
Abstract
Although marketing scholars often seek to contribute new knowledge that is applicable across industries, some industries have unique characteristics that require industry-specific knowledge development. The authors argue that this requirement applies to the life sciences industry, defined as companies in pharmaceuticals, biotechnology, and therapeutic medical devices. Marketers in the life sciences industry face novel and unique challenges along eight decision areas in therapy creation, therapy launch, and therapy promotion. In therapy creation, they face therapy pipeline optimization, innovation alliance formation, and therapy positioning decisions. In therapy launch, they face global market entry timing and key opinion leader selection decisions. Therapy promotion mostly revolves around sales force management, communication management, and stimulating patient compliance. The authors qualify these decision areas according to their practical importance and academic potential. The article derives preliminary generalizations and propositions from prior research and practice and steers further research in specific directions. The authors believe that marketing of the life sciences offers a fertile area for further research because, among other things, its potential impact transcends any problems typically investigated by marketing scholars.
Keywords
In this article, we argue that this requirement also applies to the life sciences industry. In our definition, this industry spans companies in pharmaceuticals, biotechnology, and therapeutic medical devices, and it forms the innovative producer side of the health care industry. Two fundamental dimensions underlie the life sciences industry: science-based knowledge (know-why) and quality of life.
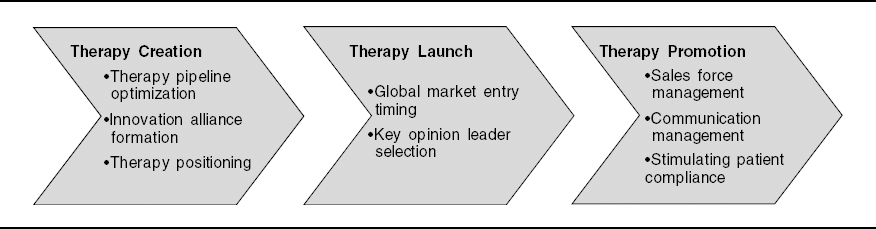
Life sciences companies are significantly more linked to science than any other industry and convert the know-why they develop into new therapies (therapy creation). The resultant therapy is launched into society only after scientific review of its impact on people's quality of life through examination of the therapy's safety, efficacy, and incremental cost effectiveness (therapy launch). Life sciences firms promote their life sciences therapies to both health care providers and patients within the regulatory framework designed by society (therapy promotion). Marketers face unique challenges in therapy creation, therapy launch, and therapy promotion decisions (see Figure 1).
Key Marketing Decision Areas in Life Sciences Firms
The scant survival probability of newly created therapeutic inventions—only 1 in 5000–10,000 new inventions eventually makes it to market—leads to life sciences development portfolios being uniquely shaped as funnels (Ding and Eliashberg 2002). Life sciences marketers decide on therapy positioning—the match between indication and new therapy—many years before market entry. Market entry for new therapies is strictly regulated, differentially so across countries. If market access is granted, manufacturers get a limited time—in most cases, 20 years as of initial application filing, 10–12 of which are typically spent in clinical development—of market exclusivity, after which generic therapies can enter the market. Life sciences firms’ marketing efforts are typically capped (e.g., in many European countries) and/or regulated (e.g., some states in the United States require medical sales representatives to undergo a certification process). Life sciences is also one of the few industries in which manufacturers are legally prohibited from communicating directly with their end customer (with the exception of New Zealand and the United States).
The life sciences industry constitutes an important and growing part of the economy; for example, the U.S. life sciences industry represented $271 billion of global sales in 2007 (Pharmaceutical Research and Manufacturers of America 2008). In the United States, prescription drug spending—the life sciences industry's largest component—is expected to accelerate through 2017 (Centers for Medicare & Medicaid Services, Office of the Actuary 2008).
Because of its vast importance and unique challenges, the marketing literature has recently turned to the life sciences industry to study sales force effectiveness (Manchanda and Chintagunta 2004; Manchanda and Honka 2005; Manchanda, Rossi, and Chintagunta 2004; Mizik and Jacobson 2004; Venkataraman and Stremersch 2007), therapy compliance (Bowman, Heilman, and Seetharaman 2004; Wosinska 2005), communication effectiveness (Cleanthous 2004; Iizuka and Jin 2005; Macias and Lewis 2003; Mukherji, Dutta, and Rajiv 2004; Wosinska 2006), and innovation (Chandy et al. 2006; Ding and Eliashberg 2002; Prabhu, Chandy, and Ellis 2005; Sorescu, Chandy, and Prabhu 2003, 2007; Wuyts, Dutta, and Stremersch 2004), among other areas.
The objectives of the current research are to evaluate prior research, suggest new directions for further research, and ignite life sciences marketing as an important area for scholarly research. We achieve these objectives by defining the life sciences industry and discerning its boundaries, deriving the key marketing decision areas in this industry, formulating generalizations and propositions derived from prior research and state-of-the-art practice, and steering further research in specific directions.
Defining the Life Sciences Industry and Its Boundaries
Underlying Dimensions of the Life Sciences Industry
A first constitutive characteristic of the life sciences industry is that this industry creates scientific knowledge regarding why a certain therapy affects the human body in a certain way. Science represents “know-why” (Kogut and Zander 1992), in contrast to technology, which represents “know-how” (Quinn, Baruch, and Zien 1997). The average number of scientific studies a firm cites when applying for a patent for its inventions (science linkage), rather than other prior patents (know-how development), can be used as a measure of the extent to which the firm is science based (Narin 2001).
A second constitutive characteristic of the life sciences industry is that the preventive or curative therapies it creates are scientifically reviewed regarding their effect on people's quality of life, after which they are promoted to patients and providers to convince them of the acclaimed effects. Improvement in quality of life is expressed as an increase in “quality-adjusted life years” (often referred to as QALYs) and can lie in enhanced effectiveness, reduced side effects, and improved convenience (Garber and Phelps 1997). It is based on both quantity and quality of life years generated by the medical interventions.
The Components of the Life Sciences Industry
We discern three components within the life sciences industry: pharmaceutical, biotechnological, and therapeutic medical devices. These three industries are science based because their patents typically refer to more scientific studies than any other industry. For example, Narin (2001) shows that pharmaceutical and biotechnology firms, respectively, cited 7.3 and 14.4 scientific references per patent, which were the two highest science linkages of all technology areas. Though not separately identified in Narin's study, therapeutic medical devices are also science based. First, the average science linkage of all medical devices and equipment companies, which includes therapeutic medical devices, is more than twice the average of the high-tech industry, such as aerospace or information and communication technologies (Narin 2001). Second, therapeutic medical devices companies, such as Nektar Therapeutics or ArthroCare, belong to the most science-based companies in the economy. 1
Nektar Therapeutics offers noninvasive deep-long delivery systems. ArthroCare offers minimally invasive surgical procedures involving tissue removal and treatment.
These three industries also market products that aim to improve the quality of life. They market inorganic compounds (pharmaceutical), organic compounds (biotechnology), or therapeutic devices that affect the (diseased) human body. Take breast cancer as an example. Pharmaceutical firms aim to improve breast cancer patients’ condition through chemotherapy, and biotechnology firms may offer targeted therapies in well-identified patient types (e.g., Herceptin by Genentech). Device-based therapies are also often used with the same objective of increasing quality-adjusted life years (e.g., through radiotherapy).
Discerning the Boundaries of the Life Sciences Industry
Our definition of the life sciences industry enables us to discern life sciences boundary industries (see Figure 2)—namely, cosmeceuticals, medical devices and equipment, and nutraceuticals. Each of these industries contains a small segment that belongs to the life sciences industry because it produces therapies that are science based and improve quality of life.

The Life Sciences Industry and Its Boundaries
Typical cosmeceuticals are antiwrinkle agents or balms to treat eczema or burning wounds. They prevent, treat, or cure diseases, mostly of the skin. Therefore, they are distinct from mere cosmetics, which aim to alter appearance of the skin, eyes, hair, nails, and so forth. Some cosmeceuticals (i.e., cosmetics-based therapies) are science based (e.g., acne care products with therapeutic antiseptics).
Medical devices and equipment vary from wheelchairs to imaging devices (e.g., magnetic resonance imaging) to stents. Equipment such as wheelchairs improve the patient's quality of life (e.g., through mobility), but they are not science based. In contrast, medical imaging devices do not therapeutically improve humans’ quality of life but represent considerable know-why (science). Some devices (i.e., device-based therapies), such as stents, implants, and pacemakers, enhance the quality of life and are science based; thus, they belong to the life sciences industry.
Nutraceuticals refer to products such as nutritional supplements, vitamin- or calcium-enriched foods, and polyunsaturated fatty acids. Nutraceuticals may improve quality of life beyond merely feeding the body (foods). However, only a subset of these products (i.e., food-based therapies) is science based and, thus, part of the life sciences industry. An example is sterol-derived, cholesterol-lowering BENECOL.
Therapies exist that include both a device and a cosmeceutical or nutraceutical component. Examples include breast implants (cosmeceuticals and devices) and nutrigenomics, that is, personalized diet recommendations based on diagnostics of bodily fluids (nutraceuticals and devices). Figure 3 positions the life sciences industry in the health care market (adapted from Burns 2005). Payment flows from left to right, from payers to providers, over financial intermediaries. Products flow from right to left, from producers to providers, over product intermediaries. The life sciences industry is the producer side of the health care market.
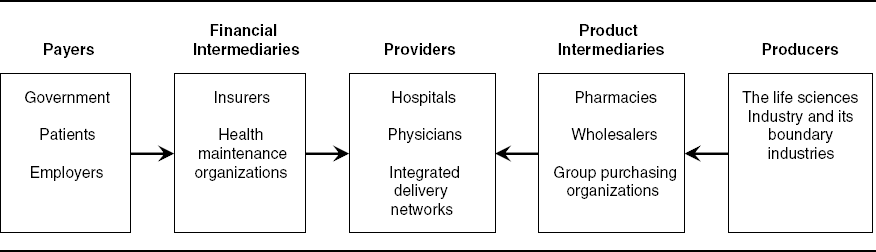
The Life Sciences Industry in the Health Care Market
Key Marketing Decision Areas in the Life Sciences Industry
Next, we derive the key decision areas for marketers in the life sciences industry. We first discuss our methodology, after which we identify and qualify the key marketing decision areas on managerial relevance and scholarly potential.
Methodology
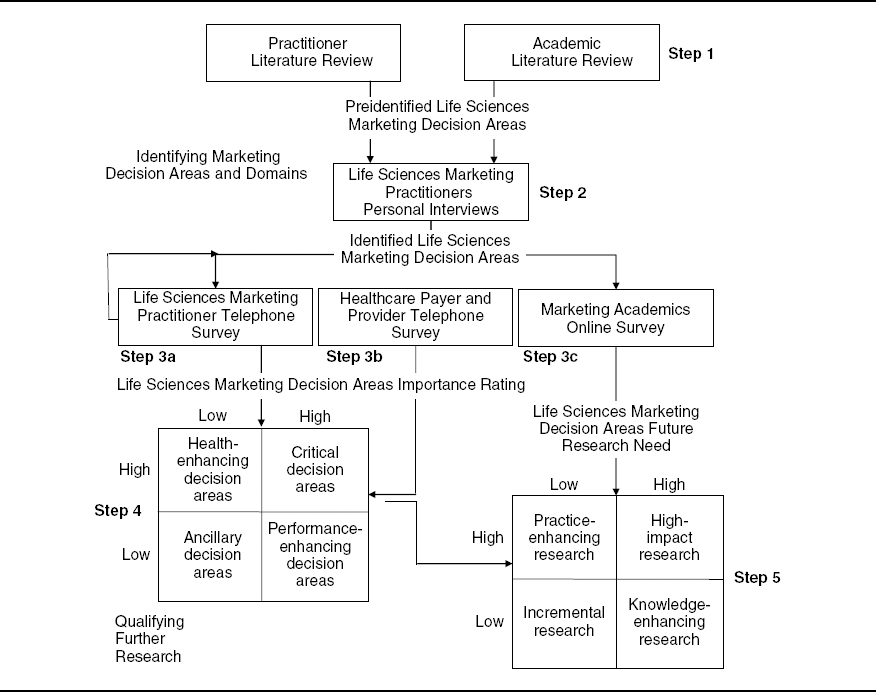
Figure 4 graphically depicts our methodology. We first identified marketing decision areas in life sciences from a literature study (Step 1). 2 Appendix A provides an overview of the major publications in life sciences marketing according to the three areas we defined—therapy creation, launch, and promotion. These publications include International Journal of Research in Marketing, Journal of Consumer Research, Journal of Marketing, Journal of Marketing Research, and Marketing Science, which have been used in prior research as a good representation of the major journals in marketing (Stremersch and Verhoef 2005; Stremersch, Verniers, and Verhoef 2007).
Our sample of academic literature included (1) marketing journals, such as Journal of Marketing; (2) journals on the boundaries of the marketing discipline, such as Management Science; (3) specialized journals in life sciences and health economics, such as Journal of Health Economics; (4) recent proceedings of conferences, such as the INFORMS Marketing Science Conference (2000–2008) and the Association for Consumer Research conference (2000–2008); and (5) unpublished working papers. In the study of the industry literature, we included Journal of Medical Marketing, Life Sciences, Medical Device Technology, Medical Marketing & Media, Pharmaceutical Executive, and Pharma Marketing News, among others.
Methodology
Given its relatedness in the health care value chain, Appendix B provides an overview of the health psychology literature in the same major marketing journals. It discerns three frameworks in this literature: health-related behavior, health risk perception, and health communication. Two early schools of thought underlie these frameworks: protection motivation theory and the health belief model. Protection motivation theory predicts protection intentions as a function of severity, vulnerability, response efficacy, and self-efficacy and is used to test the effectiveness of health communication (Maddux and Rogers 1983; Rogers 1975; see also Keller and Lehmann 2008). The health belief model (Becker 1974; Rosenstock 1974) proposes that increasing risk perceptions should lead to precautionary behavior (see Menon, Raghubir, and Agrawal 2008).
Though more distant to the life sciences marketing field, we also reviewed the health economics literature. The literature provides good reviews on the cost of innovation (see DiMasi, Hansen, and Grabowski 2003), price competition among pharmaceutical firms (see Bhattacharya and Vogt 2003; Scherer 1993), the effect of generic entry on branded drug prices (see Frank and Salkever 1997; Grabowski and Vernon 1992), health care policy (see Drummond, Jönsson, and Rutten 1997; Scherer 2004), and reference pricing (see López-Casasnovas and Puig-Junoy 2000).
In Step 2, we conducted two-hour personal interviews with nine marketing experts in life sciences companies, such as Amgen, GlaxoSmithKline, Novartis, Novo Nordisk, and Philips Medical Systems. To have sufficient confidence in our findings and to qualify the marketing decision areas we identified in terms of importance, we conducted quantitative telephone surveys with marketing managers at life sciences firms and with health care payers and providers, and we conducted an online survey of marketing academics.
We sampled marketing managers (Step 3a) using a snowballing technique, first contacting respondents we knew personally, then contacting executives the first respondents identified as useful respondents, and so on. In total, we contacted 110 executives, 96 of whom agreed to participate in the telephone interview (for a response rate of 87%): 40 managers of pharmaceutical firms (e.g., Astellas Pharma, AstraZeneca, Bristol-Myers Squibb, GlaxoSmithKline, Johnson & Johnson, MSD, Novartis, Novo Nordisk, Organon, Pfizer, Roche, Sanofi-Aventis, Schering-Plough, Wyeth), 28 managers of biotech firms (e.g., Amgen, Biogen Idec, Galapagos, Genzyme, Novo Nordisk, Organon), and 28 managers of medical devices companies (e.g., 3M Medical Specialties, AGFA HealthCare, B. Braun, Coloplast, Johnson & Johnson, Philips Medical Systems, Siemens Medical Solutions). We overweighted the pharmaceutical industry, given its larger size compared with the others. From these managers, we inventoried key decision areas (open question) and the importance of each previously identified (Steps 1 and 2) decision area for the firm on a 1–7 scale.
We sampled health care payers and providers (Step 3b) from contact lists provided by IMS Health. From a sample of 545 payers and providers, 112 respondents participated (for a response rate of 21%), 81 of whom were physicians (health care providers) and 31 of whom were representatives of health care government and health management organizations (health care payers). From this sample, we assessed the impact of the previously identified (Steps 1–3a) marketing decision areas on patient welfare on a 1–7 scale.
We sampled academics (Step 3c) using two criteria: (1) They had a position in marketing, and (2) they had knowledge relevant to the life sciences industry through their academic research. From a sample of 78, the following 29 academics eventually participated (for a response rate of 37%): N. Agrawal, M. Ahearne, R. Bezawada, L. Bolton, D. Bowman, R. Chandy, A. Ching, M. Dekimpe, M. Ding, X. Dong, J. Eliashberg, P.A. Keller, L. Krishnamurthi, M.F. Luce, P. Manchanda, M.K. Mantrala, N. Mizik, C. Moorman, H. Nair, J.C. Prabhu, V. Shankar, C. Sismeiro, A. Sorescu, E.R. Spangenberg, P. Stern, D. Vakratsas, C. Van den Bulte, S. Venkataraman, and S. Wuyts. For each of the previously identified marketing decision areas (Steps 1–3a), we asked the academics to assess (on a 1–7 scale) the extent to which (1) they are covered by current marketing research in progress, (2) they deserve more scholarly attention in the future, and (3) they are perceived by academics as important for life sciences marketers in practice.
Step 4 yields the practical impact of life sciences marketing decision areas from both a firm profit perspective and a patient welfare perspective. Step 5 consists of mapping the need for academic research, as perceived by academics, onto decision area importance, as perceived by practitioners (combining the input of both marketing managers and health care providers and payers).
Identification of Key Marketing Decision Areas
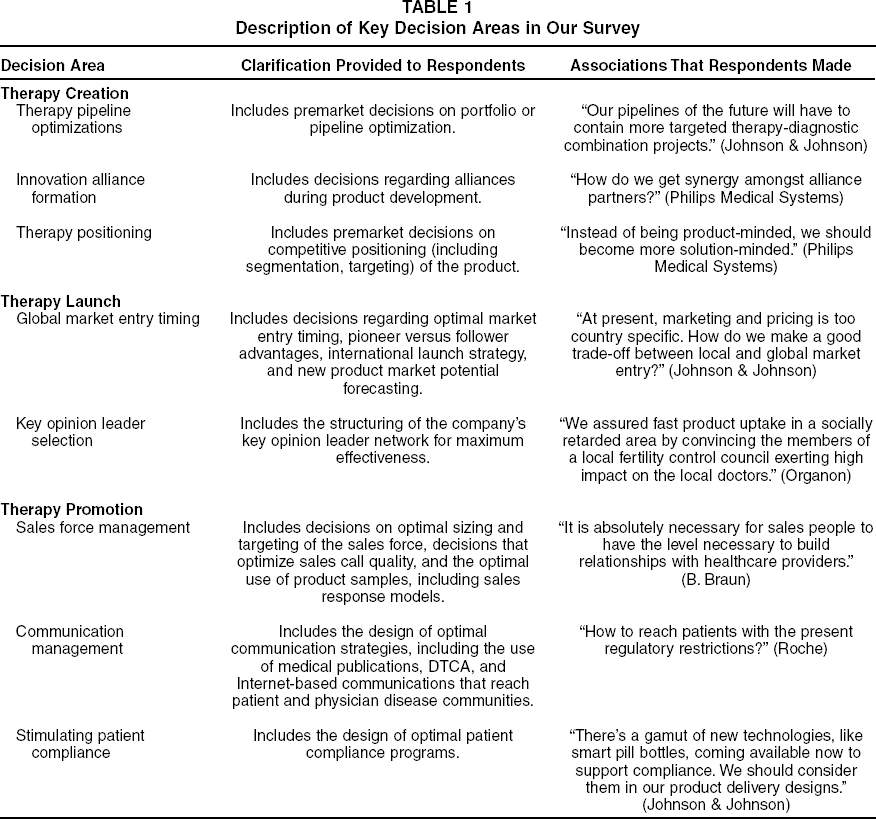
Figure 1 contains the marketing decision areas we retained as key areas, grouped into three higher-level decision domains: therapy creation, therapy launch, and therapy promotion. In therapy creation, the key decision areas are therapy pipeline optimization, innovation alliance formation, and therapy positioning. The key decision areas in therapy launch are global market entry timing and key opinion leader selection. The key decision areas in therapy promotion are sales force management, communication management, and stimulating patient compliance. Table 1 describes each decision area. The second column presents the clarification we provided to respondents when we asked them to rate the decision area's importance. The third column contains the associations respondents made for each decision area during our interviews.
Description of Key Decision Areas in Our Survey
Qualifying Key Marketing Decision Areas in Terms of Research Potential
In Step 4 (for more details, see Figure 5), we join relevance in terms of business performance (averaged over all life sciences firms we surveyed) and relevance in terms of patient welfare (average of the averages over all surveyed payers on the one hand and all surveyed providers on the other hand 3 ). Average importance to business performance ranged from 4.8 (innovation alliance formation) to 5.6 (sales force management), while average importance ratings to patient welfare ranged from 3.6 (therapy positioning) to 5.2 (communication management), all on a scale ranging from 1 to 7. In Figure 4, we qualify the different cells as follows: (1) “Critical decision areas” are of above-median importance to both business performance and patient welfare, (2) performance-enhancing decision areas are of above-median importance to business performance and of below-median importance to patient welfare, (3) health-enhancing decision areas are of below-median importance to business performance and of above-median importance to patient welfare, and (4) ancillary decision areas are of below-median importance to both business performance and patient welfare.
The responses of payers were similar to the responses of providers. The correlation between the average ratings across both groups of respondents was .90, yielding a similar ranking on importance of decision areas.

Importance of Decision Areas to Firm Performance and Patient Welfare
Communication management and key opinion leader selection appear to be critical decision areas. Global market entry timing and sales force management are performance-enhancing decision areas. The low relevance of sales force management to patient welfare may explain why many hospitals and physicians have begun to deny access to pharmaceutical sales representatives. Therapy pipeline optimization and stimulating patient compliance are health-enhancing decision areas. Innovation alliance formation and therapy positioning decisions are ancillary, probably to therapy pipeline optimization.
In Step 5 (for more details, see Figure 6), we confront the practical importance of decision areas (taken to be the highest of importance in terms of business performance and patient welfare) with the need for academic research, as perceived by academics. The average need for further academic research ranges from 5.0 (sales force management) to 5.8 (stimulating patient compliance) on a scale ranging from 1 to 7. In Figure 4, we qualify the cells as follows: (1) High-impact research is research that promises to be an important contribution to academic knowledge and of high, immediate, practical relevance to business performance and/or patient welfare; (2) knowledge-enhancing research is research that promises to be an important contribution to academic knowledge but is not necessarily of immediate, practical relevance; (3) practice-enhancing research is research of high, immediate, practical relevance to business performance and/or patient welfare but is not necessarily of immediate academic importance; and (4) incremental research is research that is neither of high, immediate, practical relevance nor necessarily an important contribution to academic knowledge.

Research Agenda
Although all four types of research are valuable in their own right, the chance of gaining a breakthrough insight is the highest in the “high-impact” (top-right) quadrant of Step 5 in Figure 4 (for more details, see Figure 6). Such decision areas are therapy pipeline optimization, global market entry timing, key opinion leader selection, and stimulating patient compliance. Further research on innovation alliance formation is qualified as knowledge-enhancing research. The academic knowledge generated can be ancillary to decision areas such as therapy pipeline optimization. Communication and sales force management are practice-enhancing areas. Research on therapy positioning is likely to be incremental.
Academics assessed the need for further research on therapy positioning as low because they considered this decision area of low practical relevance, while they assessed the need for further research on sales force and communication management as low because it is already largely addressed in prior and ongoing research, even though its relevance remains high.
Generalizations, Propositions, and Directions for Further Research
Drawing on prior research and practice, we formulate preliminary generalizations (G) to evaluate early streams of research in this area, and we develop propositions (P) that provide direction for further research. Preliminary generalizations are already supported by the existing literature, but they may benefit from additional testing through techniques such as meta-analyses. Propositions are exploratory and at least partly supported by verbal logic, mathematical proof, or empirical evidence (Stremersch and Tellis 2002).
Therapy Creation
Therapy pipeline optimization
In life sciences firms, therapy pipelines contain all innovation projects along the following temporal stages: During discovery, therapy candidates are screened for maximum activity on the biological target. Preclinical development and clinical development entail further development, using in vitro or animal experiments and human experiments, respectively.
Prior research on therapy pipelines aimed to determine the optimal number and sequencing of innovation projects that a firm's resource base could support and that served its goal to maximize the number of commercially launched innovations (see Blau et al. 2004; Chandy et al. 2006; Ding and Eliashberg 2002; Loch and Kavadias 2002). This research found that there is an inverted U-shaped relationship between the number of innovation projects undertaken and the number of innovations commercially launched. However, scholars in this literature stream did not discern the different temporal stages in the therapy pipeline. Although companies’ ability to convert innovation projects in commercially launched products may suffer from taking on too many projects in development, this may not be the case in discovery, in which more exploration leads to more effective knowledge on biological targets, resulting in more new therapy opportunities. Thus:
There is a positive relationship between the number of innovation discovery projects initiated and the number of patented inventions of a firm.
There is an inverted U-shaped relationship between the number of innovation development projects initiated and the number of commercially launched innovations of a firm.
The optimal number of innovation development projects a firm should undertake may also be contingent on the type of innovation project. Targeted (specific for certain patient types) therapy innovation projects require fewer resources in development and feature higher probabilities of ultimate regulatory approval (Vernon and Hughen 2005). Thus:
Innovation development projects on targeted therapies lead to more commercially launched innovations than the same number of innovation development projects on nontargeted therapies.
Scholars might also study other types of innovation projects as contingency factors beyond targeted or nontargeted projects, such as radical versus incremental projects. Studying the therapy pipeline in the context of patent expiry might also be fruitful. Firms may anticipate expiry in multiple ways, such as the development of combination drugs, more convenient administration and dosage methods, and reengineered variants with higher effectiveness or less serious side effects. To develop and test such a contingency framework, scholars could analyze databases, such as the Pharmaprojects database, the R&D Focus Database that IMS Health maintains, and the Food and Drug Administration's (FDA's) Orange Book, all of which contain detailed pipeline information. As outcome variables, scholars could gather information on the number of approved new patents (U.S. Patent and Trademark Office) and new therapies (the FDA's Orange Book). Beyond direct innovation measures, they could also examine the impact of therapy pipeline decisions on sales, profits, or stock market returns.
Innovation alliance formation
As we noted previously, practitioners consider decisions on innovation alliances ancillary decisions. At the same time, this decision area has provided an ideal and often-used testing ground for theory development on interfirm cooperation. The reason is that the life sciences industry provides possibly the richest documentation on such alliances (e.g., Recap's database on interfirm agreements) and their outcomes (e.g., patents, new products, profits, sales, share price).
Similarity between parties in an alliance is probably most often studied. Dissimilarity between partners yields greater learning opportunity because there is less knowledge redundancy, while similarity between partners makes it easier to understand each other and share information. The tension between both arguments has led many researchers (Cloodt, Hagedoorn, and Van Kranenburg 2006; Prabhu, Chandy, and Ellis 2005; Wuyts et al. 2005) to find a curvilinear relationship between knowledge similarity between alliance partners and the innovative outcome that the alliance yields. This leads us to the following preliminary generalization:
There is an inverted U-shaped relationship between knowledge similarity between alliance partners and the number of new therapies the alliance yields.
Scholars have also studied the differential effect of alliances on radical versus incremental innovation (Wuyts, Dutta, and Stremersch 2004). For radical innovation, it is instrumental that alliance partners repeatedly cooperate to stimulate knowledge transfer through the development of relationship-specific heuristics and the sharing of mental models, among other things (Madhaven and Grover 1998; Uzzi 1997). Genentech and Roche provide a successful example of such repeated collaboration. For incremental innovation, large portfolios may be beneficial because of scale effects in development (Ahuja 2000; Wuyts, Dutta, and Stremersch 2004). We offer the following preliminary generalizations:
As the level of repeated partnering in a firm's innovation alliances portfolio increases, its radical innovation output increases.
As the number of alliance partners in a firm's innovation alliances portfolio increases, its incremental innovation output increases.
Further research on interfirm cooperation will likely continue to use the life sciences industry as a testing ground for theory development, with continued use of databases (e.g., Pharmaprojects, Recap), newspapers and magazines, and surveys. Novel breakthroughs are likely to be in the areas of social networks and the balance between internal and external innovation.
Therapy positioning
Therapy positioning refers to research-and-development (R&D) decisions on the envisioned therapy toward specific indications. The practitioners we surveyed considered therapy positioning an ancillary decision area, while academics did not foresee a strong need for further research. Therefore, we do not derive theoretical generalizations or propositions. Decision makers need to balance three key dimensions: (1) the likelihood that the therapy will be approved for the respective indication, (2) the price they will obtain from the therapy, and (3) the market size for the respective indication over time.
If positioned for a mild indication, a therapy may reach a large market, but at relatively low prices and with possible denial of approval. Consider Elidel (pimecrolimus), a therapy for eczema by Novartis. Novartis introduced Elidel for a mild to moderate indication of eczema—that is, for first-line use. Competitor Fujisawa introduced a variant of this molecule, Prograf (tacrolimus), which was targeted at moderate to severe indications of eczema—that is, for second-line use. Although both products showed scientific evidence, only tacrolimus was endorsed by the U.K. government, because the former could not show that it represented a good value for the money (Gregson et al. 2005) for the moderate indication. It was subsequently endorsed after resubmission, but then also for the severe indication. If positioned for a severe indication, a therapy may have a higher likelihood of being approved at a high price, but it may pertain to a relatively small market. For example, Symbicort by AstraZeneca was first approved for severe asthma, after which AstraZeneca enlarged the market for Symbicort to chronic obstructive pulmonary disease (COPD).
Because there are many possible indications, all with different levels of uncertainty for the respective therapy to be approved and varying price expectations, further research should aim to specify decision support models that simulate market size using patient flow dynamics (first use, reuse, switching from competition) at various price expectations and approval likelihoods.
Therapy Launch
Global market entry timing
Previous research has shown that pioneers do not have long-lasting market advantages (Golder and Tellis 1993; Shankar, Carpenter, and Krishnamurthi 1999). In the life sciences industry, an important moderator of the market return on a pioneering therapy may be whether it pertains to generic or branded therapies. In the case of branded therapies, pioneers are the first entrants in a therapeutic category (e.g., Mevacor [1987] for statins). In the case of generic therapies, pioneers are the first generic available for a specific therapy (e.g., the first generic Simvastatin, the statin introduced by Merck as Zocor).
There are many cases of late branded entrants that took over pioneers through increased effectiveness, higher convenience, or weaker side effects. Examples include Zocor and Lipitor in statins (increased effectiveness), Symbicort in asthma/COPD (higher convenience), and Xyzal in antihistamines (weaker side effects).
Contrary to common wisdom in other industries and contrary to branded variants in life sciences, generics may yield strong pioneering advantages. The first generic variant for a specific therapy (“the pioneer”) may attract and maintain a disproportionately large market share. The reasons for this are multifold. It takes substantial effort from physicians and pharmacists to explain bioequivalence between different variants (Gupta, Yu, and Guha 2006). At the same time, only the pioneering generic therapy benefits from the large price differential with the alternative (the branded variant). Generics that subsequently enter do not show as large of a price differential anymore, and when they do, the generic pioneer may readily match the lower price, with market shares remaining stable (Hollis 2002). The first generic entrant also typically makes supranormal profits before the entry of a second generic because it provides the only (cheap) alternative for an expensive branded variant (Gupta, Yu, and Guha 2006). Thus:
Pioneering yields market share advantages for generic therapies.
The life sciences industry lends itself well to the examination of order-of-entry effects because entry is well documented (e.g., with the FDA
Firms typically do not launch a new treatment simultaneously across the globe. Rather, they use specific launch sequences, often driven by a country's regulatory system, economic wealth, and size (Danzon, Wang, and Wang 2005; Kyle 2007; Verniers, Stremersch, and Croux 2008). Differential launch timing across countries has been shown not to affect unit sales (Stremersch and Lemmens 2009), though it has been shown to affect launch price (Verniers, Stremersch, and Croux 2008). In the life sciences industry, launch price is rarely a market price; rather, it is often an agreed-on price between the supplier and the government or insurance firm, which acts as a (co)payer. In such negotiations, entry timing may be used by both the payer and the firm as an instrument to affect the agreed-on price.
An important contingency factor that has not received any attention is the role of cross-country influence in launch sequencing. Often, this cross-country influence is institutionalized because payers will use the price of a therapy in a defined set of other countries (the “referent” countries), if available, as a reference price for the negotiations in their own country (the “referencing” country). Such regulation incentivizes companies to avoid spillover effects (Hunter 2005). Thus:
Firms that launch a new therapy in a referencing country early relative to the set of referent countries obtain a higher price than firms that launch a new therapy in a referencing country late relative to the set of referent countries.
To test this proposition, regulatory data can be gathered from Urch Publishing and the Organisation for Economic Co-operation and Development, both of which track international regulatory health systems (including identification of the set of referent countries for each referencing country), and integrated with IMS Health data on international prices and introduction dates. It is also possible to include firm effects (firms may have differential policies, depending on their home market or size) or therapy effects (payers across countries may have differential price and market access policies for different therapy classes). In addition, diffusion studies can deliver valuable and complementary insights into launch decisions. Examples of such valuable inquiries that may inform launch decisions are improved models of physician learning and international diffusion studies.
Key opinion leader selection
Life sciences firms often stimulate reviews of their therapy by select key opinion leaders because such leaders may serve as product champions to their peers. The effect of such opinion leaders on other physicians’ prescriptions can be large when considerable uncertainty exists (e.g., a change in the regulation or the introduction of a new therapy) or when physicians experience normative pressures (e.g., there is strong formulary adherence) (Coleman, Katz, and Menzel 1966; Iyengar, Valente, and Van den Bulte 2008). For example, Nair, Manchanda, and Bhatia (2006) show that the effect of opinion leader prescriptions is 100 times larger than the detailing effect on regular physicians after the market underwent a change in National Institutes of Health guidelines.
However, we cannot take the positive role of opinion leaders for granted (e.g., Van den Bulte and Lilien 2001), and further research should inventory the contingencies that affect the role of opinion leaders. In such research, it is worthwhile to consider two types of key opinion leaders with potentially differential effectiveness: clinical and market leaders. Clinical leaders are experts within the respective disease and therapy class with a strong reputation, as evidenced by their publication records in top-ranked medical journals. They are typically involved in premarket product testing and have cooperated with the firm to reduce clinical uncertainty of the therapy. In contrast, market leaders are tightly connected to the local patient and physician communities. They are typically general practitioners with large practices who gain recognition by the satisfaction and loyalty of their patients. They deliver key experiential messages on the therapy to their peers.
For example, as a contingency factor, consider whether uncertainty manifests in terms of effectiveness or side effects of a life sciences therapy. The impact of uncertainty on effectiveness can be reduced through quantitative assessments without much detail on specific physician practices (i.e., large scale, study based). Conversely, the impact of side effects information is more qualitative and dependent on the specific composition of a practice (i.e., case based). Because clinical leaders support quantitative assessments of effectiveness and market leaders share case detail on side effects from practices similar to other physicians, we propose the following:
The greater the uncertainty on therapy effectiveness, the higher is the impact of clinical leaders, compared with market leaders, on other physicians’ prescription behavior.
The greater the uncertainty on therapy side effects, the higher is the impact of market leaders, compared with clinical leaders, on other physicians’ prescription behavior.
Another contingency factor to consider is the physician's institutional setting. Hospitals have formal ethical guidelines (Gallego, Taylor, and Brien 2007) to which an individual practitioner must adhere, which increases the return on legitimacy compared with general practitioners. Clinical leaders enhance legitimacy to a greater degree than market leaders, which fits with their high impact on formulary decisions. At the same time, market leaders achieve their influence through similarity of practice. In general, the practice of a market leader is more similar to a general practitioner practice than to a hospital-based practice. Thus:
Clinical leaders have a greater impact on hospital-based physicians’ prescription behavior than market leaders.
Market leaders have a greater impact on general practitioners’ prescription behavior than clinical leaders.
Researching these propositions can include surveying all physicians of a certain area to inventory their opinion leaders, including Likert-type scales on each of the identified leaders regarding the extent to which they are clinical and/or market leaders.
Therapy Promotion
Sales force management
A first decision area in therapy promotion is sales force management. Visits by the sales force of life sciences firms to physicians are referred to as “detailing.” Much academic research has emerged on the effectiveness (return on investment) of detailing (Azoulay 2002; Berndt et al. 1995; Leeflang, Wieringa, and Wittink 2004; Manchanda and Chintagunta 2004; Manchanda, Dong, and Chintagunta 2004; Manchanda and Honka 2005; Manchanda, Rossi, and Chintagunta 2004; Mantrala, Sinha, and Zoltners 1994; Mizik and Jacobson 2004; Narayanan, Desiraju, and Chintagunta 2004; Narayanan, Manchanda, and Chintagunta 2005; Parsons and Vanden Abeele 1981; Venkataraman and Stremersch 2007). We derive the following generalization from this literature:
The mean effect of detailing on brand prescriptions is (a) positive but (b) small.
“Mean” in G4 refers to the mean across brands and physicians. Prior literature has shown high physician- and drug-level heterogeneity, including some brands and physicians showing a negative return on detailing (Leeflang, Wieringa, and Wittink 2004), and has investigated specific contingency factors, such as drug characteristics (e.g., side effects, effectiveness [Venkataraman and Stremersch 2007], and physician traits [e.g., Gönül et al. 2001]).
There is room for further study. A first opportunity is to increase the reliability of this preliminary generalization through meta-analysis. Kremer and colleagues (2008) offer a first attempt at such generalization, but they provide only a limited number of significant moderators and omit drugs’ clinical profile. A second opportunity lies in the development of models that allow for policy experiments. Although we have reliable estimates of the mean effect of detailing, all models are estimated on data that show relatively little policy variance, which inhibits any extrapolation to policy shifts in detailing, either by the manufacturer (many firms are now considering drastically reducing their detailing efforts) or by the regulator (several European countries are considering curtailing detailing). The third opportunity lies in developing physician targeting models based on volume, physician responsiveness to detailing, and competitive detailing patterns (for working papers in this tradition, see Dong, Manchanda, and Chintagunta 2008; Kappe, Stremersch, and Venkataraman 2008).
By far, the most room for novel research seems to be in the content of detailing visits. Past and, for most companies, present detailing calls present only favorable information using positively biased information sets—that is, only studies favorable to the brand are presented, or side effects are omitted. This sales model seems increasingly dysfunctional, with hospitals and physicians reacting adversely to detailing, even rejecting it altogether, which is symptomatic for the conflicting logics between life sciences firms and the rest of the health care value chain (Singh, Jayanti, and Gannon 2008).
We propose that life sciences firms can gain substantial returns from communicating unfavorable information in their detailing calls, for two main reasons (Leffler 1981). First, in view of their ethical, gatekeeping function to patients, physicians prefer more complete information, even if unfavorable, over ambiguity. Second, communicating unfavorable information may enhance the legitimacy of the sales representative and the firm (Singh, Jayanti, and Gannon 2008). In turn, this enhanced legitimacy may deliver sustained physician access and increased trust in the firm's messages. Both will strengthen long-term return on investment from detailing. Thus:
Communication of complete (including both favorable and unfavorable) therapy information in sales calls may affect more positively the firm's long-term return on investment from detailing than just communicating favorable therapy information.
The effect postulated in P7a is larger in the case of therapies for life-threatening illnesses than in the case of non-life-threatening illnesses.
The relationship postulated in P7a is larger in hospital environments than in outpatient environments.
In P7b and P7c, we conjecture that the effect of disclosure of complete information may be contingent on whether the disease is life threatening and on the physician's institutional setting. Agents confronted with a decision of high importance attach a greater value to information (Celsi and Olson 1988). Therefore, physicians’ preference for more complete information, even if unfavorable, over ambiguity will be higher in the case of life-threatening diseases than in the case of non-life-threatening diseases. For example, there is more value in reducing ambiguity about the side effects of chemotherapy, even if it concerns an increased probability of pneumonia versus an increased probability of insomnia caused by antihistamines. As we argued previously, practitioners in hospitals may have a higher return on legitimacy than general practitioners in the outpatient environment. Revealing unfavorable information together with favorable information enhances a sales representative's legitimacy.
There are several possible tests of P7a–P7c. IMS Health's U.S. panel data include data on which attributes of a drug were discussed in a sales call. Adding information on how drugs in a category compare on each of these attributes may reveal whether favorable rather than unfavorable attributes were discussed. Several individual firms have records on which studies were covered in sales calls, which can reveal whether unfavorable studies were covered. The return on investment from long-term detailing can be regressed on both types of data to test the propositions. Longitudinal experiments can also be conducted to test the propositions, in which physicians or medical school students are detailed within a simulation.
Communication management
Although communication efforts of life sciences firms may target both consumers and physicians, the budgets dedicated to the former group are more than ten times larger than the budgets dedicated to the latter (Kremer et al. 2008), and from the interviews we held with practitioners, direct-to-consumer advertising (DTCA) is also the most challenging. The academic literature on DTCA (Berndt et al. 1995; Bowman, Heilman, and Seetharaman 2004; Iizuka and Jin 2005; Narayanan, Desiraju, and Chintagunta 2004; Wosinka 2005) mostly examines overall effectiveness of DTCA and yields the following preliminary generalization:
DTCA has a positive effect on (a) the number of patients seeing a physician for the respective disease for which a therapy is advertised and (b) total category-level demand in the category of the therapy that is advertised.
Further research on other potential outcomes of DTCA, such as its effect on brand choice, would be fruitful because it is fraught with debate. Iizuka and Jin (2005) and Wosinska (2005) find that DTCA does not affect drug brand choice, while Berndt and colleagues (1995) and Narayanan, Desiraju, and Chintagunta (2004) find a positive effect of DTCA on drug brand choice. Such research could involve meta-analysis or the analysis of contingency frameworks.
An example of a contingency factor is the degree to which DTCA messages include favorable and unfavorable information. Although unfavorable information (e.g., information on serious side effects of therapy) may arouse consumers (Moorman 1990), it may also yield negative emotions that hinder information processing (Agrawal, Menon, and Aaker 2007; Keller 1999). Thus:
The effect of DTCA on brand-level demand is higher the more the advertisement depicts favorable, rather than unfavorable, therapy information.
At the same time, no study develops a process view on the effects of DTCA on the demand for a specific therapy. The process involves DTCA triggering a patient's request for a therapy at the physician's office, which the physician can accommodate or not. The role of patient requests and the factors that affect the degree to which the physician accommodates them are not addressed in the academic literature at this point (for an exception, see Venkataraman and Stremersch 2007). Developing such a process view may yield relevant insights for managers (e.g., on audience targeting). As an example, consider audience gender. Prior research has shown that women are more concerned about their health (Verbrugge 1985) and interact more assertively in health care settings (Kaplan et al. 1995) than men and that physicians are more empathic to female than male patients (Hooper et al. 1982). Consequently, DTCA may more easily trigger requests among women, and female requests may be more easily accommodated by physicians than male requests. Thus:
The effect of DTCA on brand-level demand is higher among female viewers than among male viewers.
Many other boundary conditions can be formulated on aspects such as the type of disease and patient-physician relationships, all of which may inform ad content and target audience decisions of firms. Data availability on DTCA is high. Secondary data sources include ACNielsen and TNS Media. Both data types can be connected with aggregate-level sales data (e.g., from IMS Health) or panel-level data (e.g., from IMS Health or Verispan). In addition, experimental studies may have high potential because they may reveal underlying psychological processes.
Stimulating patient compliance
As our survey results show, life sciences firms undervalue the importance of stimulating patient compliance, from both a patient welfare and a profit perspective. Our interviews with managers revealed that they consider their impact on patient compliance minimal, though they believe that it is mostly affected by the provider in his or her interaction with the patient. In contrast, our survey among providers and payers shows that they believe that life sciences firms’ efforts to stimulate patient compliance may have important effects on patient welfare.
Despite its high relevance, academic research has not studied the role of the life sciences firm in patient compliance in depth. Prior research has found that provider expertise (Dellande, Gilly, and Graham 2004), the attitudinal homophily between patient and provider (Dellande, Gilly, and Graham 2004), the frequency of contact between patient and provider (Bowman, Heilman, and Seetharaman 2004), reminder messages (Becker and Rosenstock 1984; Rosenstock 1985), and the burden of therapy (Kahn et al. 1997; Kahn and Luce 2003, 2006) all affect patient compliance. The only research that exists on how life sciences firms may affect patient compliance examines warning labels. For example, Ferguson, Discenza, and Miller (1987) find that warning labels that include information on the consequences of poor compliance are effective.
Today, life sciences firms sporadically institute new types of compliance programs, the effectiveness of which remains void of academic scrutiny. We categorize such compliance programs in technology-enabled and customer relationship management– (CRM-) enabled programs.
Such CRM-enabled programs typically used in practice are direct mail or call campaigns. Pfizer has developed a “Staying on Track” CRM program for its statin drug Lipitor (Arnold 2004). Such programs monitor patients’ disease and refill status, motivate patients to stay on therapy regimen, and provide patients with therapy risk-related information tailored to the stage of therapy with their specific symptoms and motivations (Hopfield, Linden, and Tevelow 2006).
Technology-enabled programs include a technological device to remind patients to take their pills. Bang & Olufsen Medicon's blister card-based “The Helping Hand” gives a visual indication of therapy compliance through red or green LEDs (light-emitting diodes) as soon as a blister is inserted into the device. Another example is “SIMPill,” a smart pill bottle that reminds patients through SMS (short message service) that they have forgotten to take their medicine.
Both types of programs connect to different behavioral rationales for poor compliance: a patient's belief in self-efficacy and mindfulness. A patient's belief in self-efficacy refers to the belief of being capable of carrying through the prescribed therapy, and mindfulness refers to awareness of actions to be taken (Keller 2006). Customer relationship management-enabled programs promote a patient's belief in self-efficacy, and technology-enabled programs promote mindfulness. The potential of CRM programs to promote mindfulness is limited because the reminder frequency within a CRM program is unable to match therapy frequency (one or multiple therapy occurrences a day). Conversely, technology programs cannot offer the patient interpersonal coaching (e.g., Bandura 1982) to stay on therapy.
Given their differential behavioral rationales, the effectiveness of both programs is likely to depend on factors such as disease complexity and symptom salience. First, the more complex a disease, the higher is the likelihood that poor compliance is driven by disbelief in self-efficacy. As such, CRM-enabled programs can effectively reduce such uncertainty, but technology-enabled programs cannot. Second, the less salient the symptoms of a disease (e.g., the flu is a disease with salient symptoms and high cholesterol is a disease with low salience), the more compliance will be driven by mindfulness. When salience is low, technology-enabled programs will be more effective in stimulating compliance than CRM-enabled programs.
As disease complexity increases, CRM-enabled compliance programs increase in effectiveness to stimulate patient compliance, compared with technology-enabled compliance programs.
As symptom salience decreases, technology-enabled compliance programs increase in effectiveness to stimulate patient compliance, compared with CRM-enabled compliance programs.
Further research might consider a broader array of contingency factors than those developed in these propositions. Such research promises to be impactful for both academia and practice, but at the same time, it is challenging to execute. Relatively few firms have instituted a compliance program, patient-level data are difficult to obtain, and patients self-select into a program (which may cause sample selection issues). One method may be to conduct a conjoint experiment using physicians as informants on patient behavior. In such a conjoint experiment, program design factors could be manipulated, and their effect on patient compliance (as informed by the physician) could be estimated. Test-retest reliability and comparison with actual cases could further support the validity of such an approach. A more demanding alternative is cooperation with a life sciences firm that is open to a field experiment, including a longitudinal survey to the compliance program participants. More generally, the field of compliance would benefit from extensive survey research across patient-physician relationships because compliance is intrinsically embedded in this relationship.
Conclusion
Some industries require industry-specific knowledge development because they have unique characteristics that yield specific challenges for marketers. In this research, we aim to advocate such knowledge development for life sciences marketing. This article has implications for both life sciences marketing practice and academia.
Life Sciences Marketing Practice
Defining life sciences—to our surprise, no useful definition existed in the literature—proved to be challenging but, at the same time, eye-opening. Discerning clear boundaries to the domain enabled us to demarcate boundary areas, such as cosmetics-, device-, and food-based therapies, while integrating pharmaceuticals, biotechnology, and medical devices. With an increasing patient-centered view on health and personalization in medicine (see Camacho, Landsman, and Stremersch 2009), life sciences companies that develop an integrated view on patients’ health—rather than considering themselves a pharmaceutical, biotech, or medical devices company—will be best equipped for the future. Such integration is challenging. For example, with its historical structure along product divisions, Philips is challenged to develop an integrated view on opportunities in personalized medicine because such opportunities often stretch across the firm's personal care, medical devices, and consumer electronics divisions. Another related challenge for life sciences firms is to enhance their typical curative offering to include prevention, patient monitoring, and patient wellness. For example, firms with a diabetes franchise have moved historically from providing therapies (e.g., glucose) to providing monitoring devices (e.g., blood monitoring personal digital assistants) and, more recently, have faced the challenge to move into comprehensive care, which extends toward patient wellness (e.g., prevention and awareness on probable consequences of diabetes, such as blindness and wound care).
We also found substantial divergence in the evaluation of the importance of certain decision areas between life sciences marketers and health care payers and providers or, alternatively worded, between profits and patient welfare. While marketing managers emphasize the profit implications of sales force management, health care payers and providers emphasize patient welfare implications of life sciences firms’ actions to stimulate patient compliance. Such divergence gives rise to potential conflict in the health care value chain. As Singh, Jayanti, and Gannon (2008) argue, there is a strong need for the life sciences industry to escape such conflicting logic in the short run and increasingly adopt a partnership model, which could lead to enhanced legitimacy in the long run for life sciences firms.
Although further testing is needed, the generalizations and propositions we derive may provoke some firms to alter their marketing approach. For example, our propositions on opinion leaders encourage a dual-layer strategy of firms, such that at launch, they may rely on clinical leaders (mostly through research cooperation), and as experience with the therapy's side effects grows, market leaders may be actively involved (e.g., through specialized detailing). Although some firms already have such a dual-layer strategy, this is not (yet) common practice among life sciences firms. Another example is the differentiation between CRM-enabled and technology-enabled compliance programs. As the quotation from a Johnson & Johnson marketer in Table 1 shows, most life sciences firms are just beginning to consider compliance programs. Our propositions on compliance should encourage them to analyze the underlying characteristics of the disease and the patients to steer them to a suitable type of program. The review of prior research and the generalizations we derive from it may also inform practice. The positive expectations of many firms regarding the effect of DTCA on brand sales (note the high spending on DTCA among life sciences firms) are unrealistic in light of prior research findings.
Life Sciences Marketing Academia
This article shows that a bright future for this nascent field within marketing is imminent (Stremersch 2008). Among the many reasons are that (1) this context presents unique and often challenging problems, (2) for which high-quality data are available and (3) that have an impact that transcends the problems typically investigated by marketing scholars. On the supply side, universities are likely to invest considerable research funds in life sciences marketing as a research program that transcends various schools (business, medicine, economics), creates vast societal influence (regarding public policy, firms, the press, and the public at large), and does not have a pure for-profit nature (compared with other business school research).
We have demarcated the boundaries of this new domain; categorized the main decisions of life sciences marketers; and provided generalizations, propositions, and research directions to stimulate and steer research in this nascent field. As with the advent of any new field, there are as many cynics who claim that nothing is fundamentally different about life sciences marketing and that conventional insights can easily be extended to such markets without adaptation as there are enthusiasts who embrace these markets as being as different as the moon is from the earth. The former group often finds a dominant argument in the data-driven nature of the original contributions to life sciences marketing. However, in itself, this is not a reason an industry cannot be guided by different principles, thus leading to unique challenges. The same applies to the argument that some challenges are also present in other industries, in a slightly modified form. In the dialectic tradition, we try to build the case for the enthusiasts. Early interest at conferences, in journals, and in MBA program offices seems to favor the enthusiasts. The least we have hopefully achieved with this article is to define the playing field on which cynics and enthusiasts will interact, both in research and in teaching.
Footnotes
Overview of Life Sciences Marketing Literature

| Authors | Decision Areas | Main Findings | Conceptual Framework | Method Used | Empirical Base |
|---|---|---|---|---|---|
|
|
|||||
| Sorescu, Chandy, and Prabhu (2007) | IAF | Pharmaceutical firms with large product capital assets are better at selecting targets with innovation potential and deploying this innovation potential. The performance consequences of this superiority in the selection and deployment of target firms manifests itself in long-term financial rewards to the acquiring firm. | Resource-based view of the firm | Ordinary least squares (OLS) regression model | 238 acquisitions in 7 countries (1992–2002) |
| Chandy et al. (2006) | TPO | Firms that (1) focus on a moderate number of ideas in areas of importance and in which they have expertise and (2) deliberate for a moderate length of time on promising ideas have the highest conversion ability. | Problem solving | Discrete choice model | 322 drug ideas by 38 firms (1980–1985) |
| Prabhu, Chandy, and Ellis (2005) | IAF | Innovation outcomes of acquisitions are driven by the preacquisition knowledge of the acquirer and its similarity with the target's knowledge. | Knowledge-based view of the firm | Distributed-lag model | 35 pharmaceutical firms that acquired 157 targets (1988–1997) |
| Moorman, Du, and Mela (2005) | TP | Firms can make strategic use of regulation by thinking about costs and benefits of regulation relative to competition. The introduction of the Nutrition Label and Education Act (NLEA) (Public Law 101–535) led to (1) an increase in small-share firm exits and (2) a greater increase in distribution for large-share firms. No concurrent increase in price by large-share firms following the NLEA was observed. | Economics of information | Random effects probit on longitudinal quasi-experimental data | Universal Product Codes at the firm and brand levels for 109 categories from 2186 firms (Supermarket Review data) and for 265 categories from 29,374 firms (Infoscan) per year (1991, 1993, and 1995) |
| Wuyts, Dutta, and Stremersch (2004) | IAF | Alliance portfolio technological diversity has a positive affect on incremental and radical innovation output but has a negative direct effect on profitability. Repeated partnering has a positive effect on radical innovation and a curvilinear effect on profitability. Alliance portfolio size has a positive effect on incremental innovation output and firm profitability. | Knowledge-based view of the firm | Negative binomial and OLS regression model | 991 R&D agreements (1985–1998) |
| Sorescu, Chandy, and Prabhu (2003) | TPO | Firms that provide higher per-product levels of marketing and technology support obtain much greater financial rewards from their radical innovations than other firms. Firms that have greater depth and breadth in their product portfolio also gain more from their radical innovations. | Risk- and resource-based view of the firm | Random effects Poisson model | 255 breakthroughs introduced by 66 publicly traded firms (1991–2000) |
| Moorman and Slotegraaf (1999) | TP | Product marketing and technology capabilities coinfluence the degree to which firms improve the quality of their brands and the speed of these improvements. Capabilities’ most valuable characteristic is to serve as flexible strategic options consistent with a changing environment. | Resource-based view of the firm and economics of information | Regression on longitudinal quasi-experimental data | 124 brands across 22 categories (1991–1993, 1994–1996) |
| Moorman (1998) | TP | Marketers respond to the introduction of the NLEA by changing the quality of their brands and extensions, thus occupying distinct strategic positions. It also shifts healthy brands away from competing on price. Conversely, nonhealthy brands rely more on price promotion post-NLEA. | Economics of information | Regression on longitudinal quasi-experimental data | 269 consumers pre-NLEA, 212 post-NLEA, 124 products (1987–1996) |
|
|
|||||
| Aboulnasr et al. (2008) | GMET | The likelihood of competitive product response to radical innovation is substantially higher when the introducing firm is large or when it derives a larger part of its revenues from the introduction market. The response is greatest when the radical innovation is introduced in a small market by a large firm. | New product growth | Hazard model | 52 radical product innovations introduced by 32 different companies in 27 therapeutic categories (1997–2001) |
| Rao, Chandy, and Prabhu (2008) | GMET | New biotech ventures that acquire legitimacy externally by forming alliances with established firms gain more from their new products than new ventures that do not form such alliances. Among new ventures that do not form alliances, those that acquire legitimacy internally by creating a history of product launches or by hiring reputed executives or scientists gain more from their new products than those that do not. Pursuit of external legitimacy by firms that already have internal legitimacy leads to lower rewards to innovation. | New product growth | Maximum likelihood estimation and OLS regressions | 93 FDA-approved biotech product introductions (1982–2002) |
| Akçura, Gönül, and Petrova (2004) | GMET | Price promotions may be deficient as a tool to increase market share in over-the-counter leg-and-back pain relievers. | Choice behavior with learning | Bayesian learning model with Kaiman filter | 3519 purchase observation in panel of 69 consumers of over-the-counter leg-and-back pain relievers (1993–1995) |
| Desiraju, Nair, and Chintagunta (2004) | GMET | Developing countries have lower diffusion speeds than and maximum penetration levels relative to developed countries. Laggard developed countries have higher speeds. Laggard developing countries do not have higher diffusion speeds. Per-capita expenditures on health care have a positive effect on diffusion speed (particularly for developed countries). Higher prices tend to decrease diffusion speed. | New product growth | Hierarchical Bayesian diffusion model | Newly launched antidepressant drugs in 15 countries (1987–1993) |
| DeSarbo et al. (2001) | GMET | The specialist-physician population can be split into three segments with respect to the stage of adoption of innovations in a therapeutic category. | Market information mapping | Latent structure spatial model | Top 7 brands prescribed among 258 specialists |
| Shankar, Carpenter, and Krishnamurthi (1999) | GMET | Growth-stage entrants reach their asymptotic sales level faster than pioneers or mature-stage entrants. They are not hurt by competitor diffusion and enjoy a greater response to perceived product quality than pioneers and mature-stage entrants. Pioneers reach their asymptotic sales levels more slowly than later entrants. Mature-stage entrants are most disadvantaged. Buyers are most responsive to pioneer marketing efforts. | New product growth | Dynamic brand sales model | 29 ethical brands in 6 therapeutic areas (1970s, 1980s) |
| Shankar, Carpenter, and Krishnamurthi (1998) | GMET | Compared with pioneers or noninnovative late movers, innovative late movers can create a sustainable advantage by enjoying higher market potential and higher repeat purchase rates. They grow faster than the pioneer, slowing the pioneer's diffusion and reducing the pioneer's marketing effectiveness. They are advantaged asymmetrically; their diffusion can hurt other brands’ sales, but their sales are not affected by competitors. Noninnovative late movers face smaller potential markets, lower repeat rates, and less marketing effectiveness than the pioneer. | New product growth | Generalization of the Bass diffusion model for brand sales | 13 ethical brands in 2 chronic ailment therapeutic categories (1970s, 1980s) |
| Shankar (1997) | GMET | A pioneer that adopts a follower (leader) role with respect to a marketing-mix variable in a static (growing) market and witnesses a decrease (increase) in own elasticity and margin after a new entry should accommodate (retaliate) in that variable. | New product growth | Game theory | Full category of chronic care ethical drugs (1970s, 1980s) |
|
|
|||||
| Chintagunta and Desiraju (2005) | SFM | There is considerable heterogeneity in preferences and market response for pricing and detailing across markets, which favors a regional approach to strategy. The effects of within- and across-market interactions vary across markets and across brands within a market. | Competitive marketing-mix interactions | Category sales and market share model | Antidepressant sales (1988–1999) |
| Wosinska (2005) | CM, SPC | The impact of DTCA on patient compliance is small in economic terms, the effect spills over to other brands, and in certain cases the effect may decrease average compliance rates. | Compliance behavior | Negative binomial model | Panel of 16,011 patients, 123,736 gaps between prescriptions (1996–1999) |
| Bowman, Heilman, and Seetharaman (2004) | CM, SPC | Mindfulness is a predictor of patient compliance. Patients are most at risk for noncompliance right after and some duration after a medical treatment. Satisfaction with efficacy is a better predictor of compliance than satisfaction with side effects or costs. Advertising shows a mixed influence. Direct channel shoppers are more compliant than indirect channel consumers. | Compliance behavior | OLS regression and Tobit models | 6238 patients making 44,345 purchases (2001–2002) |
| Manchanda, Rossi, and Chintagunta (2004) | SFM | High-volume physicians are detailed to a greater extent than low-volume physicians without regard to responsiveness to detailing. Unresponsive but high-volume physicians are detailed the most. | Prescription behavior | Hierarchical Bayesian estimation of negative binomial model | Monthly prescription volume of 1000 U.S. physicians for one drug, the name of which is not revealed (1999–2001) |
| Narayanan, Desiraju, and Chintagunta (2004) | SFM, CM | DTCA and detailing affect pharmaceutical demand synergistically Detailing raises price elasticity and has a higher return on investment than does DTCA. The interaction between price and detailing is negative. DTCA has a significant effect on category sales, but detailing does not. Both detailing and DTCA affect brand shares, and detailing has a much greater effect than DTCA. | Prescription behavior | Category sales and market share model | Monthly antihistamine prescriptions in the United States (1993–2002) |
| Gönül et al. (2001) | SFM | Physicians show fairly limited price sensitivity. Detailing and samples have a mostly informative effect on physicians. Physicians with a relatively large number of Medicare or health management organization patients are less influenced by promotion than other physicians. | Prescription behavior | Latent class multinomial logit model | 1785 patient visits to 157 physicians in the United States for a chronic condition common among the elderly (1991–1994) |
| Ahearne, Gruen, and Jarvis (1999) | SFM | Perceived salesperson attractiveness has a significant, positive effect on salesperson performance, but the effect diminishes as the length of the salesperson-physician relationship increases. Attractiveness leads to higher levels of perceived communication ability, likability, expertise, and trustworthiness. | Social psychology | Regression analysis on survey data | 339 U.S. physicians |
| Dekimpe and Hanssens (1999) | SFM, CM | Strategic scenarios (business as usual, hysteresis in response, escalation, and evolving business practice) have a major impact on marketing effectiveness and long-term profitability. Multivariate persistence measures are proposed to identify which of four scenarios is taking place. | Marketing strategy response | Vector autoregressive models | Monthly sample of five years for a pioneering and challenger brand in one pharmaceutical category in the United States |
| Hahn et al. (1994) | CM | Effectiveness of communication on product trial is related mainly to product quality and market growth. Effectiveness of word of mouth is associated with product class characteristics and market competitiveness. The effect of product trial on repeat purchases is related to product quality and market characteristics, such as size, growth, competitiveness, and familiarity. | New product growth | Four-segment trial-repeat model | 21 ethical drugs in 7 therapeutic categories, launched from 1981 to 1984 |
| Mantrala, Sinha, and Zoltners (1994) | SFM | The agency theoretic model-based approach can assist management in evaluating and optimally structuring multiproduct sales quota bonus plans. | Agency theory | Utility model on conjoint data | 12 sales people in a single company |
| Parsons and Vanden Abeele (1981) | SFM | Sales call elasticity varies over time as a function of the collateral material (samples and handouts). | Marketing strategy response | OLS regression model | Monthly sales for an established drug within the steroid group of prophylactic medicines for women in Belgium (1973–1974) |
Notes: Decision areas: CM = communication management, GMET = global market entry timing, IAF = innovation alliance formation, SFM = sales force management, SPC = stimulating patient compliance, TP = therapy positioning, and TPO = therapy pipeline optimization. Note that no research was published (yet) on key opinion leader selection in the five major marketing journals we studied.
Overview of Health Psychology Literature
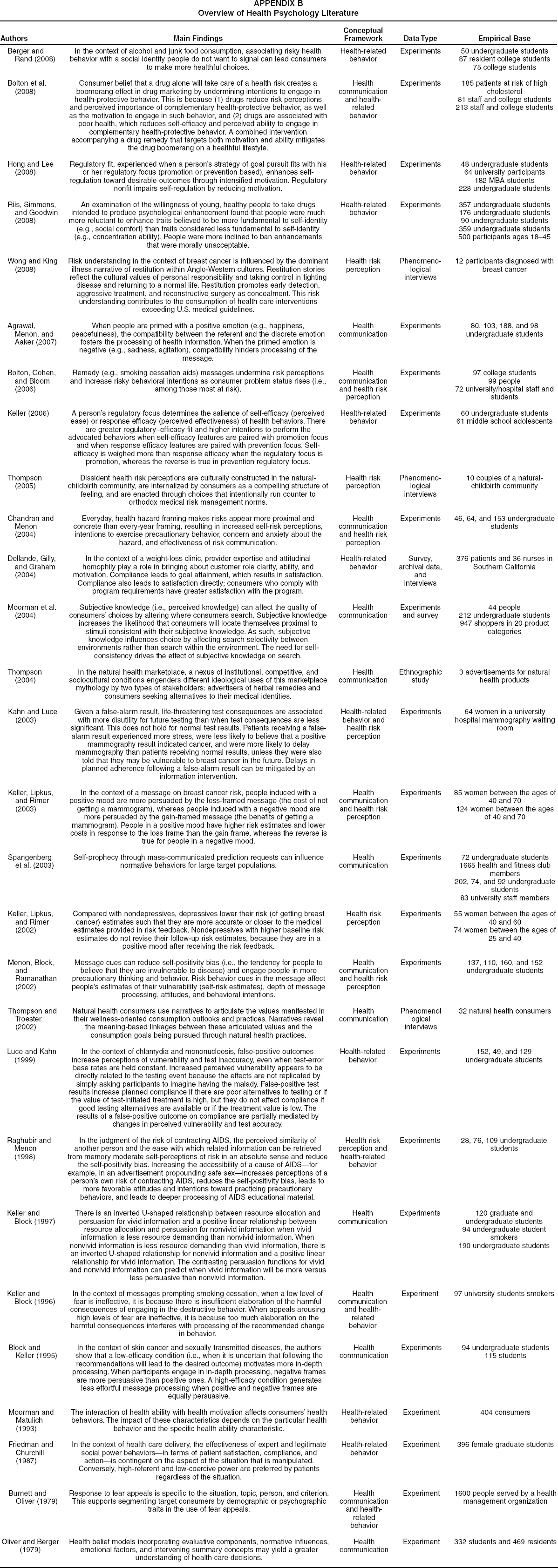
| Authors | Main Findings | Conceptual Framework | Data Type | Empirical Base |
|---|---|---|---|---|
| Berger and Rand (2008) | In the context of alcohol and junk food consumption, associating risky health behavior with a social identity people do not want to signal can lead consumers to make more healthful choices. | Health-related behavior | Experiments | 50 undergraduate students 87 resident college students 75 college students |
| Bolton et al. (2008) | Consumer belief that a drug alone will take care of a health risk creates a boomerang effect in drug marketing by undermining intentions to engage in health-protective behavior. This is because (1) drugs reduce risk perceptions and perceived importance of complementary health-protective behavior, as well as the motivation to engage in such behavior, and (2) drugs are associated with poor health, which reduces self-efficacy and perceived ability to engage in complementary health-protective behavior. A combined intervention accompanying a drug remedy that targets both motivation and ability mitigates the drug boomerang on a healthful lifestyle. | Health communication and health-related behavior | Experiments | 185 patients at risk of high cholesterol 81 staff and college students 213 staff and college students |
| Hong and Lee (2008) | Regulatory fit, experienced when a person's strategy of goal pursuit fits with his or her regulatory focus (promotion or prevention based), enhances self-regulation toward desirable outcomes through intensified motivation. Regulatory nonfit impairs self-regulation by reducing motivation. | Health-related behavior | Experiments | 48 undergraduate students 64 university participants 182 MBA students 228 undergraduate students |
| Riis, Simmons, and Goodwin (2008) | An examination of the willingness of young, healthy people to take drugs intended to produce psychological enhancement found that people were much more reluctant to enhance traits believed to be more fundamental to self-identity (e.g., social comfort) than traits considered less fundamental to self-identity (e.g., concentration ability). People were more inclined to ban enhancements that were morally unacceptable. | Health-related behavior | Experiments | 357 undergraduate students 176 undergraduate students 90 undergraduate students 359 undergraduate students 500 participants ages 18–45 |
| Wong and King (2008) | Risk understanding in the context of breast cancer is influenced by the dominant illness narrative of restitution within Anglo-Western cultures. Restitution stories reflect the cultural values of personal responsibility and taking control in fighting disease and returning to a normal life. Restitution promotes early detection, aggressive treatment, and reconstructive surgery as concealment. This risk understanding contributes to the consumption of health care interventions exceeding U.S. medical guidelines. | Health risk perception | Phenomenological interviews | 12 participants diagnosed with breast cancer |
| Agrawal, Menon, and Aaker (2007) | When people are primed with a positive emotion (e.g., happiness, peacefulness), the compatibility between the referent and the discrete emotion fosters the processing of health information. When the primed emotion is negative (e.g., sadness, agitation), compatibility hinders processing of the message. | Health communication | Experiments | 80, 103, 188, and 98 undergraduate students |
| Bolton, Cohen, and Bloom (2006) | Remedy (e.g., smoking cessation aids) messages undermine risk perceptions and increase risky behavioral intentions as consumer problem status rises (i.e., among those most at risk). | Health communication and health risk perception | Experiments | 97 college students 99 people 72 university/hospital staff and students |
| Keller (2006) | A person's regulatory focus determines the salience of self-efficacy (perceived ease) or response efficacy (perceived effectiveness) of health behaviors. There are greater regulatory-efficacy fit and higher intentions to perform the advocated behaviors when self-efficacy features are paired with promotion focus and when response efficacy features are paired with prevention focus. Self-efficacy is weighed more than response efficacy when the regulatory focus is promotion, whereas the reverse is true in prevention regulatory focus. | Health-related behavior | Experiments | 60 undergraduate students 61 middle school adolescents |
| Thompson (2005) | Dissident health risk perceptions are culturally constructed in the natural-childbirth community, are internalized by consumers as a compelling structure of feeling, and are enacted through choices that intentionally run counter to orthodox medical risk management norms. | Health risk perception | Phenomenological interviews | 10 couples of a natural-childbirth community |
| Chandran and Menon (2004) | Everyday, health hazard framing makes risks appear more proximal and concrete than every-year framing, resulting in increased self-risk perceptions, intentions to exercise precautionary behavior, concern and anxiety about the hazard, and effectiveness of risk communication. | Health communication and health risk perception | Experiments | 46, 64, and 153 undergraduate students |
| Dellande, Gilly, and Graham (2004) | In the context of a weight-loss clinic, provider expertise and attitudinal homophily play a role in bringing about customer role clarity, ability, and motivation. Compliance leads to goal attainment, which results in satisfaction. Compliance also leads to satisfaction directly; consumers who comply with program requirements have greater satisfaction with the program. | Health-related behavior | Survey, archival data, and interviews | 376 patients and 36 nurses in Southern California |
| Moorman et al. (2004) | Subjective knowledge (i.e., perceived knowledge) can affect the quality of consumers’ choices by altering where consumers search. Subjective knowledge increases the likelihood that consumers will locate themselves proximal to stimuli consistent with their subjective knowledge. As such, subjective knowledge influences choice by affecting search selectivity between environments rather than search within the environment. The need for self-consistency drives the effect of subjective knowledge on search. | Health communication | Experiments and survey | 44 people 212 undergraduate students 947 shoppers in 20 product categories |
| Thompson (2004) | In the natural health marketplace, a nexus of institutional, competitive, and sociocultural conditions engenders different ideological uses of this marketplace mythology by two types of stakeholders: advertisers of herbal remedies and consumers seeking alternatives to their medical identities. | Health communication | Ethnographic study | 3 advertisements for natural health products |
| Kahn and Luce (2003) | Given a false-alarm result, life-threatening test consequences are associated with more disutility for future testing than when test consequences are less significant. This does not hold for normal test results. Patients receiving a false-alarm result experienced more stress, were less likely to believe that a positive mammography result indicated cancer, and were more likely to delay mammography than patients receiving normal results, unless they were also told that they may be vulnerable to breast cancer in the future. Delays in planned adherence following a false-alarm result can be mitigated by an information intervention. | Health-related behavior and health risk perception | Experiments | 64 women in a university hospital mammography waiting room |
| Keller, Lipkus, and Rimer (2003) | In the context of a message on breast cancer risk, people induced with a positive mood are more persuaded by the loss-framed message (the cost of not getting a mammogram), whereas people induced with a negative mood are more persuaded by the gain-framed message (the benefits of getting a mammogram). People in a positive mood have higher risk estimates and lower costs in response to the loss frame than the gain frame, whereas the reverse is true for people in a negative mood. | Health communication and health risk perception | Experiments | 85 women between the ages of 40 and 70 124 women between the ages of 40 and 70 |
| Spangenberg et al. (2003) | Self-prophecy through mass-communicated prediction requests can influence normative behaviors for large target populations. | Health communication | Experiments | 72 undergraduate students 1665 health and fitness club members 202, 74, and 92 undergraduate students 83 university staff members |
| Keller, Lipkus, and Rimer (2002) | Compared with nondepressives, depressives lower their risk (of getting breast cancer) estimates such that they are more accurate or closer to the medical estimates provided in risk feedback. Nondepressives with higher baseline risk estimates do not revise their follow-up risk estimates, because they are in a positive mood after receiving the risk feedback. | Health risk perception | Experiments | 55 women between the ages of 40 and 60 74 women between the ages of 25 and 40 |
| Menon, Block, and Ramanathan (2002) | Message cues can reduce self-positivity bias (i.e., the tendency for people to believe that they are invulnerable to disease) and engage people in more precautionary thinking and behavior. Risk behavior cues in the message affect people's estimates of their vulnerability (self-risk estimates), depth of message processing, attitudes, and behavioral intentions. | Health communication and health risk perception | Experiments | 137, 110, 160, and 152 undergraduate students |
| Thompson and Troester (2002) | Natural health consumers use narratives to articulate the values manifested in their wellness-oriented consumption outlooks and practices. Narratives reveal the meaning-based linkages between these articulated values and the consumption goals being pursued through natural health practices. | Health communication | Phenomenological interviews | 32 natural health consumers |
| Luce and Kahn (1999) | In the context of chlamydia and mononucleosis, false-positive outcomes increase perceptions of vulnerability and test inaccuracy, even when test-error base rates are held constant. Increased perceived vulnerability appears to be directly related to the testing event because the effects are not replicated by simply asking participants to imagine having the malady. False-positive test results increase planned compliance if there are poor alternatives to testing or if the value of test-initiated treatment is high, but they do not affect compliance if good testing alternatives are available or if the treatment value is low. The results of a false-positive outcome on compliance are partially mediated by changes in perceived vulnerability and test accuracy. | Health-related behavior | Experiments | 152, 49, and 129 undergraduate students |
| Raghubir and Menon (1998) | In the judgment of the risk of contracting AIDS, the perceived similarity of another person and the ease with which related information can be retrieved from memory moderate self-perceptions of risk in an absolute sense and reduce the self-positivity bias. Increasing the accessibility of a cause of AIDS—for example, in an advertisement propounding safe sex—increases perceptions of a person's own risk of contracting AIDS, reduces the self-positivity bias, leads to more favorable attitudes and intentions toward practicing precautionary behaviors, and leads to deeper processing of AIDS educational material. | Health risk perception and health-related behavior | Experiments | 28, 76, 109 undergraduate students |
| Keller and Block (1997) | There is an inverted U-shaped relationship between resource allocation and persuasion for vivid information and a positive linear relationship between resource allocation and persuasion for nonvivid information when vivid information is less resource demanding than nonvivid information. When nonvivid information is less resource demanding than vivid information, there is an inverted U-shaped relationship for nonvivid information and a positive linear relationship for vivid information. The contrasting persuasion functions for vivid and nonvivid information can predict when vivid information will be more versus less persuasive than nonvivid information. | Health communication | Experiments | 120 graduate and undergraduate students 94 undergraduate student smokers 190 undergraduate students |
| Keller and Block (1996) | In the context of messages prompting smoking cessation, when a low level of fear is ineffective, it is because there is insufficient elaboration of the harmful consequences of engaging in the destructive behavior. When appeals arousing high levels of fear are ineffective, it is because too much elaboration on the harmful consequences interferes with processing of the recommended change in behavior. | Health communication and health-related behavior | Experiment | 97 university students smokers |
| Block and Keller (1995) | In the context of skin cancer and sexually transmitted diseases, the authors show that a low-efficacy condition (i.e., when it is uncertain that following the recommendations will lead to the desired outcome) motivates more in-depth processing. When participants engage in in-depth processing, negative frames are more persuasive than positive ones. A high-efficacy condition generates less effortful message processing when positive and negative frames are equally persuasive. | Health communication | Experiments | 94 undergraduate students 115 students |
| Moorman and Matulich (1993) | The interaction of health ability with health motivation affects consumers’ health behaviors. The impact of these characteristics depends on the particular health behavior and the specific health ability characteristic. | Health-related behavior | Experiment | 404 consumers |
| Friedman and Churchill (1987) | In the context of health care delivery, the effectiveness of expert and legitimate social power behaviors—in terms of patient satisfaction, compliance, and action—is contingent on the aspect of the situation that is manipulated. Conversely, high-referent and low-coercive power are preferred by patients regardless of the situation. | Health-related behavior | Experiment | 396 female graduate students |
| Burnett and Oliver (1979) | Response to fear appeals is specific to the situation, topic, person, and criterion. This supports segmenting target consumers by demographic or psychographic traits in the use of fear appeals. | Health communication and health-related behavior | Experiment | 1600 people served by a health management organization |
| Oliver and Berger (1979) | Health belief models incorporating evaluative components, normative influences, emotional factors, and intervening summary concepts may yield a greater understanding of health care decisions. | Health communication | Experiment | 332 students and 469 residents |