
Abstract
In the 30 years since carotid angioplasty was first reported, carotid artery stenting (CAS) has emerged as an alternative to carotid endarterectomy for the treatment of carotid artery disease. In a 2500-patient randomized trial, the recently published CREST (Carotid Revascularization Endarterectomy versus Stent Trial) data showed that the risk of stroke, myocardial infarction, or death did not differ significantly in the group undergoing CAS and the patients undergoing carotid endarterectomy, regardless of symptom status. 1
The progression of supra-aortic vessel angioplasty and stenting to this position has been facilitated/accompanied by the development of dedicated tools for the procedure (wires, guiding catheters, long sheaths, balloons, stents, multiple cerebral protection devices) and creative and refined techniques, such as the one described by Ryer and Oderich 2 for innominate artery stent placement.
Lesions of the innominate artery become symptomatic as a result of obstruction of blood flow to the common carotid artery (CCA) and subclavian artery (SA) or embolization from subtotal occlusions that can lead to anterior or posterior circulation stroke. Surgical treatment requires a trans-thoracic procedure, which is associated with considerable morbidity and mortality rates. According to recent reports, endovascular treatment has been performed with satisfactory results and low complication rates. 3
For many years, lesions located at the origin of the innominate artery, left CCA, and left SA were included in the list of “safe endovascular procedures” that could be done even without protection. We now know that embolization during arterial angioplasty and stenting is universal and unpredictable; sensitive organs such as the brain should be protected to avoid symptomatic or silent brain infarcts.
The “2-wire technique” by Ryer and Oderich brings to the table a safe way to protect the anterior circulation using a filter delivered over a 0.014-inch guidewire to the CCA or internal carotid artery (ICA). The lesion is then crossed from above with support from a guiding sheath using a 0.018-inch guidewire in a “through-and-through” configuration. The combination of these 2 different size guidewires came from a simple observation that 0.014 + 0.018 = 0.032, which is smaller than the 0. 035-inch lumen of the balloon-expandable stent shaft used for the treatment of these lesions. Therefore, the device can and should be mounted and tracked to the target lesion over both wires at the same time. If, for any reason, the stent delivery system is mounted over only the 0.018-inch guidewire and the stent is deployed, the carotid filter would be jailed around the stent, and retrieval of the filter may became impossible without conversion to conventional surgery.
The “through-and-through technique,” also known as “body floss technique,” is very useful to improve trackability and stability of devices in tortuous and/or narrow vascular anatomy. When a long guidewire is pulled by both ends from different access sites, it becomes a perfect rail for device advancement, but at the same time, it behaves like a sharp blade that can produce endothelial damage, vessel dissection, and even complete vessel transection. The use of a catheter covering the wire, ideally along its entire length, is mandatory to avoid such catastrophic complications.
The 2-wire technique provides protection to the anterior circulation with a filter but leaves the posterior circulation unprotected, exposing the patient to a potential embolic complication at the vertebrobasilar territory. This event was seen in 2% of the 89 patients treated without any protection by Hüttl et al. 4 The use of a 5-F occlusion balloon catheter can serve a double purpose: preventing the wire from damaging the vessels and protecting the vertebral artery by inflating the balloon at the origin of the SA, thus redirecting all the flow to the filter-protected carotid artery.
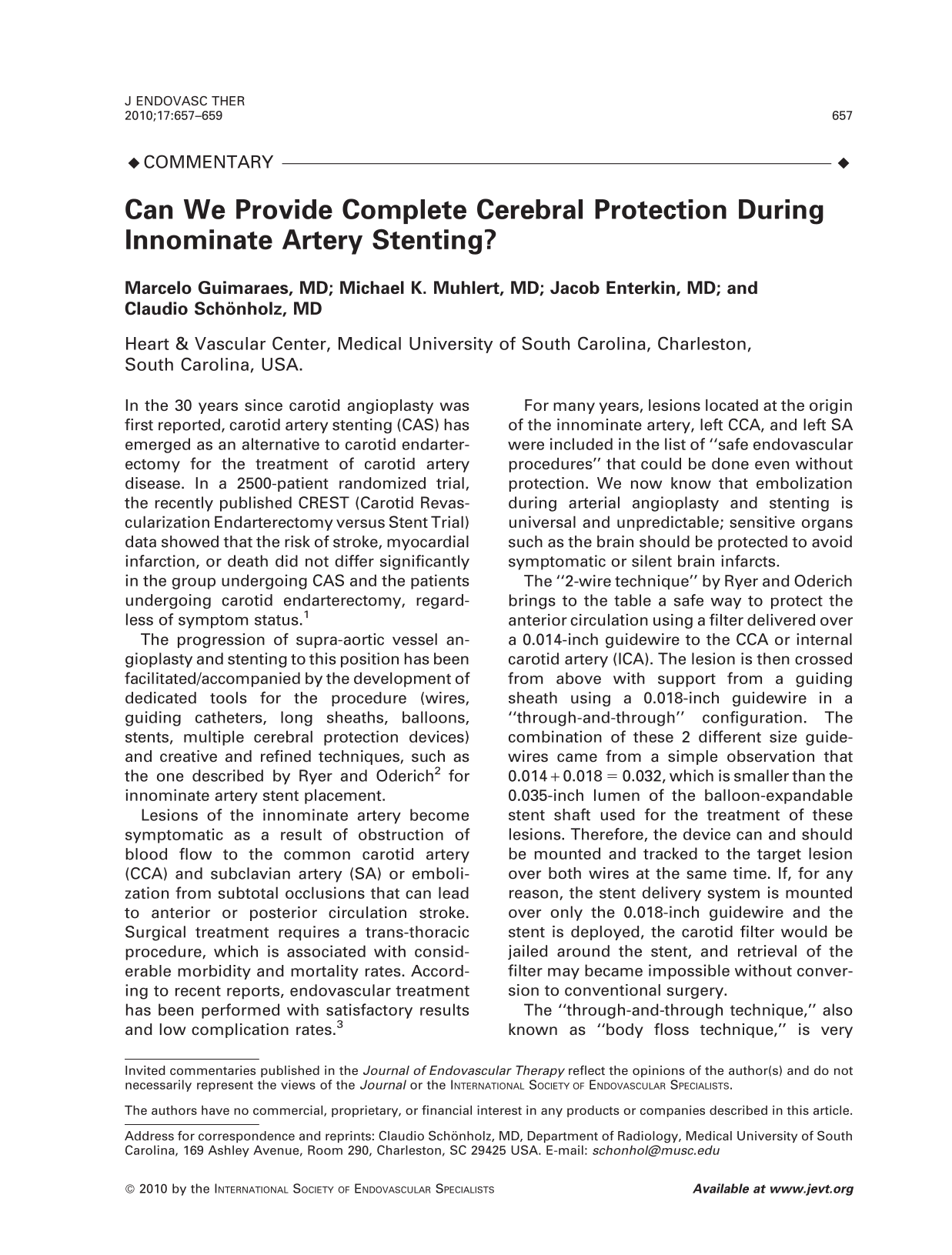
After reviewing Ryer and Oderich's technical note, we had the opportunity to apply this useful technique in a 76-year-old patient with recent history of right middle cerebral artery territory stroke and recurrent transient ischemic attacks. Computed tomographic angiography showed a subocclusive, calcified innominate artery stenosis confirmed by angiography (Figure, A). The procedure we used incorporated some modifications and improvements in the technique mentioned above.
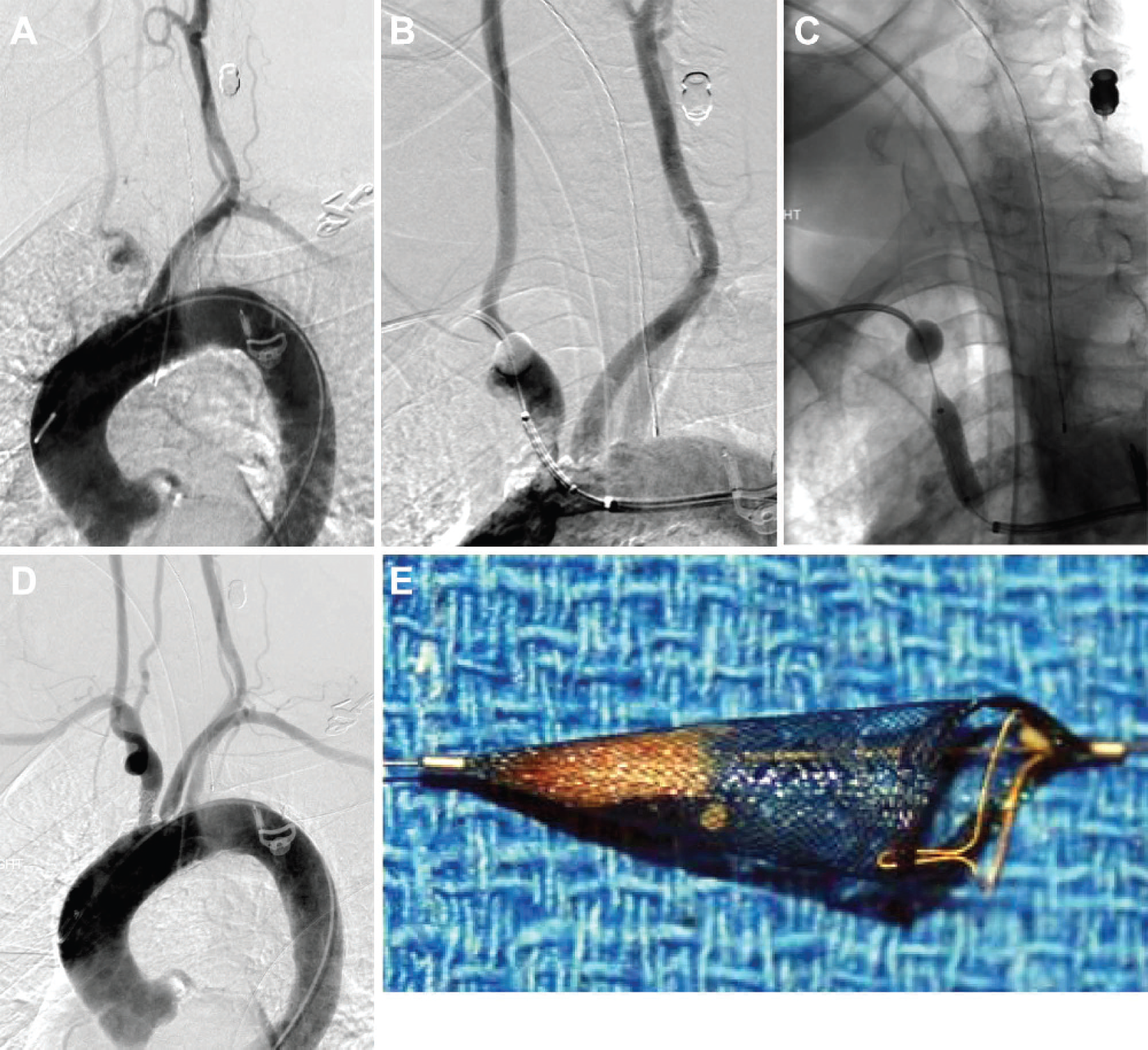
(
Under general anesthesia (due to patient comorbidities), the lesion was crossed from a brachial access with a 0.018-inch, 300-cm V18 guidewire (Boston Scientific, Natick, MA, USA), which was snared at the abdominal aorta to avoid the risk of cerebral embolization during snare manipulation. A 7-F Shuttle sheath (Cook Medical, Bloomington, IN, USA) placed from the groin was used as the access for the 25-mm snare. Once the wire was pulled out of the femoral access, a 4-F, 120-cm-long vertebral catheter was used to cross the lesion. Through this catheter a 0.014-inch guidewire was advanced in parallel to the 0.018-inch guidewire and, under roadmapping, advanced safely into the right ICA. Over the 0.014-inch guidewire, a 6-mm carotid Spider filter (ev3 Inc., Plymouth, MN, USA) was advanced and deployed at the proximal ICA. In order to prevent wire damage to the brachial, axillary, and subclavian arteries during advancement of the guiding catheter using the through-and-through technique, a 5-F occlusion balloon catheter was advanced through the brachial 6-F sheath to the origin of the SA. By inflating the balloon of this catheter at the SA origin during innominate artery predilation and stent placement, all blood flow was directed to the filter-protected carotid artery, preventing embolization in the vertebrobasilar territory (Figure, B). In this symptomatic patient with an ulcerated and calcified lesion, a balloon-expandable 7×22-mm covered stent (Advanta V12; Atrium, Hudson, NH, USA) was deployed with the intention of excluding the plaque from the circulation. A covered stent was selected to prevent plaque protrusion through the stent struts (Figure, C and D). At the end of the procedure, the subclavian balloon was deflated and the carotid filter retrieved. Examination of the filter (Figure, E) showed a large amount of plaque material, which demonstrates the need for cerebral protection during these procedures.
In conclusion, the 2-wire technique is an important contribution to the field of endovascular procedures, and Drs. Ryer and Oderich should be congratulated for sharing this creative technique. We have integrated a 5-F occlusion balloon to improve the safety of the through-and-through technique and achieved complete cerebral protection by balloon occlusion of the SA.