
Abstract
BACKGROUND:
Vancomycin-resistant enterococci (VRE) are a common cause of nosocomial urinary tract infections (UTIs) among hospitalized patients. Clinicians need to differentiate between VRE-associated urinary colonization, asymptomatic bacteriuria, and UTIs to determine the need for treatment and length of therapy.
OBJECTIVE:
To characterize the diagnosis and management of VRE from urinary sources, including compliance with institutional treatment guidelines, and identify risk factors associated with clinical failure.
METHODS:
We performed a retrospective, single-center, cohort study among patients with VRE-positive cultures from urinary sources over a 3-year study period (July 2008-September 2011). Descriptive statistics were used to evaluate demographics, diagnostics, guideline compliance, pharmacotherapy, and outcomes. Risk factors associated with clinical failure were identified by multivariate logistic regression analysis.
RESULTS:
Two hundred sixty-nine distinct episodes of VRE met inclusion criteria among 252 patients. Forty-seven percent and 77% of episodes occurred in patients admitted to an intensive care unit and hospitalized for 7 or more days, respectively. Fifty-eight percent of the episodes were classified as asymptomatic bacteriuria or colonization. Compliance with institutional treatment guidelines for the appropriate drug, dose, and duration occurred in approximately 70% of the cases. Among noncompliant cases (n = 83), 48 (58%) were overtreated, and 35 (42%) were undertreated. Clinical failure among all cases was common, including mortality (17.1%). Factors independently associated with clinical failure determined on multivariate analysis included weight 100 kg or more (OR 5.30; 95% CI 1.42–12.21; p = 0.014), renal disease (OR 2.57; 95% CI 1.02–6.47; p = 0.048), indwelling catheter (OR 4.62; 95% CI 1.05–18.24; p = 0.046), and VRE bloodstream infection (OR 15.71; 95% CI 2.9–128.7; p < 0.001).
CONCLUSIONS:
Improved education is needed to minimize cases of overtreatment and undertreatment of VRE-associated UTIs and decrease inappropriate drug-related costs and clinical failure rates. Risk factors for clinical failure can be used to risk stratify VRE-associated UTIs and further guide treatment decisions.
Enterococci are gram-positive cocci commonly found as part of the endogenous gastrointestinal flora. 1 While they are generally considered a low-grade pathogen in otherwise healthy individuals, increased microbial virulence and host susceptibility within the hospital environment have contributed to the emergence of enterococci as one of the most common nosocomial pathogens. 1 –3 Among US hospitals, enterococci are the second most commonly isolated microorganism from catheter-associated urinary tract infections (UTIs). 4 Although over a dozen different enterococcal species exist, Enterococcus faecalis and E. faecium are the most common species responsible for most infections in humans. 1
Over the past decade, there has been a growing concern over the increasing incidence of vancomycin-resistant enterococci (VRE). It is estimated that the number of VRE infections in US hospitals has increased about 2-fold, from 9820 to 21,352 discharges between 2000 and 2006. 5 National Healthcare Safety Network reported that, between 2006 and 2007, 29% of all catheter-associated enterococcal UTIs were vancomycin resistant. 4 Among urinary isolates of E. faecium, vancomycin resistance was even more common, at 81%. Risk factors for the development of VRE infections include the use of broad-spectrum antibiotics, VRE colonization, residence in long-term care or a nursing home facility, poor infection control practices, presence of indwelling catheters, and immunosuppression. 1 –3 Furthermore, VRE infections pose a significant infection control problem to the institutions, since they are associated with limited treatment options, increased health care costs, morbidity, and mortality. 1,3 –7
Since the urinary tract is one of the most common sites of VRE infections, it is important that clinicians differentiate between VRE-associated urinary colonization, asymptomatic bacteriuria, and UTIs to determine the need for treatment, optimal pharmacotherapy, and length of therapy. Patients with sole colonization of VRE generally do not require treatment. 1 –3,7 Treatment should be reserved for patients with confirmed UTIs or for certain high-risk patient populations, such as pregnant women, patients with urinary hardware (eg, nephrostomy tubes and urinary stents), and immunosuppressed patients. 8 –11 In general, since VRE-associated UTIs are of complicated nature in the large majority of patients, duration of therapy should be 7–14 days (Figure 1). 2,3,7
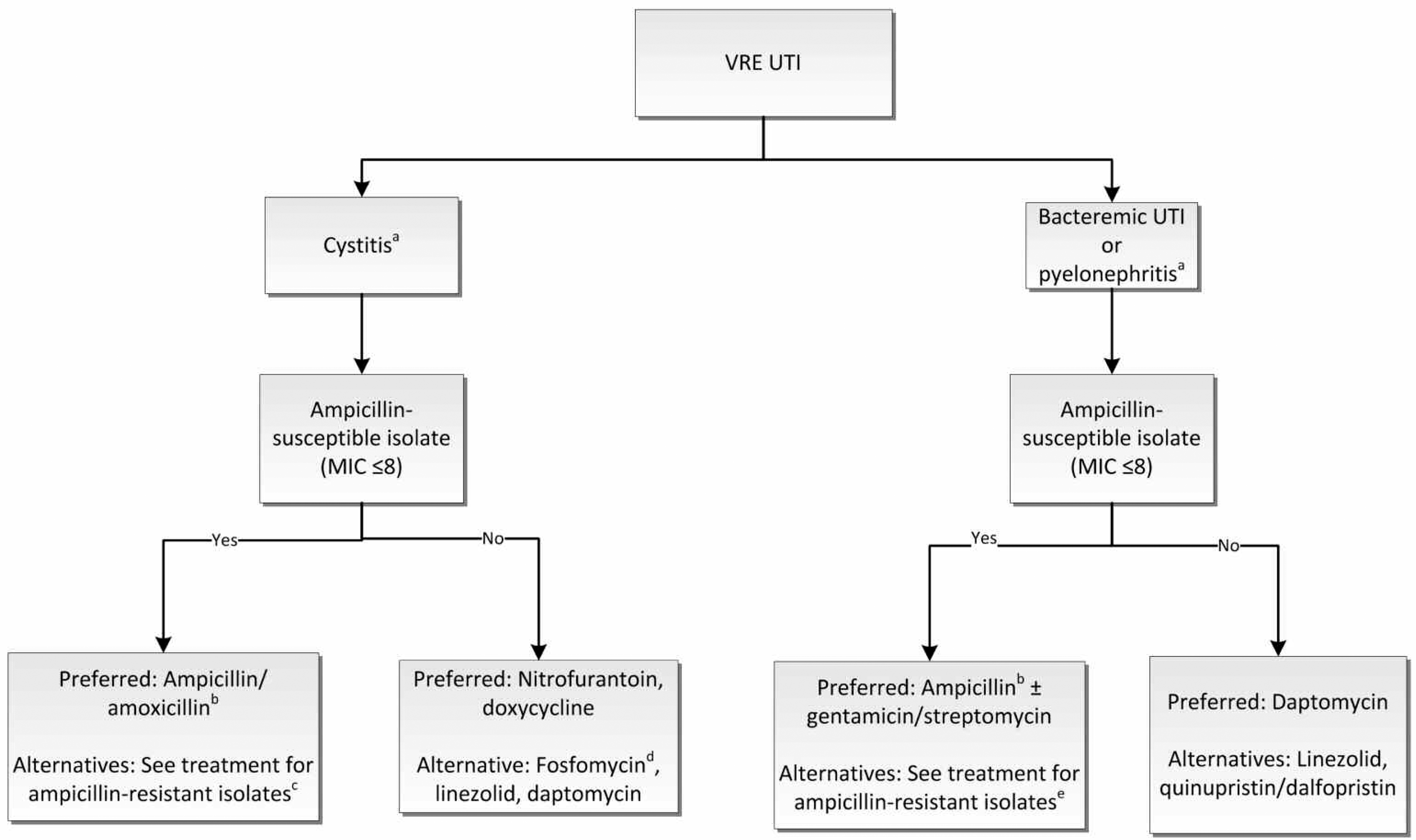
University of California Davis Medical Center treatment algorithm for vancomycin-resistant enterococcal UTIs. MIC = minimum inhibitory concentration; UTI = urinary tract infection; VRE = vancomycin-resistant enterococci.
We developed institutional guidelines for the treatment of VRE-associated UTIs in 2007 to address concerns of inappropriate use of daptomycin and linezolid for questionable diagnoses of VRE-associated UTIs. An extensive review of the management of VRE-associated UTIs, including the updated University of California Davis Medical Center (UCDMC) treatment algorithm (Figure 1), has been published. 2 In summary, our treatment guidelines emphasize the use of less expensive antibiotics with activity against VRE (eg, nitrofurantoin, fosfomycin, doxycycline, and, in select cases, amoxicillin/ampicillin) as the preferred agents for uncomplicated VRE-associated cystitis. 2,12 –14 Newer antibiotics, such as linezolid, daptomycin, and tigecycline, are potential treatment options, but should be reserved for more complicated infections. 2,7
The primary objective of this study was to characterize the diagnosis and management of VRE from urinary sources in inpatients, with particular attention to antimicrobial selection, utilization, and cost, as well as compliance with the institutional VRE-associated UTI treatment guidelines. Secondary objectives were to identify complications associated with VRE-associated UTIs and risk factors associated with clinical failure.
Methods
STUDY DESIGN AND PATIENT POPULATION
This retrospective, single-center, cohort study evaluated consecutive patient encounters with VRE-positive cultures from urinary sources, identified by the microbiology laboratory, over a 3-year study period (from July 1, 2008, to September 30, 2011). The study was conducted at UCDMC, a 631-bed tertiary academic medical center in Sacramento, CA. Patients were included if they had a VRE-positive urinary culture. Patients younger than 18 years, prisoners, and patients with incomplete medical records to determine the treatment course were excluded from the study. The study was approved by the UCDMC institutional review board.
DATA COLLECTION
Patient data were extracted from the UCDMC electronic medical record (EMR). Data included demographic information, concurrent diseases, risk factors, diagnostic procedures, treatment, microbiologic and epidemiologic findings, and outcomes as detailed below.
patient demographics: age, sex, weight, body mass index, service, and intensive care unit (ICU) admission; concurrent diseases, risk factors, and complicated factors: diabetes, renal disease, immunosuppression, history of Clostridium difficile colitis in the last year, VRE infection or colonization documented in the last year, use of broad-spectrum antibiotics in the last 30 days, hospitalizations/health care exposure in the last 90 days, presence of indwelling catheters and urinary hardware, presence of functional or structural abnormalities within the urinary tract, and length of stay; diagnostic evaluation: urinalysis, presence of pyuria, bacteriuria, and urinary symptoms; microbiologic and epidemiologic findings: classification of VRE from urinary sources (asymptomatic abacteriuria, asymptomatic urinary colonization, asymptomatic bacteriuria, cystitis, pyelonephritis, or prostatitis with further classification as urosepsis and/or bacteremic VRE-associated UTI), urinary cultures at onset and within 7 days of completing treatment, urinary source (eg, urine, catheter, urinary stent), community acquired, hospital acquired (including ICU stay at time of isolation), or health care associated, and antimicrobial susceptibilities; treatment: empiric and definitive antimicrobial treatment, antimicrobial dosing, removal of urinary hardware within 7 days of VRE isolation from a urinary source, and guideline compliance; and clinical and microbiologic outcomes: clinical failure, microbiologic failure, 30-day infection-related readmission, and 30-day all-cause mortality;
The UCDMC VRE-associated UTI treatment guidelines were used to assess compliance, including antimicrobial selection, antimicrobial dosing, and duration of therapy (Figure 1). 2 Use of infectious disease (ID) consultation was also assessed.
STUDY DEFINITIONS
Patients were classified on the basis of the definitions listed here. Complicating factors were defined as a urinary tract with functional or structural abnormalities, including long-term indwelling catheters, recent urinary instrumentation, neurogenic bladder, renal calculi, male sex, and/or a history of recurrent UTIs. 2,8,10,11 A high-risk patient was defined as any individual who was immunosuppressed, pregnant, and/or had at least 1 complicating factor. 2,8 –11 Immunosuppression was defined as any patient with grade 3 neutropenia or higher (absolute neutrophil count <1000 cells/mm3), prednisone intake of more than 10 mg daily (or equivalent glucocorticoid) for longer than 7 days, immunosuppressive therapy following solid organ or hematologic transplant, and/or presence of HIV/AIDS. Renal disease was defined as a serum creatinine level above 1.5 mg/dL at the time of VRE isolation and/or documentation of chronic kidney disease or acute kidney injury in the EMR. VRE colonization was defined as VRE identified from any culture in the last year. Broad-spectrum antibiotics associated with increased risk for VRE colonization were defined as third- or fourth-generation cephalosporins, fluoroquinolones, carbapenems, and β-lactam/β-lactam inhibitor combinations. 15,16
The following definitions were used for diagnostic, microbiologic, and epidemiologic findings. Asymptomatic abacteriuria was defined as a urine culture with less than 104 CFUs/mL of VRE with a normal urinalysis in a patient with no symptoms. Asymptomatic urinary colonization was defined as a urine culture with 104 CFUs/mL or more of VRE with a normal urinalysis in a patient with no symptoms. Asymptomatic bacteriuria was defined as pyuria plus a urine culture with 104 CFUs/mL or more of VRE in a patient with no symptoms. Asymptomatic patients without a urinalysis were assumed to have no VRE and were classified as having asymptomatic abacteruria or asymptomatic colonization, as appropriate. Pyuria was defined as 10/mL or more white blood cells in a noncatheterized patient or 5/mL or more white blood cells in a catheterized patient. A UTI was defined as a urine culture with 105 CFUs/mL or more of VRE or pyuria with 104 CFUs/mL or more of VRE from a patient with at least 1 documented sign or symptom for a UTI (eg, fever, frequency, urgency, dysuria, flank pain). 2,8,9,17 Urosepsis was defined as 2 or more systemic inflammatory response criteria plus evidence of a UTI. 18 A bacteremic VRE-associated UTI was defined as VRE isolated from both urine and blood cultures among patients who met criteria for a UTI. Patients with multiple positive VRE cultures from urine sources were documented as new cases if the positive urine culture was detected more than 7 days after the initial culture. Recurrent UTI was defined as 2 VRE-associated UTIs within 6 months or as 3 positive cultures with VRE within the preceding 12 months. 19 Health care—associated VRE exposure was defined as the presence of urinary VRE isolated more than 48 hours after admission among patients hospitalized in the last 90 days or among residents of skilled nursing facility. 20,21 Hospital-acquired VRE exposure was defined as the acquisition of urinary VRE 48 hours after hospital admission. 22
The following definitions were used for the treatment course and patient outcomes. Inadequate empiric therapy was defined as initial use of antimicrobial agents that did not have activity against the microorganisms causing the infection between 24 hours before urine collection for culture and the time the susceptibility results were available. 23 Definitive antibiotic therapy referred to antimicrobial therapy initiated after the culture and susceptibility results were available. For treatment to be considered fully compliant, antimicrobial agents used for definitive therapy needed to match institutional guideline recommendations (including drug, dose, and duration). Overtreatment was defined as treatment received for a VRE-associated UTI when it was not indicated or treatment received when indicated, using a broad-spectrum antimicrobial, an excessive antimicrobial dose, or excessive duration of therapy per institutional guidelines. Undertreatment was defined as lack of treatment when indicated or inadequate treatment (antimicrobial selection, dose, and/or duration of therapy) per institutional guidelines (Figure 1). 2
The composite end point of clinical failure was defined as documented failure in the EMR by a physician, treatment failure (need to extend therapy within 30 days of completing treatment among patients receiving antimicrobial therapy), microbiologic failure (repeat isolate positive within 7 days of completing treatment among patients receiving antimicrobials or within 7 days from initial positive culture among patients not receiving antimicrobial therapy, excluding asymptomatic patients), 30-day infection-related readmission, and/or 30-day all-cause mortality. An evaluable case was defined as a case with adequate EMRs to determine microbiologic and/or clinical outcomes required for the composite end point of clinical failure. Finally, development of a multidrug-resistant pathogen was defined as acquisition of a microbiologic pathogen that is resistant to at least 1 agent from 3 or more antimicrobial classes 7 days from treatment initiation for VRE. 24,25
STATISTICAL ANALYSIS
Descriptive statistics were used to present patient demographics, concurrent diseases and complicating factors, diagnostic criteria, microbiologic data, clinical diagnosis, treatment course, guideline compliance, and patient outcomes. A Student 2-sample t-test and χ 2 or Fisher exact test were used, as appropriate, to evaluate continuous and binary demographic data, respectively, between evaluable and nonevaluable patients. A 2-tailed χ 2 test was used to evaluate the association of ID consultation and guideline compliance, inadequate treatment, and clinical failure. Among evaluable patients, risk factors associated with clinical failure were identified by performing a 2-tailed χ 2 or Fisher exact test, as appropriate, and multivariate logistic regression analysis. Variables at p < 0.20 on univariate analysis were included in the multivariate analysis in an unconditional forward and backward manner. Odds ratios with 95% confidence intervals and corresponding p values were determined. p Values <0.05 were considered statistically significant. Statistical analyses were completed using Minitab software, version 14.
Results
Two hundred ninety-eight consecutive VRE isolates from urinary sources were screened, of which 269 distinct cases met inclusion criteria among 252 patients. There were 252 episodes of E. faecium and 20 episodes of E. faecalis (both species isolated in 3 cases). Baseline demographic and clinical characteristics for all patients, evaluable patients, and nonevaluable patients are summarized in Table 1. Evaluable and nonevaluable patients were similar at baseline. Nearly half (47.2%) of the episodes occurred in patients admitted to an ICU, with an average ICU stay of 21 days (range 1–155), and 76.6% of episodes occurred in patients hospitalized for 7 or more days with an overall mean length of stay of 56 days (range 1–389), representing a high-acuity cohort of patients. Among patients admitted to the ICU, 77 (60.6%), 46 (36.2%), and 4 (3.1%) were considered medical, surgical-emergent, and surgical-elective admissions, respectively. Many patients also had significant comorbidities, including renal disease (42.0%), diabetes (39.8%), and immunosuppression (36.4%).
Patient Demographics, Baseline Characteristics, and Risk Factors for VRE-Associated Urinary Tract Infection
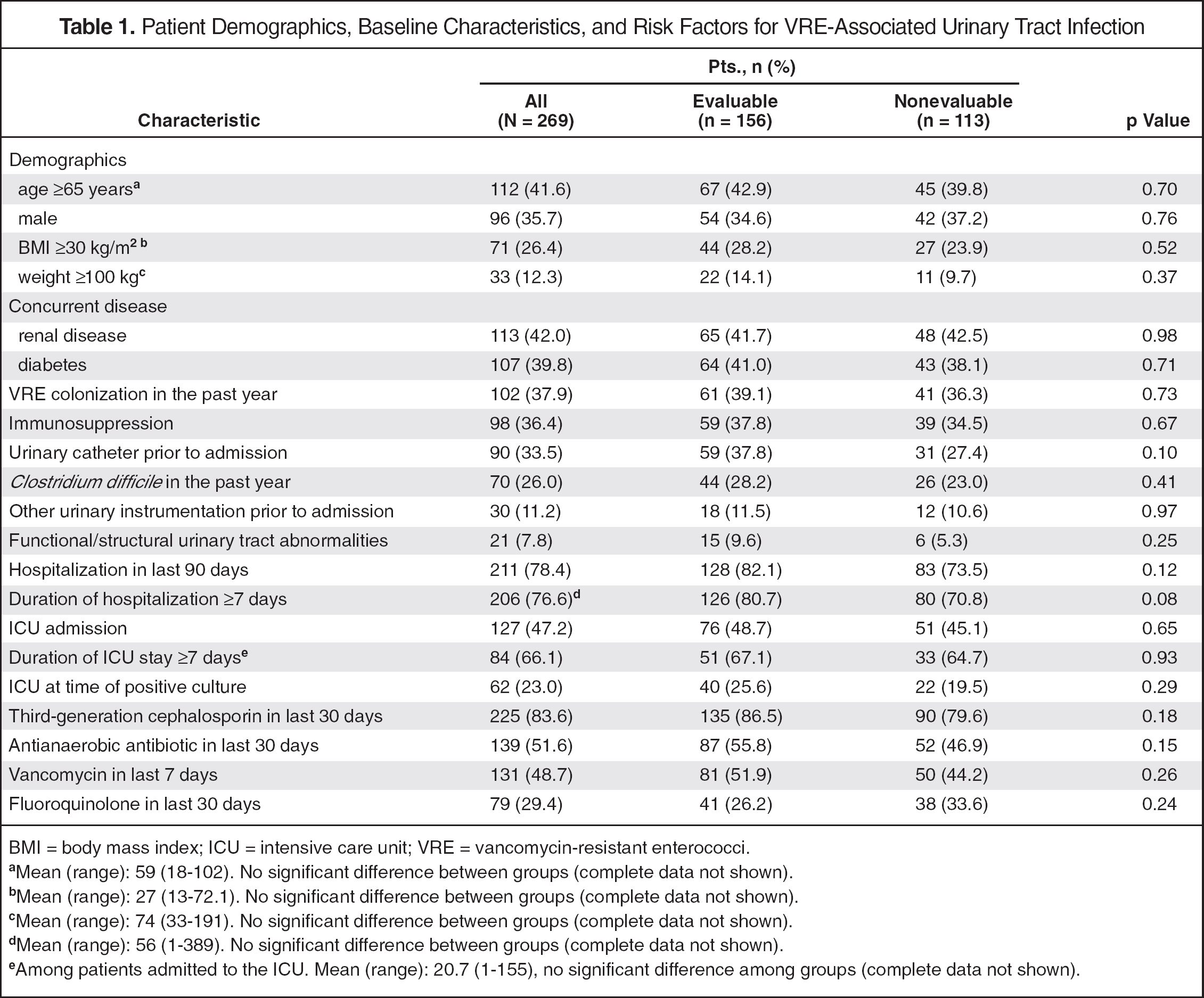
BMI = body mass index; ICU = intensive care unit; VRE = vancomycin-resistant enterococci.
Mean (range): 59 (18–102). No significant difference between groups (complete data not shown).
Mean (range): 27 (13–72.1). No significant difference between groups (complete data not shown).
Mean (range): 74 (33–191). No significant difference between groups (complete data not shown).
Mean (range): 56 (1–389). No significant difference between groups (complete data not shown).
Among patients admitted to the ICU. Mean (range): 20.7 (1–155), no significant difference among groups (complete data not shown).
Diagnostic criteria used to characterize the VRE urinary isolates are summarized in Table 2. Most VRE urinary isolates were either hospital-acquired (66.2%) or health care—associated (13.0%). Fifty-eight percent of the episodes were classified as asymptomatic bacteriuria, colonization, or abacteriuria that generally did not require antimicrobial therapy. Among distinct cases (n = 269), there were 72 (26.7%) episodes of cystitis, 26 (9.7%) episodes of pyelonephritis, and 3 (1.1%) episodes of prostatitis. Fifty-eight (21.6%) cases met the criteria for urosepsis and 17 (6.3%) cases were diagnosed as VRE-associated bacteremia.
Assessment of VRE Urinary Isolates and Diagnostic Criteria for VRE-Associated Urinary Tract Infection a
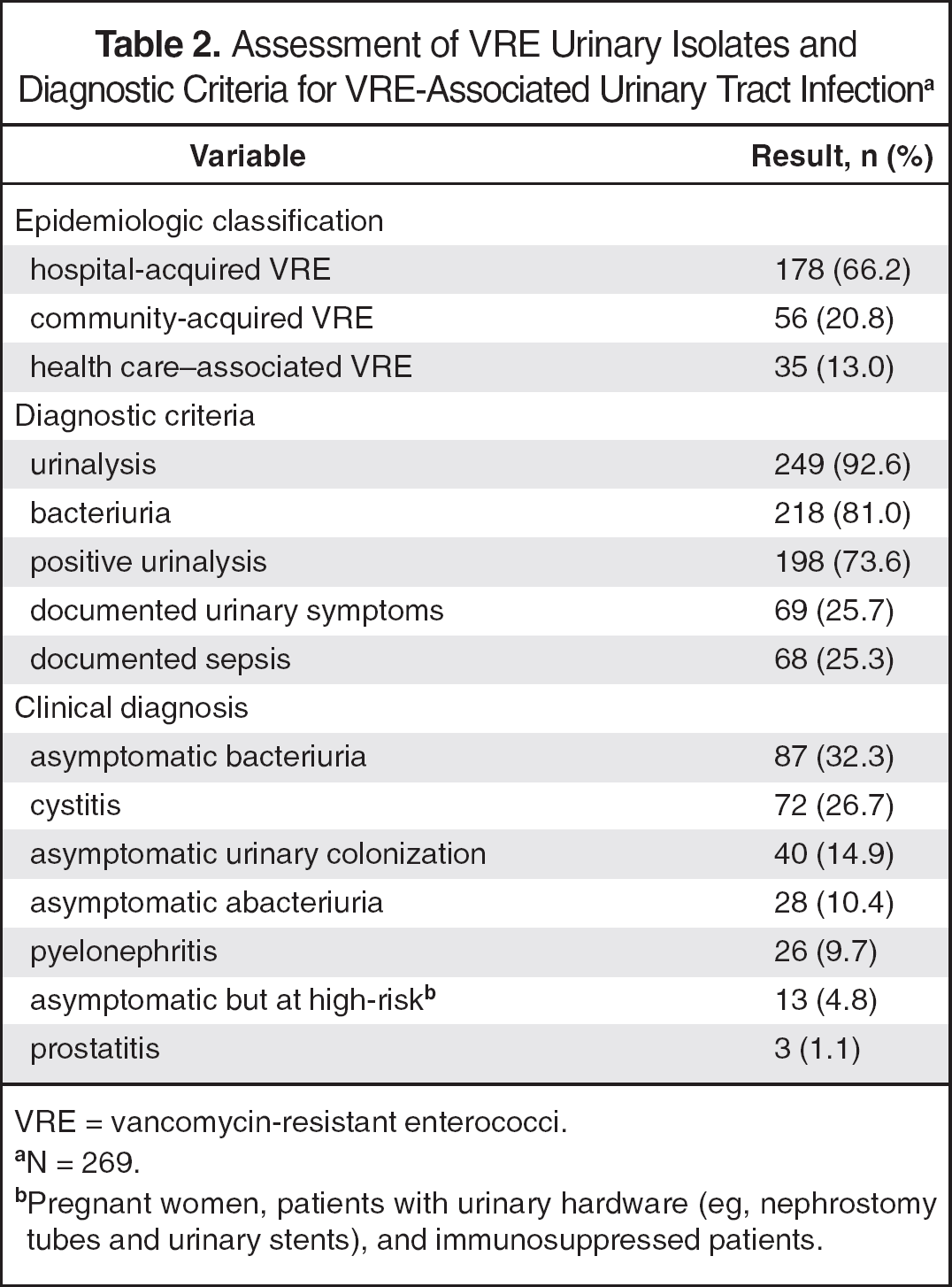
VRE = vancomycin-resistant enterococci.
N = 269.
Pregnant women, patients with urinary hardware (eg, nephrostomy tubes and urinary stents), and immunosuppressed patients.
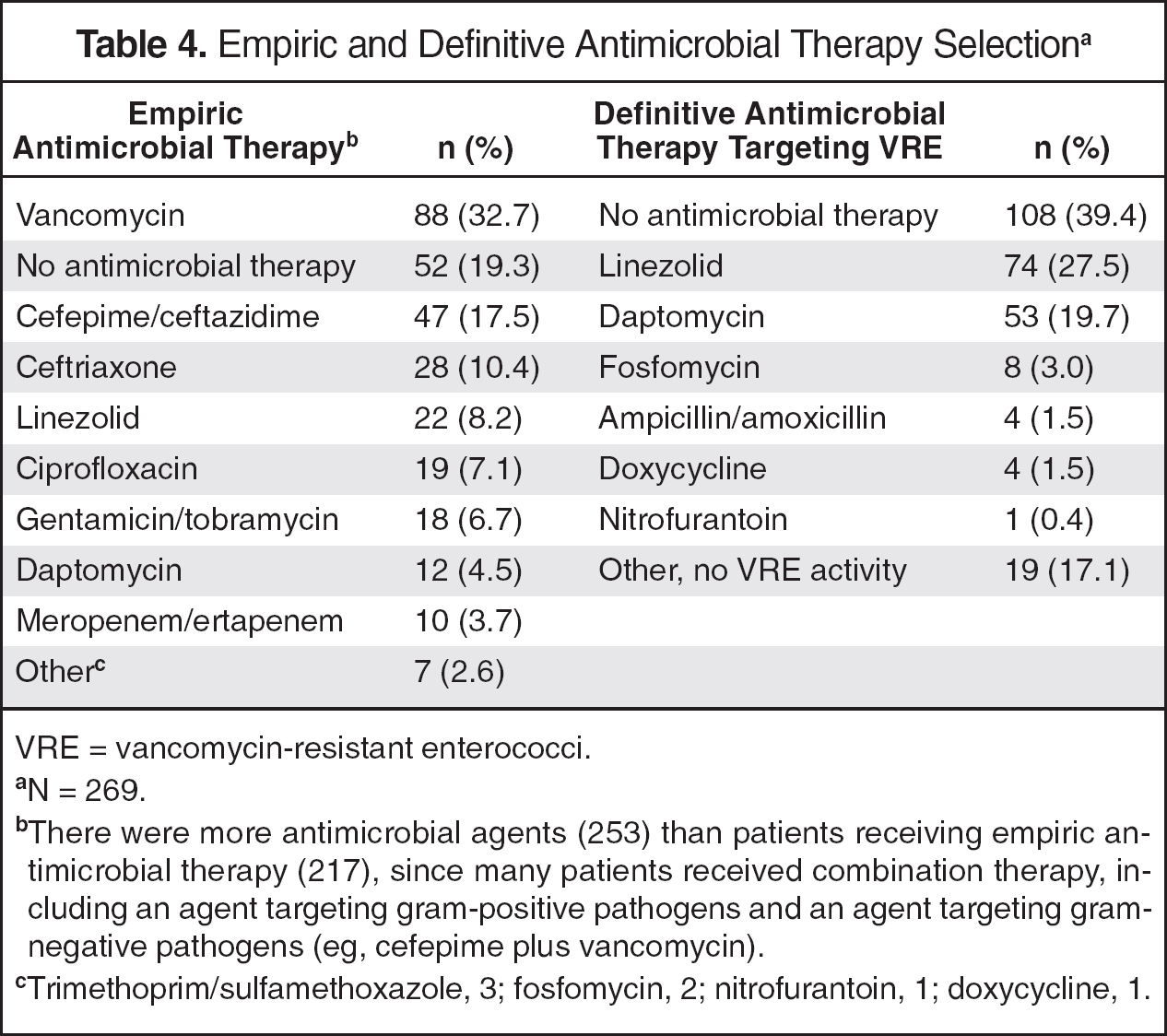
The treatment course, guideline compliance, and urinary catheter care are summarized in Table 3. A wide variety of antimicrobial agents was used for empiric treatment; however, only 37 (13.7%) were active against VRE (Table 4). One-hundred sixty-three (60.6%) patients received definitive treatment for VRE from urinary isolates for an average duration of 7.9 days (range 1–21), including 74 (27.5%) patients with linezolid and 53 (19.7%) with daptomycin (Table 4). Catheter removal was documented in 90 (50.6%) patients with a urinary catheter in place. Guideline compliance for drug selection was found in 75.8% of cases, 73.6% for dosing, 70.8% for duration of therapy, and 70.5% for all 3 components of the treatment guidelines (full guideline compliance). ID consultation increased the likelihood of full guideline compliance (84.2% vs 59.5%, p < 0.0001).
Treatment Course, Guideline Compliance, and Catheter Care a
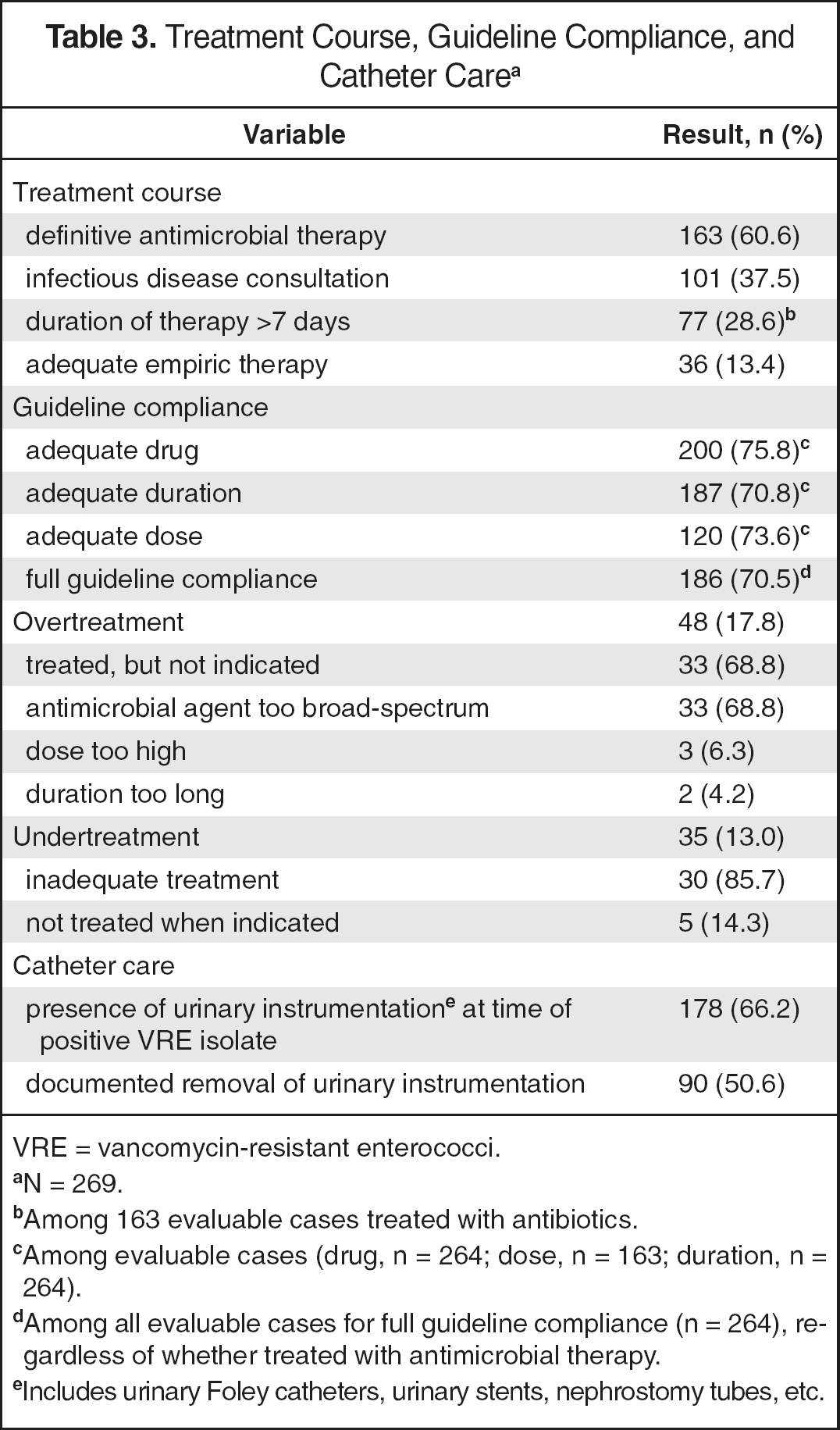
VRE = vancomycin-resistant enterococci.
N = 269.
Among 163 evaluable cases treated with antibiotics.
Among evaluable cases (drug, n = 264; dose, n = 163; duration, n = 264).
Among all evaluable cases for full guideline compliance (n = 264), regardless of whether treated with antimicrobial therapy.
Includes urinary Foley catheters, urinary stents, nephrostomy tubes, etc.
Empiric and Definitive Antimicrobial Therapy Selection a
VRE = vancomycin-resistant enterococci.
N = 269.
There were more antimicrobial agents (253) than patients receiving empiric antimicrobial therapy (217), since many patients received combination therapy, including an agent targeting gram-positive pathogens and an agent targeting gram-negative pathogens (eg, cefepime plus vancomycin).
Trimethoprim/sulfamethoxazole, 3; fosfomycin, 2; nitrofurantoin, 1; doxycycline, 1.
Forty-eight (17.8%) urinary VRE isolates were overtreated, mostly because of administration of antimicrobial therapy when not indicated (Table 3). Among 155 asymptomatic patients who did not require antimicrobial therapy, 33 (21.3%) received treatment, with a mean duration of 7.2 days (range 1–16). Antibiotics prescribed for asymptomatic patients included linezolid (n = 21, 170 days), daptomycin (n = 10, 55 days), doxycycline (n = 1, 7 days), and fosfomycin (n = 2, 2 doses). In 33 cases, antimicrobial therapy was considered too broad (ie, using linezolid or daptomycin for VRE cystitis susceptible to nitrofurantoin, fosfomycin, or doxycycline). Finally, there were 3 cases in which the antibiotic dose was deemed too high (ie, daptomycin 6 mg/kg for cystitis without evidence of bacteremia) and 2 cases in which the duration was deemed too long.
Thirty-five (13.0%) patients were undertreated, including 23 who received antimicrobial treatment that lacked activity against VRE (ceftriaxone, n = 13; ciprofloxacin, n = 5; levofloxacin, n = 2; vancomycin, n = 2; nitrofurantoin, n = 1), 5 who did not receive treatment when indicated, 4 with inadequate duration of therapy, 2 with inadequate daptomycin dosing for bacteremic UTIs, and 1 with pyelonephritis case with fosfomycin.
Among evaluable cases (n = 156), 68 (43.6%), 53 (34.0%), 48 (30.8%), and 32 (20.5%) resulted in the composite end point of clinical failure, treatment failure, microbiologic failure, and 30-day all-cause mortality, respectively. Clinical failure was more common among evaluable patients who were undertreated compared to those who received adequate definitive therapy (15 of 23 vs 54 of 133, p = 0.04). Among all 269 cases, complications were common, including 30- day all-cause mortality (46, 17.1%), recurrent VRE-associated UTI (55, 20.4%), readmission for UTI (18, 6.7%), development of a multidrug-resistant pathogen (5, 1.9%), C. difficile colitis (2, 0.07%), or documented adverse drug event (1, 0.04%). Some patients had more than 1 complication.
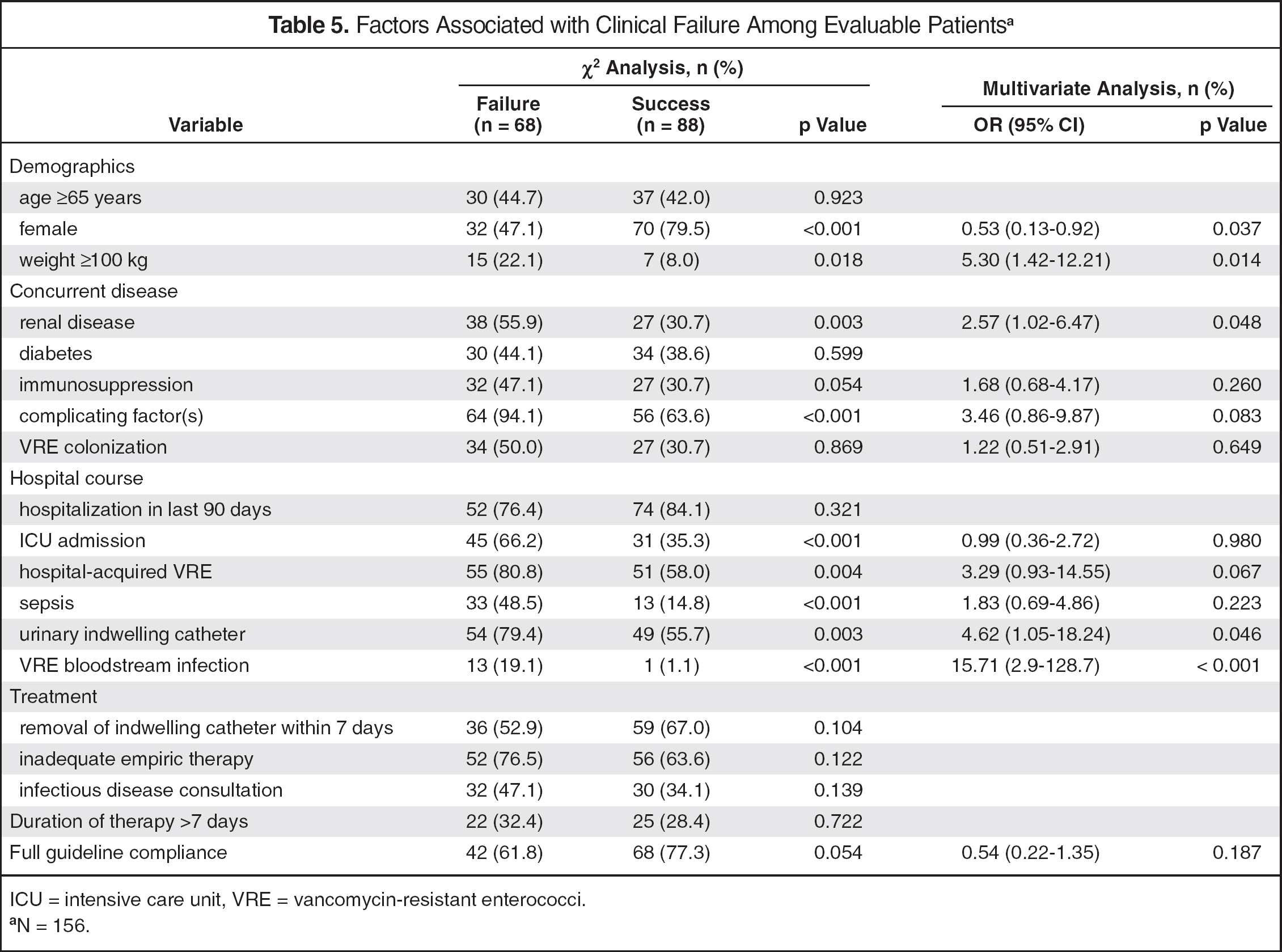
Weight 100 kg or more (p = 0.018), renal disease (p = 0.003), complicating factors (p < 0.001), ICU admission (p < 0.001), sepsis (p < 0.001), urinary indwelling catheters (p = 0.003), and VRE bloodstream infections (p < 0.001) were more common among patients who failed therapy (Table 5). Factors independently associated with clinical failure upon multivariate analysis included weight 100 kg or more (OR 5.30; p = 0.014), renal disease (OR 2.57; p = 0.048), indwelling catheter (OR 4.62; p = 0.046), and VRE bloodstream infection (OR 15.71; p < 0.001) (Table 5). Female sex was found to be protective of clinical failure upon multivariate analysis (OR 0.53; p = 0.037).
Factors Associated with Clinical Failure Among Evaluable Patients a
ICU = intensive care unit, VRE = vancomycin-resistant enterococci.
N = 156.
Discussion
We conducted a retrospective analysis of EMRs to characterize the diagnosis and management of VRE from a urinary source at a large academic medical center. Among evaluable patients, full compliance with the institutional VRE-associated UTI guidelines, including drug, dose, and duration was over 70%. However, on closer analysis of cases found to be noncompliant with the treatment guidelines, 58% were overtreated and 42% were undertreated (18% and 13% among all patients, respectively). Overtreatment and undertreatment of UTIs and/or bacteriuria are problems that have been reported elsewhere. A recent retrospective study reported clinical outcomes of enterococcal bacteriuria and UTI. 26 The investigators found that approximately one third of all asymptomatic bacteriuria cases were inappropriately treated with antibiotics, while about 15% of all UTI cases were inappropriately undertreated; these findings are similar to ours.
Most overtreated cases received linezolid or daptomycin when treatment was not indicated, resulting in more than 200 days of excess antimicrobial treatment and approximately $50,000 in unnecessary antimicrobial-related costs (inpatient acquisition drug costs) over the 3-year study period. This unnecessarily exposes patients to broad-spectrum antibiotics, resulting in increased hospital expenditures and increased risk of antimicrobial resistance.
Most undertreated cases received antimicrobial therapy without activity against VRE. With the exception of one nitrofurantoin-resistant case, these patients received antibiotics against which VRE was inherently resistant, such as cephalosporins. Inadequate treatment had a negative impact on patient outcomes, since undertreated cases were more likely to experience clinical failure than were those who were adequately treated. This finding provides an important opportunity for antimicrobial stewardship as it highlights the need for improved clinician education regarding VRE treatment options, antimicrobial dosing, and adequate duration of therapy.
ID consultation improved the likelihood of guideline compliance, emphasizing the value of consulting with these specialists. However, unexpectedly, ID consultation did not affect patient outcomes. This is likely because these specialists were more likely to be consulted for patients at higher risk with factors associated with clinical failure, including urosepsis and VRE bacteremia. Overall, it is important to treat documented VRE-associated UTIs appropriately, especially because our study found high rates of urosepsis and poor patient outcomes, including mortality. However, it is controversial whether VRE is independently predictive of mortality or only associated with mortality and a marker of prolonged hospitalization and severity of illness. 27 –29
In the multivariate analysis, we found indwelling catheter placement, VRE bloodstream infections, renal disease, and weight 100 kg or more to be independently associated with clinical failure. Indwelling catheters are a well-documented risk factor for VRE-associated UTIs. 17 They facilitate ascension of pathogens to the bladder and can introduce bacteria into the bladder either during insertion and/or through bacterial adhesion to the catheter and subsequent biofilm development. 9 The Infectious Diseases Society of America recommends several prevention strategies to reduce the incidence of catheter-associated UTIs, including that urinary catheters be placed only when clearly indicated and that they are removed as soon as they are no longer required. 9 Furthermore, our study identified VRE bacteremia as a risk factor for clinical failure. Several other reports have also found VRE bacteremia to be an independent risk factor for mortality and increased length of stay. 30 Specifically, vancomycin-resistant E. faecium has been associated with worse patient outcomes and mortality when compared to vancomycin-resistant E. faecalis, presumably because of higher virulence and less optimal antimicrobial therapies available. 31,32 Increased mortality among patients with VRE bacteremia is thought to occur mainly due to higher severity of illness, which may include immunosuppression, allogenic bone marrow transplantation, and septic shock. 32 –34 Therefore, it is important to prevent nosocomial VRE transmission and infection in patients with risk factors for VRE colonization. Renal disease, particularly when end stage in patients receiving dialysis, has also been reported to increase the risk for colonization and infection with VRE. 3 However, our definition of renal disease did not differentiate between patients with acute kidney injury and those with chronic kidney disease.
As previously mentioned, weight 100 kg or more was associated with clinical failure in our study. In general, obesity has been linked to numerous complications including a proinflammatory state, impaired immune response, altered composition of commensal gut bacteria, and increased severity of certain respiratory infections. 35 Our findings also raise the possibility of suboptimal antimicrobial dosing in obese patients. Published reports on antimicrobial dosing in obese patients are scarce and largely based on case series and anecdotal reports. 36 For example, although linezolid has been shown to achieve adequate urinary concentrations for uncomplicated gram-positive UTIs, despite primarily nonrenal clearance, it is unclear whether linezolid in a fixed-dose regimen achieves adequate urinary concentrations among morbidly obese patients with complicated VRE-associated UTIs. 37 Daptomycin dosing is weight-based; however, recent evidence suggests that higher daptomycin minimum inhibitory concentrations for enterococci may warrant higher doses (eg, 8 mg/kg/day or more). 38,39 Our treatment algorithm considered daptomycin doses of 6 mg/kg/day or higher as appropriate for VRE bacteremic UTIs. However, although higher daptomycin doses have been demonstrated to be safe, it has yet to be determined whether they lead to improved patient outcomes compared to the currently approved dosing recommendations. Overall, further research evaluating optimal dosing in obese patients is needed, especially among those with more complicated infections.
Inadequate empiric therapy was not associated with clinical failure. Since few (13.7%) patients received empiric therapy against VRE, our study was likely underpowered to detect a difference. However, it has been reported that empiric administration of antimicrobial therapy against VRE did not improve patient outcomes when compared to patients who had a 72-hour or greater delay in receiving VRE active antimicrobial therapy. 33 We also found that full compliance with the guideline had no significant effect on the rates of clinical failure. This may be related to the fact that noncompliance with the VRE-associated UTI guidelines included cases of overtreatment that was not associated with clinical failure. Furthermore, because of the lack of evidence-based data supporting our institutional guidelines, it is possible that noncompliance with the guidelines may not have been inappropriate for certain cases. However, as previously noted, undertreatment was associated with clinical failure. Finally, we found female sex to be protective against clinical failure, likely because of the complicated nature of UTIs associated with male sex, such as more frequent instrumentation, structural abnormalities, and anatomic differences. 2,8,11
The results of this study provide several opportunities to improve management of VRE-associated UTIs at our institution. Overtreatment and undertreatment of these infections resulted in unnecessary health care expenditures and higher clinical failure rates, respectively. Consequently, antimicrobial stewardship programs may benefit from targeting patients with VRE from urinary sources to improve patient outcomes, optimize antimicrobial therapy, decrease costs, and provide clinician education. Additionally, risk factors associated with clinical failure can be used to risk stratify VRE-associated UTIs. We plan to modify our guidelines to include more recommendations on diagnostic criteria and risk stratification. For example, patients who are obese or have evidence of complicating factors (male sex, urinary hardware placement) may require closer monitoring and/or more aggressive antimicrobial therapy. The high mortality and clinical failure rates associated with VRE bloodstream infections suggest the benefit of a separate VRE bloodstream infection algorithm and/or consideration of ID consultation. Finally, we found that a large proportion of isolates were not tested for susceptibilities to less-expensive antimicrobial agents with intrinsic activity against VRE suitable for treatment of VRE cystitis (eg, nitrofurantoin, doxycycline/minocycline, and fosfomycin). It may be beneficial to report these susceptibilities among patients with VRE from urinary sources to better reserve broad-spectrum antibiotics (eg, daptomycin and linezolid); however, clinical judgment is still needed when interpreting reported susceptibilities, since these agents should be reserved for VRE cystitis. 2
There are several limitations to this study. The retrospective design impaired our ability to state causation and may introduce bias and confounding variables. Patients with urinary VRE isolates identified at an outside institution were not included in the study, unless they had a repeat urinary VRE isolate while receiving care at our institution. Further, because of the retrospective design, it was difficult to ascertain whether the urine cultures positive for VRE were performed because of concern for a UTI or as an infection control measure. The identification and classification of UTI cases and presence of complicating factors, such as instrumentation, relied on the thoroughness of physicians' and nurses' documentation in the EMR. Our institutional guidelines, while previously published, have not been validated and may not be generalizable to other institutions. Thus, it is possible that noncompliance with our institutional guidelines may not be inappropriate for all cases. Furthermore, many cases were lost to follow-up and outcomes were not available, since patients could have received care outside of our institution. Thus, it is possible that cases of treatment/microbiologic/clinical failure may be overreported because patients with more complicated cases were more likely to remain hospitalized or require further follow-up care, whereas the healthier patients with less-complicated illness were less likely to need further care. Severity of illness scoring (eg, Charlson Comorbidity Index, Simplified Acute Physiology score, or Mortality Probability Model score) to assess baseline risk for mortality were not tabulated because of the inability to completely and accurately tabulate such scores with the retrospective design of the study. Assessment of other possible or confirmed infections was not accounted for other than documentation of other pathogens identified from urinary isolates and evaluation of multidrug resistance. Infection-related mortality was not evaluated because, as another limitation of the retrospective design, we were unable to determine the cause of death in many cases.
Finally, analysis of comprehensive costs associated with inappropriate management of VRE-associated UTIs, including excessive antimicrobial use or complications from clinical failure, were beyond the scope of this study.
In conclusion, new antimicrobial stewardship opportunities, including improved clinician education and awareness, are needed to minimize cases of VRE overtreatment and undertreatment and associated health care expenditures at our institution. Risk factors for clinical failure were identified, including obesity, renal disease, urinary hardware and VRE bloodstream infections. Updated institutional VRE-associated UTI treatment guidelines with an emphasis on appropriate diagnosis and risk stratification may be useful to help guide future treatment decisions.