
Abstract
Purpose:
To investigate the incidence, anatomical location, and clinical impact of fractures and/or compression of infrapopliteal balloon-expandable metal stents implanted for critical limb ischemia (CLI) treatment.
Methods:
This prospective study included 63 CLI patients (45 men; mean age 71.3±9.5 years) who had been treated with infrapopliteal angioplasty and stent placement for 191 lesions in 84 limbs. In all, 369 stents (296 stainless steel and 73 cobalt-chromium alloy) were implanted; 239 were placed overlapping in tandem lesions. Mean length of the overall stented segment was 4.4±6.3 cm (range 1.6–14.0). Stents were located in the tibioperoneal (n=34), anterior tibial (n=195), posterior tibial (n=63), and peroneal (n=77) arteries. Follow-up consisted of digital subtraction angiography and infrapopliteal radiography imaging at 2 different angles. Evaluation of stents for the presence of fracture and/or compression was done after digital processing at the highest possible magnification. Stent fractures were defined according to published standards, whereas compression was classified as severe shape alteration and/or collapse of the stent mesh. Angiographic restenosis was based on a 50% threshold.
Results:
Mean follow-up was 15±11 months (range 6–60). Image analysis detected 1 (0.3%) severe stent fracture (complete separation and misalignment of stent struts) and 11 (3.0%) stent compressions. Infrapopliteal stent fracture and compressions were associated with increased artery restenosis [100% (12/12) versus 47.3% (169/357), p<0.001] and an increased rate of clinical deterioration and clinically-driven reinterventions [41.7% (5/12 limbs) versus 19.4% (14/72 limbs), p=0.04]. The single fracture and most of the compressions were located in the distal third of the anterior tibial artery.
Conclusion:
Stent fractures and compressions of infrapopliteal balloon-expandable metal stents are infrequent. However, they may be related to increased restenosis.
Keywords
The engineering of low-profile, thin-strut bare or drug-eluting metal stents has radically improved the endovascular treatment of heavily diseased low-caliber infrapopliteal arteries in patients suffering from critical limb ischemia (CLI). 1 Several controlled and cohort studies have provided strong proof-of-concept for infrapopliteal stenting in the amelioration of CLI disease.1-3 Bare or drug-eluting stents, initially designed for the coronary arteries, have been successfully applied in the tibial arteries of CLI patients, augmenting technical success and primary patency and achieving encouraging wound healing and limb salvage rates. 4
Nonetheless, despite continuous developments in stent materials and alloy designs, there have been several reports of stent fracture or compression involving a variety of vascular and extravascular areas treated with percutaneous stent placement.5-12 Investigators have hypothesized and documented a significant correlation between stent fracture or compression and diminished vessel patency since the early ages of stenting.13,14 However, systematic clinical trials evaluating mechanical stent fatigue and failure have been limited to the coronary and superficial femoral arteries, the latter being notorious for its unique biomechanical forces and associated increased stent fracture and restenosis rates.13-15 Until now, no clinical trial has addressed the incidence and clinical significance of these metal fatigue events in the infrapopliteal arteries. We report a prospective single-center study evaluating the incidence, anatomical location, and association with restenosis of fractures and/or compression in coronary balloon-expandable metal stents implanted in the infrapopliteal arteries.
METHODS
Study Design
Under a protocol approved by the hospital's Ethical and Scientific Committee, candidates were recruited from a prospective database of CLI patients who had been treated with infrapopliteal endovascular techniques.2,3 Only patients who complied with the prescribed antiplatelet medication (clopidogrel 75 mg/d and aspirin 100 mg/d for 6 months and either aspirin or clopidogrel thereafter) were eligible for this study. Non-ambulatory patients, cases with incomplete angiographic or clinical records, and patients with complex infrapopliteal bifurcation or trifurcation stenting procedures were excluded. The follow-up protocol in all infrapopliteal stent patients included digital subtraction angiography (DSA) below the knee at 6 months, 1 year, and annually thereafter to promptly identify restenosis and impending arterial occlusion.
Patient Enrollment
Between September 2006 and January 2008, 63 patients (45 men; mean age 71.3±9.5 years) who had previously been treated with angioplasty and infrapopliteal stenting gave informed consent and were enrolled in the study. Baseline clinical variables of the patients were extracted from the database (Table 1). In total, 84 limbs with 191 lesions had received 369 balloon-expandable coronary stents, specifically, 296 stainless-steel and 73 cobalt-chromium alloy designs. Among these, 239 stents were placed in tandem lesions in an overlapping manner (<5 mm). The majority of the stents (291, 79%) were a coated sirolimus-eluting (Cypher; Cordis, a Johnson & Johnson company, Miami Lakes, FL, USA) or an everolimus-eluting design (Xience, Abbott Vascular, Redwood City, CA, USA). Mean overall length of the stented lesion was 4.4±6.3 cm (range 1.6–14.0). Stents were located in the anterior tibial (195, 53%), posterior tibial (63, 17%), peroneal (77, 21%), and tibioperoneal (34, 9%) arteries (Table 2).
Baseline Demographics in 63 Critical Limb Ischemia (CLI) Patients
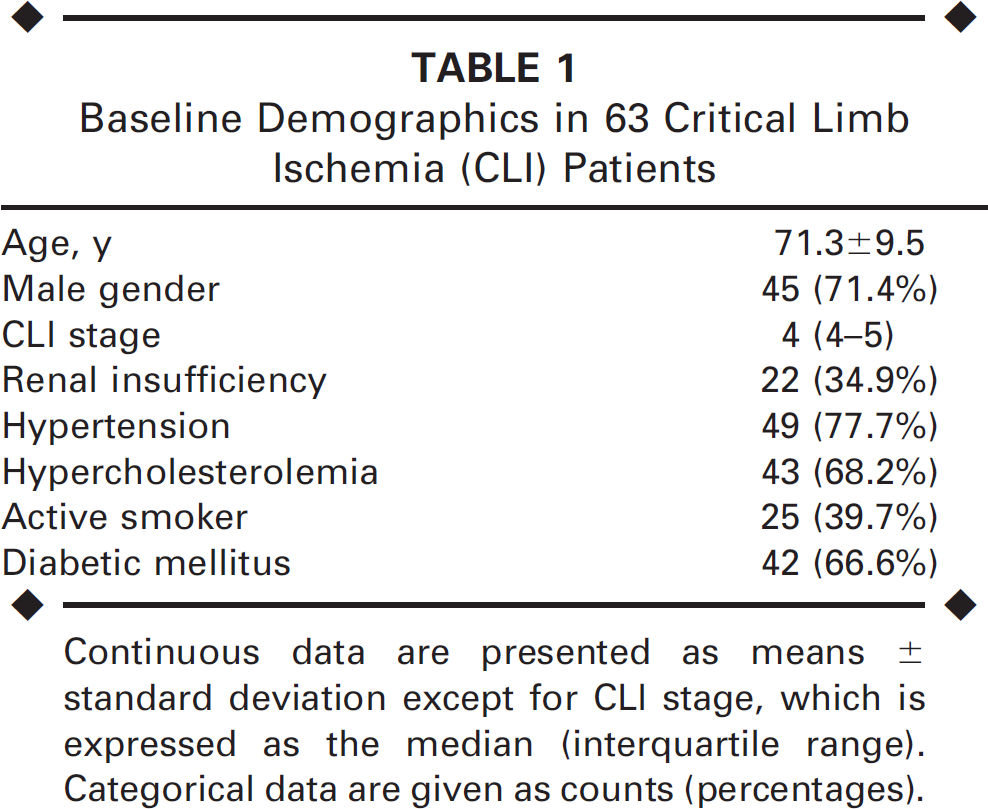
Continuous data are presented as means ± standard deviation except for CLI stage, which is expressed as the median (interquartile range). Categorical data are given as counts (percentages).
Anatomical Location of Infrapopliteal Balloon-Expandable Stents
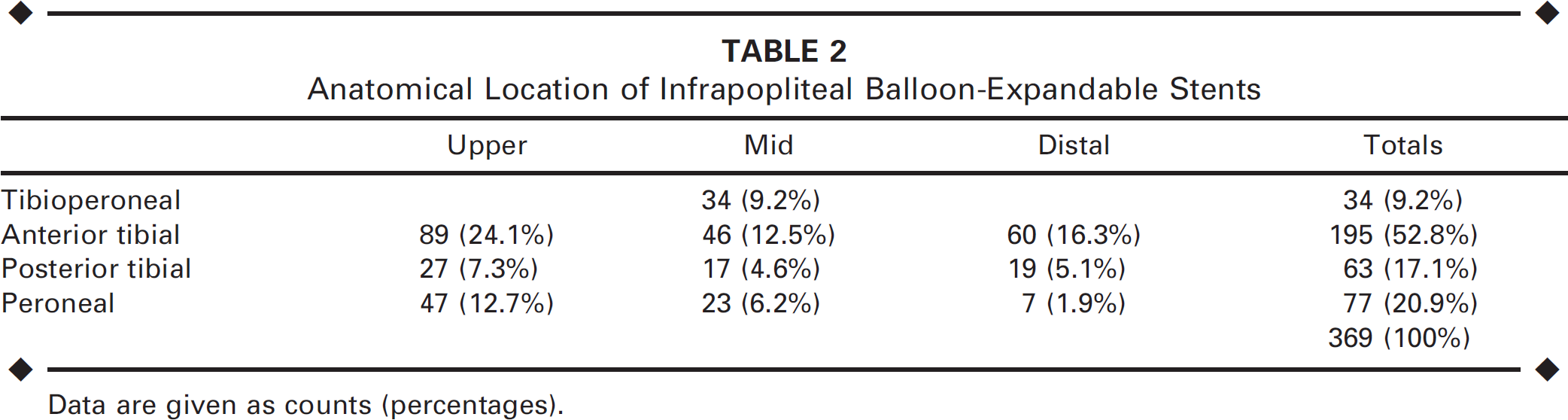
Data are given as counts (percentages).
Imaging Techniques and Definitions
Infrapopliteal radiographic imaging at 2 different angulations (>45% apart) was performed formed after completion of the scheduled DSA follow-up. Images were directly captured either from the angiography unit or from a digital radiographic imaging unit and saved in DICOM format. Digital images were then transferred to the Department of Medical Physics for processing using the Analyze PC image processing software (version 8.1; AnalyzeDirect, Inc., Lexana, KS, USA). The following spatial filters were applied: adaptive restoration (with an 8×8×1 kernel) and inhomogeneity correction (with a window value of 80).
Morphological characteristics of the stents were analyzed with regard to their type (bare or drug-eluting), arterial site, presence of eccentric or concentric vessel wall calcification, overlapping placement, diameter, and length. Evaluation of the stents for fracture and/or compression was done at the highest possible magnification. Stent fractures were graded according to 5 distinct types as proposed by Jaff et al., 15 whereas stent compression was defined as severe shape alteration and/or collapse of the strut interstitial matrix (Table 3). Arterial implantation sites were divided in 3 regions (upper, mid, and lower calf) to account for any anatomical differences and evaluate the different extrinsic forces applied on the metal stent struts from muscles, fibrous aponeuroses, and osseous structures surrounding or juxtaposing the infrapopliteal arteries. All documented cases of fractures or compressions were verified by comparison with archived baseline angiographic and fluoroscopic images from the day of the index infrapopliteal revascularization procedure.
Categories and Definitions of Stent Fractures and Deformations
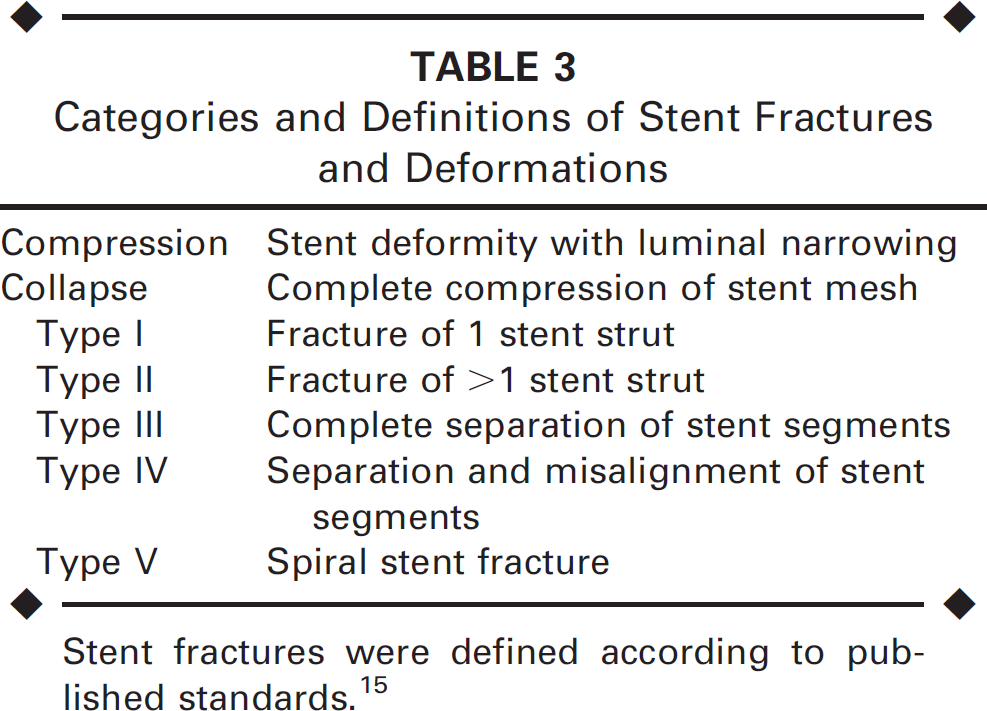
Stent fractures were defined according to published standards. 15
In addition, stent fractures and deformations were correlated with any site-specific angiographic restenosis, which was determined on a 50% threshold from the follow-up DSA imaging in the corresponding in-stent areas as previously described.2,3 All images and data were reviewed by 2 experienced interventional radiologists; consensus was reached in cases of ambiguous findings or borderline differences.
Statistical Analysis
Categorical variables were given as counts and percentages. Continuous variables were expressed as medians and the 25th/75th interquartile range or as means ± standard deviation if they passed the Kolmogorov-Smirnov normality test. Group comparisons were performed with application of the chi-square test. Multiple groups were compared using a 1-way analysis of variance test. The threshold of statistical significance was set at α=0.05.
RESULTS
Over a mean follow-up of 15±11 months (range 6–60), digital image analysis detected 12 (3.2%) cases of below-the-knee stent fracture and/or compression (Table 4) in the 369 stents. There was 1 (0.3%) severe grade IV stent fracture (complete separation of struts and misalignment of stent segments; Fig. 1) and 11 (3.0%) stent compressions (Fig. 2). There was no significant difference in the rate of stent fracture and/or compression between stainless-steel (9/296, 3.0%) and cobalt-chromium (3/75, 4.0%) stents (p=0.34). Likewise, there was no significant difference between drug-eluting (11/291, 3.8%) and bare metal (1/ 78, 1.3%) stents (p=0.13). The mean follow-up of the patient group that exhibited stent fracture or deformation (14±8 months) was not significantly different from that of the rest of the cohort (16±11 months).
Fractures and Deformations of Infrapopliteal Balloon-Expandable Stents
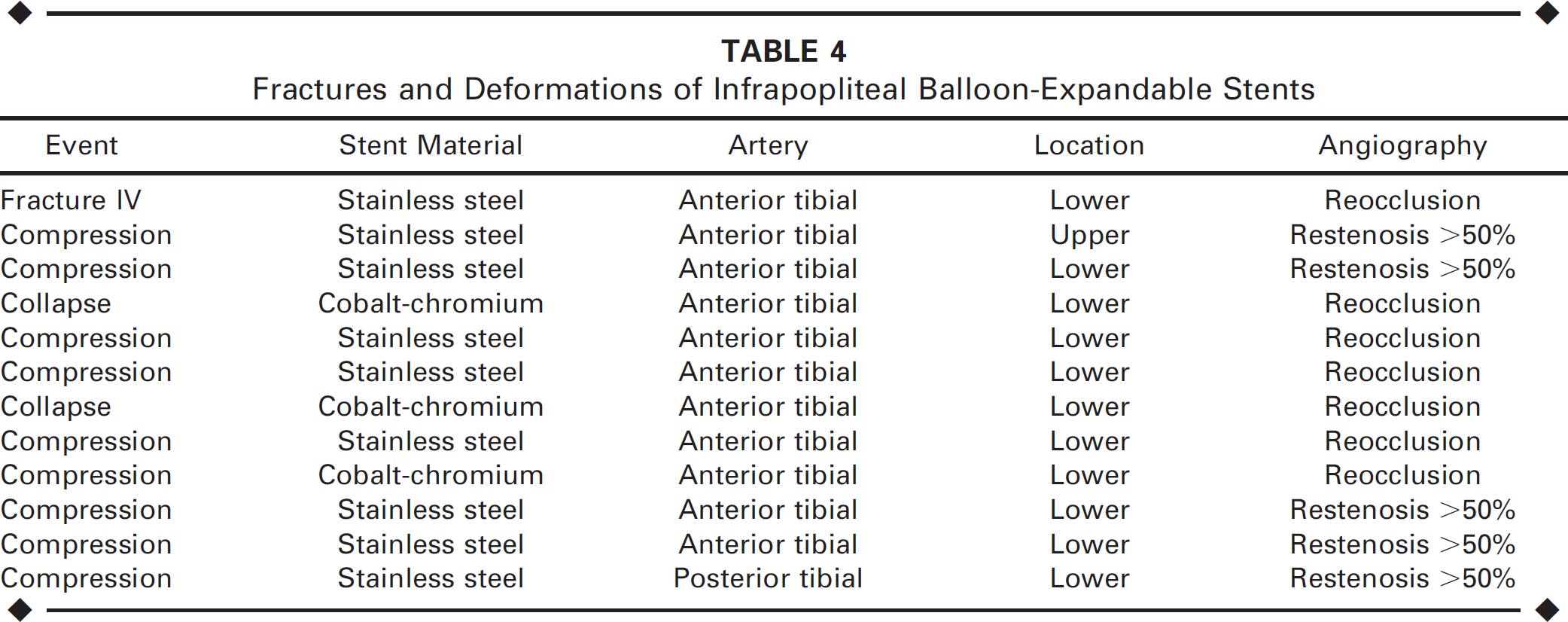
All 12 cases of stent fracture or compression (Fig. 3) were associated with angiographic binary (>50%) restenosis (5/12, 41.7%) or occlusion (7/12, 58.3%) of the respective lesion. Five (41.7%) patients had relapse of their CLI symptoms; all underwent repeat infrapopliteal angioplasty. Reintervention failed in 1 patient because of inability to cross the collapsed stent in the distal anterior tibial artery (ATA); the patient eventually underwent a major above-the-ankle amputation. In the remaining 7 limbs, no reintervention was performed because there was no clinical indication of recurrent CLI symptoms. Comparing the 12 patients with signs of stent fatigue to the remainder of the cohort, infrapopliteal stent fracture or compression was associated with increased restenosis/reocclusion [100% (12/12) versus 47.3% (169/357), p<0.001] and an increased rate of clinical deterioration and repeat procedures [41.7% (5/12 limbs) versus 19.4% (14/72 limbs), p=0.04].
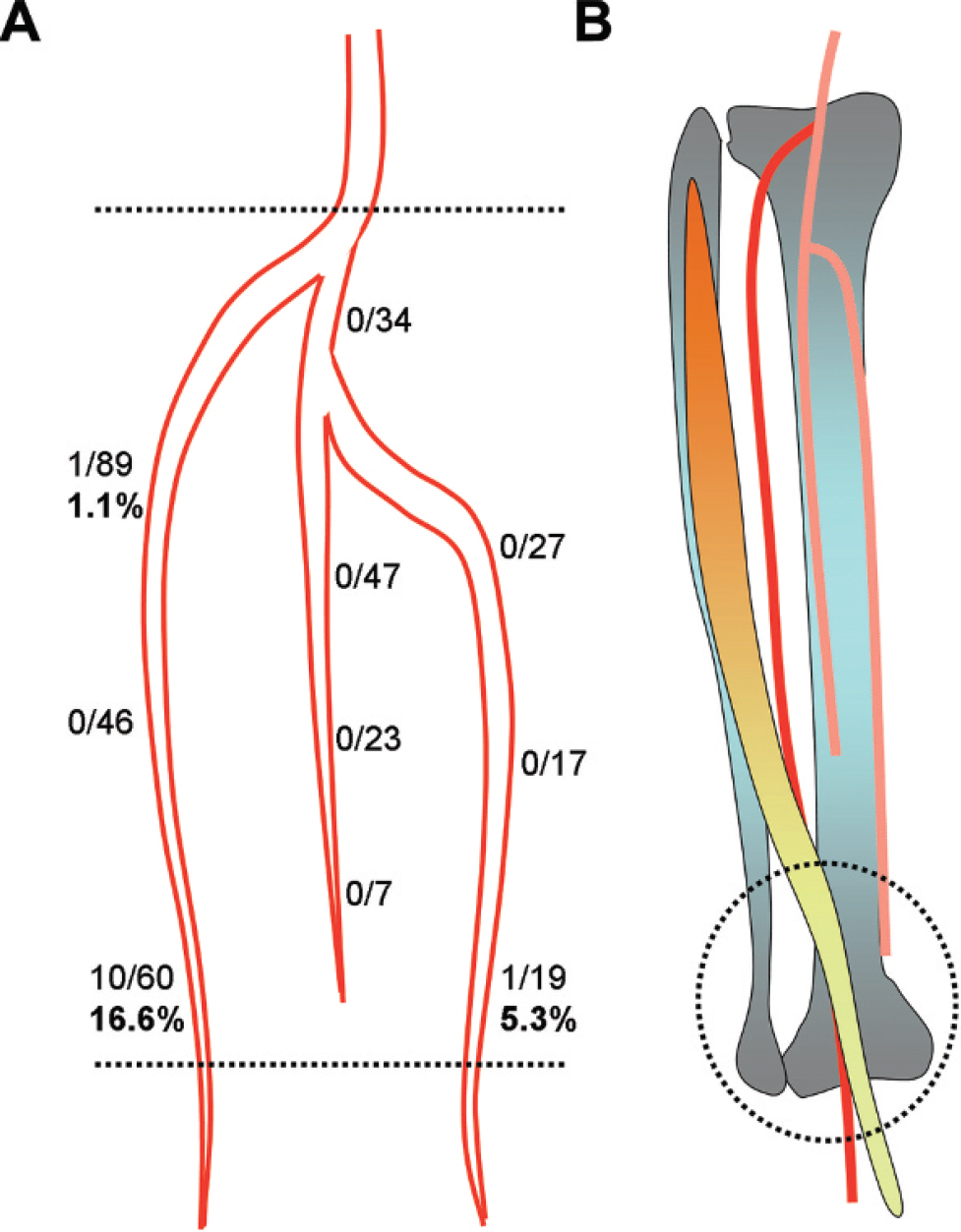
The single stent fracture and 9 of the 11 cases of stent deformation or compression occurred in the distal third of the ATA in close proximity to the lateral malleolus (p<0.001). One stent compression was noted in the proximal ATA and the last one in the distal posterior tibial artery at the level of the medial malleolus (Table 4). Specifically, the overall rate of stent fracture and/or compressions (Fig. 4A) along the distal ATA was 16.6% (10 of 60 stents examined in total). There was no statistical correlation between the above events and overlapping stent placement. Finally, no significant differences were noted between the patients who had an event (either fracture or compression) and the rest of the cohort regarding baseline demographics and other stent morphological characteristics.

Severe grade IV stent fracture observed 12 months after placement of 4 overlapping balloon-expandable metal stents in the distal anterior tibial artery. Note the separation and misalignment of stent struts (white arrows).

Distal compression of 2 overlapping balloon-expandable stents found 15 months after placement in the anterior tibial artery at the level of the lateral malleolus. Note the significant lumen narrowing in the magnified radiographic image (white arrowheads).
DISCUSSION
Application of bare or drug-eluting balloon-expandable metal stents in the infrapopliteal arteries of CLI patients has been shown to have a >90% technical success rate and encouraging midterm limb salvage.1–3,16,17 Despite continuous improvements in stent alloy materials and balloon profiles, fracture or deformation of the stent strut matrix has been an inherent problem that has been linked to excessive neointimal hyperplasia and negative vessel remodeling.13,14 Coronary and femoral artery stenting trials have documented the adverse relation between stent fracture and/or compression and vessel patency.5,6,13,14,18 Above all, the femoropopliteal artery is notorious for its high restenosis and stent fracture rates, especially at the adductor hiatus level.14,19 Exposure to high compression, torsion, flexion, and elongation forces from the surrounding muscles is responsible for the high susceptibility of femoropopliteal stents to compression and fractures, with an up to 30% reported incidence.14,20,21 However, little is known about the impact of mechanical forces exerted on infrapopliteal arterial stents. To the best of our knowledge, there is only one case report of infrapopliteal stent fracture in the literature, which was presumably iatrogenic following bifurcation stenting with the crush technique. 22
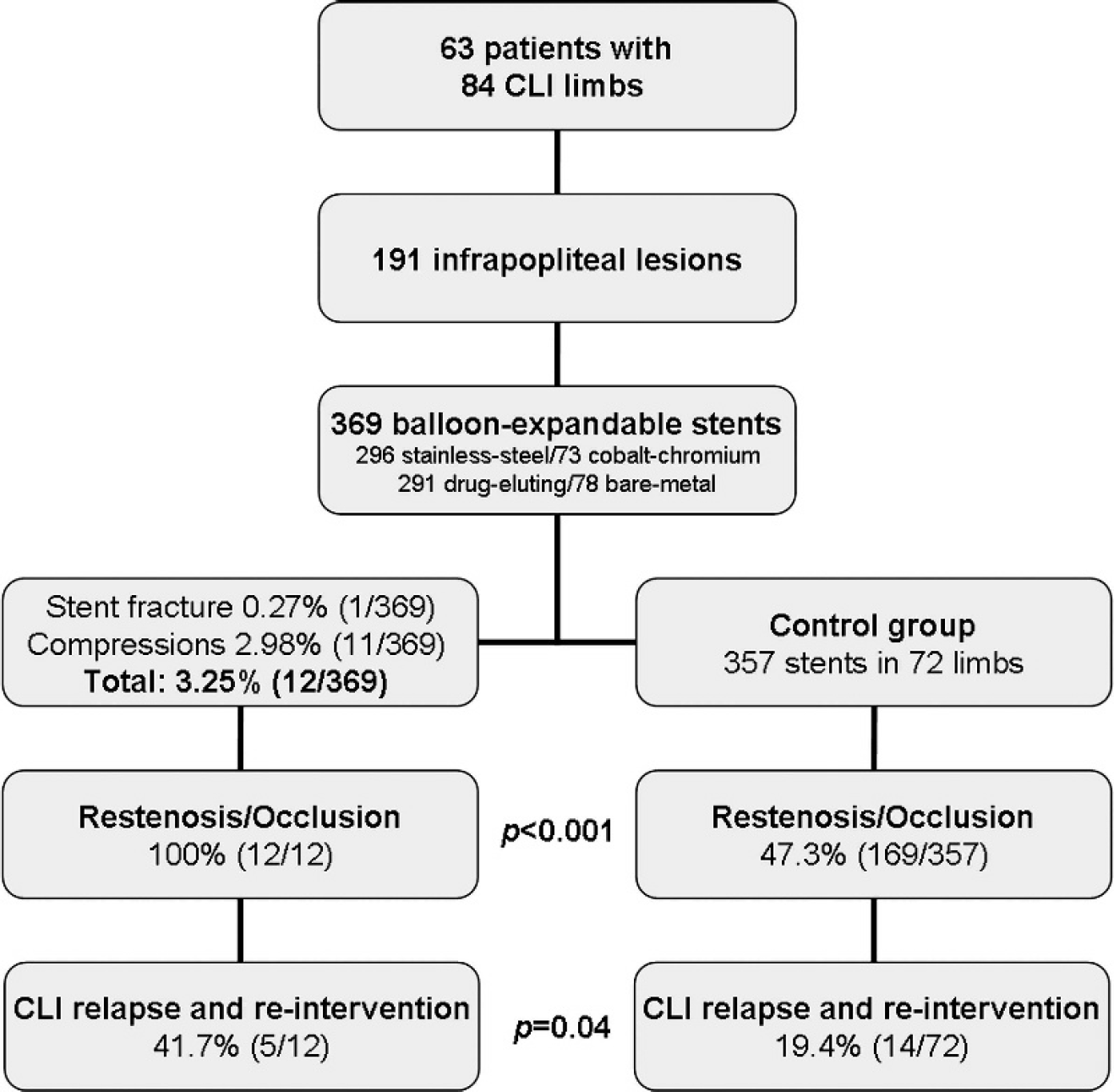
Flowchart shows the overall patient population and groups of stents examined. Restenosis and reintervention events of the fractured and deformed cases were compared to the rest of the cohort.
(
The present investigation was designed to address the lack of evidence regarding the pathology of fractures and/or compressions of stents placed in the infrapopliteal arteries. The patients in the study had a great variety of both stainless-steel and cobalt-chromium stent platforms, either bare or drug-coated, which were followed for >1 year on average. Interestingly, we identified only a single (0.3%) severe stent fracture in the distal ATA. On the other hand, stent compressions occurred 10 times more frequently (3%). Although this rate seems trivial, it should be noted that all cases of stent fracture or compression resulted in high-grade restenosis or occlusion of the respective segment. Moreover, infrapopliteal stent fracture or compression was associated with a more than double rate of clinical deterioration and repeat procedures (41.7%) in those cases versus the rest of the cohort (19.4%, p=0.04). Repeat infrapopliteal recanalization failed in 1 case because the stent was completely collapsed and intraluminal or subintimal wire crossing was impossible. Unfortunately, major amputation above the ankle was the end result in that patient.
Statistical analysis did not detect any correlation of infrapopliteal stent fatigue to stent material (stainless-steel versus cobalt-chromium) or stent coating (bare metal versus drug-eluting polymer). Notably, the single fracture and most of the compression events occurred in the distal third of the ATA. It is plausible that specific anatomical relationships of the artery at that level may be responsible for the increased vulnerability to stent deformations. The proximal and mid thirds of the ATA rest on the interosseous membrane, while the distal third lies on the tibia (Fig. 4B). In addition, the distal third of the ATA is crossed and overlaid by musculotendinous structures (extensor hallucis longus and extensor digitalis longus) and the ligaments of the ankle articular capsule. 23 The above combination may render the distal ATA especially susceptible to external or internal axial forces, leading to repetitive compression of stents against the underlying rigid bone surface of the tibia.
The above observations and speculations may be of utmost importance for the engineering of new thin-strut self-expanding stents specifically dedicated to the distal infrapopliteal arteries. However, the present study is limited by the fact that no independent plain radiographic imaging was performed at more frequent time points other than during regular angiographic follow-up. Therefore, the exact timing of stent deformations and their temporal relationship to the development of restenosis or occlusion could not be determined, especially since almost half of the cases were asymptomatic. Furthermore, the present study was limited to the investigation of balloon-expandable metal stents, which suffer only plastic permanent compression in contradistinction to the elastic mechanical properties of self-expanding metal stents.
Conclusion
Stent fractures and compressions of infrapopliteal balloon-expandable metal stents seem to occur mostly in the distal anterior tibial artery. Despite their infrequency, they are related to increased restenosis. Large-scale observational studies with timely follow-up imaging are necessary to further elucidate the clinical significance of these complications and the implications for novel stent designs dedicated to the infrapopliteal arteries.