
Abstract
Purpose:
To evaluate results with the retrievable Günther Tulip (GT) and Celect inferior vena cava filters (IVCFs) placed at the intensive care unit (ICU) bedside under “real-time” intravascular ultrasound (IVUS) guidance in multiple-trauma patients.
Methods:
Between December 2004 and December 2008, 187 multiple-trauma patients (109 men; mean age 44±2 years, range 17‒71) with contraindications to low-dose anticoagulation therapy or sequential compression devices had Günther Tulip (n=97) or Celect (n=90) retrievable IVCFs placed under real-time IVUS guidance. Günther Tulip filters were inserted using a “double-puncture” technique. The Celect IVCFs were placed with a simplified single-puncture technique in which the filter introducer sheath was advanced until the radiopaque tip “covered” the IVUS image of the renal vein, indicating that the filter sheath was in position for filter deployment. The 2 filter groups were compared on the endpoints of technical implantation success, retrievability, prevention of PE, and procedure-related deep vein thrombosis (DVT).
Results:
As verified by abdominal radiography, 93.1% (174/187) of IVCFs were placed without complications; 6 IVCFs (all GT; p=0.03 versus Celect) were misplaced in the iliac vein but uneventfully retrieved and replaced in the IVC within 24 hours. Two insertion site femoral vein DVTs (both in the dual puncture group; p>0.2) and 5 groin hematomas occurred during follow-up. GT filters were in place a mean of 107 days and Celect 97 days. In this time, 2 pulmonary embolisms occurred (1 in each group; p>0.2). Of the 115 filters scheduled for retrieval (50 Günther Tulip, 65 Celect), 33 (23 Günther Tulip, 10 Celect) could not be retrieved (p=0.0004). Vena cavography identified filter tilting (>20°) in 21 cases (15 GT, 6 Celect), while 12 filters (8 GT, 4 Celect) had extended indwell times (mean 187 days) and excessive tissue ingrowth covering the retrieval hook. Subjectively, the Celect filters were clinically “easier” to retrieve; they also had fewer cases of significant tilt (>20%) than the GT filters, but the difference was not statistically significant.
Conclusion:
GT and Celect IVCFs placed at the ICU bedside under IVUS guidance in multiple-trauma patients was simple, safe, and avoided transporting critically ill patients out of the ICU. Further investigation of the single sheath IVUS technique and the role of retrievable IVCFs in multi-trauma patients is warranted.
Keywords
Trauma patients with multiple injuries oftentimes cannot receive anticoagulation therapy or sequential compression device prophylaxis. Pulmonary embolism (PE), which has been reported in up to 23% of these high-risk patients, 1 is typically associated with significant morbidity and mortality.
Retrievable inferior vena cava filters (IVCF) prevent life-threatening PE, with minimal morbidity during the immediate injury and perioperative periods when the risk of PE is highest, while averting the potential long-term sequelae of a permanent IVCF. 2 The first commercially available retrievable filters to receive Food and Drug Administration approval were the Günther Tulip, OptEase, and Recovery. These filters all conferred a high degree of PE protection, but reports of filter migration, IVC thromboses, and unsuccessful filter retrieval led to the development of “second-generation” retrievable filters. The next-generation evolution of the Günther Tulip filter is the Celect, which has secondary “arms” designed to help center the filter and reduce tilt, thereby improving retrievability over time.
The objective of this study was to evaluate the placement and retrievability of the Günther Tulip and Celect filters at the ICU bedside under intravascular ultrasound (IVUS) guidance in multiple-trauma patients.
METHODS
Patient Population
Between December 1, 2004, and December 1, 2008, 187 multiple-trauma patients (109 men; mean age 44±2 years, range 17–71) with relative or absolute contraindications to low-dose anticoagulation therapy or barriers to placement of sequential compression devices underwent ICU bedside placement of Günther Tulip (97 patients through February 2007) or Celect (90 patients after March 1, 2007) retrievable IVCFs (Fig. 1; Cook Inc., Bloomington, IN, USA) under real-time IVUS guidance. All patients sustained multiple-trauma injuries, the majority (167, 94.1%) from motor vehicle crashes (mean Injury Severity Score of 28.5±2.2). The study was approved by our Institutional Review Board and complied with the reporting standards for IVC filter placement and patient follow-up from the Eastern Association for the Surgery of Trauma. 3

Günther Tulip and Celect Vena Cava Filters.
Filter Placement
Bedside placement of the Günther Tulip filters was performed under aseptic conditions using a previously described technique 4 ; 2 femoral vein punctures were made 1 cm apart, and 2 0.035-inch Glidewires (Terumo, Somerset, NJ, USA) were passed into the vena cava. An 8-F sheath was introduced over 1 Glidewire (IVUS wire) and a 6-F sheath over the second Glidewire (filter wire). A PV 8.2-MHz IVUS probe (Volcano Therapeutics, Rancho Cordero, CA, USA) was passed to the level of the right atrium, and the IVC was interrogated with a pullback technique that identified the liver, hepatic veins, renal artery, and renal veins. The transverse IVC diameter was measured at the infrarenal location to ensure that the 30-mm maximal size limitation was not exceeded. The IVUS probe was pulled back to the level of the most inferior renal vein, and the IVC filter sheath was introduced over the second Glidewire and advanced beyond the IVUS probe. As the filter was advanced in the sheath, the IVUS identified its passage beyond the renal veins until the echogenic “scatter” from the filter disappeared. The sheath and filter were pulled back to a point adjacent to the IVUS probe, the IVUS probe was withdrawn caudally to prevent “caging” the filter, and the filter was deployed, after which the introducer, IVUS probe, and sheaths were removed. An anteroposterior abdominal radiogram was obtained to evaluate the IVCF location. Prophylactic low-molecular-weight heparin was instituted as soon as it was believed safe by the attending trauma surgeon; pneumatic compression devices were used whenever possible.
Before filter retrieval, all patients underwent venous color-flow duplex ultrasound scanning of the lower extremities to rule out lower extremity DVT. All filter retrieval procedures were performed in the catheterization laboratory from a right jugular vein approach using the Cook retrieval system under ultrasound guidance. Before retrieval, vena cavography was performed to assess the IVCF for trapped emboli or thrombus within the filter. A significant (>25%) filter volume for trapped thrombus was considered a contraindication to filter removal. After retrieval, repeat vena cavography was performed to evaluate the IVC for contrast extravasation, intraluminal defects, or residual stenosis.
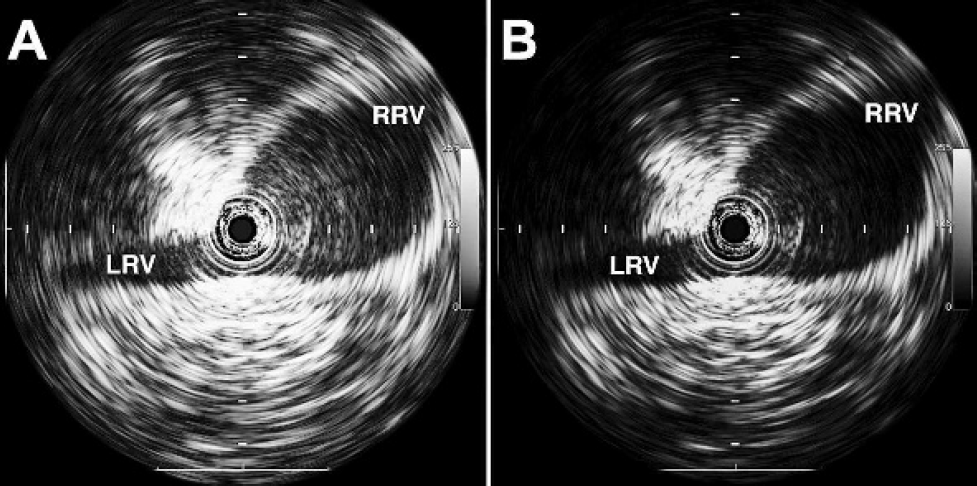
Since March 2007 following publication of an article by Jacobs et al., 5 we have also used a “single sheath” IVUS technique that involves a single femoral vena puncture, the Celect filter 9-F sheath, and a 260-cm 0.035-inch Glidewire. The IVUS catheter was introduced over the Glidewire and the IVC was interrogated as described above. After the renal veins were identified (Fig. 2A), the filter introducer sheath was advanced until the radiopaque tip of the sheath “covered” the IVUS catheter and the image of the renal veins lost its “brightness” (Fig. 2B). The tip of the introducer sheath can be repeatedly passed over the IVUS catheter (while holding the IVUS catheter in place) to confirm the location of the sheath tip just below the renal veins. The introducer sheath was then held in place while the IVUS catheter and guidewire were removed. The filter was then advanced into the sheath until the distal marker reached the Tuohy-Borst side-arm adapter, indicating the tip of the filter (the hook) was at the tip of the sheath. The filter introducer catheter was secured, the 9-F sheath was pulled back to the proximal marker, and the filter was released in the standard manner. Retrieval was identical to that for the Günther Tulip filter.
(
Statistical Analysis
Fisher exact, chi-square, or Student t tests were used to compare the quantitative variables of technical success for implantation, retrievability, prevention of PE, and procedure-related deep vein thrombosis (DVT). p<0.05 was considered to indicate a significant difference. Analyses were performed using SPSS statistical software (SPSS, Chicago, IL, USA).
RESULTS
In the 4-year study period, 187 IVCFs were deployed, the majority (172, 91.9%) within 48 hours of admission (161 via the right femoral vein and 21 via the left femoral vein). Six (3.2%) IVCFs were misplaced in the right iliac vein with the dual puncture technique; these filters were uneventfully retrieved and were replaced in the IVC within 48 hours. No filters were misplaced with the single puncture technique (p=0.03). In all, 174 (93.0%) filters were placed without complications in the vena cava as verified by post-procedure abdominal radiography. Procedural complications included 5 (2.7%) groin hematomas: 4 with the double puncture and 1 with the single puncture technique. Two (1.1%) femoral vein DVTs occurred with the double puncture technique and none with the single puncture technique (p>0.20).
Thirty-nine patients died of their injuries (29 Günther Tulip, 10 Celect patients): 25 due to multi-system organ failure and 14 after care was withdrawn because of irreversible brain injury. Two PEs were documented by contrast-enhanced computed tomography. One occurred after retrieval of a Günther Tulip filter in an ambulatory patient in the rehabilitation medicine service who had not had DVT prophylaxis initiated. The other PE was an “escape embolus” in a patient with a Celect filter. Both PEs were successfully treated with anticoagulation. There was no statistical difference in PE prevention efficacy between groups (p>0.20).
Günther Tulip filters were in place a mean of 107±2 days (range 42–261) and Celect filters a mean of 97±2 days (range 39–183) in the 148 surviving patients. Sixteen (8.6%) patients (9 Günther Tulip, 7 Celect) were lost to follow-up, and 17 filters (9 Günther Tulip, 8 Celect) were not retrieved in patients who had continued contraindications to anticoagulation because of the severity of their injuries. Of the 115 filters scheduled for retrieval (50 Günther Tulip, 65 Celect), 33 (23 Günther Tulip, 10 Celect; p=0.0004) could not be retrieved due to filter tilting and/or prolonged indwell times. Pre-retrieval vena cavography (compared against the long axis of the IVC) identified tilting (>20°) in 21 filters (15 Günther Tulip and 6 Celect). The other 12 filters (8 Günther Tulip, 4 Celect) had extended indwell times (range 168–210 days), and retrieval attempts were unsuccessful due to inability to capture the filter hook because of excessive tissue ingrowth. Thus, 82 (71.3%; 27 Günther Tulip, 55 Celect) of the filters were retrieved. One had trapped thrombus identified by vena cavography at the time of retrieval. None had structural defects, and only 1 Celect filter migrated (caudally 2 cm). Post-retrieval vena cavagrams demonstrated no contrast extravasation, intraluminal defects, or IVC narrowing.
DISCUSSION
Pulmonary embolus remains a leading cause of late mortality in the multiple-trauma patient. 6 Practice management guidelines for post-trauma–related venous thromboembolism prophylaxis from the Eastern Association for the Surgery of Trauma suggest the use of sequential compression devices in addition to low-molecular-weight heparin in all high-risk trauma patients. 7 Unfortunately, in this group of patients in whom it is needed most, appropriate DVT or PE prophylaxis cannot be used in nearly 50% of at-risk patients because of a contraindication to anticoagulation or because mechanical compression devices cannot be applied owing to external fixation, casts, or traction devices. 8 Many trauma centers, therefore, have opted for the prophylactic use of vena cava filters to prevent PE in multiple-trauma patients. 9 Although there is no Level I data, there are Level II and III data that support the use of IVC filters in multi-trauma patients who cannot be anticoagulated or have failed anticoagulation to prevent PE. In these series, prophylactic IVCF placement was a safe and effective method of reducing the reported PE mortality rates by half. 10 In our series of patients, there was only 1 PE while the filter was in place (an “escape” embolus trapped in a Celect device). Another PE occurred after the filter was removed in a patient in whom DVT prophylaxis was unfortunately not initiated. Both of these patients were successfully treated by anticoagulation, which emphasizes the role of retrievable filters as an effective “bridge” to anticoagulation until venous thromboembolism prophylaxis can be initiated.
Only 6 filters were misplaced with the double puncture technique early in our series. The risk of misplacement with IVUS guidance appears to be slightly higher than standard insertion techniques, but the situation can be immediately recognized and rectified without morbidity. With the single puncture technique, however, no filters were misplaced.
Our original bedside double-puncture technique enabled continuous ultrasonography of the IVC and renal veins to ensure accurate filter placement. However, a theoretical disadvantage of this technique was the concern about femoral vein thrombosis. With the single-puncture technique, only 1 groin hematoma and no femoral vein DVTs occurred. The single-puncture technique has become our preferred method of bedside filter deployment because it is easier and safer since theoretically the IVUS probe cannot lodge on a filter strut. The 1% (2/187) incidence of DVT in these patients may likely be due to the fact that these patients had prophylactic filters placed and the clotting cascades were, therefore, not “activated” as they are in the presence of DVT. This, however, remains to be proven.
Several studies have indicated the efficacy and safety for retrieval of the Günther Tulip filter. Terhaar et al. 11 reported an 84.2% retrieval success rate in 19 patients with a mean indwell time of 43.6 days (range 7–126). Another study by De Gregorio and colleagues 12 reported a 98% (31/32) 30-day (range 29–34) retrieval rate, while Looby et al. 13 reported 45 patients with a mean indwell time of 33.6 days (range 14–112) with an 80% (36/45) success rate. A previous study by our group 14 of 41 multiple-trauma patients investigated the retrievability of Günther Tulip filters after indwell times of >180 days. The mean indwell time for these patients was 261.5 days (range 182–403). Within this group, 31 (75.6%) filters were retrieved, while 10 were irretrievable due to filter tilt >15°.
Filter tilt may affect both filter function and retrievability due to excessive tissue ingrowth of filter components that come in contact with the IVC wall. A tilted filter may reduce the filter's ability to trap clots and inhibit retrieval by preventing snaring of the retrieval hook. In a multicenter study reported by Smouse et al., 15 of 554 patients who had Günther Tulip filters placed, retrieval was attempted in 248. Twenty-seven (10.8%) filters could not be retrieved due to filter tilt that caused hook orientation toward the vena cava wall.
The Celect filter was developed with secondary leg design changes to reduce filter tilt and extend the safe retrieval period beyond that of the Günther Tulip filter. In a multinational trial reported by Lyon et al, 16 57 of 95 patients with Celect filters had attempted filter retrieval between 5 and 466 days (mean 175.3); 55 (96.5%) were successfully retrieved. The 2 unsuccessful retrievals were attributed to filter tilt and excessive tissue ingrowth that imbedded the retrieval hook in the IVC wall after 1 year.
In our series, mean indwell times were ~100 days for both filters. Retrieval failed in almost a third of attempts due to filter tilting or prolonged indwell time that made it impossible to capture the filter hook because of excessive tissue ingrowth. Although the differences in filter tilt and indwell time between the Günther Tulip and Celect filters were not statistically different, the clinical “impression” was that the Celect filter tilts less and is easier to retrieve. This, however, needs to be proven, and more data will need to be obtained before any clinical recommendations can be made based on these findings.
Conclusion
The role of retrievable IVCFs placed at the ICU bedside under IVUS guidance in multi-trauma patients avoided the risk of transporting critically ill patients with invasive monitors and respirators out of the ICU. IVUS-guided placement of the Günther Tulip and Celect filters was simple, accurate, safe, and prevented fatal PE. Further investigation of the single sheath IVUS technique and the role of retrievable IVCFs in patients with multiple injuries is warranted.