
Abstract
Purpose:
To analyze the initial and long-term results of endovascular aneurysm repair (EVAR) in high-surgical-risk patients (i.e., age ≥80 years, serum creatinine level ≥3 mg/dL, severe pulmonary dysfunction, severe cardiac dysfunction).
Methods:
From April 2002 to June 2009, 50 consecutive high-surgical-risk patients (42 men; mean age 74.0±8.7, range 54–91) with an abdominal aortic aneurysm (AAA; mean diameter 64.8 mm) who were treated electively using a bifurcated aortic endograft (32 Excluder, 18 Zenith) were entered in a prospective registry. Thirty-five (70%) patients were classified ASA III and 15 (30%) were ASA IV. High-risk status was corroborated using the Customized Probability Index (CPI). Primary endpoints were operative mortality and long-term survival; secondary endpoints were the frequency of reintervention, evolution of the aneurysm sac, and rates of primary and secondary patency and rupture.
Results:
The mean CPI score was 11.04±6.3. Operative mortality was 2% (1/50). There were 4 endoleaks, 1 case of endotension, and 1 endograft limb occlusion. Two patients required reintervention during the mean follow-up of 35.6 months. Survival at 3 years was 94%. Primary and secondary patency rates at 3 years were 98% and 100%, respectively. There were no ruptures.
Conclusion:
Initial and long-term results with endovascular treatment of AAA in high-surgical-risk patients were satisfactory and appear to justify this approach in this patient population.
Keywords
Two prospective randomized studies1,2 that analyzed outcomes following endovascular aneurysm repair (EVAR) in low-surgical-risk patients reported a significant reduction in immediate morbidity and mortality rates compared to conventional open repair. Nevertheless, uncertainty concerning the long-term outcome of aortic endografts has prompted many scientific societies, among them the American Association for Vascular Surgery/Society for Vascular Surgery, 3 to recommend that EVAR should be reserved for the elderly and the so-called high-surgical-risk patients as long as the anatomy is favorable. However, recent EVAR studies have reported a high frequency of reinterventions 4—6 and elevated rates of immediate and late morbidity and mortality in high-surgical-risk patients, 6 which has raised the question if EVAR is the best treatment option for such patients. This study describes our results with EVAR in a cohort of high-surgical-risk patients treated by the same group of surgeons using commercially available bifurcated endografts and followed for >3 years on average.
METHODS
Study Design and Patient Sample
From April 2002 to June 2009, 55 consecutive patients with infrarenal AAA undergoing implantation of a bifurcated aortic endograft were entered into a prospective registry to collect data concerning diagnosis, operative risk, treatment, and follow-up according to a standardized protocol. All patients had contrast-enhanced computed tomographic angiography (CTA) with 3-dimensional reconstruction preoperatively. Suitability for EVAR was based on a (1) AAA diameter ≥5.5 cm; (2) a proximal neck >15 mm long, <60° angulated, and without thrombus or extensive calcification (>50% circumference); and (3) external iliac artery diameters ≥7 mm. 3 To qualify for this analysis, patients were classified as high surgical risk3,7—9 if they met one or more of the following criteria: age ≥80 years, serum creatinine level ≥3 mg/dL, severe pulmonary dysfunction (defined as 1-second forced expiratory volume <1 L, PaO2 <60 mmHg, PaCO2 >45 mmHg, or minimal effort dyspnea), or severe cardiac dysfunction [defined as acute myocardial infarction (MI) within 3 months; left ventricular ejection fraction (LVEF) ≤25%; recent (within 3 months) or recurrent symptomatic congestive heart failure (CHF); severe and diffuse coronary artery disease (CAD) unsuitable for revascularization with or without unstable angina; symptomatic aortic stenosis; or unstable angina at rest].
To corroborate the high-risk status, the Customized Probability Index (CPI) was calculated for all patients in the study.10,11 The CPI, which has been validated for all vascular surgery patients, includes components representing the 3 most commonly cited factors associated with outcome after AAA repair, assigning risk points for cardiac, pulmonary, and renal diseases while compensating for the use of statins and beta-blockers.11—13
Based on these criteria, 3 patients with low surgical risk and 2 with ruptured AAA were excluded, leaving 50 patients (42 men; mean age 74.0±8.7, range 54–91) deemed to be high surgical risk (Table 1). Most (35, 70%) patients were classified as ASA (American Society of Anesthesiologists) 14 III; 15 (30%) were ASA IV. Of the 31 patients with severe cardiac dysfunction, 12 had severe and diffuse CAD unsuitable for revascularization (7 with and 5 without unstable angina), 10 had LVEF ≤25%, and 9 had multiple associated heart problems (recent or recurrent symptomatic CHF, arrhythmias, and CAD). Of the 17 patients with severe pulmonary dysfunction, 6 had minimal effort dyspnea, 5 had 1-second forced expiratory volume <1 L, 4 had PaO2 <60 mmHg, and 2 had concomitant pulmonary problems (minimal effort dyspnea and pulmonary emphysema requiring home oxygen). Six patients had serum creatinine ≥2 mg/dL but none was ≥3 mg/dL. Mean aneurysm diameter was 64.8±7.4 mm. The proximal neck measured a mean 25±9.5 mm (range 15–56) in length and 22.7±3.2 mm in diameter (range 17–29).
Characteristics of 50 High-Surgical-Risk Patients Submitted to EVAR
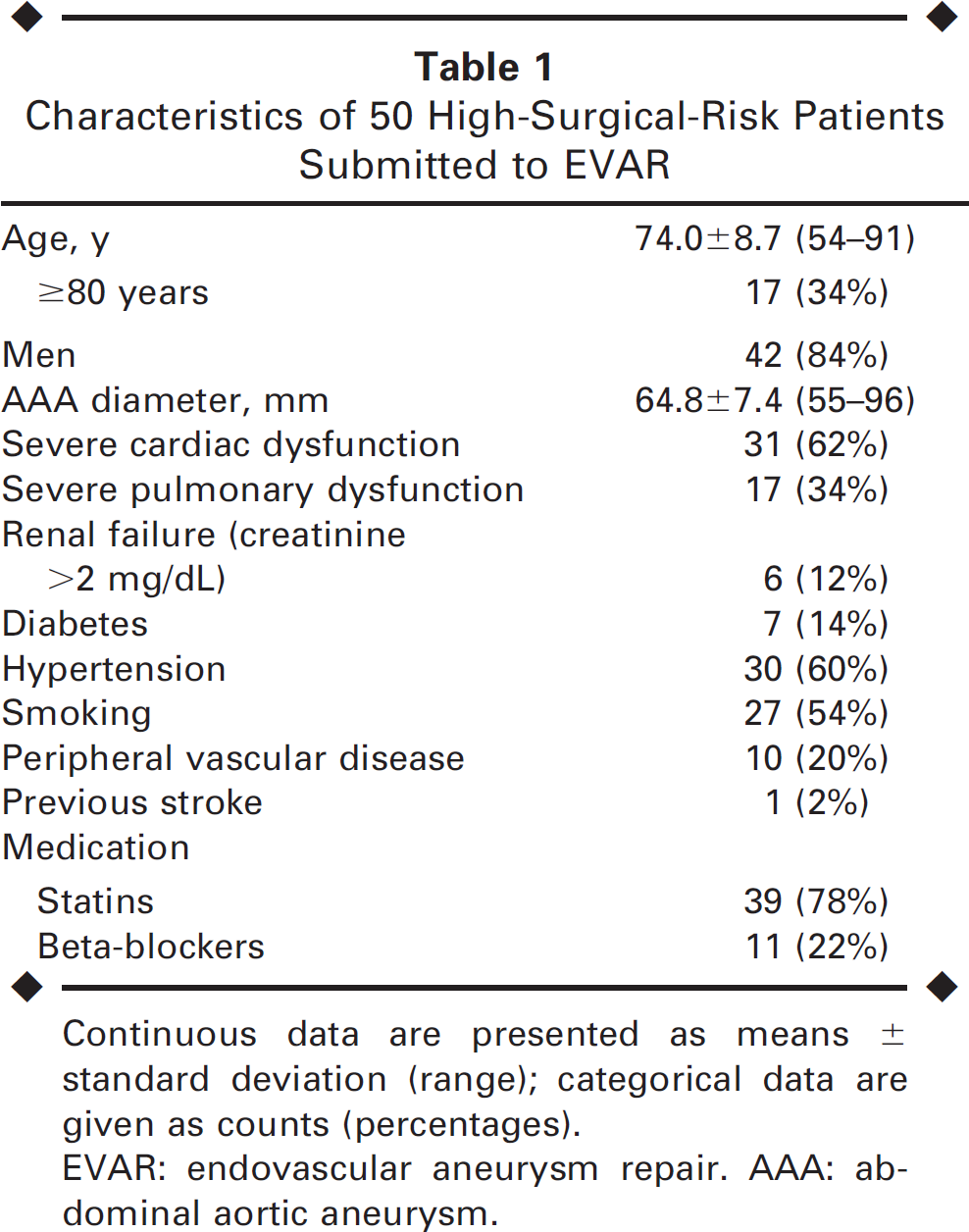
Continuous data are presented as means ± standard deviation (range); categorical data are given as counts (percentages).
EVAR: endovascular aneurysm repair. AAA: abdominal aortic aneurysm.
EVAR Technique
Informed consent was obtained from all patients after the technique, risks, and possible complications were discussed in detail. All procedures were performed in surgical suites with the patients prepared for open surgery in case of conversion due to failure of the endovascular approach or the occurrence of serious complications. Patients were given 1 g of intravenous cefazolin for infection prophylaxis and placed under epidural anesthesia. After dissection of the common femoral arteries, 5000 units of heparin were administered intravenously. Thirty-two Excluder (W. L. Gore & Associates, Flagstaff, AZ, USA) and 18 Zenith (Cook Inc., Bloomington, IN, USA) stent-grafts were implanted. Digital subtraction angiography was performed at the end of the procedure in all cases. Postoperative follow-up consisted of clinical examination and CTA or duplex scans at 1, 6, and 12 months after EVAR and at every 12 months thereafter.
Study Endpoints and Statistical Analysis
Primary endpoints were operative mortality and late survival. Secondary objectives were primary and secondary patency rates, frequency of reinterventions, and the status of the aneurysm sac after stent-graft implantation. Operative mortality was defined as death due to any cause up to 30 days after stent-graft implantation. Reintervention was defined as any surgical or endovascular procedure performed to maintain a satisfactory clinical outcome or to treat a specific complication related to the stent-graft or the aneurysm. The status of the aneurysm sac was evaluated by postoperative measurement of aneurysm cross-sectional diameter on CTAs performed during follow-up. In addition, blood loss, duration of the procedures, and time in the intensive care unit (ICU) and in the hospital were also analyzed. Statistical analyses were performed using Statgraphics (version 5.1; StatPoint Technologies, Warrenton, VA, USA). Continuous data are presented as means ± standard deviation; categorical data are given as counts (percentages).
RESULTS
The mean CPI score for the 50 patients was 11.0±6.3 (range 3–24). All 15 ASA IV patients had at least 2 criteria for high risk (age ≥80 years, renal failure, severe pulmonary dysfunction, or severe cardiac dysfunction) associated with multiple severe comorbidities. The 35 patients classified as ASA III had at least one high-risk criterion associated with other minor problems such as hypertension, tobacco abuse, or diabetes. No patient had more than 2 criteria for high risk.
EVAR was technically feasible in all patients (100%). Five patients required balloon angioplasty of the common iliac arteries (CIA) to facilitate stent-graft implantation. Eight patients were submitted to embolization of one of the internal iliac arteries due to ipsilateral CIA aneurysm (stent-graft landing zone in the external iliac artery). Mean blood loss was 193.16 mL (range 100–550) in procedures lasting a mean 178.1 minutes (range 90— 270). Mean stays in the ICU and hospital were 25.5 hours (range 0–72) and 3.0 days (range 1–5), respectively. One 85-year-old man with a history of multiple MIs (LVEF 20%) died from an acute MI on the seventh postoperative day (operative mortality 2%).
Mean follow-up was 35.6 months, during which 2 (4.1%) patients died (14th and 47th postoperative months) of acute MI (both patients had severe and diffuse CAD). The survival rate at 3 years was 94% (Figure). Primary and secondary patency rates at 3 years were 98% and 100%, respectively.
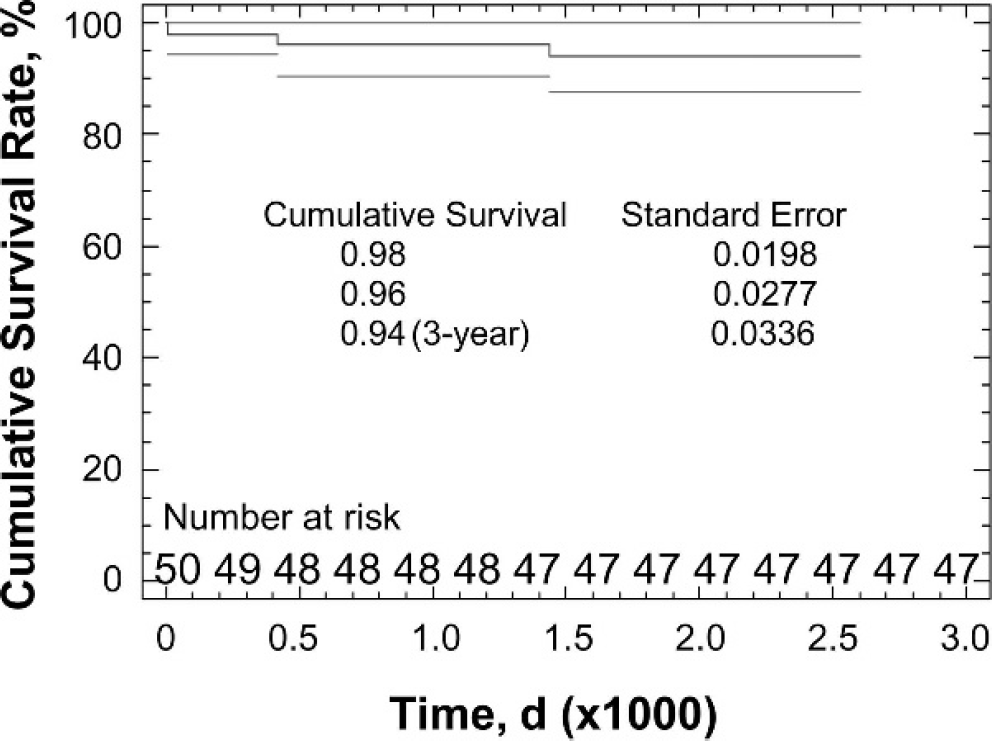
Kaplan-Meier curve of survival for the 50 high-risk patients who underwent EVAR. Gray lines denote the 95% confidence interval.
Three patients had buttock claudication after internal iliac artery embolization, with complete resolution of symptoms between 3 and 12 months. Acute renal failure in 1 patient (precipitated by iodinated contrast) responded well to clinical treatment (hydration and diuretics). There were 3 type II endoleaks (2 early and 1 late), 1 type Ib endoleak, and 1 case of endotension. One early type II endoleak sealed spontaneously at 3 months after the procedure; the second early type II endoleak persists, but the aneurysm diameter is stable.
Two (4%) patients required reintervention during follow-up. In one, the main body of the Excluder bifurcated endograft was made of low-permeability polytetrafluoroethylene (PTFE) and the contralateral leg of high-permeability PTFE. This patient had an immediate type Ib endoleak that sealed after balloon angioplasty. Doppler ultrasonography and CTA 2 years after the initial procedure showed that the aneurysm diameter had increased (this was the only patient with an increased AAA diameter after EVAR). Digital angiography showed a late type II endoleak maintained by the inferior mesenteric artery (IMA), which was ligated laparoscopically. Because the AAA continued to expand after IMA ligation, it was then thought that the patient could have endotension caused by extravasation through the contralateral leg of the Excluder stent-graft.15,16 A second contralateral leg (made of low-permeability PTFE) was implanted; CTA 3 months after the procedure showed a stable aneurysm diameter. The second patient who required reintervention had occlusion of the right limb of a Zenith stent-graft with lower limb ischemia; a balloon-expandable stent was implanted with a good outcome.
Overall, the aneurysm sac decreased in size by 2 to 23 mm in 28 (56%) patients in this series. In the 21 remaining patients, the aneurysm sac remained stable during the entire follow-up period. There was no case of AAA rupture after EVAR.
DISCUSSION
Previous studies have suggested that endovascular AAA repair may be a good alternative to open repair for patients with severe comorbidities.17—23 Operative mortality rates in the literature range from 0% to 5.3% for this population of high-risk patients. The EVAR-2 trial, 6 a prospective randomized study comparing surveillance to endovascular AAA repair in patients for whom open treatment was contraindicated, reported a periprocedural mortality rate of 9% and a survival rate of only 34% in the endovascular group after a 4-year follow-up. This study raised the concern that EVAR might not provide any advantage over surveillance in high-risk patients. In contrast, however, the operative mortality in our high-surgical-risk cohort was only 2% and survival at 3 years was 94%; none of the deaths was due to AAA rupture or stent-graft complications. Over the 35-month follow-up, the frequency of reinterventions was low (4%, n=2). Aneurysm sac diameters were reduced in more than half of the cases.
Some may contend that the results of our study were better than EVAR-2 because our criteria for high risk were more lenient. However, the criteria used in this study (cardiac, pulmonary, and renal) were very similar to those of EVAR-2, 8 so that 92% (46/50) of our patients would have probably qualified as EVAR-2 patients. All of our patients were ASA classes III/IV, classically considered as high risk for open treatment of AAA. 17 The only difference between both studies is that we considered age >80 years as an independent criterion for high risk. Regardless, of the 17 patients >80 years old, only 4 (8%) had age as an isolated risk factor (and probably would not have been included in the EVAR-2). Further, when we used the validated CPI score11,12 to ascribe fitness status at baseline for all the patients in our study, the mean score was comparable to the mean score in the EVAR-2 trial 13 : 11.0±6.3 versus 10.0±11.3, respectively.
In addition, several large studies17,19,22,24—26 (Table 2) also achieved favorable results with EVAR in patients considered at high risk for conventional open repair. In a single-center experience, Iannelli et al. 18 encountered no deaths in the perioperative period among 34 high-risk EVAR patients compared to a 14.3% mortality rate for 28 high-risk patients undergoing open repair (p<0.05), but in follow-up, there was no significant difference in the death rates. With a 3-year mean follow-up in 92 patients, Jean-Baptiste et al. 25 observed a perioperative mortality rate two times greater than ours, but a good (85%) survival rate. In a recent comparative study, Hynes and Sultan 26 documented a 3% operative morality rate among their 66 high-risk EVAR patients; freedom from aneurysm-related death was 96.7% after 4 years, while overall survival was 78.8%.
Literature on Endovascular AAA Repair in High-Surgical-Risk Patients
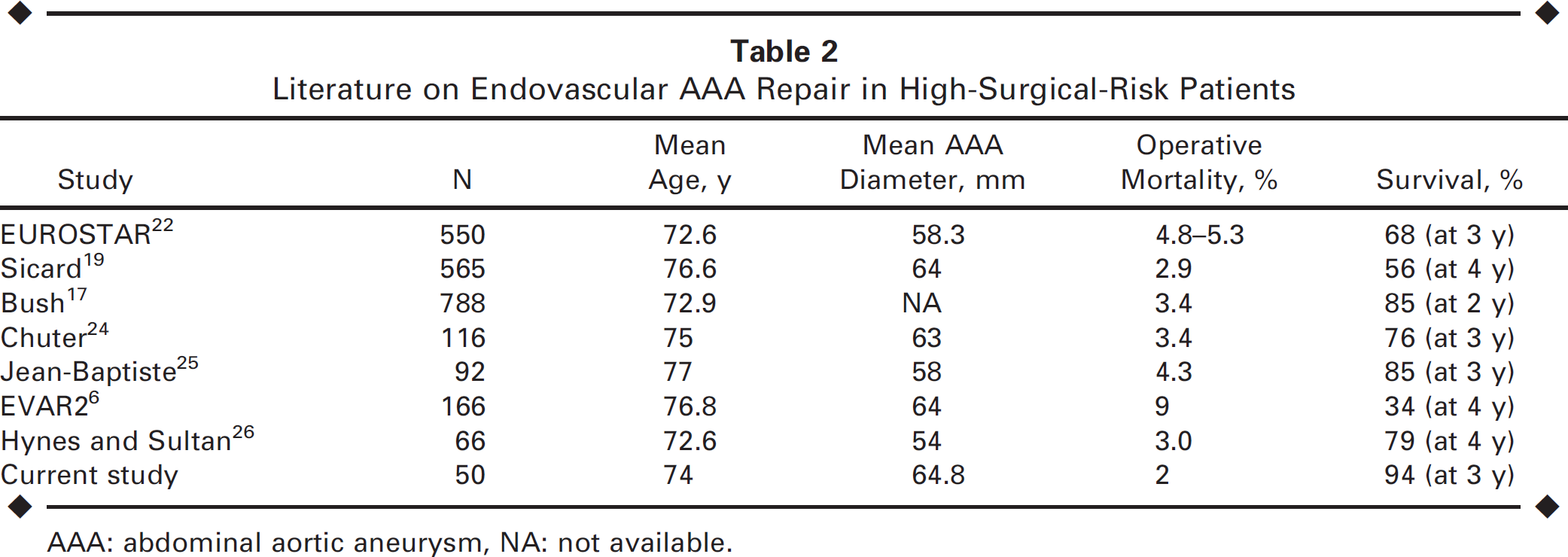
AAA: abdominal aortic aneurysm, NA: not available.
Notable limitations of this study were the retrospective analysis and lack of any control group. Although the sample was relatively small, no patient in this series was lost during follow-up.
Conclusion
Our initial and long-term results with endograft treatment of AAA in high-surgical-risk patients were satisfactory, with low operative mortality, a 3-year survival rate of 94%, and very few reinterventions. In our opinion, these results justify endovascular repair for this group of patients. The most important factor for improving the results of aortic endografts is adherence to the anatomical requirements.