
Abstract
Purpose:
To describe perforation of a Dacron aortic graft due to a post-thoracotomy dislocated rib fracture in a young Marfan patient.
Case Report:
Six months after a successful open repair of a type II dissecting thoracoabdominal aortic aneurysm (TAAA), a 40-year-old woman with Marfan syndrome underwent elective repair of a post-thoracotomy dislocated rib fracture. During the procedure, the graft ruptured; 2 TAG stent-grafts were emergently implanted to reline the existing aortic graft. The fractured rib was then resected. The postoperative course was uneventful, without residual leak at computed tomography at 3 days. At 18 months, the patient is well, without need of further operations.
Conclusion:
Early correction of any dislocated rib fracture close to a thoracic aortic graft should be considered, especially if the graft is not wrapped by the aneurysm sac. In these patients, in-graft endovascular relining associated with repair of the rib fracture may be a feasible and effective alternative to redo thoracotomy and surgical graft repair. Prior to attempting rib resection, appropriate thoracic endografts should be on hand in case an endovascular bailout is needed.
Keywords
Severe thoracic injuries related to a dislocated rib fracture are not so unusual after major trauma of the chest wall; hemothorax or pneumothorax resulting from intercostal vessel damage or lung laceration have been commonly reported. More unusual are other organ lesions, although cardiac injuries, lesions of the pericardium, rupture of subclavian artery; injuries to the liver, kidneys, or spleen; gastric perforation; and diaphragmatic hemorrhage have been reported.1—6 Direct damage to the native thoracic aorta by dislocated rib stumps has been previously reported in only 5 patients.7—11 We report the endovascular rescue of a patient with a post-thoracotomy rib fracture that eroded a surgical graft 6 months after open repair of a thoracoabdominal aortic aneurysm (TAAA).
CASE REPORT
A 40-year-old woman with Marfan syndrome and a 2-day history of back pain was referred to our department for a 75-mm type II dissecting thoracoabdominal aortic aneurysm (TAAA). Because of periaortic and left pleural effusion, she underwent emergent TAAA open repair under left heart bypass with sequential aortic clamping and cerebrospinal fluid drainage. During thoracophrenolaparotomy through the 6th intercostal space, the 6th rib was fractured by the retractor. The procedure continued with repair of the thoracoabdominal aorta using a 24-mm Gelweave Coselli Thoracoabdominal Graft (Vascutek Ltd., Renfrewshire, Scotland). Proximal anastomosis was performed distal to the origin of the left subclavian artery; no intercostals arteries were reimplanted due to inadequate aortic dissected wall, the visceral and renal arteries were selectively reimplanted to the 4 graft visceral branches, and distal anastomosis was made at the aortic bifurcation. Contrary to our standard practice, due to the relatively small diameter of the proximal third of the descending aorta, the thoracic aortic wall was not large enough to close over the proximal third of the thoracic graft; only the thoracoabdominal and abdominal segments of the graft were wrapped with the aneurysm sac.
Cases of Thoracic Aortic Rupture or Risk of Rupture Related to a Dislocated Rib Fracture
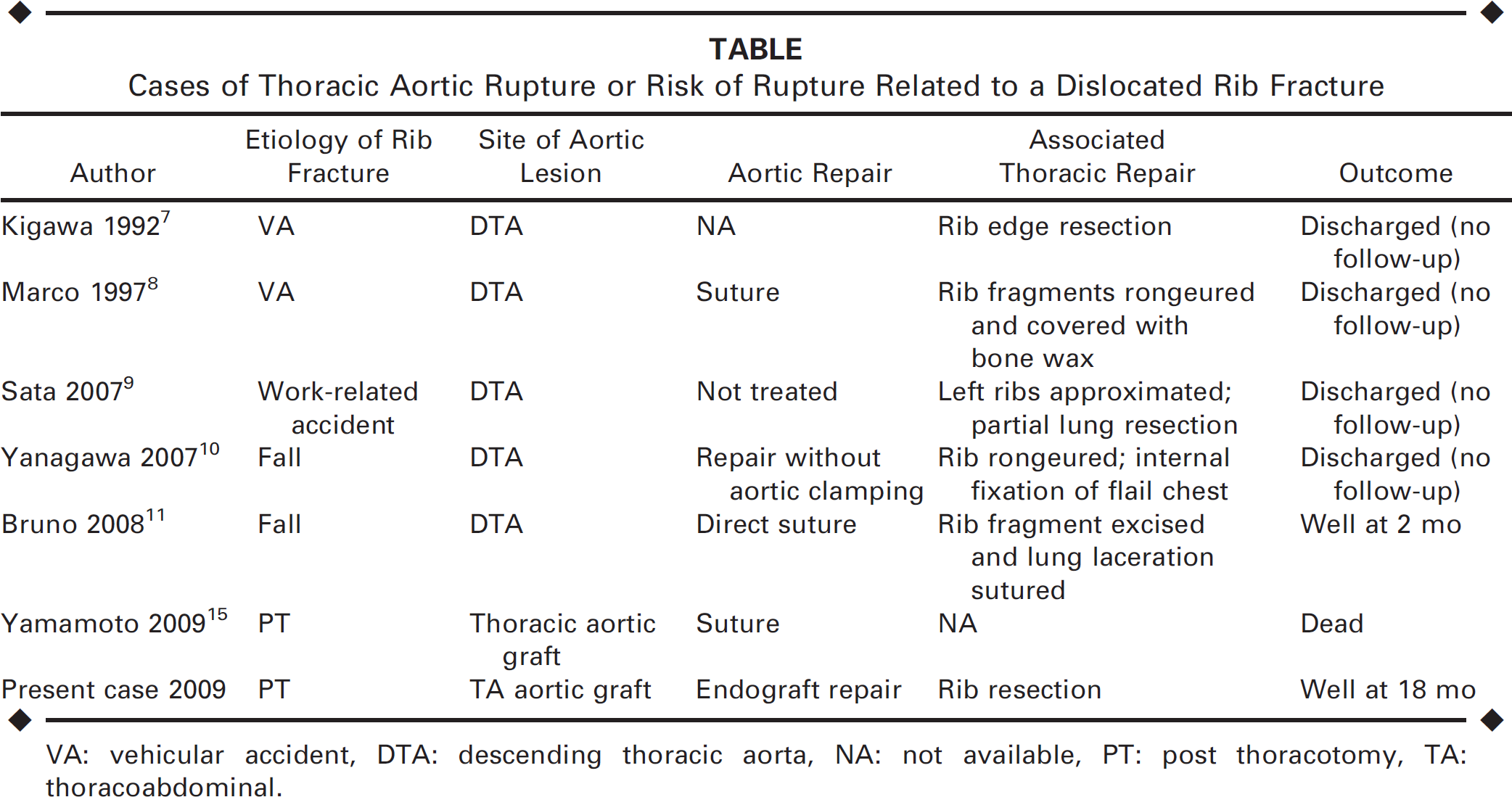
VA: vehicular accident, DTA: descending thoracic aorta, NA: not available, PT: post thoracotomy, TA: thoracoabdominal.
The postoperative thoracic computed tomography (CT) scan (Figure, A) at 6 days showed the presence of a dislocated fracture of the 6th left rib with the distal stump in direct contact with the aortic graft, which appeared elongated and in direct contact with the lateral left chest wall. The patient did not complain of any unusual thoracic pain, leaflet syndrome, or other mechanical respiratory complications and refused any further suggested treatment of the rib fracture. She returned to the referring hospital for the rehabilitation program.

(
After 6 months, a CT scan confirmed the distal rib stump in direct contact with the aortic graft. Owing to the threat of graft perforation, the patient agreed to undergo elective rib fracture surgical repair in the hospital of origin, even though at the time she was still completely asymptomatic.
The patient was positioned in a right lateral decubitus manner with the hips flexed to 30° and draped, allowing access to both the inguinal areas. A 15-cm-incision was performed on the previous thoracotomy at the site of the rib fracture. After isolation of the distal rib stump and its careful mobilization, massive bleeding from the graft occurred due to complete perforation by the rib fragment. Immediate control of bleeding was achieved by digital occlusion of the Dacron tear. Direct or patch closure without graft clamping was not possible due to the excessive blood loss and graft dissection was not possible due to the frozen chest; even partial cross clamping or side-clamping was impracticable. Temporary bleeding control was obtained with an in-graft molding latex balloon (diameter 33 mm) inserted through a left common femoral artery emergent surgical approach, and a large irregular graft tear surrounded by an area of weakened fabric below the mobilized rib stump was visualized. After 8 minutes of endovascular thoracic aortic clamping, hemodynamic stability was restored, the balloon was removed, and manual control of the bleeding was achieved to allow distal perfusion. Endovascular repair through the surgical femoral approach was then planned, with positioning of the in-graft landing zones far from the left subclavian artery and the visceral vessels. Two 28-mm TAG devices (W.L. Gore & Associates, Flagstaff, AZ, USA) were ordered and arrived at the hospital within ∼1 hour. Both endografts had to be deployed within the previous 24-mm Dacron graft to completely seal the graft leak and to resolve the graft angulation caused by in-graft deployment of the first endograft. Then, a length of about 15 cm of distal rib stump was completely resected to avoid any further direct contact between the repaired thoracic graft and the fractured rib. The postoperative course was uneventful, without residual leak at CT on 3 day (Figure, B). After 18 months of follow-up, the patient is doing well, with no other reported complications, graft degeneration, or pseudoaneurysm, and without need of further operations
DISCUSSION
Graft-related complications after open repair of thoracic aneurysms usually include anastomotic pseudoaneurysms, graft infections, fistulas, and Dacron graft changes.12—14 To the best of our knowledge, only one other case of graft perforation by a dislocated rib fracture has been published, but the patient died for massive bleeding in spite of the emergent open repair. 15 Our patient survived thanks to a emergency bailout endovascular approach. Interestingly, both patients had thoracic graft elongation and no aneurysm sac wrapping over the graft, which may have facilitated direct contact between the graft and chest wall. Moreover, both the patients had Marfan syndrome, which could play a role in excessive rib stump motion and inadequate healing of rib fractures.
Deliberate and retractor injury—related fractures of the left ribs during thoracic vascular surgery are common, and it is our standard practice to cut the 6th rib at the anterior and posterior sites during elective open surgery for types I and II TAAA. During chest wall reconstruction, the sharp edges of the rib stumps are smoothed with a rasp and simply approximated in order obtain spontaneous healing. Among our overall experience of <300 TAAA open repairs since 1988, some dislocated rib fractures have been observed on postoperative chest radiographs, but none has been associated with significant complications.
The management of a dislocated rib fracture is controversial, and surgical repair is traditionally reserved for patients requiring re-thoracotomy for other intrathoracic lesions, flail chest, severe chest wall instability, persistent pain secondary to fracture, nonunion, or loss of pulmonary function. Moreover, a redo thoracotomy could be associated with a risk of lung injury. In patients with a thoracic graft, this may cause devastating secondary thoracic aortic graft infection, so we usually are conservative in our management of dislocated rib fractures. On the other hand, a rib stump—related aortic graft perforation is a dramatic life-threatening complication in which the acute massive bleeding can lead to death in spite of an emergency thoracotomy. 15
Conclusion
Based on this case, we now favor mandatory early correction of any dislocated rib fracture close to a thoracic aortic graft, especially if the graft is not wrapped by the aneurysm sac, because fabric rupture contained by the rib stump may not be identified on imaging. In these patients, in-graft endovascular relining associated with rib resection may be a feasible and effective alternative to redo thoracotomy and surgical graft repair. Prior to attempting rib resection, appropriate thoracic endografts should be on hand in case an endovascular bailout is needed.