
Abstract
OBJECTIVE
To review the use of number needed to treat (NNT) and/or number needed to harm (NNH) values to determine their relevance in helping clinicians evaluate cost-effectiveness analyses (CEAs).
DATA SOURCES
PubMed and EconLit were searched from 1966 to September 2012.
STUDY SELECTION AND DATA EXTRACTION
Reviews, editorials, non–English-language articles, and articles that did not report NNT/NNH or cost-effectiveness ratios were excluded. CEA studies reporting cost per life-year gained, per quality-adjusted life-year (QALY), or other cost per effectiveness measure were included. Full texts of all included articles were reviewed for study information, including type of journal, impact factor of the journal, focus of study, data source, publication year, how NNT/NNH values were reported, and outcome measures.
DATA SYNTHESIS
A total of 188 studies were initially identified, with 69 meeting our inclusion criteria. Most were published in clinician-practice–focused journals (78.3%) while 5.8% were in policy-focused journals, and 15.9% in health-economics–focused journals. The majority (72.4%) of the articles were published in high-impact journals (impact factor >3.0). Many articles focused on either disease treatment (40.5%) or disease prevention (40.5%). Forty-eight percent reported NNT as a part of the CEA ratio per event. Most (53.6%) articles used data from literature reviews, while 24.6% used data from randomized clinical trials, and 20.3% used data from observational studies. In addition, 10% of the studies implemented modeling to perform CEA.
CONCLUSIONS
CEA studies sometimes include NNT ratios. Although it has several limitations, clinicians often use NNT for decision-making, so including NNT information alongside CEA findings may help clinicians better understand and apply CEA results. Further research is needed to assess how NNT/NNH might meaningfully be incorporated into CEA publications.
A concern often expressed by cost-effectiveness analysis (CEA) researchers is that the results are not consistently implemented in practice settings.1–6 The International Society for Pharmacoeconomics and Outcomes Research (ISPOR) task force on use of pharmacoeconomics/health economic information in health care decision-making conducted a systematic literature review and found several reasons for lack of use of CEA evidence in clinical research. 2 Lack of expertise in interpreting health economic measures, inability to conceptualize gains in quality-adjusted life-years (QALYs), and lack of relevance to clinical settings were among the main reasons. If health economic evidence were presented in a format more understandable to clinical decision-makers, it may increase the likelihood of such findings being implemented in practice settings. One way to improve understanding of health economic evidence by clinical decision-makers is to provide clinical end points along with health economic end points in such studies. 7
The number needed to treat (NNT) and number needed to harm (NNH) are commonly used outcome measures in clinical settings, providing a quick, short-hand approach to estimating relative efficacy of different treatments.8–13 These measures are easily understood by clinicians and are widely used in clinical decision-making, despite several limitations.14–16 For example, Stang and coworkers described how NNT may be difficult to interpret if comparators are not specifically stated, NNT is rounded unnecessarily, or the period for treatment effect is not specified. 15 Despite these shortcomings, NNT is often used as a tool in medical decision-making under the general rubric of evidence-based practice. 17 Thus, including NNT into CEA publications may increase understanding and relevance of CEA findings to clinical decision-makers.
When incorporated into CEA studies, NNT (or NNH) values may be compared with incremental cost-effectiveness ratios (ICERs). A recent example is a CEA of prostate cancer screening, based on the European Randomized Study of Screening for Prostate Cancer. 18 Investigators found that 413 persons would need to be screened for prostate-specific antigen to prevent 1 death from prostate cancer. Based on screening costs plus lifetime treatment costs for patients with prostate cancer, the ICER was $5,227,306 to prevent 1 death from prostate cancer or $262,758 per life-year saved. This article, published in a clinician-practice–focused journal, Urology, provides a well-designed CEA that incorporates NNT. Therefore, we sought to review other CEA studies that incorporated NNT to see how frequently and in which journals such studies are published.
Our purpose was to review the literature reporting results of CEA along with NNT and/or NNH. We summarized our findings by type and year of publication, impact factors of the journals, type of intervention assessed, method used to report NNT in a CEA study, conflicts of interest/funding sources, and data sources used. For this article, NNT and NNH include NNT to benefit (NNTB) and NNT to harm (NNTH), respectively. 13
Methods
We searched PubMed and EconLit from 1966 through September 2012, using the Boolean indicator “and,” the MeSH term cost-benefit analysis, or the key words cost-effectiveness analysis, cost-effectiveness, and cost-utility analysis. These terms were separately combined with the following: number needed to treat, number needed to harm, NNT, or NNH. We excluded reviews, editorials, non–English-language articles, and articles that did not present NNT, NNH, or cost-effectiveness ratios. We included CEA studies reporting cost per life-year gained, per QALY, or other cost per effectiveness measure (eg, cure, complication avoided). Of all included studies, full-text articles reviewed to extract study information by type of journal, impact factor of the journal, focus of study, data source, publication year, how NNT/NNH was reported, and outcome measures.
Based on the description and statement of each journal on the publisher's website, we classified journals into 3 categories: clinician-focused practice journals (eg, Journal of Infectious Diseases), policy-focused journals (eg, Journal of Managed Care Pharmacy), and health-economics–focused journals (eg, Pharmacoeconomics). We further reviewed the 2010 impact factor of each journal in which the articles were published. We identified greater than 3.0 as the top quartile of journals by impact factor as follows: (1) we consulted the Journal Citations Reports by Thompson Reuters, (2) we compiled a list of all of the medical, disease specialty, health policy, health services research, and health economic journals, and (3) we determined the total number of journals and divided them into quartiles by impact factor. The health care focus of each included article was defined as disease treatment, disease prevention, disease management, or patient education. We also summarized the studies according to data sources: (1) randomized controlled trials (RCTs) conducted primarily for the purpose of CEA (RCT-CEA), (2) RCTs with primary purpose other than CEAs (O-RCT-CEA), (3) observational studies based on a large database of health care observational data (OBS-CEA), and (4) CEA based on data obtained from a review of published literature (LIT-CEA). The way NNT/NNH in the CEA was reported was also summarized into 3 groups. We distinguished studies that stated NNT/NNH separately from CEA versus those that reported NNT/NNH as part of the CEA. Among those that reported NNT/NNH separately from CEA, we differentiated the studies using QALYs as the effectiveness measure.
Two authors (DWR and VG) conducted the literature search and extracted full text of the included studies. Four authors (DWR, VG, XS, and YC) reviewed the included studies. One author (VG) reviewed all of the articles. Three authors (DWR, XS, and YC) reviewed one third of the articles each. Any conflicts were resolved by discussion among all 4 authors.
Results
The flow diagram of the literature search is shown in Figure 1. Our initial PubMed and EconLit searches yielded 169 and 21 CEA articles mentioning NNT and NNH, respectively. Articles that did not meet our inclusion criteria (n = 121) were reviews (n = 33), editorials (n = 4), non–English-language (n = 11), and those that did not report NNT/NNH values (n = 73). Furthermore, 4 QALY articles including NNT/NNH were excluded because associated costs were not described. Therefore, after executing inclusion and exclusion criteria, 69 articles remained for full-text review and analysis.
From full-text review, we did not find any CEA studies incorporating NNH. This finding is based on the terminology used in the reviewed articles to represent NNT and NNH. None of the NNT values reported used an implied meaning of NNT to represent NNH/NNTH. The selected articles were summarized by treatment/disease condition, focus of study, type of CEA, and measure of NNT in Appendix I (available at www.hwbooks.com/pdf/appendices/R417.pdf). We included information about journal title, year of publication, and journal impact factor and provided additional comments. Key features, including journal type, journal impact factor, focus of studies, the way NNT was reported in CEA, and data source for each article are displayed in Table 1.
Among the 69 articles that incorporated NNT into CEA, 80% were published in clinician-practice–focused journals.8–11,14–16,18–67 Health-economics–focused journals published 11 (15.9%) articles.68–78 Overall, the majority (72.4%) of the articles incorporating NNT/NNH in CEA were published in the highest quartile of journals based on impact factor (>3.0).18,19,21–35,38,39,41,42,44,45,49,53,55–57,59,60,63,64,66,69–86 Moreover, 8.7% of all articles were published in journals with impact factors greater than 10, which were all clinician-practice–focused journals.23,24,26–28,74
A large percentage of articles focused on disease treatment (40.5%) or disease prevention (40.5%) (Table 1). The cost-effectiveness of patient education was assessed in 4.3% of the articles.42,64,87 NNT separated from CEA based on QALY was reported in 24.6% of the studies,23,27,34,37,41,43,45,46,48,54,56,77–80,82,83 whereas 27.5% of the studies reported NNT separated from CEA based on events.18,19,24–26,28,33,39,40,59,62,67,71,72,74,76,84–86 Literature was used as the data source in 53.6% of the articles.18,19,21–25,27,32,34–37,40,41,43,45,47,53,56,57,61,62,64,68–71,73,74,76–78,81–86 Randomized controlled trials (O-RCT-CEA and RCT-CEA) comprised 24.6% of the studies'data sources.26,28–30,33,38,39,42,46,48,49,58,72,75,79,80,87
Discussion
The number of CEAs published is increasing each year. The Health Economic Evaluations Database (HEED) alone consists of more than 44,000 health economic evaluations and is updated monthly with approximately 250 new studies. 88 We found only 62 health economic evaluations that incorporated NNT. Therefore, the studies incorporating NNT into CEA represent a small fraction of published health economic evaluation studies.
We classified approaches to incorporate NNT (or NNH) into CEAs into 2 categories: (1) indirect methods, and (2) direct methods. Indirect methods involve reporting NNT (or NNH) separate from QALYs or other health economic outcome measures, such as CEA ratios or incremental CEA ratios. All CEAs that currently incorporate NNT/NNH fall under this category, based on our review. For example, a CEA published in the Annals of Internal Medicine (2010 impact factor = 16.729) compared the cost-effectiveness of implantable cardioverter-defibrillator and amiodarone after myocardial infarction and reported NNT (defined as NNT to prevent 1 arrhythmic death) separately from cost per QALY gained as follows: in comparison with amiodarone, the ICER for implantable cardioverter-defibrillator was $71,700–557,900 per QALY gained. NNT was 9.6 to 21.2 for implantable cardioverter-defibrillator and 14.4–146.8 for amiodarone, depending on the ejection fraction (varied from <0.3 to >0.4).23 In another example, a CEA published in British Medical Journal (2010 impact factor = 13.471) examined the cost-effectiveness of community occupational therapy for older patients with dementia, reporting NNT per 1 successful treatment of dementia as 2.8 (95% CI 2.7–2.9). Cost per QALY gained for occupational therapy, in comparison with usual care, was $10,666/QALY. 28 These 2 articles demonstrate a concise manner for interpreting NNT alongside CEA.
Direct methods involve using mathematical models to establish direct functional relationships between NNT (or NNH) and health economic outcome measures. Such relationships vary on a case-by-case basis and require adjustment for other factors, such as the time horizon of the analysis. For example, Kristiansen and Gyrd-Hansen found that, as a treatment's effectiveness changes over time (improves or decreases), NNT also varies and the relationship between NNT and quality of life changes. 89 As a result, use of NNT ratios alone in long-term CEA studies may be misleading.
Examples of such direct methods regarding risk-benefit assessment can be found in the literature. 90 These include outcome measures such as Quality-adjusted Time Without Symptoms and Toxicity (Q-TWiST), Relative Value Adjusted Number Needed to Treat (RV-NNT) and RV-NNH, and Incremental Net Health Benefit (INHB).90–92 For instance, Q-TWiST is an estimator to determine QALYs by adjusting life expectancy with the respective utility weights by summing (1) QALYs based on time with toxicity from chemotherapy, (2) followed QALYs for time free of symptoms of disease or chemotherapy toxicity, (3) plus QALYs for time with disease symptoms. 92 As proven, Q-TWiST is an asymptomatically consistent and normally distributed estimator with variance that can be consistently calculated. 93 The establishment of a direct functional relationship between NNT and QALY is beyond the scope of this review. Nonetheless, further research in this field may lead to better understanding of such relationships.
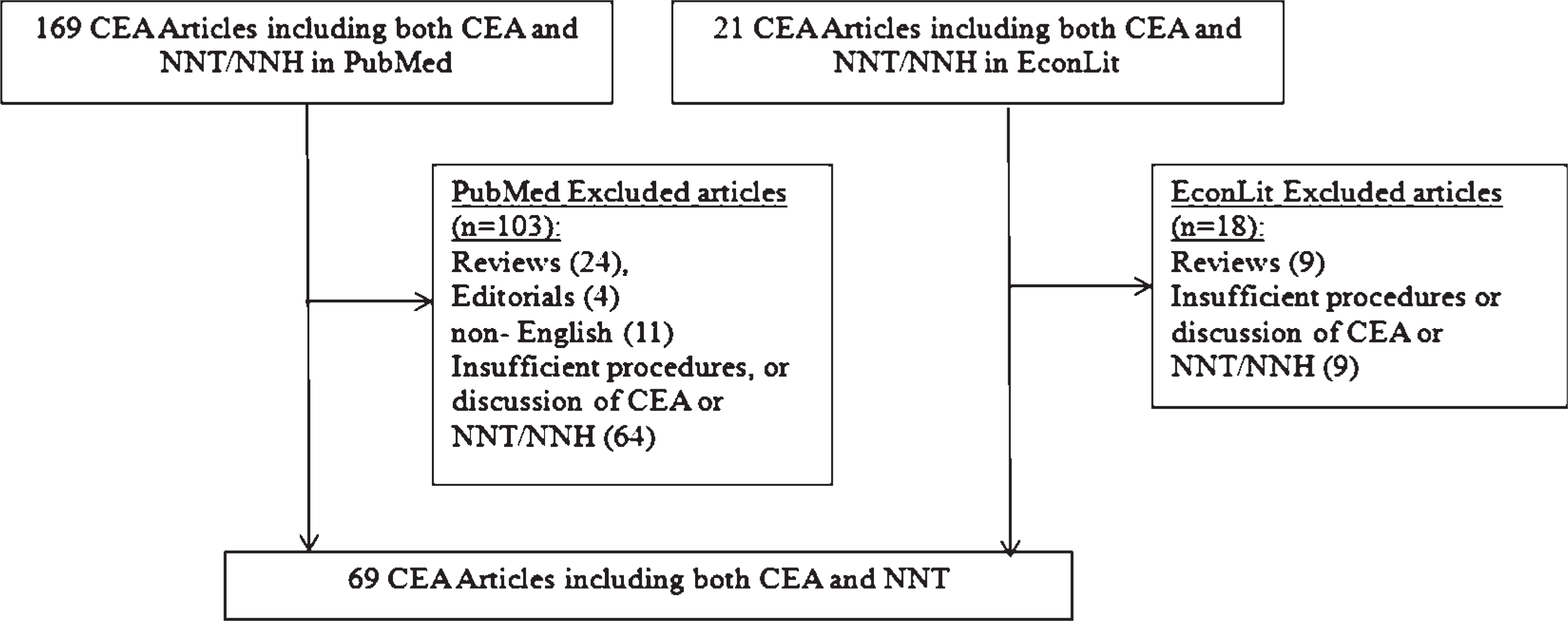
Literature search flowchart. CEA = cost-effectiveness analysis, NNH = number needed to harm, NNT = number needed to treat.
Indirect methods to incorporate NNT (or NNH) into CEAs may be more transparent than direct methods, since the former do not suffer from constraints of establishing a functional relationship between NNT (or NNH) and health economic outcomes measures. Either way, QALYs are health economic measures incorporating both benefits and harms of each treatment's outcome. 17 In contrast, NNT (or NNH) simply summarizes the proportion of patients impacted positively (or negatively) by the treatment. Further, QALY values at the terminal ends of decision tree models summarize the impact of all outcomes along the branch of the decision tree on health-related quality of life, while NNT (or NNH) usually describes 1 or 2 potential outcomes. NNT cannot be compared across different health conditions and response variables (eg, interventions to treat the common cold vs cancer). Therefore, QALYs provide significantly more information regarding the impact of different outcomes that may result from therapeutic alternatives rather than the few outcomes addressed by NNT or NNH. Incorporating both values may help clinicians perceive the relationships between the measures.
Notably, we found that 40.5% of CEA articles incorporating NNT involved comparisons of a specific disease treatment and an additional 40.5% involved disease prevention. Only a small proportion of studies involved disease management (14.5%) or educational interventions (4.3%). This reflects the relative proportions of treatment and prevention CEAs versus disease management CEAs. It may also be associated with the multiple outcomes measured by disease management studies, which would require the reporting of several NNT values.
We found that 72.4% of all of the eligible articles were published in the top quartile of journals by impact factor and only 2% of the articles were published in the bottom quartile (impact factor ≤1). Since most articles that integrate NNT into CEAs were published in clinician-practice–focused journals (78.3%), these findings indicate that CEA studies incorporating NNT are generally of high clinical impact. This does not indicate that CEA studies are of higher quality, which would involve assessment of the methodologic sophistication and scientific rigor in the conduct of the study, among other factors. The data sources for the CEA studies incorporating NNT were based on published work (53.4%), followed by studies reporting data from randomized clinical trials (24.6%, Table 1). This may simply reflect the use of literature review in high proportions of published CEAs. NNTs have utility only when the evidence on which they are based fulfills criteria of quality, validity, and size. 94 Of all types of studies, randomized clinical trials, especially large randomized trials, are most likely to best fulfill all of these criteria. Nonetheless, we found only 24.6% of randomized trials (O-RCT-CEA plus RCT-CEA) that incorporated NNT.
Classification of 69 Reviewed Studies
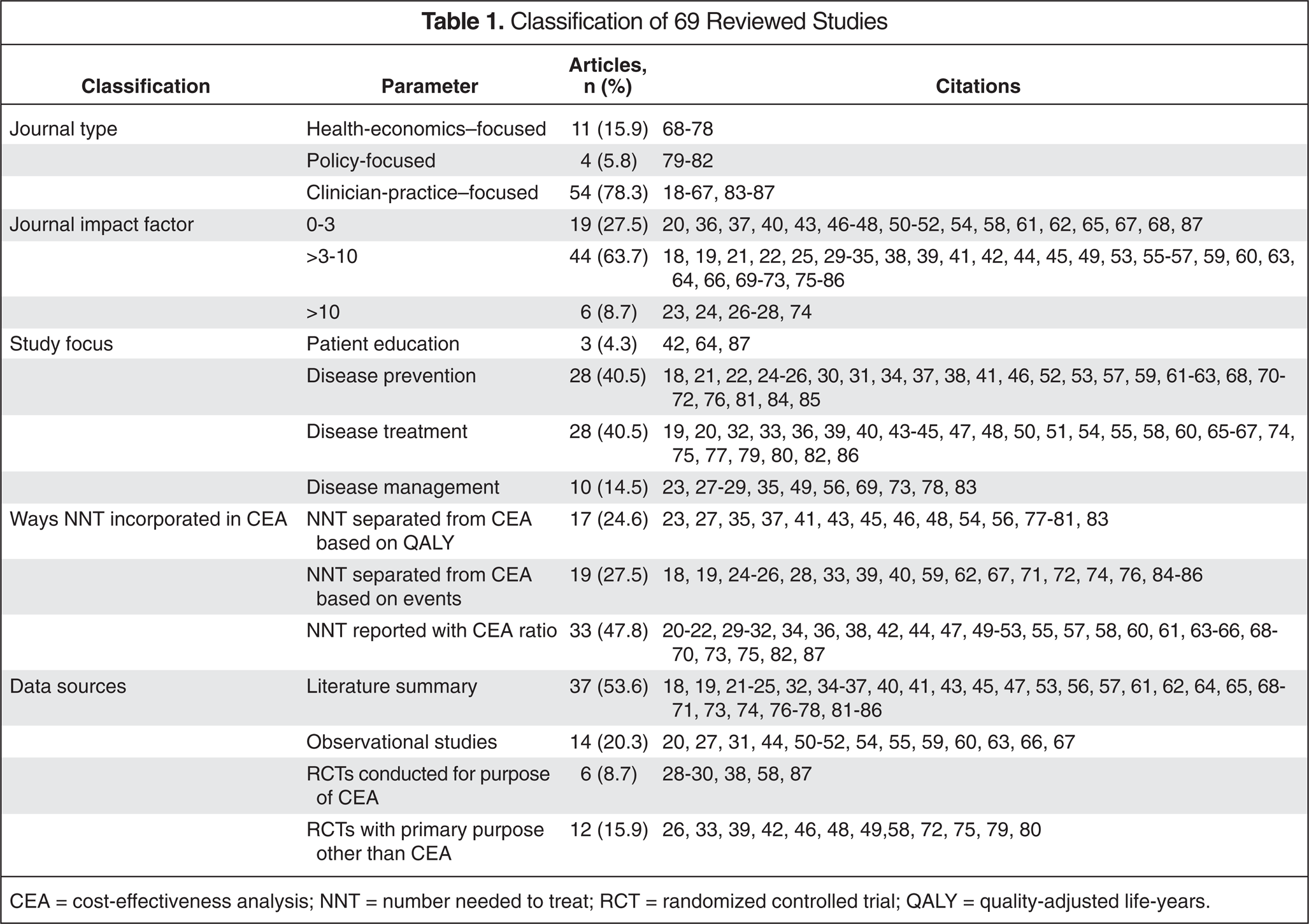
CEA = cost-effectiveness analysis; NNT = number needed to treat; RCT = randomized controlled trial; QALY = quality-adjusted life-years.
Further research regarding the co-reporting of NNT within CEAs might involve (1) developing surveys of clinicians comparing their understanding of CEAs with or without NNTs, (2) establishing tools for adjusting NNT/NNH by quality of life measures, similar to Q-TWiST, RV-NNT, RV-NNH, or INHB, (3) comparing of implementation of CEAs that include NNT versus those that do not, or (4) incorporating other risk-benefit assessment techniques, such as Multi-Criteria Decision Analysis, into estimates of NNT/NNH. 90
Our study is not without limitations. First, we excluded non–English-language literature from our search. Although not likely to impact our findings substantially, 8 additional studies in other languages came up in our search before the application of inclusion/exclusion criteria. Second, we did not consider the time horizon of each study as an evaluation criterion in our study. As previously shown, NNT should not be used for measures of benefit in CEAs when benefits or adverse effects vary over time. 89 Third, some CEA studies incorporating NNT may not have been published because of the existing bias in the literature (ie, only CEA studies having favorable or positive results were published). Fourth, because of resource constraints, we searched only 2 databases (PubMed and EconLit). Review of other databases, such as EMBASE, may reveal additional publications. However, per our previous experience, we expected to find few unique eligible articles by searching EMBASE.
We found a relatively small number of studies incorporating NNT into the results of CEA. The majority of the studies were published in clinician-practice–focused journals. While there are limitations to NNT, these results are commonly used clinically and can serve as a bridge to help clinicians relate these results to more detailed, and perhaps more useful, CEA. This would involve including NNT information in CEA, which may help bridge that gap of understanding and assist decision-makers in applying CEA results to decisions in clinical settings. Further research may be needed to determine whether these studies are more understandable by clinicians and increase implementation of CEA results in clinical settings. Additionally, researchers may need to explore possibilities as to how best to incorporate theoretically sound NNT/NNH values into health economic evaluations.
Summary
We reviewed the literature to identify studies that reported results of CEAs along with NNT and/or NNH. We found that CEA studies incorporating NNT are generally published in clinician-practice–focused journals, but represent a small proportion of total published CEAs. Furthermore, only 14.5% and 4.3% of the CEA articles incorporating NNT focused on disease management and educational interventions, respectively. Since NNT/NNH are often used as decision tools by clinicians, it may increase clinical relevance and application of CEA results to include this information. Increased understanding of relationships between CEA and NNT/NNH may help clinicians apply CEA findings in practice. We recommend further research to explore whether NNT/NNH could be meaningfully incorporated into health economic evaluation studies.