
Abstract
Purpose:
To report the 2-year results of the MELODIE trial, which evaluated the safety and effectiveness of the balloon-expandable Express LD Vascular stent for the treatment of atherosclerotic iliac artery disease.
Methods:
This prospective, multicenter, single-arm trial enrolled 151 patients (113 men; mean age 60.1±8.4 years) with 163 de novo or restenotic iliac lesions. The primary endpoint, 6-month angiographic mean percent loss of luminal diameter, was compared to an objective performance criterion (OPC) based on published results with the Palmaz stent. Follow-up included ankle-brachial index (ABI) measurement and symptom assessment (Fontaine classification) at discharge, 30 days, and 6, 12, and 24 months. Arteriography was performed at 6 months and computed tomographic angiography (CTA) at 1 and 2 years.
Results:
The primary endpoint of 6-month mean percent luminal diameter loss was 16.2% (upper 95% confidence boundary of 19.1%) and non-inferior to the 20% OPC (p=0.006). Primary patency was 92.1% at 6 months and 87.8% at 2 years. The rate of major adverse events (MAE) was 6.3% at 6 months and 10.2% at 2 years. Of the 3 event types included in the definition of MAE, only target lesion revascularization occurred; no distal embolization or device- or procedure-related deaths were recorded. The percent of patients with Fontaine stage IIb symptoms or worse improved from 84.1% before the procedure to 16.8% at 2 years (p<0.0001). The 2-year ABI remained significantly improved compared to baseline (0.85 versus 0.63, p<0.0001).
Conclusion:
The Express LD Vascular stent is safe, effective, and non-inferior to the Palmaz stent for treatment of iliac artery stenosis.
Peripheral vascular disease is common and increases in prevalence with age, affecting up to 29% of adults in the United States aged 50 years and older. 1 Iliac atherosclerosis, which accounts for about one third of peripheral atherosclerotic lesions, 2 can cause claudication and, in severe cases, limb-threatening ischemia. Surgical bypass was commonly performed in the past to treat iliac disease but has become less common with the development of minimally invasive endovascular techniques. Several studies have shown that periprocedural morbidity and mortality are lower and long-term outcomes are similar with percutaneous transluminal angioplasty (PTA) compared to surgery.2-5 As in other vascular territories, iliac PTA is limited by such complications as vessel recoil, dissection, distal embolization, acute closure, and restenosis. In an attempt to improve outcomes, stent use has increased, and a number of studies favor iliac stenting over simple PTA.6-8 A meta-analysis comparing iliac stenting to PTA found that stenting had higher rates of technical success and was associated with a 39% reduction in the risk of long-term loss of patency. 9 The increased use of stents for treatment of peripheral vascular disease has spurred demand for new and improved stents.
Both balloon-expandable and self-expanding stents have been used to treat atherosclerosis in iliac arteries. Balloon-expandable stents exert greater radial force on the wall of the vessel during deployment than self-expanding stents do, which makes balloon-expandable stents potentially more suitable for treating calcified, resistant, or fibrous lesions. Also, balloon-expandable stents can be placed with greater precision due to their minimal predictable foreshortening and mode of deployment.10,11 Balloon-expandable stents made of stainless steel are typically more radiopaque than self-expanding stents, which are usually made of inert, non-ferromagnetic metals, such as nitinol. Self-expanding stents are generally more flexible and easier to track through tortuous vessels than balloon-expandable models.10,12 Self-expanding stents also re-expand following deformity and are thus favored in situations where the stent will be exposed to external compression. 13 In addition, self-expanding stents may cause less stress and lower levels of damage to the vessel wall than balloon-expandable stents. 14
The Express LD Vascular stent is a second-generation balloon-expandable stainless steel stent designed to be flexible and easy to deliver while still maintaining sufficient radial strength and radiopacity. The safety and efficacy of this stent were evaluated in the MELODIE trial, a prospective,
METHODS
The MELODIE trial was designed to test if outcomes in patients treated with the balloon-expandable Express LD Vascular Pre-mounted Stent System (Boston Scientific Corporation, Natick, MA, USA) were non-inferior to a calculated objective performance criterion (OPC) based on published results with the Palmaz balloon-expandable stent (Cordis, a Johnson & Johnson company, Warren, NJ, USA). The MELODIE trial was designed to support regulatory approval in Japan, which required a primary endpoint based on follow-up angiography. The Palmaz stent was chosen as a comparator because it was the only balloon-expandable stent with published clinical trial data reporting outcomes based on follow-up angiography after iliac stenting. It was also the only balloon-expandable stent that had been approved by the US Food and Drug Administration for use in iliac arteries. 15 The MELODIE study was conducted in accordance with Good Clinical Practice and the Declaration of Helsinki regarding investigation in humans. The trial is registered on the National Institutes of Health website (Clinical-trials.gov, Identifier NCT00352222).
Patient Selection and Study Centers
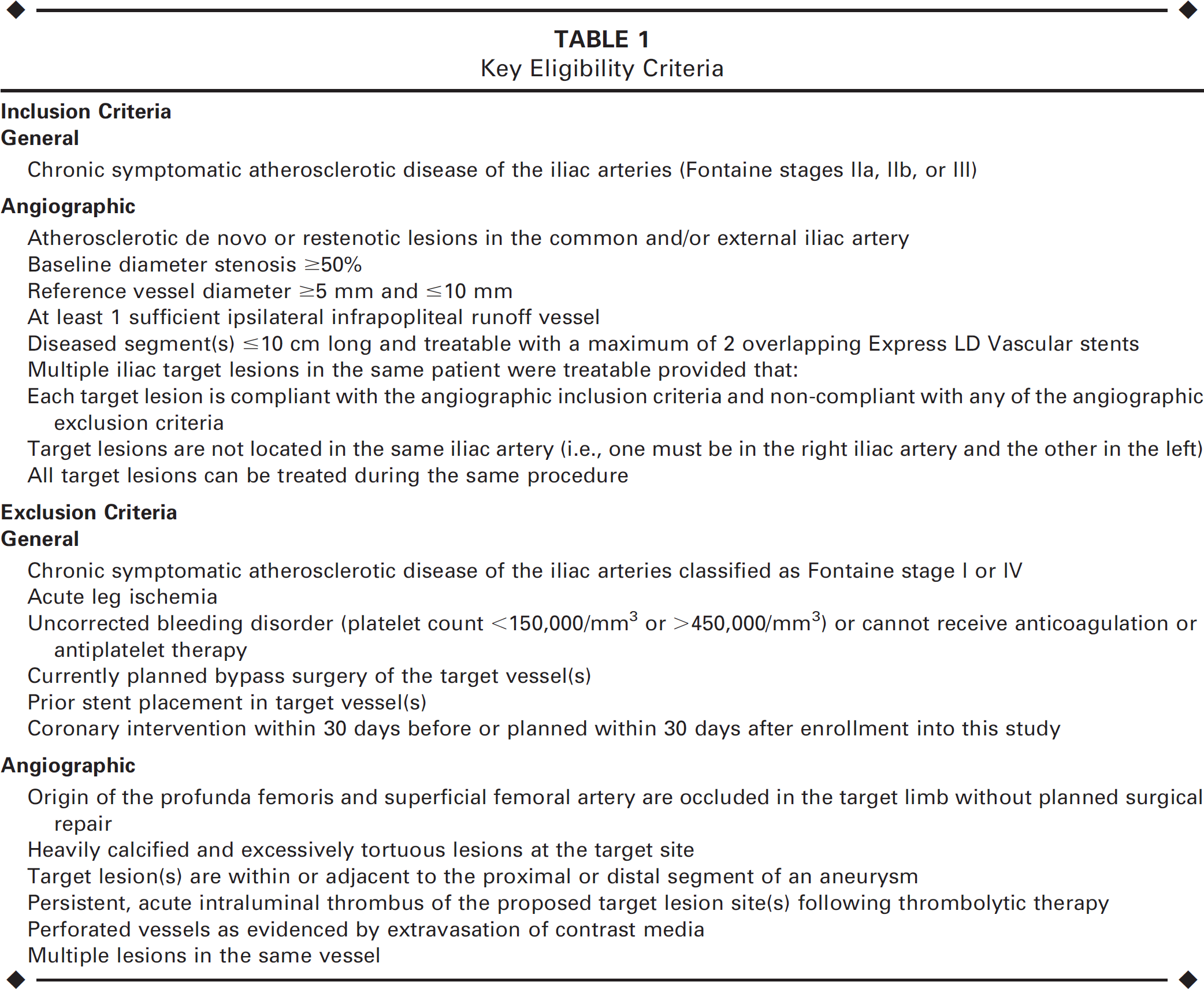
Ten investigative centers (9 in Europe and 1 in Canada; see the Appendix) participated in the study after receiving approval from their local institutional or human ethical review boards. All patients provided written informed consent and indicated a willingness to comply with study protocols. Patients were eligible to participate in the study if they had Fontaine stage 16 IIa, IIb, or III symptoms and a de novo or restenotic iliac artery lesion with visually estimated stenosis ≥50%. The lesion had to be considered treatable with a maximum of 2 stents, and at least 1 ipsilateral infrapopliteal runoff vessel had to be patent. Patients with acute leg ischemia, heavily calcified or excessively tortuous lesions, or symptomatic atherosclerotic disease of Fontaine class I or IV were excluded from the study. Other inclusion and exclusion criteria for the trial are listed in Table 1. Patients were considered enrolled in the study when the guidewire was successfully passed through the target lesion.
Key Eligibility Criteria
Device Description
The Express LD Vascular Pre-mounted Stent System consists of a stainless steel balloon-expandable stent with platinum-iridium radiopaque markers pre-mounted on an over-the-wire stent delivery system equipped with a non-compliant balloon. Stents of 5 different lengths ranging from 17 to 57 mm with diameters between 6 and 10 mm were used in the study.
Procedure
Diagnostic angiography was performed on each patient prior to lesion treatment to assess the extent of the lesion and collateral flow; angiography was repeated immediately after stent placement to confirm proper stent positioning and deployment. Use of a stent system with an inflated diameter approximating the diameter of the reference vessel was recommended. Pre- and postdilation were performed at the discretion of the investigator to facilitate stent delivery and optimize deployment. All patients received anticoagulant and/or antiplatelet therapy according to the routine practice of the study center. After the procedure, aspirin (100 mg/d) was continued throughout the entire follow-up phase of the study; if aspirin was contraindicated, clopidogrel (75 mg/d) or ticlopidine (250 mg BID) was administered as a substitute.
Patient Population
From January 2004 to February 2005, 151 patients (113 men; mean age 60.1±8.4 years) with 163 lesions in 159 limbs were enrolled and treated at 10 study centers. Table 2 summarizes the baseline patient and lesion characteristics. The mean patient age was 60.1±8.4 years, 87.4% were past or current smokers, 12.6% had medically treated diabetes, and 10.7% had been previously treated for atherosclerosis in the iliac artery. A total of 83.3% of patients experienced claudication when walking a distance of >200 m. The mean lesion length and diameter stenosis were 32.0621.7 mm and 62.9%, respectively. A majority of lesions were classified as TASC (TransAtlantic InterSociety Consensus) 19 type A (45.1%) or B (39.1%).
Baseline Characteristics of 151 Patients With 163 Iliac Target Lesions
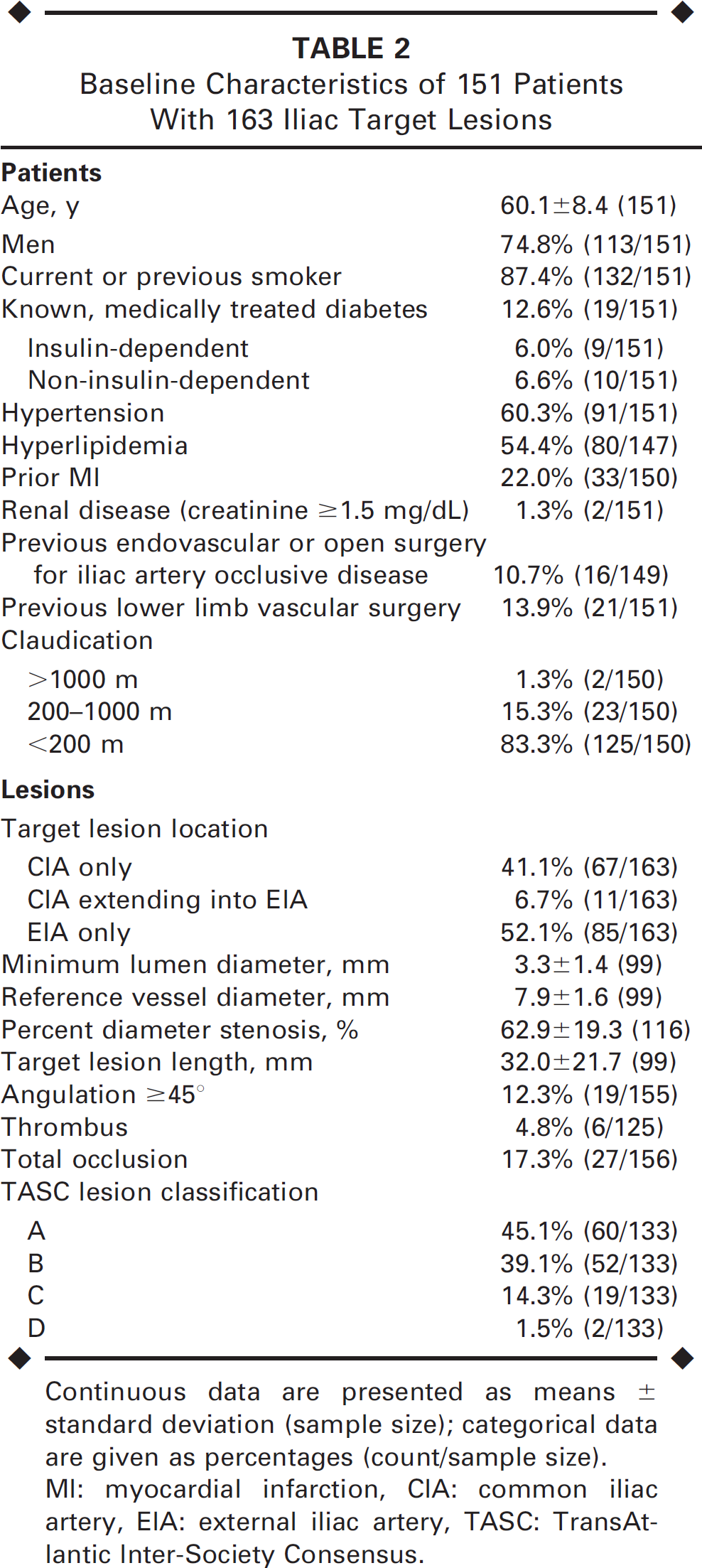
Continuous data are presented as means ± standard deviation (sample size); categorical data are given as percentages (count/sample size).
MI: myocardial infarction, CIA: common iliac artery, EIA: external iliac artery, TASC: TransAtlantic Inter-Society Consensus.
Follow-up and Imaging Analysis
Follow-up assessments included ankle-brachial index (ABI) measurement and symptom assessment (Fontaine classification) at discharge, 30 days, and 6, 12, and 24 months. Arteriography was performed at 6 months and computed tomographic angiography (CTA) at 1 and 2 years. Quantitative vessel analysis (QVA) was performed on all available angiograms by an independent core laboratory (Bio-Imaging Technologies, Leiden, The Netherlands) using the QVA-CMA system (MEDIS Medical Imaging Systems, Leiden, The Netherlands); the core laboratory also analyzed the CTA datasets.
Endpoints
The primary endpoint was the angiographic mean percent loss of luminal diameter at 6 months post procedure. This parameter was calculated using minimum luminal diameter (MLD) as follows: [(postprocedure MLD - follow-up MLD)/(postprocedure MLD)] X 100.
Key secondary endpoints included (1) cumulative rate of major adverse events (MAE), defined as device- or procedure-related death, target lesion revascularization (TLR), and device-related distal embolization that required hospitalization and/or subsequent intervention; (2) technical success, defined as successful stent implantation with residual stenosis >30%; (3) procedural success, defined as technical success in the absence of in-hospital MAE; (4) improvement in the ABI; (5) improvement in clinical symptoms as measured by the Fontaine classification; (6) patency as defined according to Society for Interventional Radiology standards 17 ; and (7) percent diameter stenosis. All MAEs were adjudicated by an independent Clinical Events Committee (see the Appendix).
Statistical Analysis
Data analyses were performed on an intent-to-treat basis. In MELODIE, the primary endpoint of mean percent lumen diameter loss was compared to an OPC in order to assess non-inferiority of iliac stenting with the Express LD Vascular stent to stenting with the Palmaz stent. Based on historical outcomes with the Palmaz stent, 15 15% lumen diameter loss was chosen as the OPC. A non-inferiority delta of 5% was added to the OPC to yield a non-inferiority boundary of 20%. A 1-sided Z test was used to test the 1-sided hypothesis of non-inferiority. Pooling of clinical data across study centers was justified using the Kruskal-Wallis test to demonstrate that mean angiographic percent loss of luminal diameter at 6 months was not substantially different across centers. P values for comparisons of continuous variables were calculated using the t test. The distribution of the Fontaine classification at baseline was compared to the 30-day, 6-month, and 1- and 2-year follow-up visits using the test of marginal homogeneity. 18 All statistical analyses were conducted using SAS (version 8.2; SAS Institute, Cary, NC, USA); p<0.05 was considered to indicate a significant difference.
RESULTS
Immediate Outcomes
In the 163 lesions treated, predilation was performed in 22.1% and postdilation in 5.5%. The majority of patients (78.1%) had a single stent implanted. A total of 41.1% of stents were placed in the common iliac artery (CIA) and 52.1% in the external iliac artery (EIA); 6.8% of stents extended from the CIA into the EIA. Technical success, defined as successful stent implantation with residual stenosis <30%, was achieved in 98.0% of the lesions treated. The 3 technical failures were due to stenosis >30% (31.2%, 32.9%, and 33.1%). Procedural success (technical success and no in-hospital MAE) was attained in 97.1% of patients. The 4 procedure failures included the 3 technical failures and 1 MAE prior to hospital discharge. The postprocedure in-stent diameter stenosis was 10.2%±9.0%, decreased from the baseline measurement of 62.9% (Table 3).
QVA Measurements of 163 Lesions From Baseline Through 6 Months
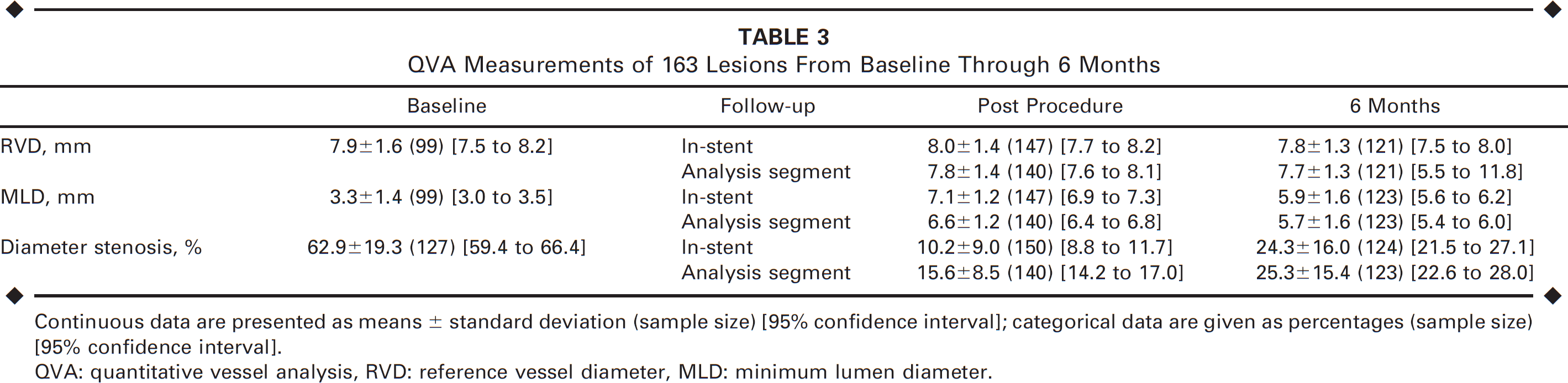
Continuous data are presented as means 6 standard deviation (sample size) [95% confidence interval]; categorical data are given as percentages (sample size)[95% confidence interval].
QVA: quantitative vessel analysis, RVD: reference vessel diameter, MLD: minimum lumen diameter.
QVA and CTA Results
Compliance with the clinical follow-up schedule was 92.0% at 6 months, 89.9% at 1 year, and 86.6% at 2 years. Follow-up with QVA at 6 months and CTA at 12 and 24 months was performed in 81.3%, 83.1%, and 83.8% of patients, respectively.
At 6 months, the mean percent luminal diameter loss by QVA for the Express LD Vascular stent was 16.2%618.4% with an upper 95% confidence boundary of 19.1%, which was below the 20% OPC plus delta value. Thus, the primary endpoint was met, indicating non-inferiority to the Palmaz stent (p=0.006). Baseline, postprocedure, and 6- month angiographic results are shown in Table 3. The mean in-stent percent diameter stenosis was 24.3%±16.0% at 6 months (by angiography) and 34.7% at 12 months and 34.5% at 24 months (by CTA).
Safety and Efficacy
Table 4 shows safety and efficacy outcomes over the course of the study. The composite MAE rate, which was 6.3% at 6 months, 8.9% at 1 year, and 10.2% through 2 years, was entirely driven by TLR because there was no distal embolization or device-/procedure-related deaths. The cumulative all-cause mortality rate was 6.9% at 2 years. Of the 9 deaths that occurred in the study, 3 were from cardiovascular causes, 5 were from cancer, and 1 was from respiratory insufficiency.
Summary of Clinical Results Across the Trial
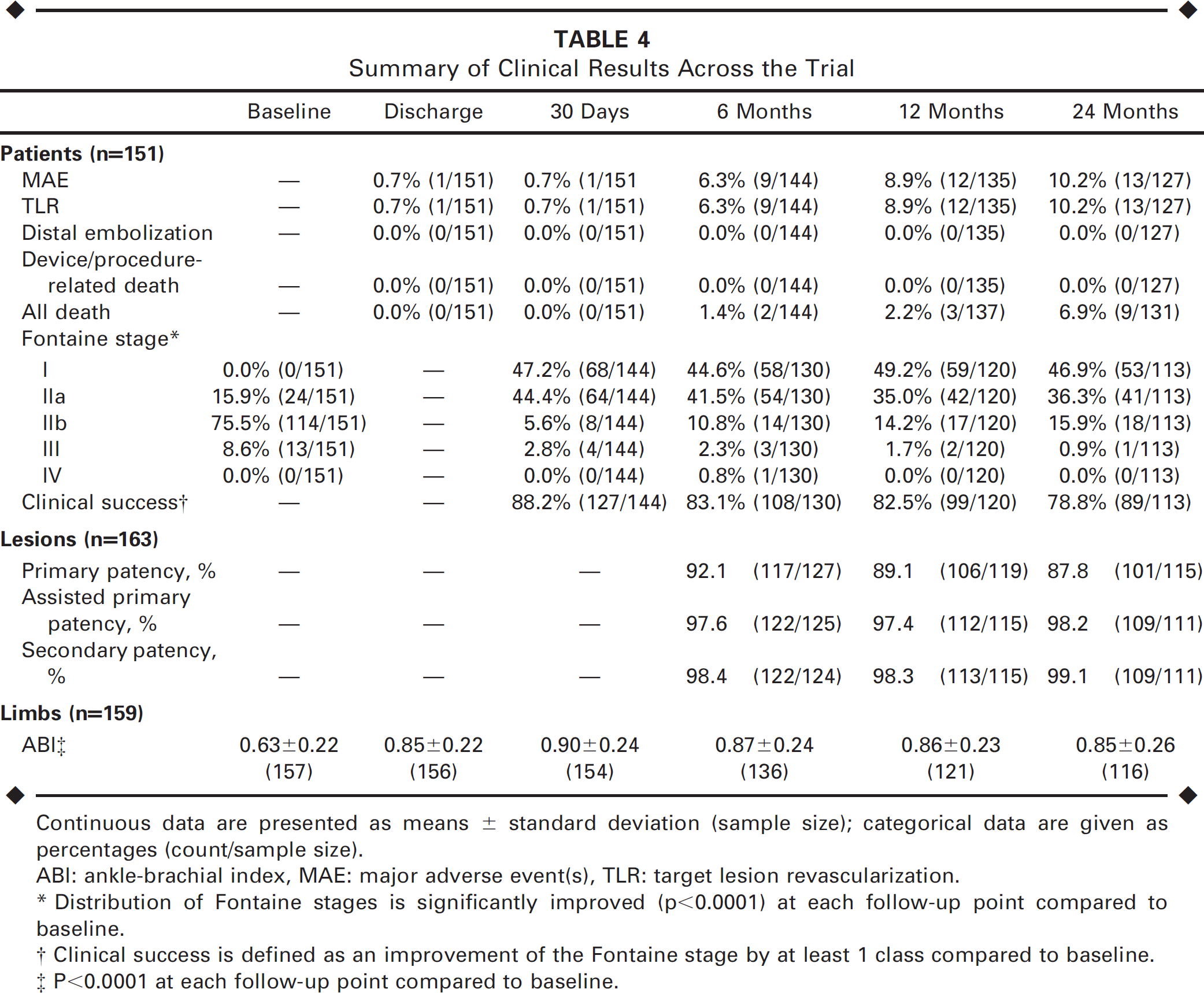
Continuous data are presented as means ± standard deviation (sample size); categorical data are given as percentages (count/sample size).
ABI: ankle-brachial index, MAE: major adverse event(s), TLR: target lesion revascularization.
Distribution of Fontaine stages is significantly improved (p≤0.0001) at each follow-up point compared to baseline.
Clinical success is defined as an improvement of the Fontaine stage by at least 1 class compared to baseline.
P<0.0001 at each follow-up point compared to baseline.
Primary patency was maintained in 92.1% of patients at 6 months, 89.1% at 12 months, and 87.8% at 24 months. Through 2 years, assisted primary patency and secondary patency were attained in 98.2% and 99.1% of patients, respectively.
Patients in the MELODIE trial experienced significant clinical improvement after iliac stenting. Prior to the index procedure, 84.1% of subjects had symptoms classified as Fontaine stage IIb or worse; 24 months later, only 16.8% of patients had symptoms classified as Fontaine stage IIb or worse (p<0.0001). Sustained enhanced perfusion of the lower extremity was demonstrated by the significant ABI improvement in the affected limb from 0.63±0.22 at baseline to 0.85±0.26 (p<0.0001) at 2 years.
DISCUSSION
The MELODIE trial is the first prospective study to evaluate the balloon-expandable Express LD Vascular stent for treatment of iliac artery stenosis. The results demonstrated that in the treatment of stenosis in the CIA or EIA, the Express LD stent was non-inferior to an OPC designed to represent outcomes with the Palmaz stent, a first-generation iliac stent. The types of patients and lesions treated in the MELODIE study were similar to those in the Palmaz study 15 ; average lesion length in both studies was 32 mm. A slightly greater proportion of patients in the MELODIE study had complete occlusion of the target lesion (17.2%) compared to the Palmaz study (13.5%), 15 while a slightly lower proportion of MELODIE versus the Palmaz patients had diabetes (12.6% versus 22.9%). 15 The distribution of stent placement location was slightly different between the 2 trials. In the Palmaz study, 15 stents were placed in the CIA, EIA, or spanning both in 66.5%, 19%, and 13.1% of patients, respectively, while in MELODIE, 41.1% and 52.1% of stents were placed in the CIA and EIA, respectively, and 6.8% of stents spanned both vessels.
The Palmaz stent was chosen as a comparator for this study because this was the only balloon-expandable stent with 6-month angiographic data described in the peer-reviewed literature when the study was initiated. However, the Palmaz stent required the operator to hand-crimp the stent onto a balloon; it was also relatively stiff and inflexible and had only half the radial strength of Express LD. As a result, it has generally been replaced by newer stents for iliac stenting. Thus, although MELODIE was designed to compare the Express LD Vascular stent to outcomes expected with the Palmaz stent, a comparison of outcomes in MELODIE with outcomes from more modern stents may be of greater relevance, given the current state of clinical practice.
While it is difficult to directly compare results across trials due to potential differences in patient populations, study design, and study execution, outcomes in MELODIE are similar to those seen in other iliac stenting trials.6,7,20–23 Like MELODIE, other trials have shown high rates of technical and procedural success and low rates of periprocedural mortality. For example, procedural success rates for the Zilver, SMART, Perflex, Symphony, and AVE Bridge stents were 98.0%, 20 98.2%, 6 94%, 7 95%, 24 and 100%, 23 respectively. The Wallstent and Jostent SelfX demonstrated technical success rates of 99% 25 and 94%, 21 respectively. In this same set of trials, mortality rates at 30 days following the procedure were 2.1%, 20 2.0%, 6 0.8%, 7 2.6%, 23 3.1%, 24 0%, 25 and 0%, 21 respectively. The Express LD stent, with a procedural success rate of 97.1% and a 30-day mortality rate of 0.0%, showed comparable results.
The 6-month and 1-year primary patency rates of 95.2% and 89.8% reported in the MELODIE trial were similar to the rates seen in other studies, although patency definitions varied across trials. Primary patency in the Zilver, SMART, Wallstent, Perflex, Jostent SelfX, Carnevale Iliac Occlusion Study, Symphony, and AVE Bridge trials were 92.9% at 9 months, 20 94.7% at 1 year, 6 91.1% at 1 year, 6 89% at 1 year, 7 96% at 1 year, 21 87% at 2 years, 26 97.0% at 6 months, 24 and 82.7% at 6 months, 23 respectively. In the MELODIE trial, primary patency at 2 years was 87.8%, demonstrating the durability of the results.
Patients in the MELODIE trial also demonstrated clinical and hemodynamic improvements comparable to those seen in other trials. The mean ABI improvement at 6 or 12 months ranged from 0.19 to 0.37 in the Zilver, 20 SMART, 6 Wallstent, 6 Perflex, 7 Jostent SelfX, 21 Symphony, 24 and AVE Bridge 23 stent trials. Similarly, patients treated with the Express LD Vascular stent showed ABI improvement from a baseline value of 0.63 to 0.85 at 2 years.
Clinical improvement, based on improved walking scores in the Zilver trial 20 and by Rutherford/Becker score improvement6,21,23 in the SMART, Wallstent, Jostent SelfX, and AVE Bridge trials, was also observed in the MELODIE trial. Eighty-eight percent of patients receiving the Express LD Vascular stent improved by at least 1 Fontaine class 30 days after the procedure; this improvement was maintained through 2 years.
Limitations
A significant limitation of the MELODIE trial was that it was a non-randomized, single-arm study that used a first-generation iliac stent as a comparator. Nevertheless, iliac stenting has been well-studied, and there is a significant body of evidence to which the Express LD Vascular stent can be compared.
A second key limitation was that the study was not powered to evaluate outcomes in subgroups or variables that might be predictive of patency. Limitations of the Express LD stent, and other balloon-expandable stents in general, include reduced flexibility and resistance to external compression compared to self-expanding stents 10 ; balloon-expandable stents also potentially cause greater stress and damage to the vessel wall than their self-expanding counterparts. 14
Conclusion
The MELODIE trial demonstrates the safety and effectiveness of iliac stenting with the balloon-expandable Express LD Vascular stent. The data confirm that iliac stenting, in general, can be performed safely and with significant benefits to patients. The 2-year clinical and angiographic follow-up data presented also document the durability of these benefits over time.
Footnotes
Acknowledgements
Acknowledgments: The authors thank Jill Bleuit, PhD, and Ed McMullen, Mmath, of Boston Scientific Corporation for assistance with manuscript preparation and biostatistical analyses, respectively.