
Abstract
BACKGROUND:
An up-to-date assessment of dipeptidyl peptidase-4 (DPP-4) inhibitors is needed to include newly available data.
OBJECTIVE:
To assess the efficacy and safety of DPP-4 inhibitors, including sitagliptin, saxagliptin, vildagliptin, and linagliptin, in type 2 diabetes.
METHODS:
We conducted a search of MEDLINE for randomized controlled trials (RCTs) of DPP-4 inhibitors in type 2 diabetes through November 2011, using the key terms sitagliptin, saxagliptin, vildagliptin, and linagliptin. We also searched for completed, but unpublished, trials at relevant web sites. RCTs were selected for meta-analysis if they (1) compared DPP-4 inhibitors with placebo or an antihyperglycemic agent; (2) had study duration of 12 or more weeks; (3) had 1 or more baseline and posttreatment efficacy and/or safety outcome; and (4) were published in English.
RESULTS:
In 62 evaluated articles, DPP-4 inhibitors lowered hemoglobin A1c (A1C) significantly more than placebo (weighted mean difference [WMD] −0.76%; 95% CI −0.83 to −0.68); however, heterogeneity was substantial (I2 = 82%). Exclusion of Japanese trials (n = 7) resulted in a reduction of heterogeneity (I2 = 59%). In the non-Japanese RCTs (n = 55), DPP-4 inhibitors were associated with a reduction in A1C (WMD −0.65%; 95% CI −0.71 to −0.60) but higher risk of hypoglycemia (odds ratio [OR] 1.30; 95% CI 1.00 to 1.68) compared to placebo. The 7 Japanese-specific RCTs showed a greater reduction in A1C (WMD −1.67%; 95% CI −1.89 to −1.44) and a nonsignificant increase in risk of hypoglycemia (OR 1.41; 95% CI 0.51 to 3.88) with DPP-4 inhibitors versus placebo. When comparing DPP-4 inhibitors to active comparators, the I2 was still high after deleting Japanese studies. In these 17 active comparator trials, there was no significant difference in A1C reduction (WMD 0.04%; 95% CI −0.09 to 0.16) or risk of hypoglycemia (OR 0.60; 95% CI 0.22 to 1.61) for DPP-4 inhibitors compared to other antihyperglycemics. There were similar odds of any or serious adverse events with DPP-4 inhibitors compared to placebo, but a decreased risk compared to other antihyperglycemics.
CONCLUSIONS:
DPP-4 inhibitors were associated with a reduction in A1C with comparable safety profiles compared to placebo, but no significant difference in A1C compared to other hyperglycemics. Differences in efficacy and safety were observed between Japanese and non-Japanese patients.
Dipeptidyl peptidase-4 (DPP-4) inhibitors work by enhancing endogenous glucagon-like peptide and glucose-dependent insulinotropic polypeptide, which are hormones released in response to food intake. The enhancement leads to insulin secretion by pancreatic β-cells, reduction in glucagon secretion, and reduction in liver glucose production. 1 Four DPP-4 inhibitors are available in the US and European Union: sitagliptin, 2 saxagliptin, 3 and linagliptin 4 (approved by the Food and Drug Administration [FDA] in 2006, 2009, and 2011, respectively), and vildagliptin (not approved by FDA, but granted marketing authorization in the European Union in 2007 5 ). Several factors perpetuate the need for further assessment of the efficacy and safety of DPP-4 inhibitors. First, the use of these agents is debated. DPP-4 inhibitors are considered as later-line treatment per the consensus algorithm of the American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD). 6 The main reason behind the later placement was the high expense and lack of long-term safety information. In contrast, the 2009 algorithm by the American Association of Clinical Endocrinologists/American College of Endocrinology placed DPP-4 inhibitors second-line after metformin for monotherapy and first-line with metformin for combination therapy. 7 Recent clinical guidelines issued by the National Institute for Health and Clinical Excellence recommend DPP-4 inhibitors as second-line therapy (after metformin) in place of sulfonylurea agents in patients at significant risk for hypoglycemia or its consequences. 8 Furthermore, there is a new concern with thiazolidinediones, which were previously used as second-line agents. The FDA recently announced restriction of the use of rosiglitazone because of the possibly increased risk of cardiovascular problems other than congestive heart failure, which is already a black box warning. 9 In addition, a recent cohort study conducted in France reported that pioglitazone exposure was significantly associated with bladder cancer incidence, with a dose-effect relationship. 10
Meta-analyses have been published on DPP-4 inhibitors11–14; however, previous studies mainly summarized the efficacy and safety of sitagliptin and vildagliptin. Richter et al. detected substantial heterogeneity in treatment effect across trials, resulting in the removal of a Japanese-specific trial of vildagliptin as a sensitivity analysis. 12 A recent review suggested that existing meta-analyses were unreliable for the Japanese population because of a high degree of heterogeneity. 15 Since 2009, two more DPP-4 inhibitors have been approved by the FDA and more studies have emerged, including several that assessed the effects of saxagliptin and linagliptin. The present meta-analysis assesses the efficacy and safety of DPP-4 inhibitors, including sitagliptin, saxagliptin, vildagliptin and linagliptin, in patients with type 2 diabetes based on published and unpublished randomized controlled trials (RCTs) and describes the evidence for Japanese patients versus non-Japanese patients to evaluate the potential confounding effect of heterogeneity.
Methods
SEARCH STRATEGY AND INCLUSION CRITERIA
We conducted a search of MEDLINE for RCTs of DPP-4 inhibitors in type 2 diabetes through November 2011. An extensive search for sitagliptin, saxagliptin, vildagliptin, and linagliptin was performed. We also searched completed, but unpublished, trials at relevant web sites (www.clinicaltrials.gov, http://www.novctrd.com, http://ctr.bms.com, http://www.astrazenecaclinicaltrials.com, http://trials.boehringer-ingelheim.com, and http://www.clinicalstudyresults.org). We also searched reference lists from the articles to ensure completeness.
Our meta-analysis included all RCTs of DPP-4 inhibitors (sitagliptin, saxagliptin, vildagliptin, and linagliptin) for use in patients aged 18 years or older with type 2 diabetes that met the following criteria: (1) compared DPP-4 inhibitors with either placebo or oral hypoglycemic medications, (2) treated patients for at least 12 weeks, (3) had at least 1 baseline and posttreatment efficacy and/or safety outcome of interest, and (4) were published in the English language.
Trials with a shorter duration (<12 weeks) were excluded because of inadequate time to assess changes in glycemic efficacy, as hemoglobin A1c (A1C) reflects glycemia during the previous 3 months. 16 We also contacted authors to obtain any missing values needed to conduct the meta-analysis.
DATA EXTRACTION
The identification of relevant abstracts, the selection of studies based on the inclusion criteria described above, and the subsequent data abstraction from full-text articles were independently completed by 2 authors and compared for accuracy. Items abstracted pertained to study characteristics, patient characteristics, and outcome results. Any discrepancies were resolved by consensus between the 2 independent reviewers. The efficacy outcomes extracted included changes in A1C and changes in weight from baseline for DPP-4 inhibitors compared with placebo or other hypoglycemic agents. To evaluate the safety data, information about hypoglycemia, any adverse events, serious adverse events, and gastrointestinal (GI) adverse events was extracted. The quality of studies was assessed by 2 independent reviewers using 5 items of the scale proposed by Jadad et al. for published studies that evaluate randomization, double-blinding, and description of withdrawals. Possible scores range from 0 to 5 (a high score indicating high quality). 17
STATISTICAL ANALYSES
For efficacy measures, mean changes in A1C and body weight as continuous variables were assessed. For these continuous variables, weighted mean differences (WMDs) and 95% confidence intervals (CIs) for changes from baseline in DPP-4 inhibitors versus comparators were calculated. Standard deviations, together with the sample size, were used to compute the weight given to each study. For safety measures, the dichotomous variables (hypoglycemia and adverse events), were assessed using odds ratio (OR) with 95% CI for DPP-4 inhibitors versus comparators. The number of participants reporting hypoglycemia and other adverse events was examined. Small sample size corrections were made when event frequencies were less than 5; the correction added the value of 0.5 to all cells of the 2×2 contingency table of the study selected for correction before calculating the OR. 18 Heterogeneity was assessed by using the Q-statistic and I 2 tests among trials. Significance of the Q-statistic test (p < 0.05) indicates a substantial level of heterogeneity. 19 The I 2 statistic describes the percentage of the variability in effect estimates that is the result of heterogeneity rather than sampling error (chance), where I 2 values of 50% or more indicate a substantial level of heterogeneity. A random-effects model was used because statistical heterogeneity was present in some analyses. 20 For efficacy and safety outcomes, the currently recommended daily doses were included in all of the selected RCTs: sitagliptin 100 mg, vildagliptin 100 mg, saxagliptin 5 mg, and linagliptin 5 mg. 21
To assess the potential confounding effect of heterogeneity, subgroup analyses were performed, stratifying specific drugs or trial characteristics and data from specific population whenever possible. To estimate possible publication bias caused by the tendency of published studies to be positive, funnel plot and Egger regression were used, considering A1C as the main outcome variable. 22 All analyses were performed using Comprehensive Meta Analysis version 2.0, Biostat.
Results
STUDY AND PATIENT CHARACTERISTICS
A total of 1022 potentially relevant articles were identified. Based on a review of these abstracts, 196 were retrieved for detailed evaluation, and 62 studies met all of the inclusion criteria.23–84 Search results are summarized in Figure 1. Participant baseline characteristics of the included studies were extracted and are summarized in Table 1. Of the 62 trials, 53 appeared in peer-reviewed journals and 9 unpublished trials33,35,47,49,69,70,73,78,79 were available from websites. A total of 30,563 patients were included for analyses. However, the total number of participants randomized to all groups was different from the number of participants used in meta-analyses of glycemic efficacy (n = 28,218), weight change (n = 14,970), hypoglycemia (n = 28,887), and other adverse events (any adverse events, 30,223; serious adverse events, 30,245; and GI adverse events, 25,776) because of available trials of these meta-analyses. There were 50 trials in which a placebo was compared with a DPP-4 inhibitor given as monotherapy or as add-on therapy to other hypoglycemic agents. Seventeen trials directly compared a DPP-4 inhibitor with a hypoglycemic agent, including metformin, a thiazolidinedione, a sulfonylurea, or an α-glucosidase inhibitor. Five trials compared a DPP-4 inhibitor with both placebo and an active hypoglycemic (glipizide, rosiglitazone, and metformin) as monotherapy or add-on therapy to metformin. In addition, of 62 trials, 7 were conducted in Japan and measured the efficacy and safety of DPP-4 inhibitors only in Japanese patients; these were analyzed separately (n = 1605). Japanese patients were more likely to be older (mean age 59.1 years vs 55.4 years) and have a longer duration of type 2 diabetes mellitus (6.19 years vs 4.84 years), lower A1C baseline (7.70% vs 8.15%), and lower body mass index (BMI) (24.7 vs 30.8) compared to non-Japanese patients in the remaining 55 trials (n = 28,958).
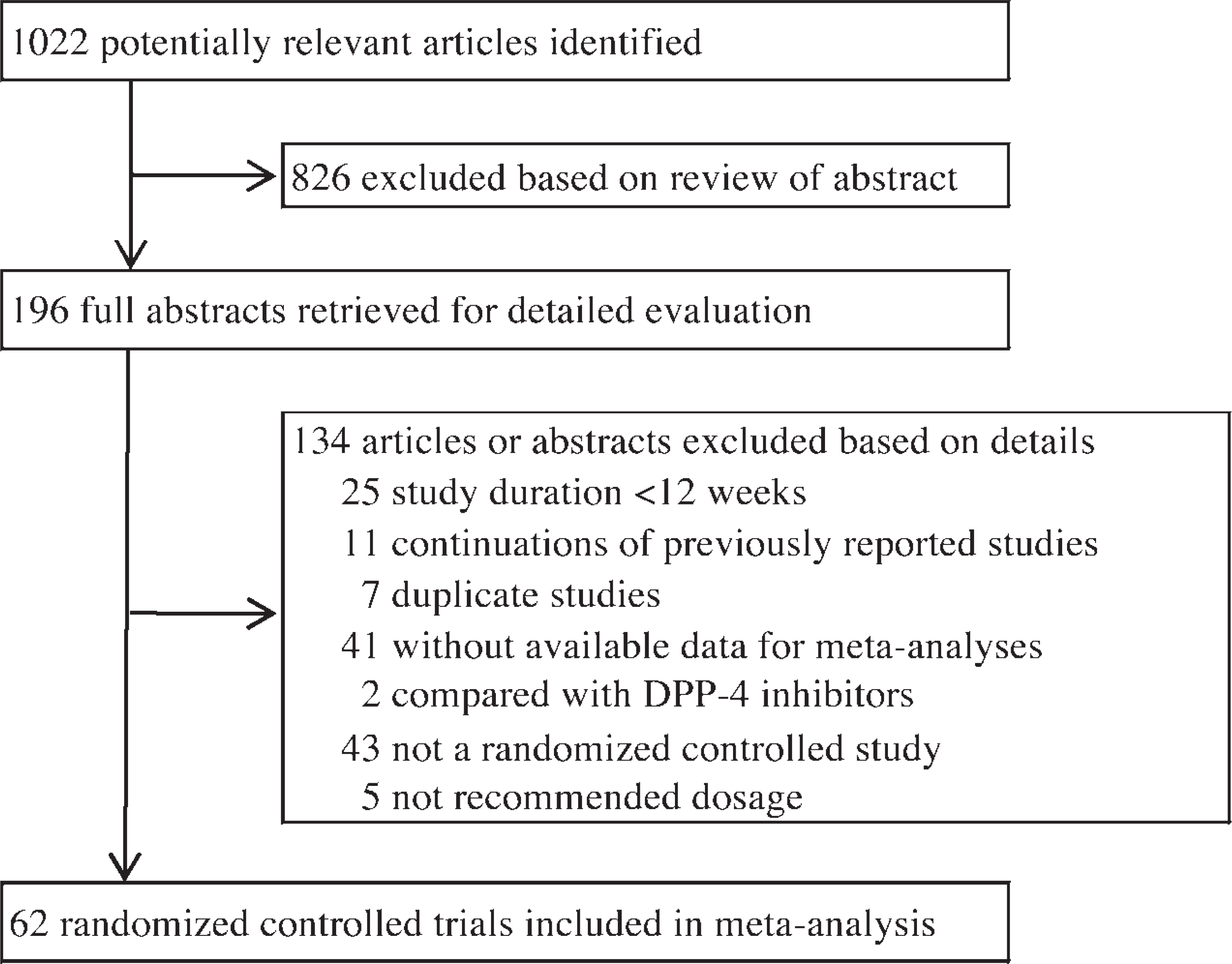
Study design. DPP-4 = dipeptidyl peptidase-4.
Characteristics of 62 Randomized Controlled Trials of Dipeptidyl Peptidase 4 Inhibitors
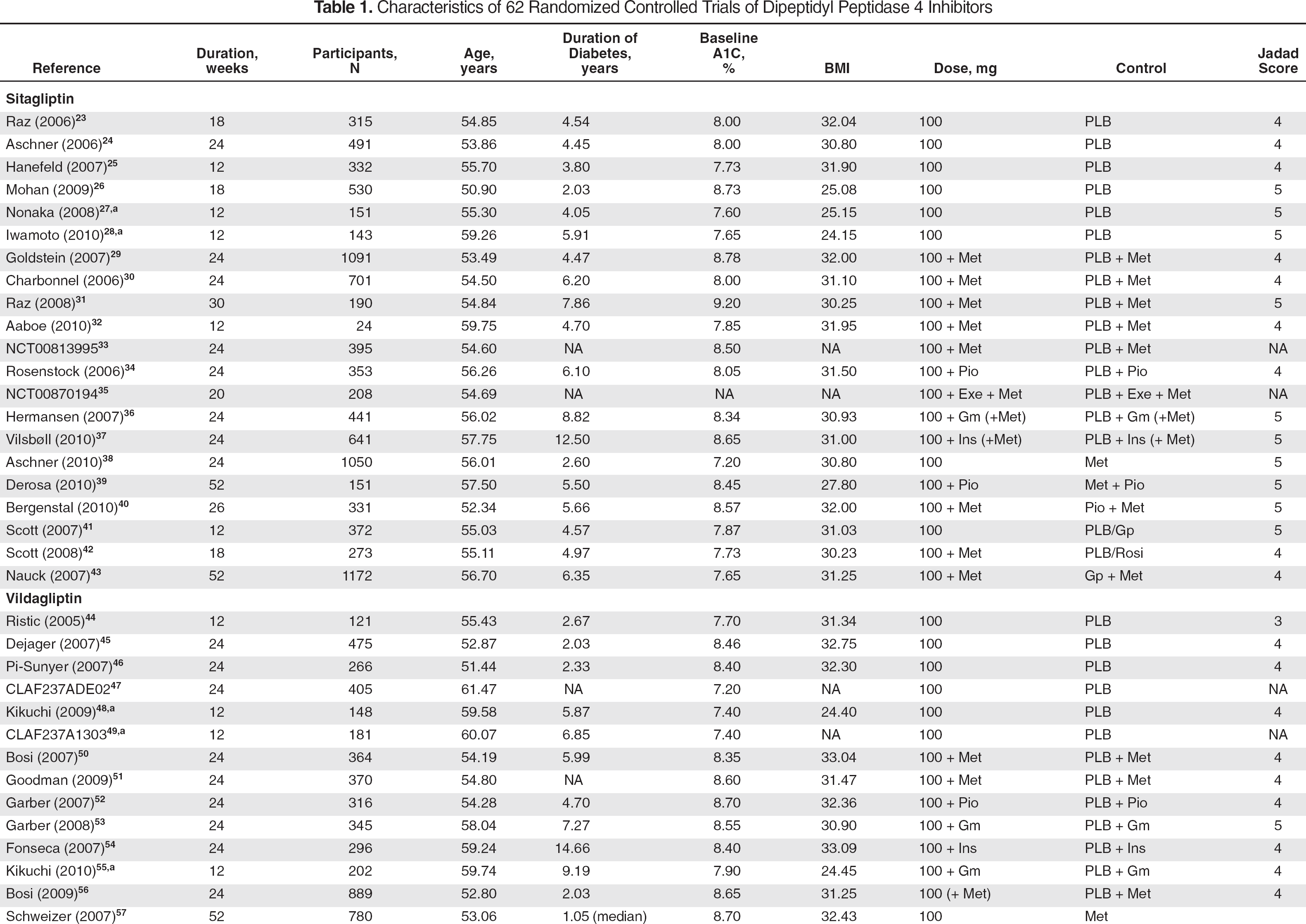
A1C = hemoglobin A
Japanese patient population.
EFFICACY
Hemoglobin A1c
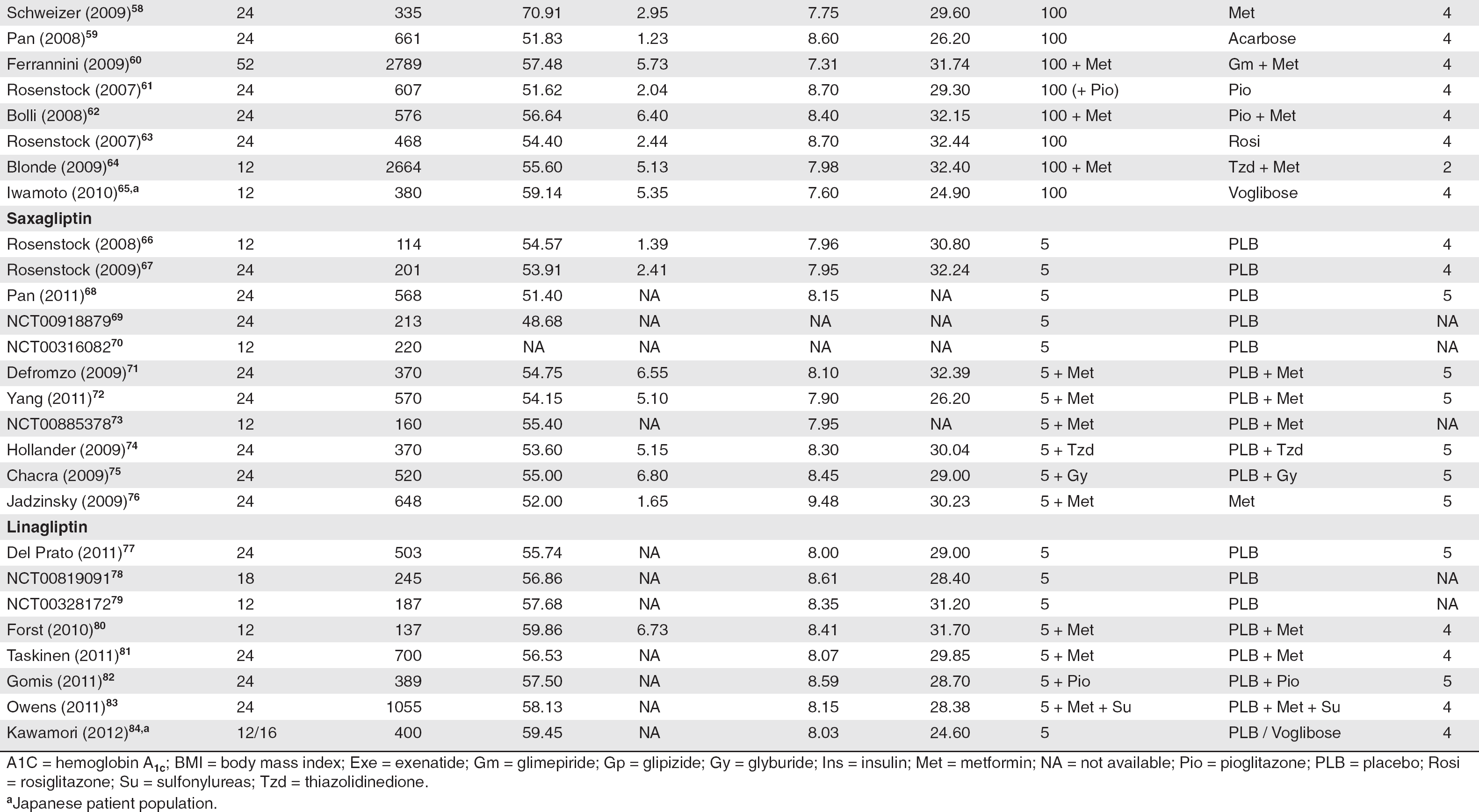
Figure 2 shows the effects of DPP-4 inhibitors on A1C decline from baseline compared with placebo and a hypoglycemic agent. Combining data from all studies comparing DPP-4 inhibitors with placebo showed that DPP-4 inhibitors lowered A1C significantly more than placebo (WMD −0.76%; 95% CI −0.83 to −0.68) did, but with a substantial amount of heterogeneity (I 2 = 82%). Exclusion of 7 trials investigating only Japanese patients (2 sitagliptin trials, 4 vildagliptin trials, and 1 linagliptin trial) resulted in a reduction of heterogeneity (I 2 = 59%) with a more stable pooled effect size of A1C reduction (WMD −0.65%; 95% CI −0.71 to −0.60) (Figure 3). Assessing data from the 7 Japanese-specific studies that compared DPP-4 inhibitors with placebo (n = 1119) showed a greater reduction in A1C than in non-Japanese patients in the remaining 55 trials (WMD −1.67%; 95% CI −1.89 to −1.44; p < 0.05).
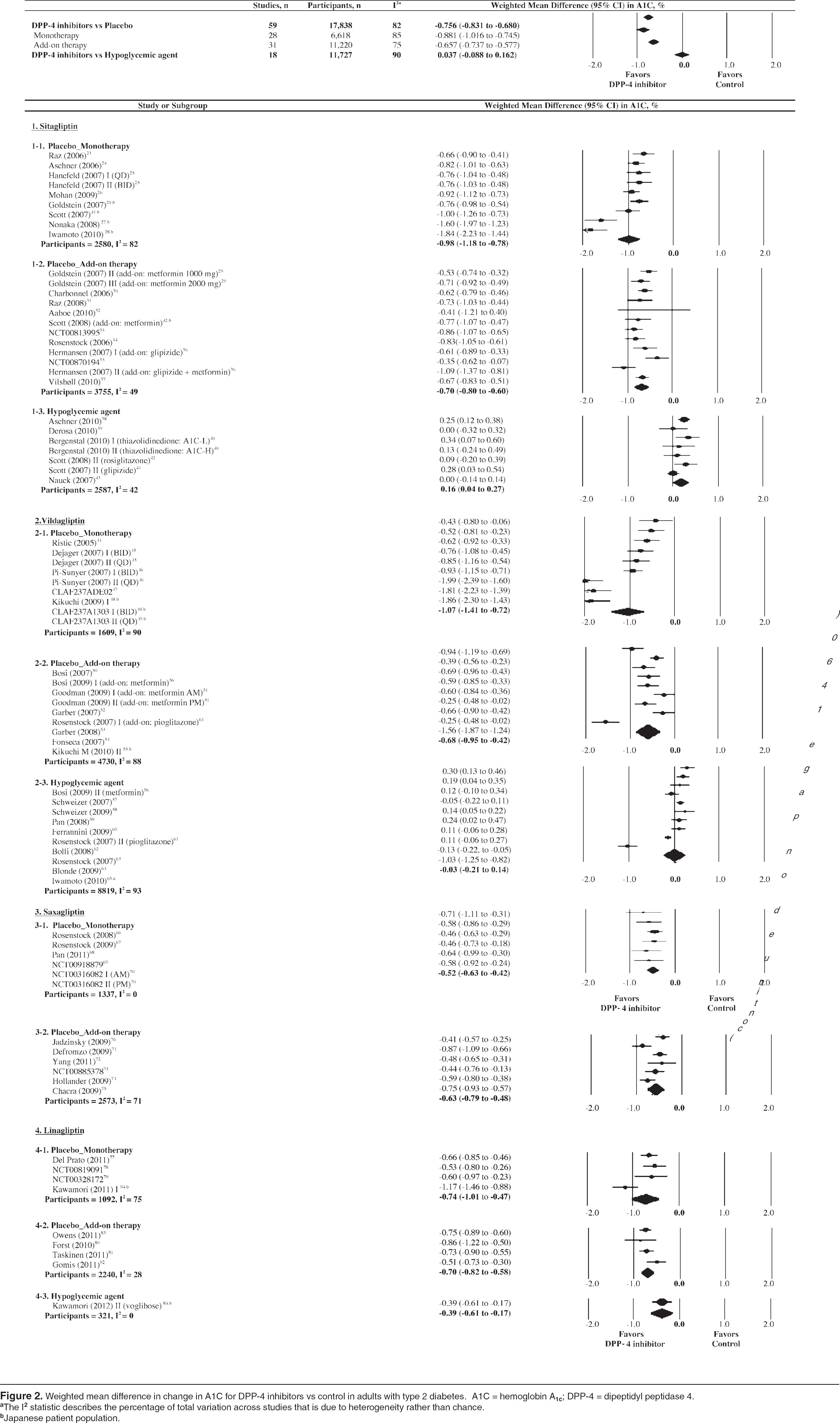
Weighted mean difference in change in A1C for DPP-4 inhibitors vs control in adults with type 2 diabetes. A1C = hemoglobin A1c; DPP-4 = dipeptidyl peptidase 4.
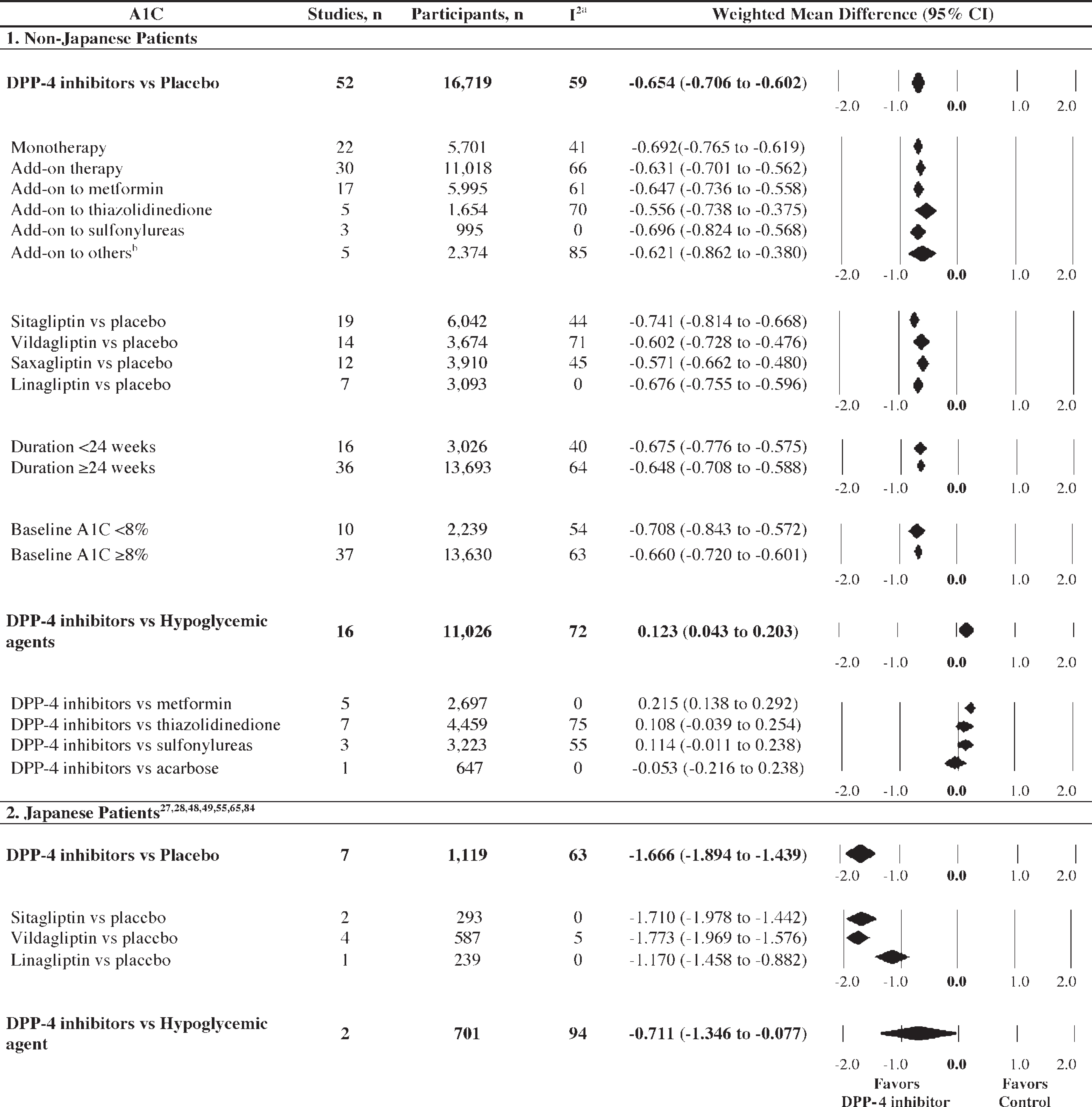
Subgroup analyses of weighted mean difference in change in A1C for DPP-4 inhibitors vs controls. A1C = hemoglobin A1c; DPP-4 = dipeptidyl peptidase 4.
For the 55 non-Japanese RCTs, there were no significant differences in reductions of A1C in comparison with a placebo between monotherapy and add-on therapy (WMD −0.69%; 95% CI −0.77 to −0.62 vs WMD = −0.63%; 95% CI −0.70 to −0.56). Lowering of the A1C compared to placebo was found for each of the 4 available DPP-4 inhibitors: sitagliptin (WMD −0.74%; 95% CI −0.81 to −0.67), vildagliptin (WMD −0.60%; 95% CI −0.73 to −0.48), saxagliptin (WMD −0.57%; 95% CI −0.66 to −0.48), and linagliptin (WMD −0.68%; 95% CI −0.76 to −0.60). For placebo-controlled trials, the extent of A1C reduction was similar in patients with baseline A1C less than 8% and A1C 8% or more and for patients in trials of shorter (<24 weeks) compared to longer (≥24 weeks) duration.
In 17 active comparator RCTs, DPP-4 inhibitors showed similar A1C reduction compared to other hypoglycemic agents combined (WMD 0.04%; 95% CI −0.09 to 0.16), but heterogeneity was substantial (I 2 = 90%) (Figure 2). As noted in Figure 3, however, with combined data from non-Japanese studies (n = 16; I 2 = 72%), DPP-4 inhibitors were slightly less effective compared to other hypoglycemic agents (WMD 0.12%; 95% CI 0.04 to 0.20), whereas 2 Japanese studies (I 2 = 94%) were associated with a greater decline in A1C compared with voglibose (WMD −0.71%; 95% CI −1.35 to −0.08). In the individual comparator trials for non-Japanese studies, noninferiority was established when DPP-4 inhibitors were compared with thiazolidinediones, sulfonylureas, and acarbose, but noninferiority was not shown when DPP-4 inhibitors were compared with metformin (WMD 0.22%; 95% CI 0.14 to 0.29).
Weight
In the 35 RCTs that reported data on changes in weight, DPP-4 inhibitors showed a small weight gain compared with placebo (n = 32; WMD 0.21 kg; 95% CI 0.15 to 0.27), but the increase was not significantly different from that with other hypoglycemic agents (n = 10; WMD −0.04 kg; 95% CI −0.36 to 0.29) (Figure 4). In the individual comparator trials, there was no significant difference in weight gain in placebo-controlled trials among drugs: sitagliptin (WMD 0.22 kg; 95% CI 0.11 to 0.32), vildagliptin (WMD 0.26 kg; 95% CI 0.14 to 0.38), saxagliptin (WMD 0.14 kg; 95% CI 0.00 to 0.27) and linagliptin (WMD 0.15 kg; 95% CI 0.03 to 0.27). A subgroup analysis for 6 Japanese-specific trials (n = 917) with placebo found that Japanese patients gained more weight (WMD 0.37 kg; 95% CI 0.21 to 0.53) than non-Japanese patients (WMD 0.18 kg; 95% CI 0.12 to 0.25), but this difference was not statistically significant (p > 0.05).
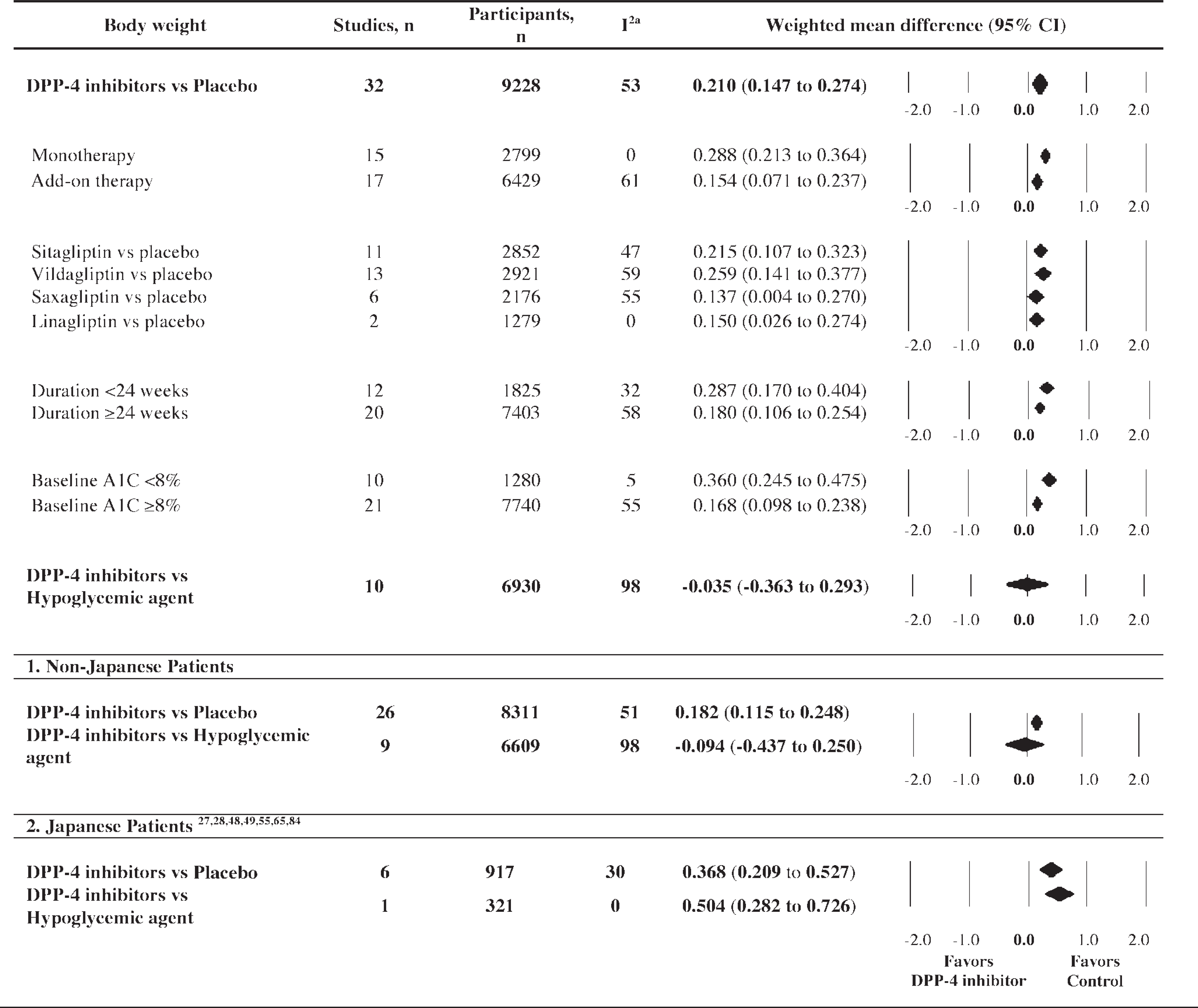
Weighted mean difference of change in body weight for DPP-4 inhibitors vs control in adults with type 2 diabetes. A1C = hemoglobin A1c; DPP-4 = dipeptidyl peptidase 4.
SAFETY
Hypoglycemia
Data on hypoglycemic episodes were retrieved in 56 of 62 trials (n = 28,887). DPP-4 inhibitors showed an increased risk of hypoglycemia (OR 1.32; 95% CI 1.04 to 1.67) compared with placebo. Although the incidence of hypoglycemia with monotherapy was not significantly different from that observed with a placebo (OR 1.04; 95% CI 0.68 to 1.58), DPP-4 inhibitor therapy combined with other hypoglycemic agents showed an incidence of hypoglycemia that was slightly higher than that of placebo (OR 1.40; 95% CI 1.00 to 1.96) (Figure 5).
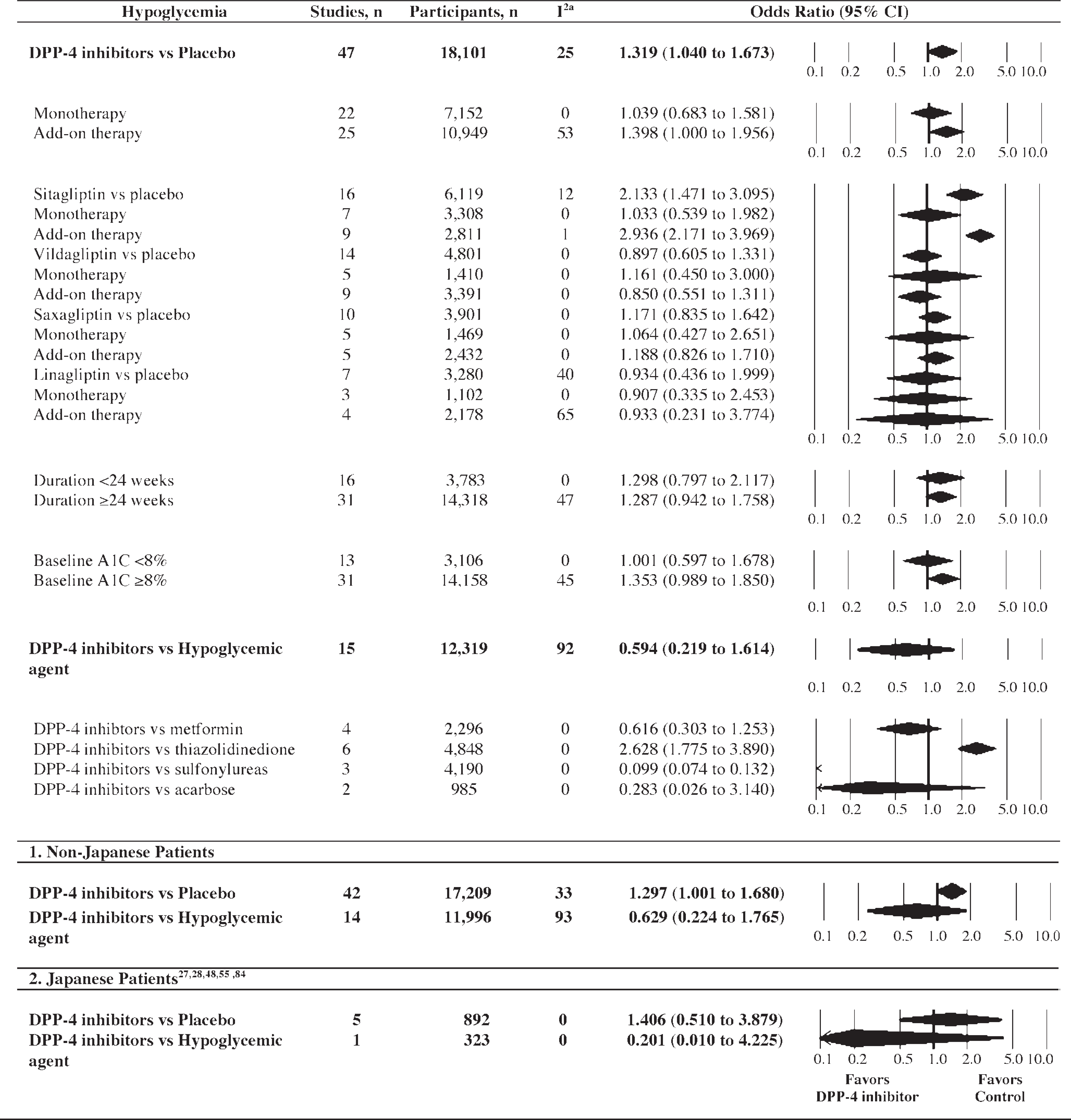
Odds ratio (95% CI) for hypoglycemia for DPP-4 inhibitors vs control in adults with type 2 diabetes. DPP-4 = dipeptidyl peptidase 4.
In the individual trials, sitagliptin combined with other hypoglycemic agents (metformin, glimepiride, pioglitazone, or insulin) was associated with a higher risk of hypoglycemia compared with placebo (OR 2.94; 95% CI 2.17 to 3.97), whereas no increased risk was observed for other DPP-4 inhibitors: vildagliptin (OR 0.85; 95% CI 0.55 to 1.31), saxagliptin (OR 1.19; 95% CI 0.83 to 1.71), and linagliptin (OR 0.93; 95% CI 0.23 to 3.77). Subgroup analysis involving non-Japanese patients reported a slightly higher risk of hypoglycemia compared with placebo (OR 1.30; 95% CI 1.00 to 1.68), whereas no significant difference in hypoglycemia was observed for Japanese patients (OR 1.41; 95% CI 0.51 to 3.88).
The risk of experiencing hypoglycemia with DPP-4 inhibitors was not significantly different compared to the risk with other hypoglycemic agents (including metformin, thiazolidinediones, sulfonylureas, and α-glucosidase inhibitors) (OR 0.60; 95% CI 0.22 to 1.61). More specifically, DPP-4 inhibitors were associated with a significantly lower hypoglycemic risk than were sulfonylureas (OR 0.10; 95% CI 0.07 to 0.13) but a significantly higher risk than with thiazolidinediones (OR 2.63; 95% CI 1.78 to 3.89). Comparing acarbose use and metformin use, there were no significant differences in the odds of hypoglycemic episodes (OR 0.28; 95% CI 0.03 to 3.14 and OR 0.62; 95% CI 0.30 to 1.25, respectively).
Other Adverse Events
Similar adverse events were observed with Japanese and non-Japanese patients (Table 2). Overall, there was a similar probability of any adverse event detected with DPP-4 inhibitors compared to placebo (OR 1.00; 95% CI 0.90 to 1.10); however, DPP-4 inhibitors had a lower risk of any adverse events compared to other hypoglycemic agents (OR 0.86; 95% CI 0.74 to 0.99). A similar result was seen with serious adverse events. Reported serious adverse events included cardiovascular events, edema, pancreatitis, and cholelithiasis in both the DPP-4 inhibitor group and the control group. DPP-4 inhibitors showed a similar incidence of serious adverse events in comparison with placebo (OR 1.04; 95% CI 0.88 to 1.24) but a decreased risk compared with other hypoglycemic agents (OR 0.78; 95% CI 0.65 to 0.93).
Summary of Adverse Events for DPP-4 Inhibitors vs Control in Adults with Type 2 Diabetes
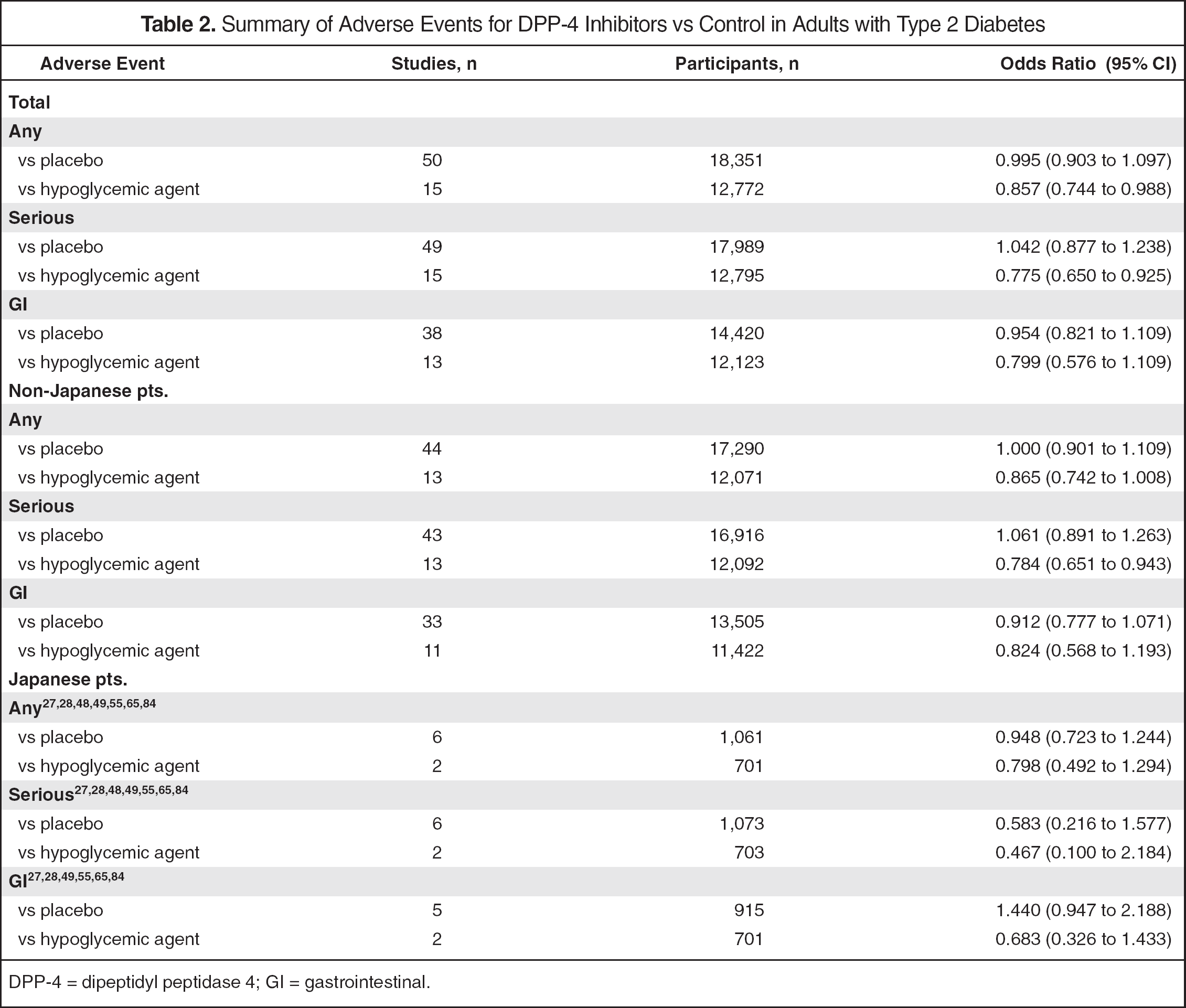
DPP-4 = dipeptidyl peptidase 4; GI = gastrointestinal.
Treatment with DPP-4 inhibitors was not associated with any increase in the overall risk of GI events (nausea, vomiting, diarrhea, and abdominal pain) in comparison with placebo (OR 0.95; 95% CI 0.82 to 1.11) or with other hypoglycemic agents (OR 0.80; 95% CI 0.58 to 1.11).
The 53 published RCTs were of generally high methodologic quality as measured by the Jadad score, with 4 being the median (range 2–5). Fifty-one studies were classified as high quality (Jadad score of 4 or 5), and only 2 studies were classified as low quality (Jadad score of 2 or 3)44,64; therefore, comparisons were not made on the basis of quality assessment scores.
Considering A1C as the main outcome variable, Egger regression revealed publication bias for placebo (p < 0.01), although no evidence was found with active comparator-controlled trials (p = 0.98). However, analysis of the 55 non-Japanese trials did not suggest any evidence of publication bias (p = 0.61).
Discussion
DPP-4 inhibitors are a relatively new therapeutic class of oral antihyperglycemic drugs for the management of type 2 diabetes. Although the ADA-EASD consensus algorithm does not recommend DPP-4 inhibitors as first- or second-line therapy because of the limited clinical data supporting their efficacy and safety and/or relative expense, except for selected cases, 6 several studies included in this meta-analysis have become available since the ADA-EASD consensus. Efficacy and safety need to be assessed through an up-to-date comprehensive review of presently available clinical trials.
This meta-analysis included a comprehensive search for all currently approved DPP-4 inhibitors, including vildagliptin, sitagliptin, saxagliptin, and linagliptin, for type 2 diabetes treatment. The addition of 21 studies since the most recently published meta-analysis 13 allowed separate analyses by specific drugs, study design, and patient characteristics, which may add valuable information concerning the use of DPP-4 inhibitors for patients with type 2 diabetes.
To our knowledge, this is the first meta-analysis that separately assessed efficacy and safety of DPP-4 inhibitors for Japanese and non-Japanese patients. A key reason for this separation of Japanese patients is their contribution to high heterogeneity; some of the results were significantly different between non-Japanese and Japanese patients.
Our analyses indicated that the magnitude of A1C decline with DPP-4 inhibitors versus placebo decreased from 0.76% to 0.66% when the 7 Japanese-specific trials were excluded. More available Japanese-specific studies resulted in a higher decrease in A1C than was shown in previous meta-analyses, in which A1C reduction ranged between 0.70%12,13 and 0.74%. 11 Notably, the extent of A1C reduction was more than doubled in Japanese-specific trials compared to non-Japanese trials (WMD −1.67 % vs −0.66%, p < 0.05) with no increased risk of hypoglycemia (OR 1.41; 95% CI 0.51 to 3.88 vs OR 1.30; 95% CI 1.00 to 1.68).
Overall, monotherapy with DPP-4 inhibitors produced a similar placebo-subtracted reduction of A1C compared to add-on therapy including metformin, sulfonylureas, pioglitazone, and insulin with no difference in the risk of experiencing hypoglycemia. No additional effect on A1C was found when used as an add-on to other agents. The findings from our analyses were consistent with those of Monami et al., who reported a similar efficacy of sitagliptin and vildagliptin in monotherapy and in combination with other agents. 13
The effect of DPP-4 inhibitors on A1C in comparison to other hypoglycemic agents indicated high heterogeneity and mixed results. The I 2 was still high after separating out Japanese-specific studies (I 2 = 72% for non-Japanese RCTs vs 94% for Japanese RCTs). In the 15 active comparator trials on non-Japanese patients, DPP-4 inhibitors were less efficacious in A1C reduction compared to other hypoglycemic agents (WMD 0.12%; 95% CI 0.04 to 0.20), with a nonsignificant difference in the risk of hypoglycemia (OR 0.63; 95% CI 0.22 to 1.77). Amori et al. found that sitagliptin and vildagliptin were less effective in reducing A1C compared to other hypoglycemic agents (WMD 0.21%; 95% CI 0.02 to 0.39), 11 which was consistent with our results including sitagliptin, vildagliptin, saxagliptin, and linagliptin in non-Japanese patients. However, combining data from all 17 studies comparing DPP-4 inhibitors with other hypoglycemic agents showed a nonsignificant difference in A1C reduction (WMD 0.04%; 95% CI −0.09 to 0.16) or risk of hypoglycemia (OR 0.60; 95% CI 0.22 to 1.61). Separate analyses were performed for 2 Japanese-specific trials, but interpretability is limited because only 2 trials for A1C and 1 trial for hypoglycemia were available. Interestingly, a slightly higher weight gain was seen in Japanese patients for DPP-4 inhibitors compared to placebo than in non-Japanese patients, although the difference was not statistically significant (0.37 vs 0.18 kg; p > 0.05).
The mechanism underlying these phenomena needs to be further elucidated. Differences in the characteristics between Japanese patients and non-Japanese patients could provide some explanation for the discrepancies in the results of clinical trials. Japanese patients were more likely to be older (mean age 59.1 vs 55.4 years) and have longer duration of type 2 diabetes mellitus (6.19 vs 4.84 years) with lower A1C baseline (7.7% vs 8.15%) and lower BMI (24.7 vs 30.8) compared with non-Japanese patients. However, the most recently published review of DPP-4 inhibitors reported that age, BMI, and race did not appear to significantly alter the pharmacokinetics of sitagliptin, vildagliptin, and saxagliptin. 85 Interestingly, a 12-week placebo-controlled study involving Japanese patients showed that oral sitagliptin 50 mg (change from baseline, −0.71%) was maximally effective at reducing A1C, with similar magnitude reductions observed in the 100-mg group (change from baseline, −0.69%). 28 There also may be pharmacogenetic or cultural lifestyle differences that may contribute to the larger reduction in A1C in Japanese patients.
The ADA guidelines emphasize prevention of hypoglycemia as critical to the treatment strategy in type 2 diabetes. 86 A low risk of hypoglycemia offers an advantage over other therapies, as concern for hypoglycemia is a major obstacle to medication adherence. 87 Our meta-analysis indicated similar rates of hypoglycemia between DPP-4 inhibitors and other hypoglycemic agents, although they had an increased risk of hypoglycemia compared with placebo. Subgroup analysis involving non-Japanese patients reported a slightly higher risk of hypoglycemia compared with placebo (OR 1.30; 95% CI 1.00 to 1.68), whereas no significant difference in hypoglycemia was observed for Japanese patients (OR 1.41; 95% CI 0.51 to 3.88).
This study has several limitations. Despite the addition of more RCTs, statistical heterogeneity was detected. This heterogeneity may have been the result of differences in design, patient characteristics, duration of diabetes, and control drug therapy. On the other hand, the separation of some recently available (published and unpublished) Japanese-specific studies reduced the impact of heterogeneity across studies, which consequently increased statistical power. Despite some strength in retrieving all available studies, it was possible that including 2 low-quality studies and 9 unpublished studies may contribute statistical heterogeneity. The possibility also exists that this analysis was influenced by publication bias, although no publication bias was detected with non-Japanese trials. Of 62 included studies, 57 were shorter than 30 weeks, so long-term efficacy and safety are still questionable. Long-term safety is a particular concern noted by the ADA-EASD. There have been some postmarketing cases of acute pancreatitis, acute renal failure, and serious allergic and hypersensitivity reactions in patients taking sitagliptin. 21 In addition, vildagliptin carries a warning to monitor liver function if transaminase levels are elevated. 3 The need for long-term data on cardiovascular outcomes is especially important given the concerns with thiazolidinediones, but these trials did not assess cardiovascular surrogates or end points, except for some trials examining the effects of treatment on lipids and blood pressure. Furthermore, this analysis was not performed at the patient level but rather presented summary data; therefore, accurate assessment of combining studies on Japanese patients may be lacking. Due to the relatively small number of Japanese-specific studies in this meta-analysis, the clinical interpretation of the results for Japanese patients may be limited. Future studies should include RCTs of DPP-4 inhibitors for use in Japanese patients with type 2 diabetes that are published both in the English and Japanese languages.
In conclusion, the results of this meta-analysis suggest that DPP-4 inhibitors in patients with type 2 diabetes mellitus were moderately effective in improving glycemia, but did not show a favorable effect on weight compared with placebo. For Japanese patients, the reduction of A1C was twice that of non-Japanese patients compared to placebo, without any increased risk of hypoglycemia. In the comparator trial from all available studies, DPP-4 inhibitors were associated with similar A1C reduction or risk of hypoglycemia compared to other hypoglycemic agents. Furthermore, DPP-4 inhibitors exhibit a significantly decreased risk of any adverse events and serious adverse events compared with other hypoglycemic agents. However, this new class of hypoglycemic agents needs continued evaluation in long-term efficacy and safety controlled trials for non-Japanese and Japanese populations.