregnancy, and surgical procedures, the relative risks increased to 2.06 (95% CI 1.79 to 2.38) in patients with cirrhotic liver disease and 2.10 (95% CI 1.91 to 2.31) in patients with noncirrhotic liver disease.
Population-Based Studies
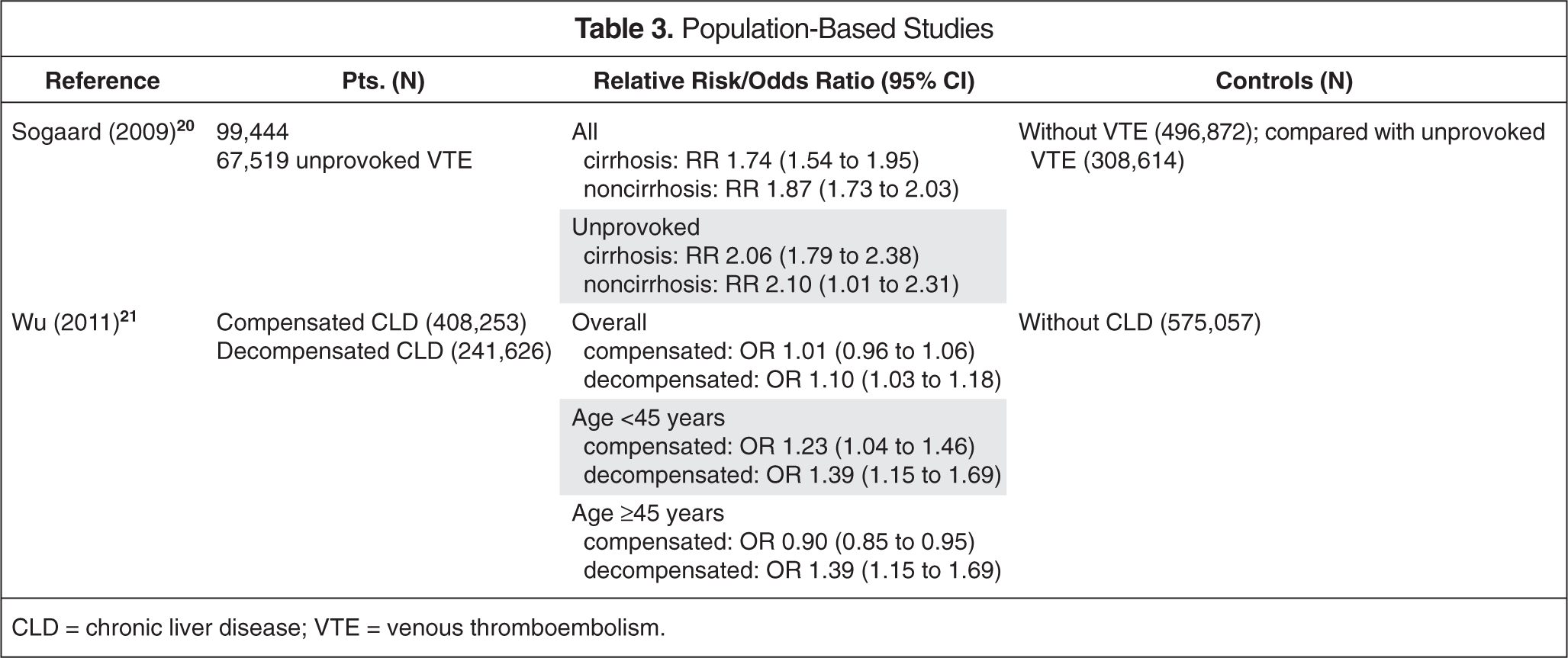
CLD = chronic liver disease; VTE = venous thromboembolism.
A similar study by Wu and Nguyen used the US Nationwide Inpatient Sample and identified 408,253 patients with compensated CLD; 241,626 with decompensated CLD, defined by the presence of ascites or variceal bleeding; and 575,057 matched controls admitted to participating inpatient facilities over 8 years. 21 While the study by Sogaard and colleagues 20 did not differentiate between patients who were admitted to the hospital and those who were not, this study identified events that occurred in an inpatient setting only. This study reported that, until the age of 45, those with compensated (OR 1.23; 95% CI 1.04 to 1.46) or decompensated (OR 1.39; 95% CI 1.15 to 1.69) CLD had a higher prevalence of VTE than did controls. Among patients older than 45, there was no significant difference in the rate of VTE between patients with decompensated CLD and controls (OR 0.97; 95% CI 0.91 to 1.04), but patients with compensated CLD who were older than 45 were at a slightly lower risk of developing VTE than were controls (OR 0.90; 95% CI 0.85 to 0.95). This may be a reflection that the VTE risk in the control group increases with age until it equals the risk of VTE conferred by CLD in younger patients. The mean ages reported in the previously published studies were all greater than 45 years (range 51-69); no studies identified a relationship between VTE incidence and age.14–19
Population-based studies have the advantage of large sample sizes, which can reduce the impact of many confounding factors. However, these studies are reliant on adequate coding of medical diagnoses and lack much detail about patients' clinical courses. Neither of these studies addressed the severity of CLD or rates of VTE prophylaxis. However, when viewed with the support of the previously described retrospective studies, they add to the data suggesting that patients with CLD are not at decreased risk for VTE compared with the general population.
Pharmacologic VTE Prophylaxis
To date, there are no data comparing the efficacy or risk of using pharmacologic prophylaxis in patients with CLD with that of other hospitalized patients. Three of the retrospective studies previously discussed reported the rate of prophylaxis to be 21-25% in patients with CLD,14,17,19 which is lower than the rate of 30-70% reported for general hospitalized medical patients.1,2,22 Dabbagh and colleagues found no difference in VTE rates between patients who received prophylaxis and those who did not in a secondary analysis, with less than one fourth of the study population receiving prophylaxis. 19 The proportion of patients receiving pharmacologic versus mechanical prophylaxis was not described. Future studies addressing this issue are critical to determine whether patients with CLD would benefit from receiving routine pharmacologic VTE prophylaxis.
The potential effects of CLD on metabolism of anticoagulants should be considered before pharmacologic therapy is recommended. A prospective observational study using anti-Xa monitoring to evaluate the pharmacokinetics of LMWH in patients with CLD included 75 patients receiving enoxaparin for VTE prophylaxis.23,24 Although none of these patients developed a thrombotic event, only 11 (15%) achieved recommended anti-Xa levels for prophylactic dosing (0.3-0.4 IU/mL). Five patients (7%) developed bleeding complications but none achieved recommended anti-Xa levels. This reported bleeding incidence is similar to that of previous studies in hospitalized patients with CLD who were not receiving anticoagulation. 25 The authors concluded that, although enoxaparin seems to be safe in patients with CLD, the usefulness of anti-Xa monitoring to determine enoxaparin dosing in this population has yet to be established. Based on this evidence, using anti-Xa levels to evaluate clinical safety or efficacy in patients with CLD is not recommended.
Discussion
Current literature has reported a VTE incidence of 0.5-6.3% in patients with CLD and a relative risk of 1.74-2.10, compared with population controls.14–20 The only results suggesting reduced VTE risk among those with CLD are from the study by Wu and Nguyen in the subset of hospitalized patients older than 45 with compensated CLD 21 ; this finding needs to be substantiated with further research. The data to date suggest that CLD is not protective against the risk of developing VTE.
Low serum albumin,14,18 high PTT, 18 and diabetes mellitus 16 have been identified as independent risk factors for the development of VTE in this CLD patient population, while INR has not been shown to correlate with the development of VTE. 19 CLD is only one of many risk factors to be considered in the development of VTE; other factors include age, comorbidities, and lifestyle. Further research focusing on independent risk factors of VTE in patients with CLD may help identify patients who would benefit the most from VTE prophylaxis.
Many outstanding issues exist when determining the risks and benefits of VTE prophylaxis in patients with CLD. Is the protection afforded by prophylactic anticoagulation the same in this population as in general hospitalized medical patients? Are the risks, particularly of bleeding, of using these agents affected by the presence of CLD? Is one prophylactic agent better for use in patients with CLD than another? More research in this area is needed before these questions can be answered.
Summary
Until more evidence on the use of VTE prophylaxis in hospitalized patients with CLD is available, the same procedures for assessing VTE risk and providing appropriate prophylaxis used with other hospitalized medical patients should be followed in patients with CLD.4,5 When indicated, based on risk factor assessment, VTE prophylaxis should not be withheld solely on the basis of CLD or elevated INR. Patients who have risk factors for VTE should be placed on pharmacologic prophylaxis with LMWH, UFH, or fondaparinux, unless contraindicated. If pharmacologic prophylaxis is contraindicated, patients should receive mechanical prophylaxis.