
Abstract
OBJECTIVE
To evaluate the efficacy, safety, and clinical utility of the combination product azilsartan medoxomil/chlorthalidone for the treatment of hypertension.
DATA SOURCES
Articles indexed in PubMed through December 2012 were identified using the MeSH terms azilsartan and chlorthalidone, Edarbyclor, TAK-490, and Edarbi. Additional information was gathered from references cited in the identified publications, the package insert, and from a review of the ClinicalTrials.gov registry.
STUDY SELECTION AND DATA EXTRACTION
English-language articles, including clinical trials and reviews involving azilsartan medoxomil/chlorthalidone or each component individually for the treatment of hypertension were reviewed.
DATA SYNTHESIS
The antihypertensive combination tablet azilsartan medoxomil/chlorthalidone is the first to combine an inhibitor of the renin-angiotensin-aldosterone system with chlorthalidone, a thiazide-type diuretic. In 4 randomized controlled trials (3 published to date), azilsartan medoxomil/chlorthalidone 40 mg/12.5 mg and 40 mg/25 mg reduced blood pressure (BP) significantly more than comparators did, including an approximately 5-mm Hg greater BP reduction than olmesartan medoxomil/hydrochlorothiazide 40 mg/25 mg and azilsartan medoxomil/hydrochlorothiazide. Reductions in 24-hour ambulatory BP and clinic BP were observed, and a greater proportion of patients achieved BP targets while receiving azilsartan medoxomil/chlorthalidone. Azilsartan medoxomil/chlorthalidone was generally well tolerated, with minor, transient increases in serum creatinine and without a significant effect on potassium homeostasis. No studies have directly examined cardiovascular morbidity and mortality benefits associated with this combination.
CONCLUSIONS
The combination of azilsartan medoxomil/chlorthalidone has demonstrated safety and efficacy in lowering BP in hypertensive patients to a greater degree than olmesartan medoxomil/hydrochlorothiazide and azilsartan medoxomil/hydrochlorothiazide. As a fixed-dose combination tablet, it offers several clinical advantages.
The prevalence of uncontrolled hypertension remains unacceptable despite efforts to increase awareness, treatment, and control of blood pressure (BP). Population-based surveys indicate that only 66% of patients treated for hypertension achieve BP control of less than 140/90 mm Hg. 1 Most hypertensive patients require 2 or more medications to adequately control BP. 2–5 Combination therapy potentiates BP-lowering by complementary mechanisms of action and leads to higher response rates compared with monotherapy.
In December 2011, the US Food and Drug Administration (FDA) approved a new fixed-dose combination antihypertensive medication for patients with an inadequate response to monotherapy or those in whom multiple drugs are required to achieve BP control. The new product combines an angiotensin receptor blocker (ARB), azilsartan medoxomil and a thiazide-type diuretic, chlorthalidone, and is marketed as Edarbyclor. Azilsartan medoxomil is the only ARB approved in a fixed-dose tablet with chlorthalidone; all other ARB combinations include hydrochlorothiazide as the diuretic component. This literature review examines the pharmacology and pharmacokinetics of azilsartan medoxomil/chlorthalidone, outlines efficacy and safety data, and provides an overview of dosing and cost considerations.
Data Sources
A literature search of PubMed and ClinicalTrials.gov was performed to identify reports on clinical trials and abstracts published through December 2012, using the search terms azilsartan medoxomil, chlorthalidone, hypertension, and blood pressure. References from the bibliographies of selected sources and the product monograph were reviewed to supplement clinical data.
Pharmacology
AZILSARTAN MEDOXOMIL
Prior to drug absorption within the gastrointestinal tract, the prodrug azilsartan medoxomil undergoes ester hydrolysis into the bioactive azilsartan moiety. 6 Azilsartan inhibits vasoconstrictive and aldosterone-secreting actions of angiotensin II through selective antagonism of the angiotensin type 1 (AT1) receptor in vascular smooth muscle and endocrine gland tissues. 6–8 Azilsartan exhibits a more than 10,000-fold greater affinity for the AT1 receptor than for the AT2 receptor. 9 Data from in vitro studies show that azilsartan has superior AT1 binding affinity and slower dissociation than olmesartan, telmisartan, valsartan, and irbesartan. 10 These advantageous properties contribute to the potent and long-lasting antihypertensive activity of azilsartan.
CHLORTHALIDONE
Chlorthalidone is a thiazide-type diuretic that differs chemically from traditional thiazides (eg, hydrochlorothiazide) by its lack of a benzothiadiazine molecular structure. 6 Diuresis occurs subsequent to inhibition of sodium and chloride reabsorption at the cortical diluting segment of the ascending loop of Henle. 6 Natriuretic effects begin approximately 2.6 hours after drug administration and can be sustained for 48–72 hours. 6 Acutely, diuretics expand urine volume, thereby decreasing extracellular fluid and plasma volume. 11 Volume loss reduces venous return, cardiac output, and BP. 11 Thiazide diuretics also activate counterregulatory systems, such as the renin-angiotensin-aldosterone system (RAAS) and the sympathetic nervous system, to restore BP. 11,12 Over time, thiazide-type diuretics promote BP lowering by decreasing total peripheral resistance (TPR) 11–13 ; however, the exact mechanism behind TPR reduction has not been elucidated. Patients with metabolic syndrome or those who exhibit low-renin hypertension (eg, blacks, the elderly, patients with diabetes mellitus) respond favorably to BP lowering with a thiazide-type diuretic. 14
Pharmacokinetics
The pharmacokinetic parameters of azilsartan medoxomil and chlorthalidone (Table 1) do not differ appreciably in the combination tablet with the exception of chlorthalidone peak plasma concentration, which is 47% higher in the combined product. 6,15 The clinical significance of this increase is unknown.
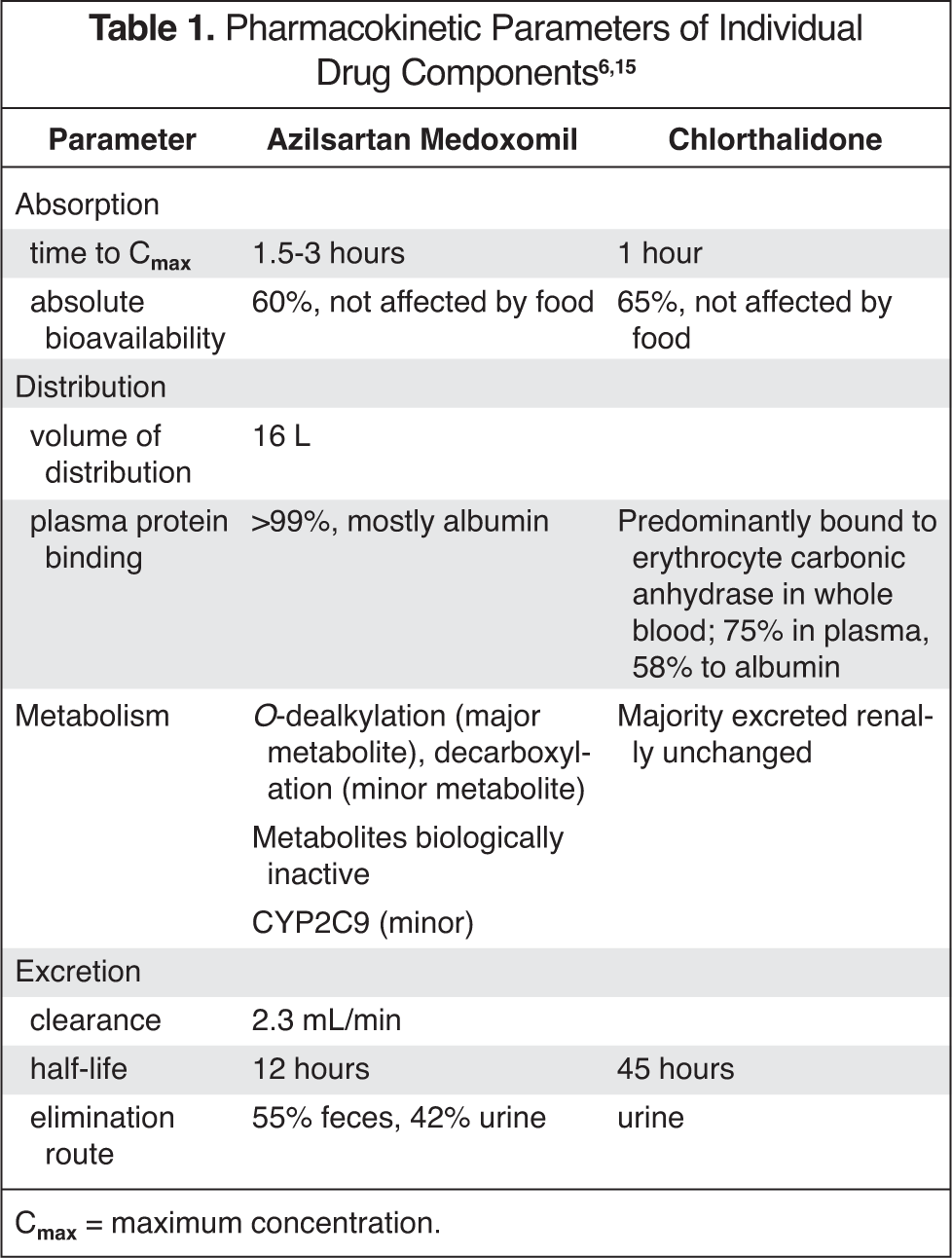
Cmax = maximum concentration.
Clinical Trials
AZILSARTAN MEDOXOMIL VERSUS OTHER ANTIHYPERTENSIVE MEDICATIONS
Clinical guidelines suggest ARBs as a first-line treatment option for hypertensive patients with compelling indications, including heart failure, left ventricular hypertrophy, chronic kidney disease, history of myocardial infarction (MI), and diabetes. 16,17 The results of clinical trials comparing azilsartan medoxomil with other antihypertensive medications are summarized in Table 2. 18–22
Clinical Trials of Azilsartan Medoxomil
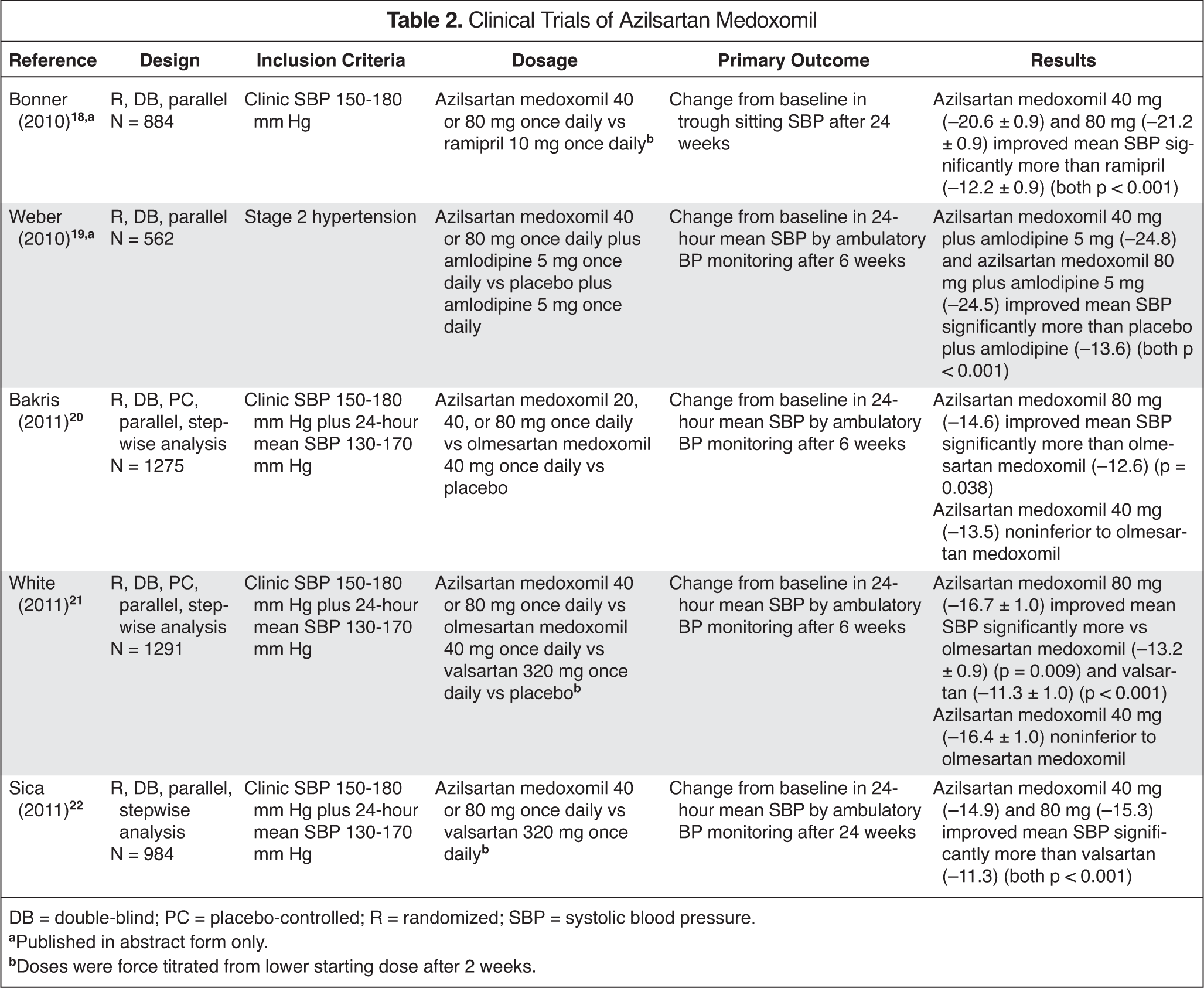
DB = double-blind; PC = placebo-controlled; R = randomized; SBP = systolic blood pressure.
Published in abstract form only.
Doses were force titrated from lower starting dose after 2 weeks.
CHLORTHALIDONE VERSUS HYDROCHLOROTHIAZIDE
Guidelines recommend thiazide diuretics as initial therapy for most patients with hypertension, and if patients require more than 1 drug to effectively control BP, 1 agent should be a diuretic. 16 Chlorthalidone is approximately 1.5–2 times as potent as hydrochlorothiazide at equivalent doses (ie, 12.5 mg of chlorthalidone is roughly equal to 18.75–25 mg of hydrochlorothiazide). 15 Further, hydrochlorothiazide has a shorter duration of action than does chlorthalidone (12–24 hours vs 24–72 hours). 15 It is unclear whether these pharmacodynamic and pharmacokinetic differences translate to differential effects on clinical outcomes. No prospective, head-to-head, randomized controlled trials (RCTs) of chlorthalidone and hydrochlorothiazide have compared differences in cardiovascular events between the 2 diuretics.
A recent systematic review of RCTs revealed that chlorthalidone reduced cardiovascular events by 21% relative to hydrochlorothiazide (p < 0.0001). 23 The effect of either diuretic on cardiovascular events was strongly correlated to each drug's antihypertensive effects. 23 For any given difference in mean achieved office systolic BP (SBP), however, the risk for cardiovascular events was lower for chlorthalidone than for hydrochlorothiazide (RR 0.82; p = 0.024). 23
Results from studies with cardiovascular end points have suggested that chlorthalidone and hydrochlorothiazide are not interchangeable. An observational cohort analysis (MRFIT [Multiple Risk Factor Intervention Trial]) of 8102 men with hypertension and at high risk for coronary heart disease (CHD) was the first study to suggest superiority of chlorthalidone over hydrochlorothiazide. 24 Participants were assigned to special intervention comprising hypertension treatment, smoking cessation counseling, and dietary guidance versus usual care. 24 Step 1 of the special intervention hypertension treatment consisted of chlorthalidone or hydrochlorothiazide 50–100 mg daily; the MRFIT staff at each clinical center determined drug selection. 24 For the first 6 years of the study, CHD mortality rates for the 9 sites predominantly prescribing hydrochlorothiazide were 44.1% higher for special intervention versus usual care (p = 0.23), whereas CHD mortality rates for the 6 sites primarily using chlorthalidone were 58.2% lower for special intervention. 24 The MRFIT advisory board thereafter changed the treatment protocol by recommending chlorthalidone (maximum 50 mg daily) over hydrochlorothiazide. 24 The protocol change was associated with improvements in CHD mortality (p = 0.04) and all-cause mortality (p = 0.06) for the 9 sites originally prescribing hydrochlorothiazide. 24
A retrospective observational cohort analysis of the MRFIT data discovered that cardiovascular events were 21% lower for chlorthalidone- versus hydrochlorothiazide-treated patients after a median follow-up period of 6 years (p = 0.0016). 25 Decreases in clinical MI, coronary artery bypass surgery, angina determined by Rose questionnaire, and peripheral artery occlusive disease accounted primarily for this difference. 25 Additionally, the chlorthalidone group had significantly lower BP (p < 0.0001), total cholesterol (p < 0.0001), and low-density lipoprotein cholesterol (LDL-C) (p = 0.0009) measurements compared with the hydrochlorothiazide group. 25
The SHEP (Systolic Hypertension in the Elderly Program) trial studied 4376 elderly (aged >60 years) patients with isolated systolic hypertension (SBP >160 mm Hg and diastolic BP [DBP] <90 mm Hg) assigned to receive active drug versus placebo. 26 Patients in the treatment group initially received chlorthalidone 12.5 mg, which was increased to 25 mg if the SBP goal was not achieved at follow-up visits. Almost half (46%) of the patients received chlorthalidone and no additional BP medications. Mean SBP levels were 11–14 mm Hg lower in the chlorthalidone-treated patients than in the placebo group. Over a mean follow-up period of 4.5 years, chlorthalidone-based therapy prevented approximately 1 of 2 incident cases of left ventricular failure (RR 0.46; 95% CI 0.33–0.65), 1 of 3 total strokes (RR 0.64; 95% CI 0.50–0.82; p = 0.0003), and 1 of 4 CHD events (RR 0.75; 95% CI 0.60–0.94) relative to placebo-based treatment. These differences were detected even though 35% of patients assigned to placebo took antihypertensive medications. 26
Although the original SHEP trial did not indicate a significant mortality benefit, 26 a 22-year follow-up of SHEP patients, using data from the National Death Index, showed improved long-term survival with chlorthalidone. 27 Patients lived approximately 1 day extra, free from cardiovascular death, for each month that they were treated with chlorthalidone versus placebo (RR 0.89; 95% CI 0.20–1.62). 27 However, information regarding drugs used in antihypertensive therapy after study termination was not available.
COMBINATION THERAPY VERSUS MONOTHERAPY
Combination therapy offers several advantages over monotherapy for BP control. Combining antihypertensives with additive mechanisms provides a greater degree of BP lowering. 28,29 A meta-analysis by Wald et al. found that combining drugs from 2 different classes yields an approximately 5-fold greater BP-lowering effect than doubling the dose of a single agent. 29 Two agents used concomitantly at lower doses may provide the same or greater level of BP lowering as a higher dose of 1 medication. Lower doses lead to fewer dose-dependent adverse effects and improved tolerability. 28,30 Initial combination therapy versus initial monotherapy reduces the time to reach target BP. Mounting evidence suggests that achieving prompt BP control confers long-term end point reduction (ie, risk of cardiac events, stroke, mortality). 31
Polypharmacy predicts poor medication adherence. 32 A fixed-dose combination of antihypertensive medications in a single pill presents an attractive alternative to multiple tablets of the separate drug components. Simplifying an antihypertensive dosing regimen and reducing pill burden significantly increases patient adherence. 32,33 A meta-analysis demonstrated that fixed-dose combinations decreased medication nonadherence to antihypertensive therapy by 21% (95% CI 1.03–1.43; p = 0.02) and improved persistence in therapy, although not significantly, by 54% (95% CI 0.95–2.49; p = 0.08) compared with the corresponding separate drug components given in separate tablets. 33
AZILSARTAN MEDOXOMIL/CHLORTHALIDONE COMBINATION THERAPY
Sica et al. performed a double-blind, factorial RCT to compare the antihypertensive efficacy of azilsartan medoxomil/chlorthalidone versus azilsartan medoxomil or chlorthalidone monotherapy in 1714 patients with stage 2 hypertension (clinic SBP ≥160 and ≤190 mm Hg) over an 8-week period. 34 Azilsartan medoxomil/chlorthalidone 40 mg/25 mg and 40 mg/12.5 mg significantly outperformed their comparative monotherapy components in lowering trough SBP by ambulatory BP monitoring (primary end point) and clinic measurement (secondary end point) (Figure 1). 34 Reductions in trough BP with ambulatory monitoring for the combination products were nearly additive, relative to the respective monotherapy components. 34 Reductions in trough SBP for ambulatory monitoring and clinic measurements were dose-related. 34
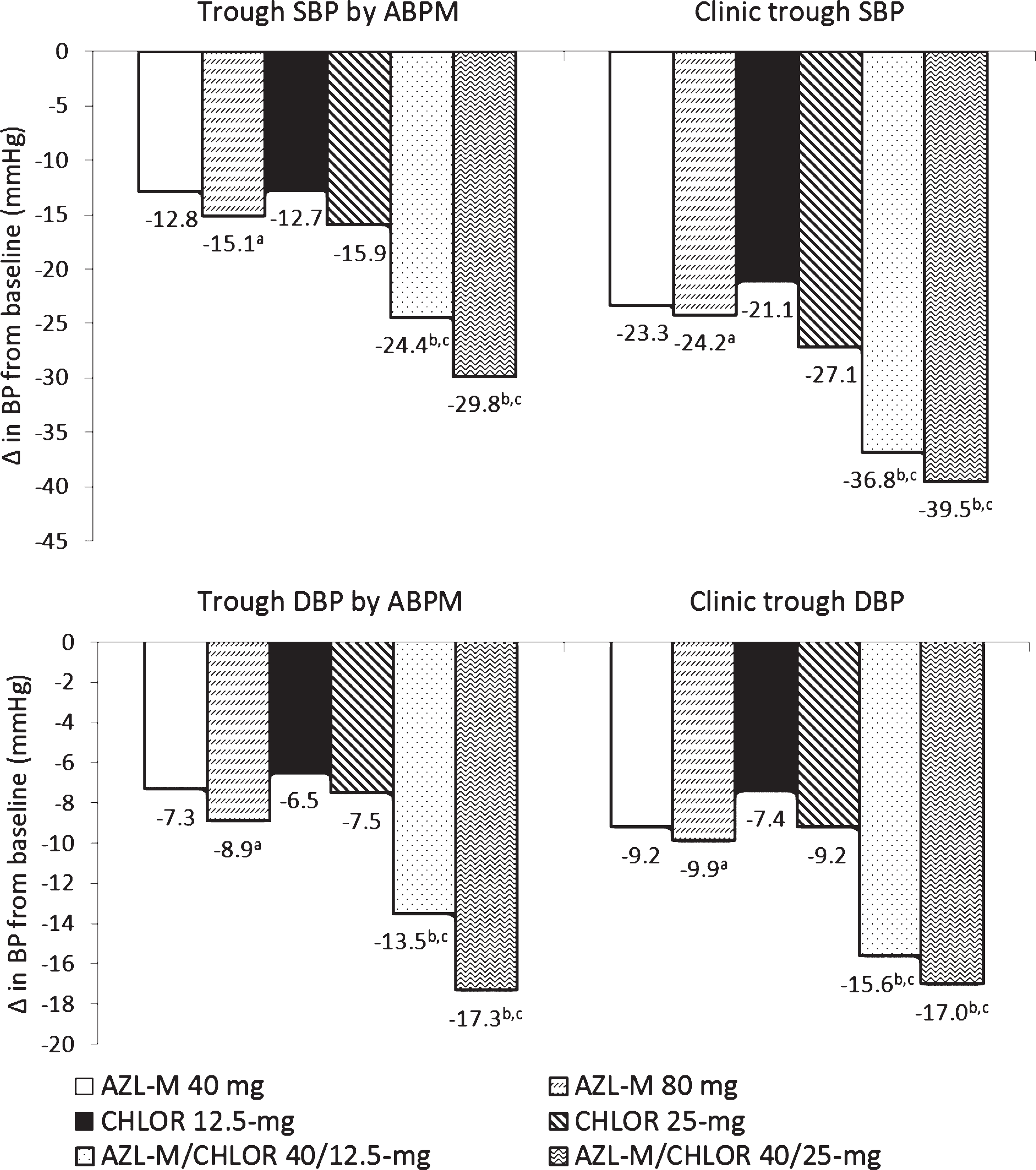
Blood pressure reductions from baseline after 8 weeks of treatment, stratified by treatment group. 34 ABPM = ambulatory blood pressure monitoring; AZL-M = azilsartan medoxomil; BP = blood pressure; CHLOR = chlorthalidone; DBP = diastolic blood pressure; SBP = systolic blood pressure.
A second RCT, conducted in 1071 patients with stage 2 hypertension, evaluated efficacy differences between azilsartan medoxomil/chlorthalidone and the highest available dose of olmesartan medoxomil/hydrochlorothiazide. 35 Treatment with azilsartan medoxomil/chlorthalidone 40 mg/25 mg reduced the primary end point, trough clinic SBP approximately 24 hours after dosing, by 5.3 mm Hg (95% CI −7.6 to −3.1 mm Hg; p < 0.001) more than olmesartan medoxomil/hydrochlorothiazide 40 mg/25 mg at the end of 12 weeks (Figure 2). 35 Reductions in trough DBP (−2.3 mm Hg; 95% CI −3.6 to −1.0 mm Hg), 24-hour mean SBP by ambulatory BP monitoring (−6.4 mm Hg; 95% CI −8.5 to −4.3 mm Hg), and 24-hour mean DBP by ambulatory BP monitoring (−3.2 mm Hg; 95% CI −4.5 to −2.0) with azilsartan medoxomil/chlorthalidone were also superior to reductions achieved with olmesartan medoxomil/hydrochlorothiazide (p < 0.001 for all comparisons). 35 A larger percentage of patients receiving azilsartan medoxomil/chlorthalidone 40 mg/25 mg than olmesartan medoxomil/hydrochlorothiazide 40 mg/25 mg patients reached target BP of less than 140/90 mm Hg (81.4% vs 74.6%; p < 0.05) or less than 130/80 mm Hg (56.1% vs 41.0%; p < 0.05). 35 Therapeutically nonequivalent chlorthalidone and hydrochlorothiazide doses limit the ability to effectively compare azilsartan medoxomil/chlorthalidone 40 mg/25 mg and olmesartan medoxomil/hydrochlorothiazide 40 mg/25 mg, and data may favor azilsartan medoxomil/chlorthalidone for this reason. However, hydrochlorothiazide is not formulated in combination with olmesartan medoxomil in doses larger than 25 mg.
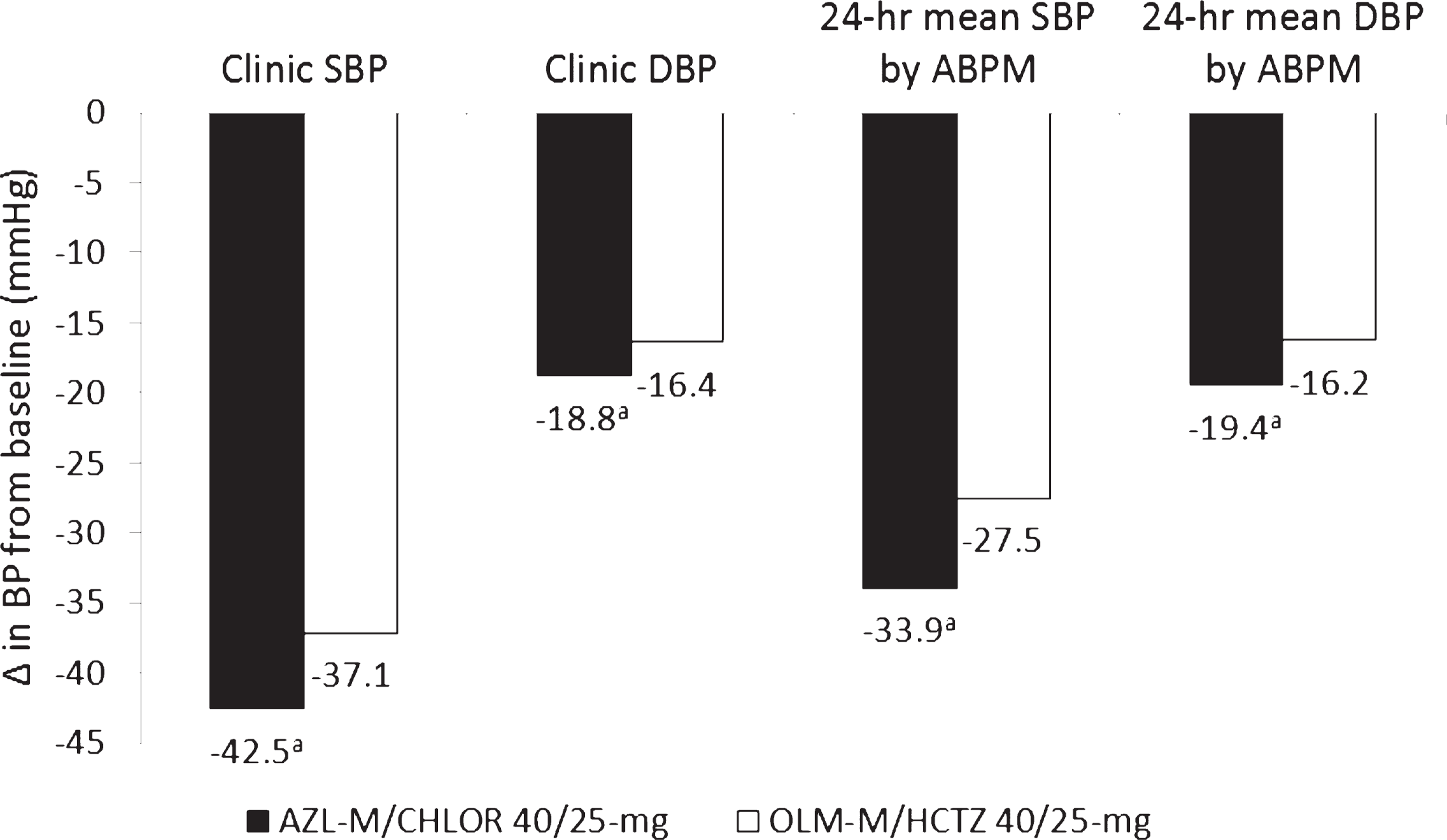
Absolute blood pressure reductions from baseline after 12 weeks of treatment. 35 ABPM = ambulatory blood pressure monitoring; AZL-M = azilsartan medoxomil; BP = blood pressure; CHLOR = chlorthalidone; DBP = diastolic blood pressure; HCTZ = hydrochlorothiazide; OLM-M = olmesartan medoxomil; SBP = systolic blood pressure.
In a study comparing different thiazide diuretics in combination with azilsartan medoxomil, 609 patients with mean clinic SBP of 160–190 mm Hg started azilsartan medoxomil 40 mg, with forced addition of chlorthalidone 12.5 mg or hydrochlorothiazide 12.5 mg at week 2. 36 After 6 total weeks of treatment, a dose doubling of the thiazide component was permitted if BP remained above target. 36 Predictably, fewer patients required titration to higher doses of azilsartan medoxomil/chlorthalidone than did those receiving azilsartan medoxomil/hydrochlorothiazide (30.8% vs 45.9%; p < 0.001). 36 Regardless of diuretic dose, seated trough SBP and 24-hour mean SBP measured in the clinic after 10 weeks of treatment responded significantly better to azilsartan medoxomil/chlorthalidone than to azilsartan medoxomil/hydrochlorothiazide (clinic BP −37.8 vs −32.8 mm Hg; 24-hour mean BP −26.6 vs −22.4 mm Hg; p < 0.001 for all comparisons). 36
Nighttime BP better predicts cardiovascular risk than 24-hour ambulatory BP, and ambulatory BP better predicts risk than office BP. 37,38 Greater reductions for azilsartan medoxomil/chlorthalidone combination therapy were consistently observed throughout the 24-hour interval, including overnight. 34,35 An additional study revealed a greater change in nighttime (12 am to 6 am) mean SBP with azilsartan medoxomil/chlorthalidone 40 mg/25 mg than with chlorthalidone 25-mg monotherapy (mean difference −12.93 mm Hg; p < 0.001). 39
No clinical trials to date have assessed clinical outcomes data for azilsartan medoxomil/chlorthalidone. However, it is well established that lowering BP reduces cardiovascular disease events, including MI, heart failure, stroke, and kidney disease, independently of other risk factors. 16 In individuals aged 40–69 years, vascular mortality risk increases 2-fold for every 20-mm Hg increase in SBP above 115 mm Hg, up to 185 mm Hg. 40 The superior BP lowering demonstrated in clinical trials with azilsartan medoxomil/chlorthalidone then may translate into benefits in cardiovascular outcomes. The ACCOMPLISH (Avoiding Cardiovascular Events Through Combination Therapy in Patients Living with Systolic Hypertension) trial challenged combination therapy with an RAAS inhibitor and hydrochlorothiazide. 41 Benazepril plus amlodipine more effectively prevented a combination of cardiovascular morbidity and mortality than did benazepril and hydrochlorothiazide combined (9.6% vs 11.8%; HR 0.80; 95% CI 0.72–0.90) 41 ; it remains questionable whether these results extend to chlorthalidone.
Safety and Tolerability
DOSING AND ADMINISTRATION
The combination tablet of azilsartan medoxomil and chlorthalidone earned FDA approval for the treatment of hypertension. Takeda Pharmaceuticals, Inc. manufactures azilsartan medoxomil/chlorthalidone (Edarbyclor) in 40-mg/12.5-mg and 40-mg/25-mg tablets. 6 The manufacturer suggests a starting dose of 40 mg/12.5 mg once daily and a dosage adjustment to the higher strength if BP goals are not achieved after 2–4 weeks. 6 Although azilsartan medoxomil alone may be dosed up to 80 mg daily, azilsartan medoxomil/chlorthalidone 80 mg/25 mg is not recommended; more patients taking this dose experienced an adverse event leading to permanent drug discontinuation (eg, dizziness, hypotension, serum creatinine [SCr] elevations). 34,35
Doses can be administered without regard to meals. 6 Azilsartan medoxomil/chlorthalidone must be dispensed and stored in its original container to avoid moisture-related degradation 6 ; this may lower adherence for patients who prefer to store their medications in pillboxes.
USE IN SPECIFIC POPULATIONS
The BP trials of azilsartan medoxomil/chlorthalidone published to date were conducted in a predominantly (70–80%) white population, with a mean age of 57 years, without serious comorbidities. 34–36 Patients with poorly controlled diabetes (hemoglobin A1c >8.0%) were excluded from each study, and only 11–17% of the study populations had diabetes. 34–36 The magnitude of BP reductions was similar for black patients and the overall study populations. 34–36 Subgroup analyses failed to demonstrate differential responses dependent on race (p > 0.1). 34–36
Patients with mild-moderate renal or hepatic impairment do not require a dose adjustment of azilsartan medoxomil/chlorthalidone. 6 Safety and efficacy have not been formally established through clinical testing in patients with severe renal (estimated glomerular filtration rate <30 mL/min/1.73 m2) or hepatic impairment. Chlorthalidone is considered ineffective when creatinine clearance is less than 30 mL/min/1.73 m2.
No dosage adjustment is necessary for geriatric patients. Nearly a quarter of patients treated in clinical trials with azilsartan medoxomil/chlorthalidone were aged 65 years or older, and 5.7% were aged 75 years or older. The medication was not studied in patients younger than 18 years. 6
Azilsartan medoxomil/chlorthalidone is pregnancy category D owing to deleterious effects on fetal renal function and the risk for fetal and neonatal morbidity and mortality when administered during the second or third trimester. Caution should be used in prescribing azilsartan medoxomil/chlorthalidone to nursing mothers since chlorthalidone is excreted into human breast milk and azilsartan medoxomil is excreted in low concentrations in the milk of lactating rats. 6
WARNINGS AND PRECAUTIONS
Volume-correction prior to administration of azilsartan medoxomil/chlorthalidone is recommended for volume- or salt-depleted patients to avoid symptomatic hypotension. 6 Clinicians should monitor renal function in patients initiated on azilsartan medoxomil/chlorthalidone therapy since inhibition of the RAAS can trigger changes including oliguria, azotemia, and, rarely, acute renal failure and death. Patients with unilateral or bilateral renal artery stenosis should avoid azilsartan medoxomil/chlorthalidone. 6
DRUG-DRUG INTERACTIONS
Drug-drug interactions must be evaluated in the context of the individual components since interaction studies have not been performed for the combination drug. Diuretic-induced sodium loss decreases renal lithium elimination, potentially leading to toxicity with chlorthalidone coadministration. 6 Azilsartan medoxomil taken with nonsteroidal antiinflammatory drugs (NSAIDs) may exacerbate deterioration of renal function. NSAIDs and azilsartan medoxomil/chlorthalidone should not be coadministered, especially in geriatric patients, volume-depleted patients, and those with preexisting renal dysfunction. Conversely, NSAIDs may reduce the antihypertensive effect of azilsartan medoxo mil/chlorthalidone. Coadministration of azilsartan medoxomil/chlorthalidone with other agents that affect the RAAS may precipitate hypotension, hyperkalemia, and renal function decline. Aliskiren should not be administered in combination with azilsartan medoxomil/chlorthalidone in patients with diabetes or a glomerular filtration rate less than 60 mL/min.
ADVERSE REACTIONS
According to the manufacturer, clinical trials have studied the adverse effect profile of azilsartan medoxomil/chlorthalidone in more than 3900 patients. 6 Of the 8.3% of patients discontinuing marketed doses of the drug, 3.6% and 2.3% of the studies cited increased SCr and dizziness, respectively, as reasons for stopping treatment. 6 Typically, SCr elevations in clinical trials were transient, nonprogressive, and reversible after drug discontinuation. 34,35 Researchers recognized a negative relationship between large reductions in BP and/or weight and SCr elevations. 34,35 Headache, hypotension, and syncope were reported infrequently. 6
Thiazide-type diuretics negatively impact metabolic parameters through effects on glucose intolerance, hypokalemia, hyperlipidemia, and an increase in incident diabetes. 2,42–44 Accumulating evidence indicates that RAAS inhibitors may mitigate the adverse metabolic effects of diuretics, including blunting the risk of new-onset diabetes 3,45,46 ; this effect has not been studied with azilsartan medoxomil/chlorthalidone.
Azilsartan attenuates the potassium-wasting effect of chlorthalidone. A shift from normal serum potassium levels to hypokalemia (<3.4 mEq/L) occurred in fewer azilsartan medoxomil/chlorthalidone–treated patients (1.7%) than in those treated with chlorthalidone alone (13.0%), but marginally more than those treated with azilsartan medoxomil (0.9%). 34 Only 1 patient treated with azilsartan medoxomil/chlorthalidone experienced a transition from normal to elevated (>5.4 mEq/L) serum potassium levels. 34
Serum uric acid increases above the upper limit of normal after 8 weeks of study drug use occurred considerably more often with azilsartan medoxomil/chlorthalidone (29.5%) than with azilsartan 40- or 80-mg (6.3%) and modestly more than with chlorthalidone 12.5- or 25-mg (21.8%). 34 Thiazide-induced volume contraction and thiazide-uric acid competition for renal tubular secretion explains the observed hyperuricemia. Rates of hyperuricemia with azilsartan medoxomil/chlorthalidone 40 mg/25 mg were slightly lower in a 12-week study (15.6%) than in the 8-week trial. 35
Angiotensin receptor blockade reduces the risk of dry cough and angioedema significantly compared with angiotensin-converting enzyme (ACE) inhibition. 47 Azilsartan medoxomil and ACE inhibitors have not been compared to determine the incidence of these adverse effects. Regardless, azilsartan medoxomil represents a logical therapeutic alternative for patients with ACE inhibitor-induced cough.
In a 12-week RCT comparing azilsartan medoxomil/chlorthalidone 40 mg/25 mg with olmesartan medoxomil/hydrochlorothiazide 40 mg/25 mg, rates of serious events (0.3% vs 2.2%, respectively) and events leading to drug discontinuation (8.7% vs 7.1%, respectively) were similar, and consecutive elevations of SCr occurred less frequently with azilsartan medoxomil/chlorthalidone (1.4% vs 2.8%). 35 On the other hand, the frequency of any adverse event was higher with azilsartan medoxomil/chlorthalidone versus olmesartan medoxomil/hydrochlorothiazide (71.3% vs 60.2%). 35
The incidence of adverse events was dose-related, with more total drug-emergent adverse events occurring with 40-mg/25mg doses (67.9%) than with 40-mg/12.5-mg doses (56.8%). 34 Doses greater than 40 mg/25 mg increased the potential for adverse events without providing consistent incremental BP reductions. 34 Step-wise titration of azilsartan medoxomil/chlorthalidone decreased adverse reactions and discontinuations versus a fixed-dose factorial design, as evidenced by the results of 3 double-blind, active controlled, titration studies. 6 These trials more closely resemble typical, real world practice because clinicians typically only increase antihypertensive doses in patients who do not achieve an adequate response to lower doses.
Formulary Considerations
The average wholesale price (AWP) of Edarbyclor is $3.32/tablet in both available strengths. 48 As the AWP is only slightly lower for the single agent (azilsartan medoxomil; $3.24/tablet), the combination tablet represents a potential cost-saving option for patients requiring more than 1 antihypertensive medication. 49 Furthermore, both azilsartan medoxomil/chlorthalidone doses outperformed the more expensive olmesartan medoxomil/hydrochlorothiazide (Benicar HCT, Daiichi Sankyo) 40 mg/25 mg dose in a clinical trial ($5.21/tablet). 48
Three ARB-diuretic combination tablets have generic availability (ie, losartan/hydrochlorothiazide, irbesartan/hydrochlorothiazide, valsartan/hydrochlorothiazide) and potentially reduced costs versus brand name only products. These agents may be less effective at lowering BP than chlorthalidone-containing combinations since the hydrochlorothiazide component does not exceed 25 mg in any ARB/hydrochlorothiazide combination tablet.
Fixed-dose combinations might pose a cost disadvantage to patients since insurance plans often exclude combination medications from their drug formularies. 50 Combining a generic ARB (ie, losartan, irbesartan) with chlorthalidone offers attractive cost savings and the flexibility to independently modify the dose of an individual component. 50 However, this alternative may negatively lower patient adherence by introducing polypharmacy.
Summary
Sufficient evidence exists to support the clinical usefulness of azilsartan medoxomil/chlorthalidone in hypertensive patients. The combination offers considerable benefits due to its unique inclusion of an RAAS inhibitor with chlorthalidone, a thiazide-type diuretic with clinical outcomes data and greater potency and a longer duration of action than hydrochlorothiazide. Fixed-dose antihypertensive combinations offer several advantages from a clinical perspective, including increased efficacy, improved convenience and patient adherence, reduced incidence of adverse effects compared with high-dose monotherapy, and lowered health care costs. Although hypertension treatment should be individualized, azilsartan medoxomil/chlorthalidone represents a reasonable option for patients with stage 2 hypertension or for patients with uncontrolled hypertension already on 1 or more drugs. Results of further studies will clarify the role of this combination in long-term reductions in end points.
Footnotes