
Abstract
BACKGROUND:
Metformin can result in vitamin B12 deficiency, potentially leading to complications such as neuropathy. Annual monitoring of vitamin B12 has been suggested; however, it is unknown whether current practice reflects this recommendation.
OBJECTIVE:
To identify vitamin B12 monitoring patterns in patients on long-term, high-dose metformin. Secondary objective was to determine the frequency of new vitamin B12 deficiency, anemia, and neuropathy documented after initiation of high-dose metformin.
METHODS:
Electronic medical records of veterans treated at the Veterans Affairs Maryland Healthcare System with high-dose metformin (≥2000 mg/day) as of November 1, 2010, were reviewed. Data regarding metformin treatment, vitamin B12 measurements, and documentation of vitamin B12 deficiency, cyanocobalamin supplementation, anemia, and neuropathy were collected. Subjects treated with metformin for less than 1 year or those with documented peripheral neuropathy, megaloblastic anemia, vitamin B12 deficiency, or a condition associated with vitamin B12 malabsorption prior to metformin initiation were excluded.
RESULTS:
Subjects (N = 235) had a mean metformin dose of 2050 mg/day and mean duration of treatment of 5.2 years. Sixty percent did not have vitamin B12 measured. Of subjects receiving metformin for 10 years or more, nearly half (46%) never had vitamin B12 measured. New documentation of vitamin B12 deficiency or cyanocobalamin supplementation was found in 5.5% of the population, and anemia was found in 12%. Of the 14% with new neuropathy, 42% did not have vitamin B12 measured.
CONCLUSIONS:
Vitamin B12 was not routinely monitored in patients on high-dose metformin, even in those at highest risk (≥10 years of therapy), or in those with potential manifestations of vitamin B12 deficiency (neuropathy). Cases of vitamin B12 deficiency and resulting anemia or neuropathy may be undiagnosed and untreated because of lack of monitoring. Prospective studies examining the effect of increased vitamin B12 monitoring on identification and treatment of vitamin B12 deficiency in patients on metformin are warranted.
Metformin, a first-line agent for the treatment of type 2 diabetes mellitus, has been shown to cause vitamin B12 malabsorption and deficiency.1,2 Serum vitamin B12 levels have been shown to be inversely correlated with dose and duration of metformin therapy, and this decrease in vitamin B12 level has been shown to persist and worsen.1,3 This effect may be due to impairment of the calcium-dependent ileal absorption of the intrinsic factor-vitamin B12 complex by metformin.3,4 Studies suggest that 10–30% of patients on long-term metformin therapy experience vitamin B12 malabsorption, while 6–9% of patients develop a vitamin B12 deficiency.5–7 High-dose (2000–2550 mg/day) and long-term (3 or more years) metformin therapy are the greatest risk factors for metformin-induced vitamin B12 deficiency. 3 For those on metformin therapy, the related vitamin B12 deficiency can take up to 10–15 years to develop.8,9 Because metformin has been on the American market for over 15 years, the prevalence of metformin-induced vitamin B12 deficiency may increase significantly. 9
To detect a vitamin B12 deficiency, serum vitamin B12 levels are usually obtained. However, the use of serum vitamin B12 levels alone to diagnose a vitamin B12 deficiency may not be as accurate as the use of other biomarkers and may lead to missed diagnoses.10,11 For patients with a subclinical vitamin B12 deficiency, obtaining a methylmalonic acid and/or homocysteine level can help determine whether a patient has a clinically significant vitamin B12 deficiency. If either or both parameters are elevated, the patient can be considered to have a clinically significant vitamin B12 deficiency and is a candidate for cyanocobalamin supplementation.11,12
It is important to thoroughly monitor for vitamin B12 deficiency in patients on metformin, as the effects of such a deficiency can be clinically significant in the diabetic population. Vitamin B12 deficiency can lead to altered mental status, megaloblastic anemia, and neurologic damage that often first presents as peripheral neuropathy.1,9,13 In diabetic patients treated with metformin, peripheral neuropathy as a result of an induced vitamin B12 deficiency may be mistaken for diabetic neuropathy. 9 The progression of neurologic damage due to vitamin B12 deficiency can be halted by oral or parenteral cobalamin supplementation. 14 However, if the vitamin B12–mediated neuropathy is misdiagnosed as diabetic neuropathy and the vitamin deficiency goes untreated, permanent neurologic damage can occur.13,15
Routine monitoring of vitamin B12 in diabetic patients on long-term metformin therapy allows for detection and correction of low serum concentrations, preventing unnecessary hematologic and neurologic complications. Annual monitoring of hematologic parameters, including serum vitamin B12 concentrations, has been suggested for patients on metformin.5–7,9 However, it is unknown how vigilantly markers of vitamin B12 deficiency are being monitored in this patient population. The purpose of this study was to evaluate monitoring of vitamin B12 levels in metformin-treated patients at the Veterans Affairs Maryland Healthcare System (VAMHCS), a multifacility network of medical centers and clinics with a total of 754 beds and 7 outpatient clinics that serves over 50,000 veterans in Maryland. The primary objective of this study was to identify serum vitamin B12 monitoring patterns in patients on long-term, high-dose metformin therapy. The secondary objective was to determine the frequency of complications associated with metformin-induced vitamin B12 malabsorption, specifically clinical or subclinical vitamin B12 deficiency, anemia, and neuropathy newly documented after initiation of high-dose metformin.
Methods
The University of Maryland School of Medicine Institutional Review Board and the VAMHCS Research and Development Committee approved this study. Eligible patients had a diagnosis of type 2 diabetes mellitus and an active prescription for high-dose metformin as of November 1, 2010. Patients were excluded if they had been receiving high-dose metformin for less than 1 year; had documented vitamin B12 deficiency, megaloblastic anemia, or peripheral neuropathy prior to high-dose metformin initiation; or had a history of pernicious anemia, atrophic gastritis, gastrointestinal surgery (ileal resection, partial or complete gastrectomy, or gastric banding or bypass), celiac sprue, Crohn disease, alcoholism, chronic pancreatitis, malabsorption syndrome, HIV infection, or Helicobacter pylori infection documented in the problem list of their electronic medical record due to the vitamin B12 malabsorption associated with these conditions. For this study, high-dose metformin was defined as a dose of at least 2000 mg/day. Long-term metformin therapy was defined as treatment with high-dose metformin for at least 1 year.
Data were collected from electronic medical records for each year of high-dose metformin treatment, from the end of year 1 of therapy to the end of the study period. Year 1 was defined as the year in which the subject was first prescribed high-dose metformin. End of study was defined as November 1, 2010. For each subject, the following data were collected: age; metformin dose; duration of high-dose metformin treatment; whether there was a new prescription for cyanocobalamin during the study period; new documentation of anemia, neuropathy, or vitamin B12 deficiency during the study period; serum vitamin B12 level; hemoglobin level; mean corpuscular volume; and serum methylmalonic acid (MMA) level. For subjects with multiple laboratory values in a single year, the highest metformin dose and MMA values and the lowest serum vitamin B12 and hemoglobin values were recorded. Descriptive statistics were compiled for patient demographics, vitamin B12 monitoring patterns, and frequency of vitamin B12 deficiency, anemia, and neuropathy.
Results
Eight hundred sixty-nine patients were identified as having an active prescription for high-dose metformin as of November 1, 2010. Charts of 300 randomized patients were reviewed for eligibility. 16 Sixty-five individuals were ineligible for the study, with the majority excluded because of peripheral neuropathy at baseline, alcohol abuse, or duration of metformin therapy of less than 1 year. Demographics of the 235 included subjects are listed in Table 1.
Demographics
VITAMIN B12 MONITORING
Vitamin B12 monitoring patterns, stratified by duration of metformin therapy, are illustrated in Figure 1. Among all subjects included in the study, 60% did not have a serum vitamin B12 level measured during high-dose metformin treatment. In addition, among subjects who had been on high-dose metformin for the longest time (at least 10 years) and were therefore at greatest risk of vitamin B12 deficiency, nearly half (46%) had never had a vitamin B12 level measured. Less than 1% of subjects had a serum vitamin B12 measured yearly. Among the 62 study subjects with a serum vitamin B12 measurement of less than 350 pg/mL (reference range 157–1059), 77% did not have a follow-up MMA level measured.
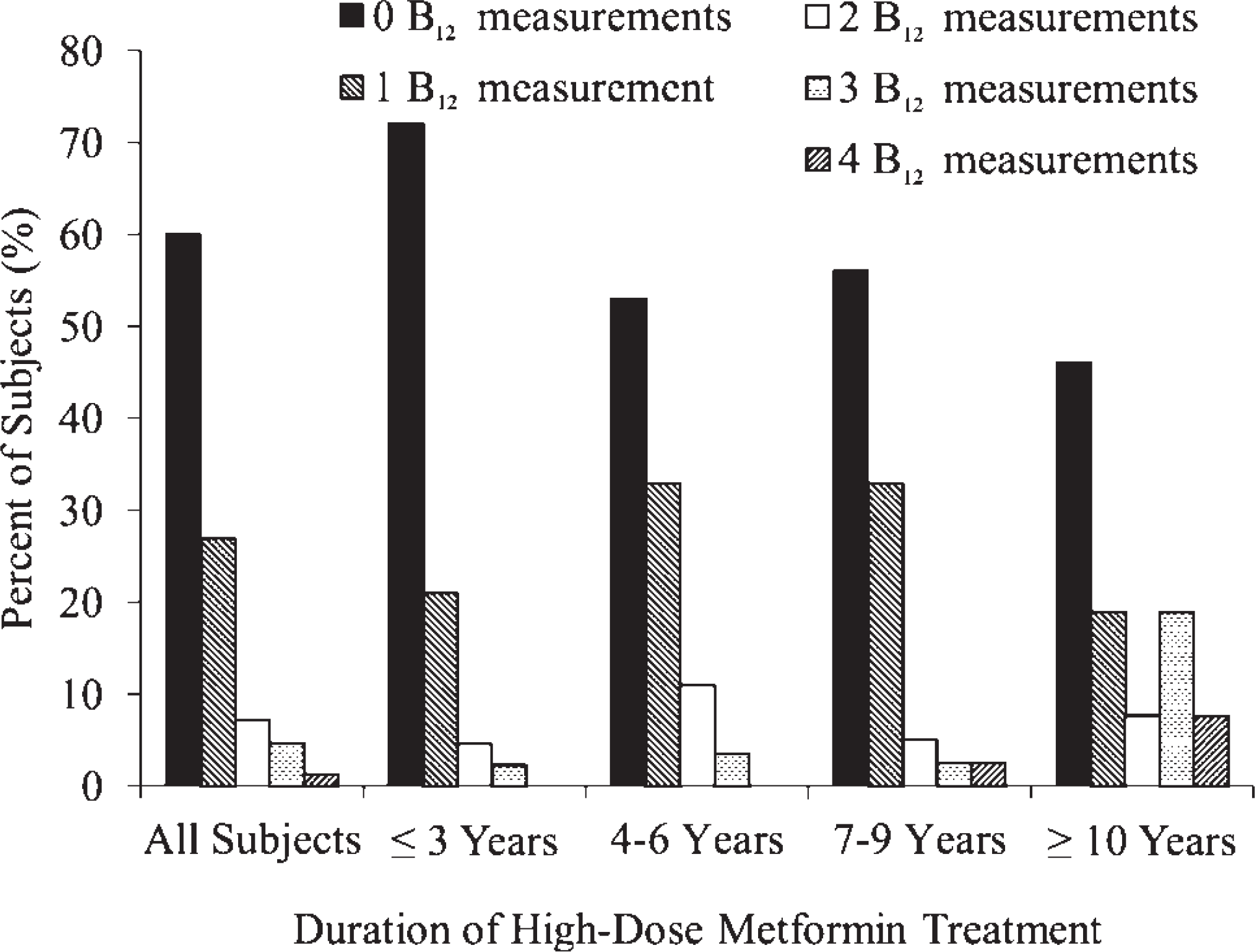
Total number of serum vitamin B12 measurements per subject by duration of high-dose (≥2000 mg/day) metformin therapy.
INCIDENCE OF VITAMIN B12 DEFICIENCY, ANEMIA, AND NEUROPATHY
Six (2.5%) subjects had a new vitamin B12 deficiency documented after a mean of 4.5 years of high-dose metformin therapy. However, 13 subjects (5.5%) had a new prescription for cyanocobalamin supplementation during the study period (Figure 2). Forty-eight (18%) patients did not have a new cyanocobalamin prescription or an MMA level measured despite having a serum vitamin B12 level less than 350 pg/mL while on metformin. New documentation of anemia and neuropathy was noted in 28 (12%) and 33 (14%) subjects, respectively. Among these subjects, 29% of those with newly documented anemia and 42% of those with newly documented neuropathy had no documentation of serum vitamin B12 measurement (Figure 3).
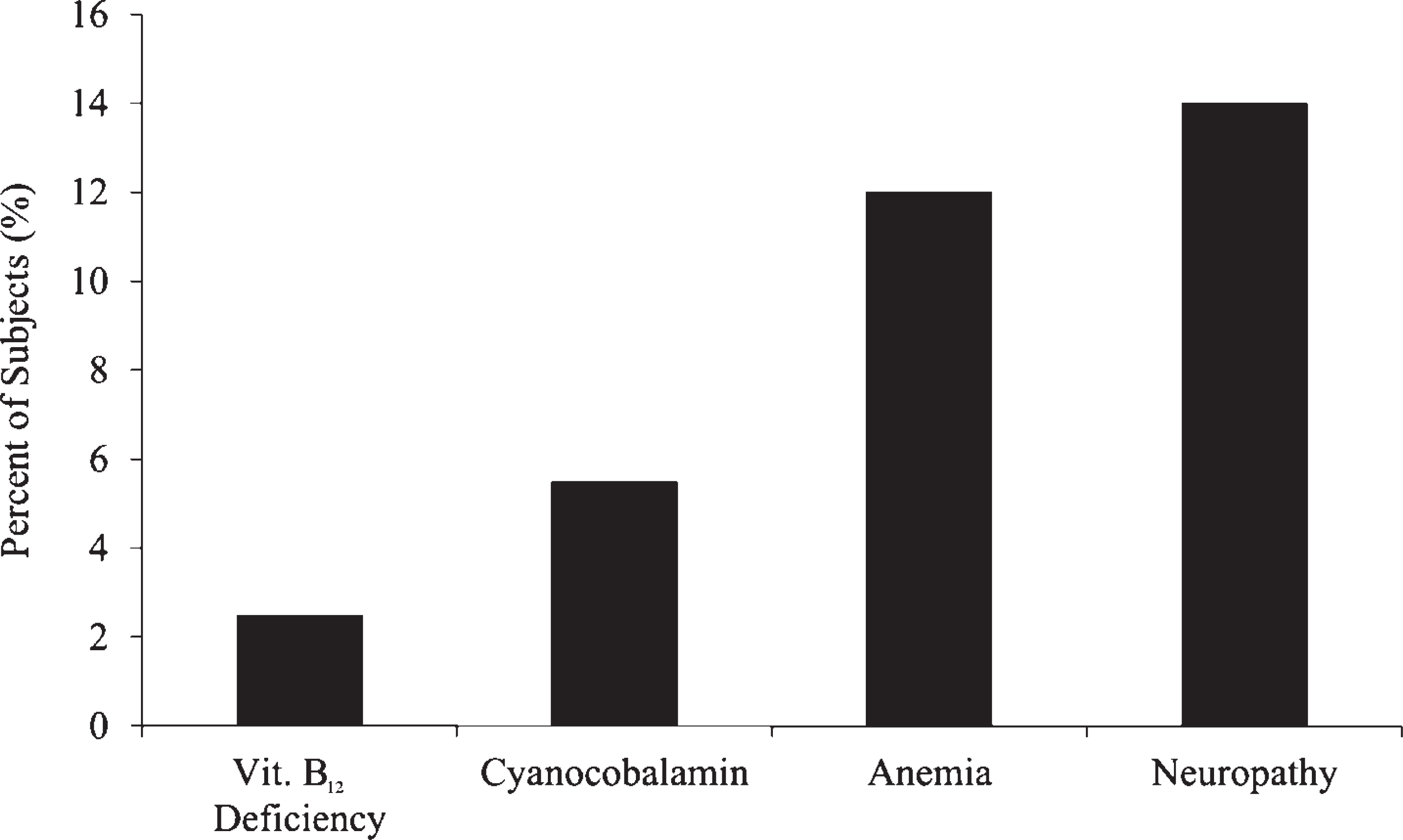
Incidence of new documentation of vitamin B12 deficiency (n = 6), cyanocobalamin use (n = 13), anemia (n = 28), and neuropathy (n = 33) among included subjects (N = 235) during high-dose metformin therapy.
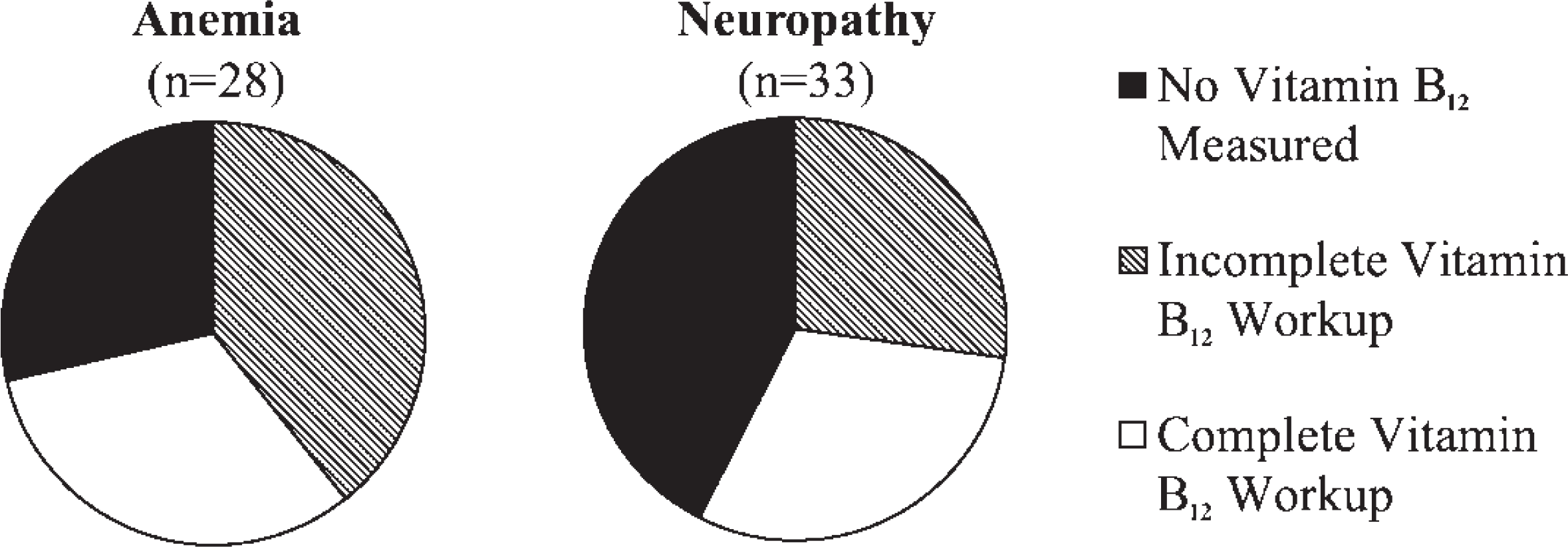
Vitamin B12 monitoring in subjects with anemia or neuropathy. Proportion of subjects with new documentation of anemia (n = 28) or neuropathy (n = 33) who did not have vitamin B12 levels measured at any time and who received an incomplete workup for vitamin B12 deficiency (defined as a vitamin B12 level <350 pg/mL without a follow-up methylmalonic acid level or cyanocobalamin prescription), or who received a complete workup for vitamin B12 deficiency (defined as a vitamin B12 level >350 pg/mL, or a vitamin B12 level <350 pg/mL with a follow-up methylmalonic acid level and/or cyanocobalamin prescription). Anemia: no vitamin B12 measured, n = 8 (29%); incomplete vitamin B12 workup, n = 11 (39%); complete vitamin B12 workup, n = 9 (32%). Neuropathy: no vitamin B12 measured, n = 14 (42%); incomplete vitamin B12 workup, n = 9 (27%); complete vitamin B12 workup, n = 10 (30%).
Discussion
VITAMIN B12 MONITORING
Less than 1% of study subjects met the recommendation of having a serum vitamin B12 level measured annually while on high-dose metformin therapy; most never had the level determined. This finding persisted regardless of the duration of high-dose metformin therapy. The risk of developing a metformin-induced vitamin B12 deficiency is positively correlated with the duration of metformin use. 3 Thus, it is notable that among subjects with a duration of high-dose metformin treatment of 10 years or more, nearly half (46%) never had a vitamin B12 level measured during therapy (Figure 1). These individuals were at the greatest risk for vitamin B12 deficiency, and the lack of monitoring in these subjects may have resulted in several cases of vitamin B12 deficiency being undiagnosed and untreated.
As previously discussed, patients with a potential subclinical vitamin B12 deficiency (defined in this study as a vitamin B12 level <350 pg/mL) should have a more sensitive marker, such as MMA, measured.2,10 In this study, subjects with low-normal vitamin B12 levels did not routinely have follow-up MMA levels evaluated. Clinically significant vitamin B12 deficiencies may have gone undiagnosed and untreated resulting from this lack of thorough monitoring.
Lack of awareness may explain the results found in this study. While monitoring vitamin B12 with metformin may be novel to some, the relationship between metformin and vitamin B12 deficiency has been recognized for several decades, and monitoring vitamin B12 was a recommendation during the time frame of this retrospective study.5–7 However, while this recommendation is included in readily available drug information sources, the clinical practice guidelines from the American Diabetes Association do not mention the need to monitor vitamin B12. The guidelines do not include such specific recommendations regarding monitoring parameters for the medications used to treat diabetes. Thus, the lack of vitamin B12 monitoring found in the study could be because many providers may be unfamiliar with this adverse effect of metformin and unaware of the recommendation to monitor the vitamin.
Given the low rates of vitamin B12 monitoring seen in this study, it is prudent to note that annual injections of vitamin B12 have been suggested as an alternative to annual monitoring of vitamin B12 levels in patients on long-term therapy. This approach may be more cost-effective and could also be considered, especially if access to primary care or laboratory services is a concern. 9
INCIDENCE OF VITAMIN B12 DEFICIENCY, ANEMIA, AND NEUROPATHY
Vitamin B12 Deficiency
A new vitamin B12 deficiency was documented in the charts of 2.5% of subjects after an average of 4.5 years of metformin therapy. However, 5.5% of subjects had new prescriptions for cyanocobalamin supplementation, which suggests that a larger percentage than was documented experienced a clinically significant decrease in vitamin B12 levels while on high-dose metformin therapy. The proportion of patients with clinically significant decreases in vitamin B12 may have been even greater, as an additional 18% had a vitamin B12 level less than 350 pg/mL but no follow-up measurement of MMA levels and no prescription for cyanocobalamin. Thus, when including the 5.5% of subjects who received cyanocobalamin supplementation and the 18% with a potential subclinical vitamin B12 deficiency, it is possible that up to 23.5% of patients may have experienced a clinically significant decrease in vitamin B12 during high-dose metformin therapy. These findings are comparable to those in other studies, which identified 10–30% of patients on long-term metformin therapy as having some degree of vitamin B12 malabsorption.5–7 The percentage of individuals in this study who received cyanocobalamin supplementation (5.5%) is slightly lower than the reported rate of vitamin B12 deficiency in patients on long-term metformin (6–9%).5–7
Anemia
Measuring vitamin B12 and folate levels is often part of a routine evaluation when a patient is found to have anemia. 17 However, 29% of subjects in this study with a new documentation of anemia during high-dose metformin therapy did not have a vitamin B12 level measured; an additional 36% with a vitamin B12 level less than 350 pg/mL did not have a follow-up MMA level or a cyanocobalamin prescription documented. Thus, up to 64% of the subjects on high-dose metformin with anemia may have had a clinically significant vitamin B12 deficiency underlying their anemia that went undetected.
Neuropathy
Neurologic damage, a possible consequence of metformin-induced vitamin B12 deficiency, can present as peripheral neuropathy and may be mistaken for diabetic neuropathy in patients on high-dose metformin. 9 In these patients, detection of a vitamin B12 deficiency and correction with cyanocobalamin is a simple means to potentially halt progression of the neuropathy and prevent permanent neurologic damage. In addition, the findings of Wile and Toth demonstrated that metformin-treated diabetic patients had more severe worsening of peripheral neuropathy compared to diabetic patients with neuropathy who were not on metformin. 18 In our study, less than one third of subjects with a new documentation of neuropathy received a comprehensive workup for vitamin B12 deficiency (Figure 3). Although particular attention should be paid to monitoring vitamin B12 levels in diabetic patients on metformin who have or develop neuropathy, the lack of vitamin B12 monitoring seen in the overall study population persisted in the subjects with neuropathy, a patient population for whom the consequences of an untreated vitamin B12 deficiency may be most significant.
STUDY STRENGTHS AND LIMITATIONS
This study has several strengths. Only subjects at high risk of metformin-induced vitamin B12 deficiency were included in the study, as all patients were on high doses for considerable periods. Thus, the subsequent finding that vitamin B12 was not being adequately monitored has greater significance given that this lack of monitoring occurred in a high-risk population. The use of an integrated electronic medical record that includes medical diagnoses and medication prescription information allows for more comprehensive data collection, and the random sample of patients included in the study provides a more accurate picture of actual clinical practice.
This study also fills a gap in the literature. While several studies demonstrating the relationship between metformin use and vitamin B12 deficiency support the need for routine monitoring of serum vitamin B12 levels, there is a lack of studies that examine whether this monitoring is being performed in the clinical setting. This study adds to the literature by highlighting the fact that patients on long-term, high-dose metformin do not routinely have vitamin B12 levels measured, despite mounting evidence in favor of doing so, and potential cases of reversible vitamin B12 deficiencies may therefore go undiagnosed.
The study is not without limitations, however. Due to the study's retrospective design, there are inherent limitations to the data. For example, with use of refill records alone, it was not possible to determine adherence to the prescribed metformin regimen. In addition, only medical conditions and medications explicitly recorded in a subject's medical record and medication lists were reviewed for inclusion, exclusion, and data collection. Thus, some patients may have had active medical conditions that were not documented in their computerized medical records, and therefore the information was not available. This may have led to an underrepresentation of the incidence of vitamin B12 deficiency, anemia, and neuropathy in this study. This is evidenced by the fact that while only 6 subjects had a documented vitamin B12 deficiency, 13 patients had a new prescription for cyanocobalamin supplementation during the study period.
Because data were obtained only from the electronic medical records of the VAMHCS, it is possible that subjects may have previously filled prescriptions, including metformin, outside of the VA system. Therefore these non-VA medications and durations of use were not documented during chart review and data collection.
Finally, data were recorded only for the period after subjects had been started on high-dose metformin. They may have been receiving a lower dose of metformin, resulting in a difference between the recorded duration of high-dose metformin therapy versus the total duration of metformin therapy at any dose. As such, the cumulative duration of metformin use at any dose was not captured and could not be analyzed in reference to the development of vitamin B12 deficiency or related complications. In addition, while all subjects were on high-dose therapy at the start and end of the study period, subjects who had temporary dose adjustments to doses <2000 mg/day during the study period were not excluded and these dose adjustments were not explicitly accounted for in the study. This is a limitation, as these subjects would technically be at a slightly lower risk during the time of lower dose therapy. However, this is unlikely to significantly affect the results, since the purpose of the study was to evaluate overall vitamin B12 monitoring patterns in a higher-risk group of patients rather than to prove a dose-dependent relationship between metformin and vitamin B12 levels.
In conclusion, the results of this study demonstrate that vitamin B12 levels are not being routinely monitored as recommended in patients on long-term, high-dose metformin therapy. The discrepancy between recommended and actual practice is possibly caused by a lack of awareness regarding the effects of metformin on vitamin B12 absorption. It is important to educate providers about the utility of checking a vitamin B12 level annually in patients on long-term, high-dose metformin therapy, given that measuring a serum vitamin B12 level is a readily available laboratory test and the detection and correction of a simple vitamin B12 deficiency can prevent unnecessary permanent neurologic damage and anemia in this patient population.
Because the vitamin B12– deficient state induced by metformin can emerge over the course of 10–15 years, this issue will likely become more clinically significant, considering that metformin has been on the US market for 16 years. It is possible that the rates of vitamin B12 deficiency attributed to long-term use of high-dose metformin could increase substantially. It is imperative that clinicians be aware of this potentially serious, yet easy-to-treat, adverse effect of metformin and be proactive in annually monitoring serum vitamin B12 levels in this high-risk population.