
Abstract
Purpose:
To evaluate the safety and patterns of use of targeted renal therapy (TRT) with the Benephit system. TRT, the delivery of therapeutic agents directly to the kidneys by renal arterial infusion, has the advantage of providing a higher local effective dose with potentially greater renal effects, while limiting systemic adverse effects due to renal first-pass elimination.
Methods:
The Benephit System Renal Infusion Therapy (Be-RITe!) Multicenter Registry was a post-market registry following patients treated using the Benephit systems for TRT. The registry enrolled 501 patients (332 men; mean age 72.2±9.5 years) at high risk for contrast-induced nephropathy (CIN) during coronary or peripheral angiography/intervention or cardiovascular surgery. The Mehran score was used to compare the actual to predicted incidence of CIN within 48 hours post procedure.
Results:
Bilateral renal artery cannulation was successful in 94.2%, with a mean cannulation time of 2.0 minutes. Either fenoldopam mesylate, sodium bicarbonate, alprostadil, or B-type natriuretic peptide (BNP) was infused for 184±212 minutes. Mean creatinine levels did not change significantly (baseline, 24, and 48 hours post procedure: 1.95, 1.99, and 1.98 mg/dL, respectively; p=NS). In 285 patients who received TRT with fenoldopam and were followed for at least 48 hours, the incidence of CIN was 71% lower than predicted (8.1% actual CIN versus 28.0% predicted; p<0.0001). Only 4 (1.4%) patients required dialysis (versus the 2.6% predicted rate, p=NS).
Conclusion:
The Benephit system and TRT during coronary and endovascular procedures in patients at high risk for renal failure is simple to use and safe. With the infusion of intrarenal fenoldopam, the incidence of CIN was significantly lower than predicted by risk score calculations.
Keywords
With increasing use of radiographic contrast media in diagnostic and interventional procedures, contrast-induced nephropathy (CIN) has become an important cause of renal dysfunction, occurring in as many as 10% to 30% of patients who receive iodine-based contrast media.1-8 CIN is associated with extended hospitalizations, increased expense, and elevated in-hospital and long-term morbidity and mortality.1,4,9–11 has been suggested that coronary angiography is underutilized in elderly patients with chronic kidney disease due to fears of worsening renal function, despite the greater benefit of an invasive strategy in this patient group. 12 Having a tool that might decrease the risk of CIN and give patients and operators a greater sense of safety may improve care to these high-risk patients.
To date, however, no adjunctive pharmacological agent has proven effective for prevention or treatment of CIN other than adequate periprocedural hydration.13-17 Many potentially beneficial agents have failed to improve outcomes, despite a sound pathophysiological basis. One proposed theory for these failures is that many systemically administered agents may not achieve adequate drug levels in the renal vasculature without induction of adverse systemic side effects. Fenoldopam, a vasodilator that improves renal blood flow and thus was expected to protect from CIN, was not superior to placebo when infused systemically in the CONTRAST trial. 17 However, a significant number of patients in that study were not able to tolerate even low doses of fenoldopam due to drug-induced hypotension, which is by itself a strong risk factor for CIN.
In comparison to systemically administered agents, direct infusion of a drug selectively into the kidneys via the renal arteries, termed targeted renal therapy (TRT), may enhance renal action with fewer systemic side effects. TRT with fenoldopam has recently been shown to produce greater increases in glomerular filtration rate (GFR) with less systemic hypotension compared to same-dose intravenous fenoldopam in patients undergoing coronary angiography and intervention. 18
TRT may be used for the infusion of various medications to the kidneys in a wide variety of clinical situations. The Benephit System Renal Infusion Therapy Registry (Be-RITe!) was conducted to capture “real world” data on usage strategies, safety, and feasibility of the Benephit Infusion Systems to deliver TRT.
METHODS
Study Design
The Benephit System Renal Infusion Therapy Registry (Be-RITe!) was a retrospective, observational, post-market preference study designed to document the patterns of use, device performance characteristics, and safety in patients treated with either of the Benephit Infusion Systems (FlowMedica, Inc., Fremont, CA, USA). The protocol did not mandate any patient characteristics, drug treatments, or adjunct procedures; these were determined by the individual operating physicians and captured on the case report forms. Pre- and postprocedural fluids and periprocedural anticoagulation were left to the discretion of the operating physicians, including hydration and the use of N-acetylcysteine. The Institutional Review Board in each participating institution approved the registry protocol.
Patients
Between May 2004 and August 2007, 501 patients (332 men; mean age 72.2±9.5 years) were enrolled in the Be-RITe! Registry at 19 participating centers (Appendix). Inclusion/ exclusion criteria were left to the discretion of the treating physician. Eleven patients from the registry were previously reported.19,20 The baseline clinical characteristics of the patients enrolled in the registry (Table 1) reflected multiple significant comorbidities predisposing to the development of CIN.
Baseline Characteristics of 501 Patients Enrolled in the Registry
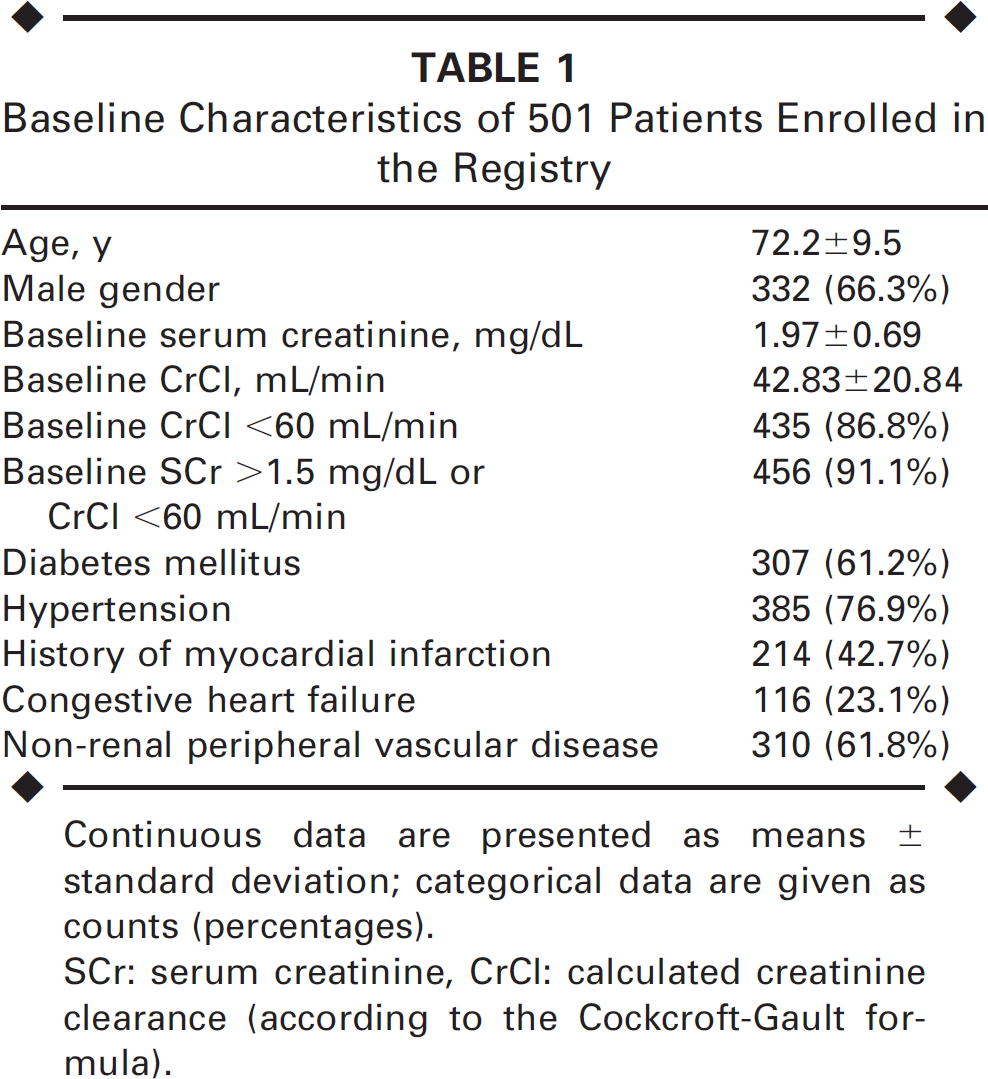
Continuous data are presented as means ± standard deviation; categorical data are given as counts (percentages).
SCr: serum creatinine, CrCl: calculated creatinine clearance (according to the Cockcroft-Gault formula).
Device Placement
The 2 types of Benephit infusion systems used in this registry, both approved by the Food and Drug Administration and Conformité Européene, were the coronary (CV) and the peripheral (PV) systems. The Benephit CV system (Fig. 1A) uses an 8-F introducer sheath with a unique Y hub that allows concurrent placement of the Benephit CV bifurcated renal artery infusion catheter and a coronary guide or diagnostic catheter (up to 6-F) through a single femoral access site. After placement of a short arterial sheath, aortography is performed using 5 to 10 mL of contrast through a pigtail diagnostic catheter to visualize the ostia of the renal arteries (Fig. 2A). The short sheath is exchanged for a 30- to 45-cm dual port, 8-F Benephit CV System introducer sheath (Fig. 2B). The Benephit CV bifurcated infusion catheter is then advanced through the side port of the delivery sheath and into place, simultaneously cannulating both renal arteries (Fig. 2C); the position may be confirmed by injection of ∼0.5 mL of diluted contrast through the bifurcated catheter lumen. Study drug administration is then immediately started through the infusion catheter. Angiography and intervention is performed by advancing diagnostic or guide catheters through the sheath via the second port (Fig. 2D).
In the setting of peripheral diagnostic or interventional procedures, surgical procedures, or procedures where TRT is performed outside of the catheterization lab or operating room, the Benephit PV Infusion System (Fig. 2B) is the system of choice. The Benephit PV system is a stand-alone system comprised of a 5-F introducer sheath and matching bifurcated infusion catheter, available in different lengths to accommodate femoral, brachial, or radial arterial accesses. In these cases, the Benephit PV 5-F sheath is often placed directly in the area of the renal arteries via a femoral, brachial, or radial approach; initial angiography is performed directly through the sheath. The Benephit PV bifurcated infusion catheter is then placed in a manner similar to that described for the CV system. Peripheral diagnostic or interventional device access, if desired, is performed via an alternate arterial access.
Intrarenal Drug Administration
Intrarenal drug infusions via the Benephit catheters were generally performed for at least the duration of the peripheral or coronary angiography or interventional or surgical procedure. In some cases, the operators continued the intrarenal infusion beyond the procedure, providing a TRT “tail” infusion. The “tail” infusion was usually accomplished using the Benephit PV system, as it is more flexible and tolerant to patient transfer from the catheterization laboratory or operating room table. The choice of medication infused, the dose, and the duration of administration were at the operator's discretion in the registry.

(A) Benephit CV and (B) Benephit PV.
To examine the potential efficacy of TRT with fenoldopam in preventing CIN, outcome data from a 285-patient subset receiving this drug and followed for at least 48 hours post procedure were compared to a “control” rate of predicted CIN calculated according to the Mehran score. 21 This score incorporates 8 integer-weighted variables: hypotension, intra-aortic balloon pump (IABP) use, congestive heart failure (CHF), chronic kidney disease, diabetes, age, anemia, and volume of contrast. When added together, the sum of these integers can predict CIN or in-hospital hemodialysis with reasonable discriminative accuracy (c-statistic 0.67). 21
Definitions
Chronic kidney disease was defined by a baseline serum creatinine >1.5 mg/dL or an estimated GFR <60 mL/min/1.73 m2 [Levey modified MDRD (Modification of Diet in Renal Disease) formula]. 22 CIN was defined as a 0.5-mg/dL or 25% increase in serum creatinine from baseline within 48 hours following contrast media administration. Anemia was defined using criteria specified by the World Health Organization: hematocrit <39% for men or <36% for women. Hypotension was defined as systolic blood pressure <80 mmHg for at least 1 hour requiring either inotropic or IABP support within 24 hours of the procedure. CHF was classified according to the New York Heart Association functional class III or IV symptoms.
Statistical Analysis
Actual observed rates of CIN and dialysis were compared with the expected rates of CIN and dialysis as predicted by the Mehran prediction score. 21 Risk score analysis included patients for whom serum creatinine was available at 48 hours.
Two-tailed Student t tests were used to compare continuous variables and a chi-square or Fisher exact test was used to compare categorical variables. Continuous data are presented as mean ± standard deviation or median and interquartile range (IQR); categorical data are presented as frequencies and percentages unless otherwise noted. P<0.05 was considered statistically significant for all tests.

Placement of the Benephit CV infusion catheter into both renal arteries. (
RESULTS
The patterns of use of TRT in the registry are described in Figure 3. In most of the patients (89.1%), TRT was given during a coronary or peripheral percutaneous procedure (34.6% and 54.5%, respectively). Almost a third (29%) of patients underwent percutaneous coronary intervention, while 45% had a peripheral percutaneous procedure. Seven percent of patients had emergent procedures for acute coronary syndromes. Iodixanol was the most common type of contrast media used (58%), followed by iopamidol (32%). The median total contrast volume used was 130.0 mL (IQR 100–175); a median of only 10 mL (IQR 5–10) of contrast was required for the placement of the Benephit Infusion System. In 52 (11%) patients, TRT was administrated during a cardiothoracic surgical procedure (n=34) or peripheral vascular surgery (n=18), without the administration of contrast (except the small volume necessary to place a Benephit device). In 2 patients, TRT was also applied in the intensive care unit for treatment of acute renal failure, such as postoperative worsening renal function and fluid overload associated with cardiorenal syndrome and CHF.
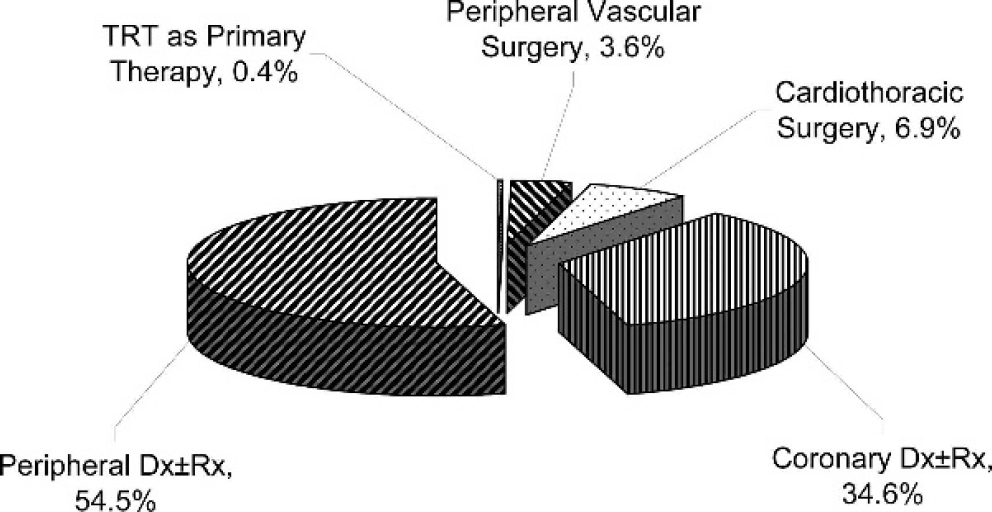
Use of TRT in the Be-RITe! Registry
Device Performance and Safety
In all patients, at least 1 renal artery was successfully accessed with the Benephit catheter; bilateral cannulation was successful in 94% of patients. Inability to cannulate the renal arteries bilaterally in the remaining 6% of patients was attributed to one or more of the following: severe aortoiliac tortuosity, renal artery stenosis, extremely acute renal artery takeoff anatomy, and interference from a renal stent. The mean time for cannulation was 1.95±1.62 minutes. After cannulation, drug infusion was successful in 100% of patients; no problems were encountered with catheter removal. Catheter-related complications were very rare, with only 1 (0.2%) case of renal artery dissection that was immediately stented without compromising renal function or causing long-term sequelae. The incidence of groin hematoma was 0.6%.
Targeted Renal Therapy
Intrarenal fenoldopam (0.05–0.80 Μg/kg/min) was used in 90.6% of patients; intrarenal sodium bicarbonate (1M, 154 mEq/L; 1-2 mL/kg/h) in 3.4%; alprostadil (20–80 ng/kg/h) in 2.4% of patients; and B-type natriuretic peptide (BNP; 0.01–0.20 Μμg/kg/min) in 0.4%. In 3.2% of the patients, the operators did not report infusion through the Benephit catheter. The mean duration of intrarenal drug infusion was 184±212 minutes. The intrarenal administration of fenoldopam was tolerated well in almost all the patients, including those with CHF and those treated with IABP. Significant hypotension with need to discontinue the infusion of fenoldopam and short-term administration of an inotropic agent occurred in only 1 (0.2%) patient.
Parameters of Efficacy
The efficacy of intrarenal administration of fenoldopam to prevent CIN was evaluated by comparing recorded outcomes to historical controls using a published predictor scoring system. Since it may take 48 hours to see a rise in the serum creatinine, the focus was on a subgroup of 285 patients who where given intrarenal fenoldopam for CIN prophylaxis and followed for at least 48 hours after a coronary or peripheral contrast-associated procedure. The 285 patients who received fenoldopam were a high-risk population: 96% had baseline serum creatinine >1.5 mg/dL or creatinine clearance <60 mL/min. The median baseline serum creatinine was 1.9 mg/dL (IQR 1.7–2.1); mean baseline creatinine clearance was 37.0±11.6 mL/min. A total of 92% of the patients had an intervention (coronary or peripheral), and 8% had a diagnostic angiogram only. The mean volume of contrast used was 145±78 mL. The Benephit infusion catheter was successfully advanced into both renal arteries in 95% of these patients, while the remaining 5% had only 1 renal artery cannulated. Fenoldopam was infused directly into the renal arteries at a dose of 0.1 to 0.8 Μg/kg/min (mean 0.38) for a mean 199±212 minutes.
The mean serum creatinine levels did not change significantly during the follow-up period from baseline (2.01±0.58 mg/dL) to the levels at 24 hours (2.03±0.59 mg/dL, p=0.038) or 48 hours (2.00±0.73, p=0.56). Based on the Mehran risk score (Table 2), 21 the predicted rate of CIN in this group of high-risk patients was 28.0% (Fig. 4). The actual observed rate of CIN in this group was only 8.1%, 71% less than predicted (p<0.0001). The predicted and actual observed rates of patients requiring dialysis were 2.6% and 1.4% (reduction of 46%, p=0.23). When comparing the predicted to actual rates of CIN in different groups of risk (Fig. 5), the relative reduction of CIN provided by TRT was significantly greater in patients with high and very high risk of developing CIN (risk score ≥11). Due to the small sample sizes, no meaningful comparisons could be made for other agent subgroups (sodium bicarbonate, alprostadil, BNP, or postsurgical procedures).
Relative Significance of Risk and Actual Rates in 285 Patients Who Received TRT With Fenoldopam and Were Followed for 48 Hours
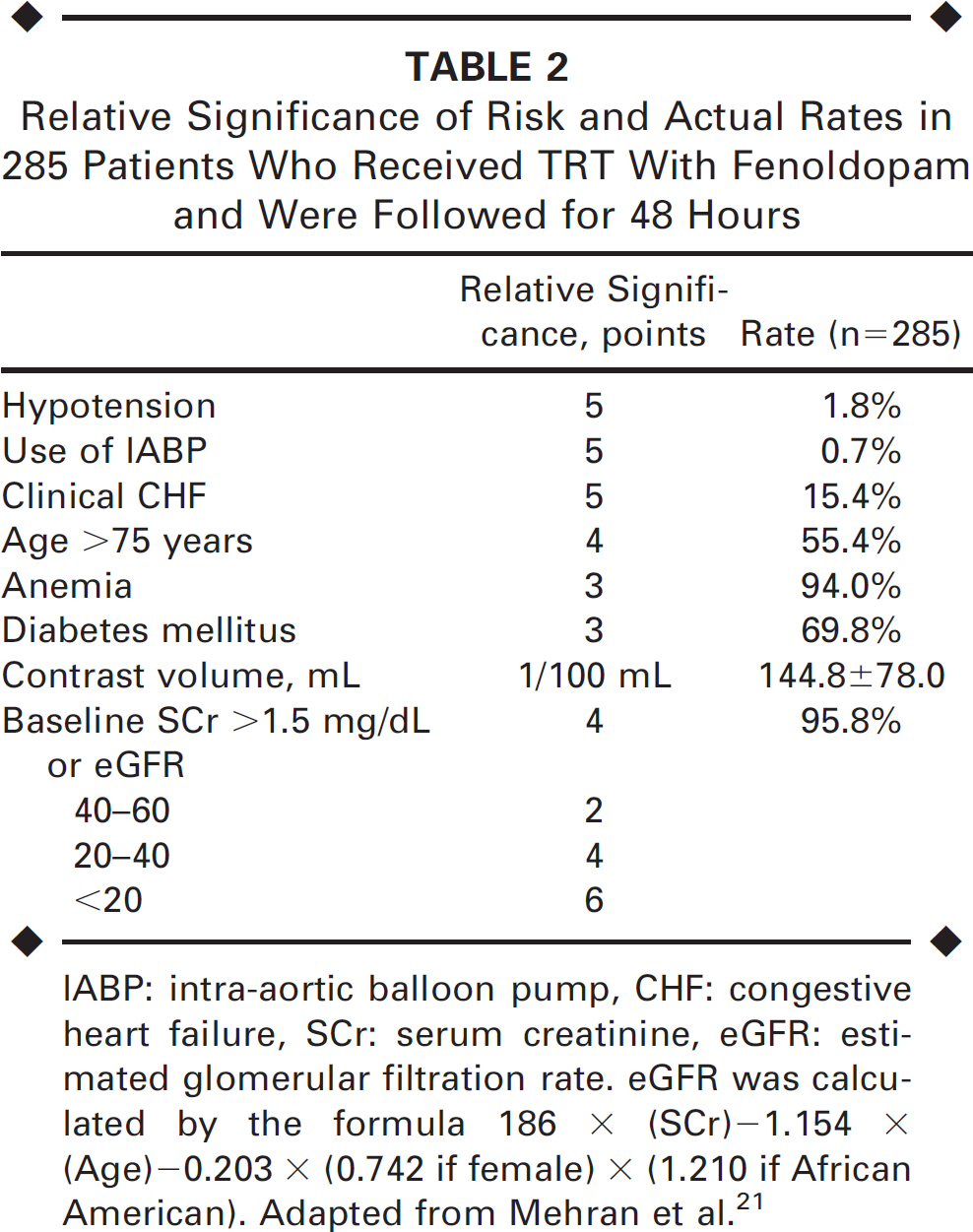
IABP: intra-aortic balloon pump, CHF: congestive heart failure, SCr: serum creatinine, eGFR: estimated glomerular filtration rate. eGFR was calculated by the formula 186 × (SCr)–1.154 × (Age)–0.203 × (0.742 if female) × (1.210 if African American). Adapted from Mehran et al. 21
DISCUSSION
Capturing the experience of 39 operators from 19 centers, the Be-RITe! Registry has demonstrated that use of the Benephit catheter is feasible and safe and appears to be a promising preventive strategy for CIN. The Benephit systems were consistently easy to use, with quick and successful cannulation of both renal arteries in the majority of patients (a third of bilateral cannulations accomplished in <1 minute), with an extremely low rate of complications.
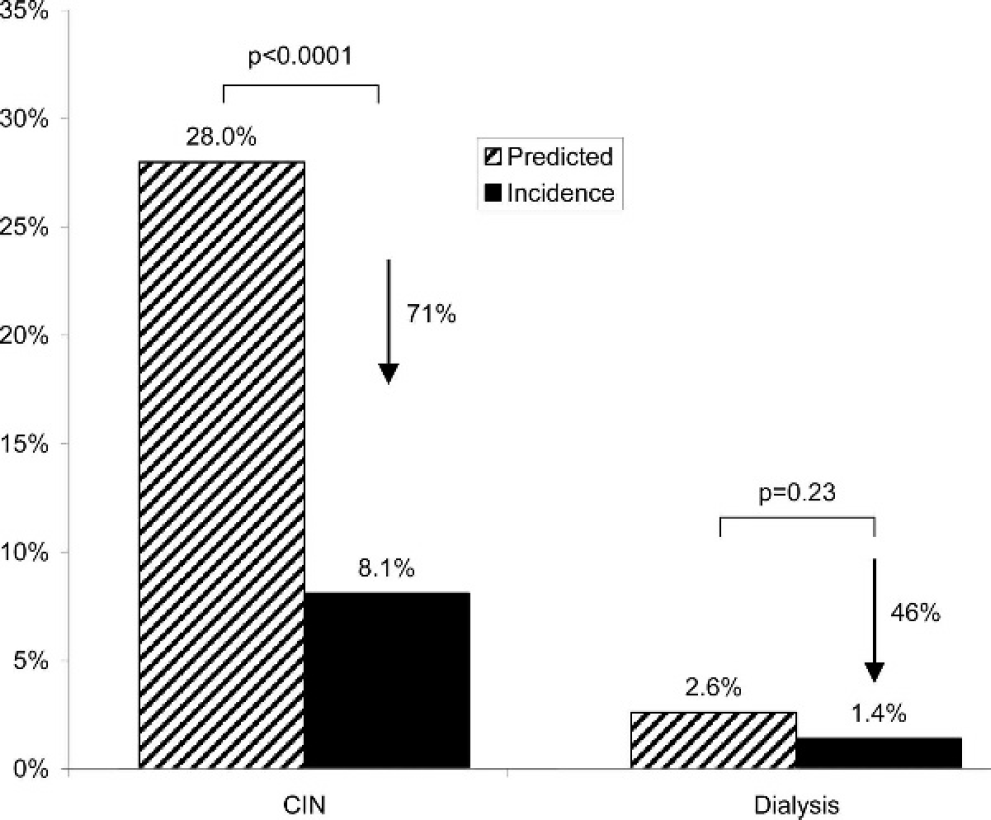
Observed versus predicted rates of CIN and dialysis in 285 patients who had coronary or peripheral contrast-related procedures and were followed for 48 hours. The predicted rates are based on the Mehran risk score. 21
The TRT strategy of administrating treatment agents directly to the kidneys via the renal arteries has multiple advantages. Administration of drugs with favorable renal effects and renal elimination pharmacokinetics offers superiority over intravenous therapy. 18 Targeting of drugs directly to the kidneys may deliver higher local drug levels and bypass renal first-pass elimination, minimizing overall systemic exposure and systemic side effects. Thus, a potent renal vasodilator such as fenoldopam may be administrated in higher doses than could be tolerated by intravenous administration, with minimal effect on blood pressure, while ultimately elevating the GFR. 18 In addition, the TRT strategy for preventing CIN with the Benephit system has potential applications in treating other situations, such as management of non-contrast-related acute renal failure, CHF, cardiorenal syndrome, and others.
Another potential advantage to TRT is that therapy can be initiated and therapeutic benefit can commence just prior to an interventional procedure without the need for the pretreatment that is required for current therapies (e.g., hydration). This may have special importance in emergent situations such as acute myocardial infarction, where the risk of developing CIN is especially high. 23
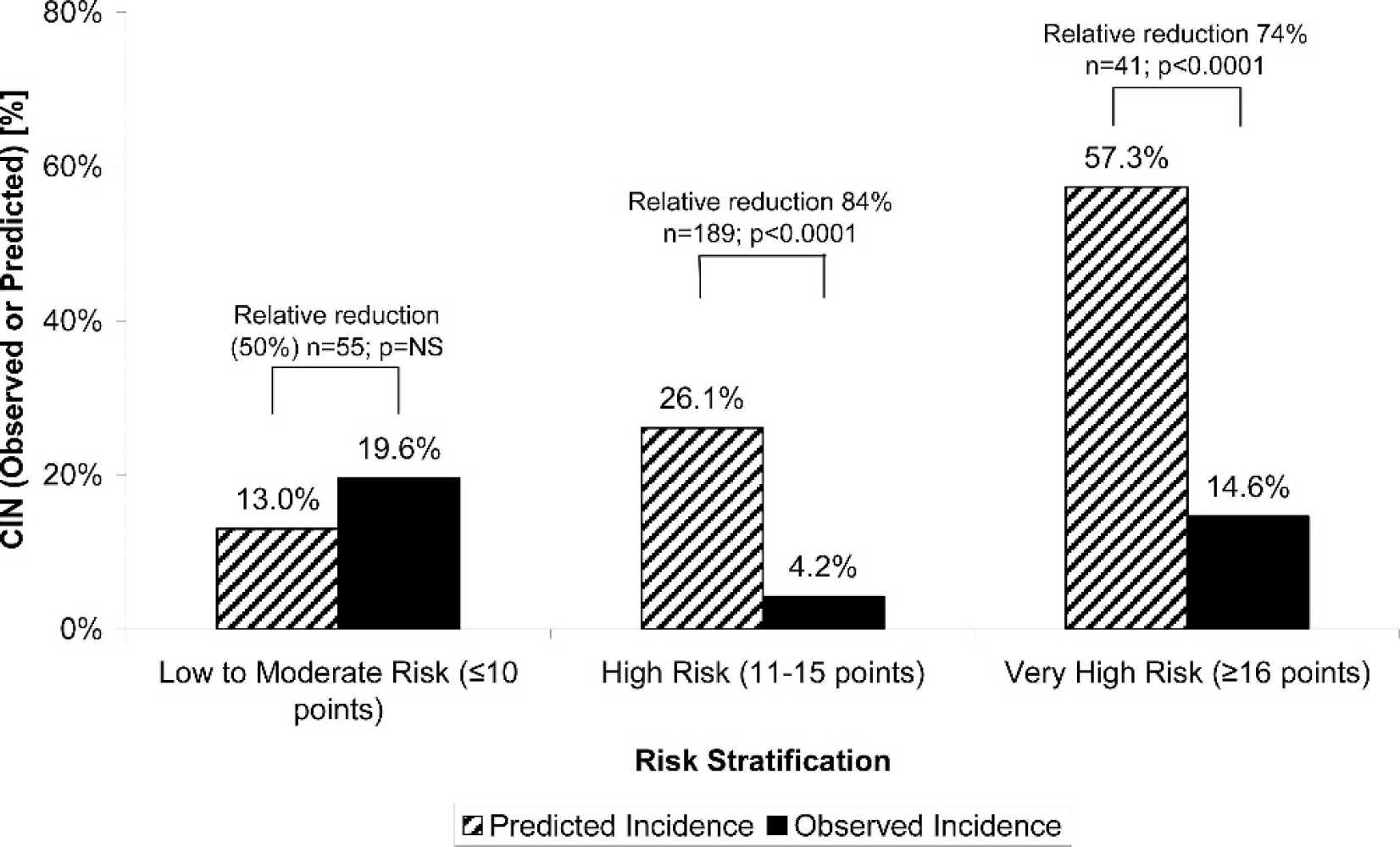
Predicated and actual rates of CIN according to the degree of risk score.
The Be-RITe! Registry was a post-market, retrospective assessment of the use of the Benephit infusion systems, so there were no pre-defined inclusion or exclusion criteria; all the management decisions (except for the instructions on how to use the Benephit devices) were left to the operators' discretion, thus achieving a “real world” usage profile. The vast majority of the patients had objective risk factors for developing CIN. The operators elected to use the TRT strategy and chose a drug designed to reduce the risk of CIN.
All 4 different agents that were infused via TRT in the Registry have pathophysiological arguments for the prevention of CIN. Alprostadil, a prostaglandin E1 analogue, may be effective in attenuating contrast-induced, prostaglandin-mediated vasoconstriction.24-27 B-type natriuretic peptide is a recombinant form of human BND that has been hypothesized to increase renal blood flow, GFR, diuresis, and natriuresis.28,29 Hydration and fluid volume expansion with the addition of bicarbonate has been suggested as a protective measure against CIN.30,31 It is unknown whether there is an optimal or maximal degree of alkalization, but some operators elected to infuse bicarbonate through the Benephit system directly into the renal artery. Patients receiving TRT with alprostadil, BNP, or bicarbonate had lower risks of CIN than the rest of the Registry group, but the small numbers in these groups that were followed for 48 hours did not allow efficacy evaluation of these strategies. No drug-related complications were observed with these other agents.
We focused on the largest registry subgroup of patients (n=285) who received TRT with fenoldopam during coronary or peripheral contrast-related procedures for CIN prophylaxis and were followed for 48 hours. These patients had high rates of multiple risk factors for CIN, as manifested by an average calculated predicted CIN rate of 28.0% based on the Mehran stratification risk score. 21 This score, easy to calculate, is developed from a large dataset of 8357 patients in whom multivariate logistic regression identified 8 independent predictors of CIN. We have used these parameters with their relative weight to estimate and predict the rate of CIN that would have occurred in these patients in the absence of intrarenal fenoldopam. To have a compatible control, we used the same criteria for the definition of CIN (0.5-mg/dL or 25% increase in serum creatinine within 48 hours following contrast administration). Using this risk stratification model as a historical control, TRT with fenoldopam resulted in a significant 71% lower rate of CIN than predicted. Likewise, the rate of patients who required dialysis was 46% lower than predicted, which did not reach statistical significance due to the low number of events.
Fenoldopam mesylate is a selective dopamine agonist acting on the dopaminergic D1 receptors in the renal arteries to increase blood flow to the renal medulla. 32 In an animal model, it has been shown that fenoldopam protects from CIN by preventing the decrease in GFR after contrast administration.33,34 Despite initial enthusiasm,35,36 2 other randomized trials failed to demonstrate a CIN-preventive effect of intravenous fenoldopam.17,37 In the large CONTRAST trial, 315 patients were randomized to intravenous administration of 0.05 to 0.1 Μg/kg/min or placebo prior to, during, and after coronary percutaneous intervention. No differences were found in the rates of CIN between the fenoldopam and placebo groups (33.6% versus 30.1%, respectively, p=NS). Two major issues should be discussed regarding this study. Despite relatively low doses of fenoldopam, ∼25% of the patients did not tolerate the resultant reduction in blood pressure, and the infusion had to be stopped. Furthermore, the resultant hypotension could have contributed to the slightly higher rate of CIN with fenoldopam. Second, the dose administered in the CONTRAST study may be insufficient to significantly increase GFR.
Our results with intrarenal fenoldopam appear more promising compared to the intravenous route used in the CONTRAST trial. When infused directly into the renal arteries, up to 90% of the fenoldopam is eliminated by the kidneys, so direct renal artery fenoldopam infusion allows administration of a higher dose while reducing the hypotensive side effect of systemic vasodilation. Furthermore, the average dose of fenoldopam given in the registry (0.4 Μg/kg/min) was 4 to 8 times higher than the doses administered in the CONTRAST trial, thus providing an even higher local effect. In a carefully designed and executed phase 1 study, Teirstein et al. 18 compared selective intrarenal fenoldopam administration to the intravenous route. This study found a significant first-pass renal clearance of fenoldopam that resulted in lower systemic plasma drug concentrations. In contrast to intravenous fenoldopam, which significantly decreased blood pressure, intrarenal fenoldopam did not decrease blood pressure more than the control. Selective intrarenal fenoldopam administration also produced greater increases in renal plasma flow and GFR than comparable doses of fenoldopam administered intravenously, consistent with the hypothesis that a greater local concentration of the drug yields greater renal effects. 18
The patients enrolled in the Be-RITe! Registry had extremely low rates of complications. There was only one case of renal artery dissection, which was treated without further morbidity. None of the patients in the registry had peripheral distal embolization. Prior to the insertion of the Benephit catheter, an abdominal angiogram is done to evaluate the exact location of the renal arteries and to exclude overt aortic atherosclerosis or renal artery stenosis. This enables the operators to have the catheter in place more quickly, with fewer maneuvers inside the aorta, reducing the risk of potential atheromatous embolization.
Limitations
This study was limited by its retrospective and observational design. The use of, or type of, TRT was not randomized, and a historical risk stratification model was employed posthoc as a control to evaluate the effectiveness of TRT with fenoldopam in protection from CIN. Unmeasured confounding variables, such as hydration volume and duration, treatment with N-acetylcysteine, proteinuria, urine output, and nephrotoxic medications, among others, may have accounted for some of the differences in outcomes. The control risk stratification model did not include these factors. 21
In addition, the population from which the risk stratification score was derived was somewhat different from that of the Be-RITe! Registry, limiting the validity of this score for the present study. The patients in the Registry had more comorbid conditions and were at higher risk for developing CIN than the patients on whom the predictive risk model was based; thus, the risk stratification score may have underestimated the advantage of TRT with fenoldopam. The predicted risk of 28% is similar to the rate of CIN observed in the CONTRAST trial, which had similar patient characteristics. 17
This analysis assessed a follow-up period of only 48 hours. Although the rise in serum creatinine occurs within the first 24 to 48 hours after exposure to contrast in many patients, the absence of data on serum creatinine beyond 48 hours after exposure may have resulted in underestimation of CIN (both predicted and observed). However, it is doubtful that a delayed creatinine elevation in patients without a significant rise within 48 hours will be clinically significant. 38
Conclusion
In the Be-RITe! Registry, TRT with the Benephit Infusion Systems appears safe and easy to perform during both endovascular and surgical procedures. Intrarenally-delivered fenoldopam with this device was associated with a decreased incidence of CIN compared to calculated predicted rates. Other renal-active medications used with TRT deserve further exploration. A randomized double-blind study is planned to further test the impact of TRT with fenoldopam over current strategies to protect from CIN.
APPENDIX
Centers and investigators in the Be-RITe! Registry: Brigham and Women's Hospital, Boston, MA: Campbell Rogers; Scripps Green Hospital, San Diego, CA: Paul Teirstein, Curtiss Stinis, Steve Lee, Justin Levisay, Matthew Price, Rafael Valencia, and Raphava Gollapudi; Stanford Medical Center, Stanford, CA: William Fearon and Alan Yeung; University of North Carolina, Chapel Hill, NC: Mauricio Cohen; New York Presbyterian Hospital, Columbia University, New York, NY: Giora Weisz, Jeffrey W. Moses, Martin B. Leon, Roxana Mehran, Gregg W. Stone, and Paul Teirstein; Brotman Medical Center, Culver City, CA: Hooman Madyoon; ML Sacco, Milan, Italy: Paolo Danna; Florida Hospital and Orlando Regional Medical Center, Orlando, FL: Barry Weinstock; North Florida Regional Medical Center, Gainesville, FL: Bret Wiechmann; Toyohashi Heart Center, Tokyo, Japan: Yoshihisa Kinoshita and Akira Murata; Providence Heart and Vascular Institute, Portland, OR: Naveen Sachdev; Dartmouth Hitchcock Medical Center, Lebanon, NH: Craig Thompson; Cardiovascular Institute of the South, Houma and Lafayette, LA: David Allie, Craig Walker, and Raghotham Patlola; University of South Alabama, Mobile, AL: Dimitras Kyriazis, Ronald O'Gorman, and Carl Maltese; Osceola Regional Medical Center, Kissimmee, FL: Padma Raju, Milimar Arsov, and Patrick Mathias; Regional Cardiology Consultants, Jackson, TN: Wood Deming; Charleston Area Medical Center, Charleston, WV: Laura Findeiss; Owensboro Heart and Vascular, Owensboro, KY: Kishor Vora.