
Abstract
Purpose
To determine the efficacy of sirolimus-eluting bioabsorbable magnesium alloy stents (SEBMAS) in restenosis prevention.
Methods
A balloon-expandable bioabsorbable magnesium alloy stent (BMAS) was created and coated with biodegradable poly(lactic acid-co-trimethylene carbonate) that contained the antiproliferative drug sirolimus (140±40 μg/cm2). Both the uncoated BMAS and the coated SEBMAS were deployed 2 cm apart in balloon-injured infrarenal abdominal aortas of 20 New Zealand white rabbits. The stented aortic segments were removed at 30, 60, 90, and 120 days (5 rabbits per interval) after implantation. The average stent strut sectional area of each group was measured to evaluate the degree of magnesium corrosion and to forecast the biodegradation time profile of the magnesium stent. Histology and histopathology of the sectioned stented aortic segments were performed to evaluate neointima formation, endothelialization, and inflammation.
Results
The SEBMAS degraded gradually after being implanted into the rabbit aorta, and total biocorrosion occurred after ∼120 days. In all groups, the lumen area was significantly greater, but the neointimal area was significantly smaller in SEBMAS segments compared with the uncoated BMAS segments (p<0.05) at all time points. There was no significant difference in the injury or inflammation scores between the groups. Endothelialization was delayed at 30 days in the SEBMAS segments vs. the uncoated BMAS segments.
Conclusion
SEBMAS further reduces intimal hyperplasia and improves the lumen area when compared to uncoated BMAS; however, it delays vascular healing and endothelialization.
Keywords
Because drug-eluting stents (DES) reduce neointima formation compared to uncoated (bare metal) stents, they have gained popularity and become an established method of treatment in percutaneous cardiovascular interventions.1–3 However, after the drug has eluted, DES pose problems similar to those of bare metal stents. They are permanent foreign bodies that continuously interact with the surrounding tissue, potentially leading to long-term endothelial dysfunction or chronic inflammatory reaction. These interactions are possible contributors to late restenosis.4,5
Degradable implants may act as a new biomedical tool that fulfill a mission and then dissolve. Advantages are a more physiological repair, reconstitution of local vascular compliance, and a temporary, limited, longitudinal and radial straightening effect, including the possibility of growth. 6 However, most biodegradable polymer stents have limited success because of their low radial strength and local inflammation. 7 Among the corrodible metals that have been considered as alternatives, 8 biodegradable magnesium alloy stents (BMAS) have been proven to be safe. 9 However, preliminary preclinical and clinical trials demonstrated that, despite a modest degree of neointima formation and late negative vascular remodeling, these stents were associated with higher restenosis rates than seen in DES.8–11 To address this issue, we developed a new type of sirolimus-eluting bioabsorbable magnesium alloy stent (SEBMAS) made of AZ31B magnesium alloy; this stent combines the characteristics of antiproliferation and a long corrosion period. We anticipated that this stent would provide a combination of limited neointima formation, enhanced mechanical stability, and complete degradation, which we evaluated in an in vivo experiment.
See commentary page 416
METHODS
Preparation of Sirolimus-Eluting Magnesium Alloy Stent
All materials used in stent construction were made by our research group (Institute of Metal Research, Chinese Academy of Sciences). The balloon-expandable BMAS were laser cut from a magnesium alloy (AZ31B) tube 3 mm in diameter and 15 mm in length, with a stent strut diameter of 155±5 μm. The surface was electrochemically polished and phosphorized to prolong the corrosion period. The stent (Fig. 1A) was then ultrasonically spray-coated with poly(lactic acid-co-trimethylene carbonate) [P(LA-TMC)] containing the antiproliferative agent sirolimus (mean 140±40 μg/cm2 per stent). The radial force of the stent was 92 kPa. The biocompatibility of the coating material was tested prior to this experiment using the platelet adhesion test (Fig. 1B,C). The in vitro hemolytic ratio and the prothrombin time in platelet-poor plasma of the sirolimus-eluting magnesium stent were 3.69%±0.12% and 15.67±0.42 seconds, respectively.
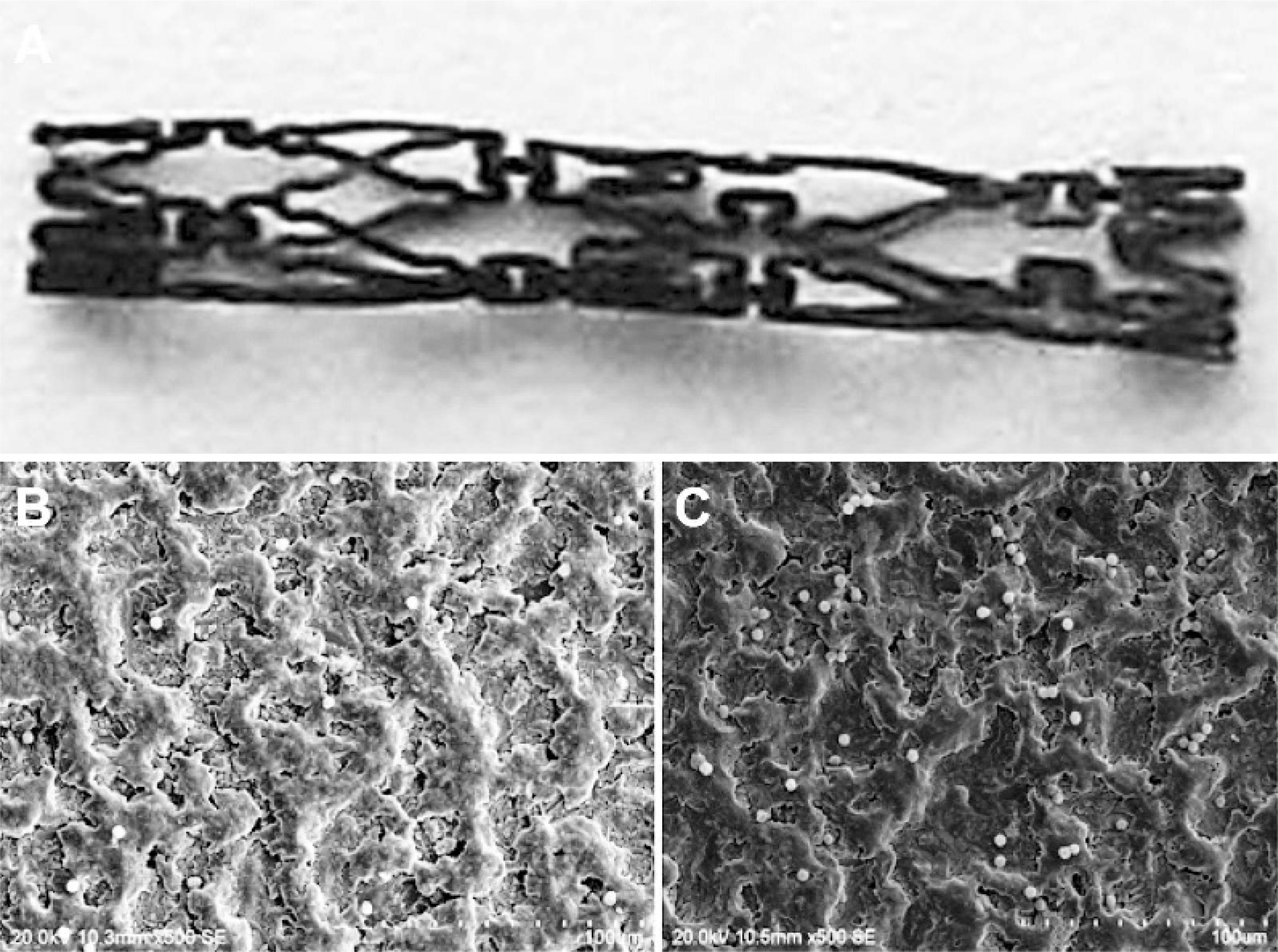
(
Study Design
Twenty young (∼6 months old) male New Zealand white rabbits weighing a mean 2.0±0.2 kg were housed, fed, and cared for according to guidelines of the Declaration of Helsinki; all procedures were approved by the Animal Care Committee in accordance with the guidelines of our university. Two stents were implanted in the infrarenal abdominal aorta of each rabbit: an uncoated BMAS proximally as a negative control and the SEBMAS distally. The 20 rabbits were divided randomly into 4 groups scheduled for sacrifice at 30, 60, 90, and 120 days after implantation. The stented aortic segments were removed and prepared for histology and histopathology to evaluate neointima formation, endothelialization, and inflammation.
Stent Implantation
Anesthesia was induced with administration of 25 mg/kg chlorpromazine and maintained with intravenous pentobarbital. A surgical incision was made in the neck, and the right carotid artery was exposed. A 5-F micropuncture set (Cook Inc., Bloomington, IN, USA) was inserted into the common carotid artery. A 4-F pigtail catheter (Terumo Medical Corporation, Somerset, NJ, USA) was introduced and pushed down to the thoracic aorta to obtain a highresolution aortogram of the abdominal aorta. The locations of the renal arteries were identified, and the diameter of the infrarenal abdominal aorta was measured as a basis for oversizing the stents. Heparin (200 U/kg) was administered through the catheter before stent placement to prevent thrombosis. The infrarenal abdominal aorta was balloon dilated to a ratio of 1:1.1 to 1:1.3. The SEBMAS and BMAS were deployed sequentially 2 cm apart in the distal and proximal infrarenal abdominal aorta, respectively, using 30 seconds of balloon inflation of 6 atm (the magnesium alloy stent is less stiff than stainless steel or other alloys, so a lower dilation pressure is adequate). The vessel-to-stent diameter ratio was within the range of 1:1.1 and 1:1.3. Completion aortography was performed to confirm the location of the stents and patency of the aorta. The right carotid artery was ligated, and the incision was sutured layer by layer. All animals received oral aspirin (2 mg/kg/d) until sacrifice to prevent thrombus formation.
Tissue Harvesting and In Vitro Radiographic Evaluation
Aortography was performed before the animals were euthanized with an overdose of pentobarbital (35 mg/kg). The stented aortic segments were flushed for 5 minutes with 200 to 300 mL of 0.9% NaCl containing 180 mg/L papaverine followed by pressure-perfusion fixation (100 mmHg) for 30 minutes and immersion fixation for 24 hours using 10% neutral-buffered formalin. After fixation, radiographs of the stented segments were taken at lower voltage (30 kV) to grossly evaluate the degree of corrosion in the low-density magnesium alloy.
Histology
The stented aortic segments were put into 10% nitric acid for 20 minutes to dissolve the remaining stent struts. The specimens were dehydrated in gradient alcohol, followed by defatification in xylene, and embedded in paraffin. Representative 5-μm sections from the proximal, middle, and distal portions of the stented aortic segments were stained with hematoxylin and eosin. The computer-assisted digital morphological analysis was done by an independent observer blinded to this study. The areas of the lumen, internal elastic lamina (IEL), and stent strut cross sections were measured. Based on these measurements, the neointimal area was determined by subtracting the area of the lumen from the IEL area.
Histopathology
The vessel injury score caused by the stent strut was determined according to Schwartz et al. 12 : grade 0 corresponded to an intact IEL, with the media compressed but not lacerated; grade 1 indicated a lacerated IEL, with the media compressed but not lacerated; grade 2 denoted a lacerated IEL and media, with the external elastic lamina (EEL) intact but compressed; and grade 3 corresponded to a lacerated EEL, with typically large lacerations of media extending through the EEL. A mean injury score and morphological parameters were calculated for each stented arterial segment. Stent strut inflammation was graded as 0: none; 1: scattered inflammatory cells; 2: inflammatory cells encompassing 50% of a strut over at least 25% to 50% of the circumference of the artery; or 3: inflammatory cells surrounding a strut over at least 25% to 50% of the circumference of the artery. The stent endothelialization score, defined as the extent of the lumen circumference covered by endothelial cells, was scored as 1 (≤25%) 2 (26%–75%), or 3 (≥76%).
Statistical Analysis
All values were expressed as mean± standard deviation. The time profile of bioabsorbable magnesium stent degradation was analyzed using the Pearson test, and the point of complete degradation was estimated from a scatter plot of stent strut cross-sectional area over time. Continuous data were compared using a paired t test, and categorical data were analyzed using a Mann-Whitney test. Analyses were conducted using Prism software (version 5.0; GraphPad Software, Inc., San Diego, CA, USA). P<0.05 denoted a statistically significant difference.
RESULTS
All stents were successfully implanted, and all the rabbits survived the scheduled follow-up period without evidence of systemic toxicity from the locally administered sirolimus. Aortography before sacrifice showed patency of the abdominal aorta in all rabbits without obstruction or thrombosis at the implantation site of stents. On gross examination of the explanted aortic segments, all were patent and without thrombus; none of the stents had migrated. Radiographs at 30 days after implantation revealed that most of the BMAS skeletons remained intact (Fig. 2A). At 60 days, some struts had lost their continuity, suggesting preliminary degradation (Fig. 2B). By 90 days, most struts had partially corroded (Fig. 2C), and by 120 days after implantation, most struts were completely corroded (Fig. 2D).
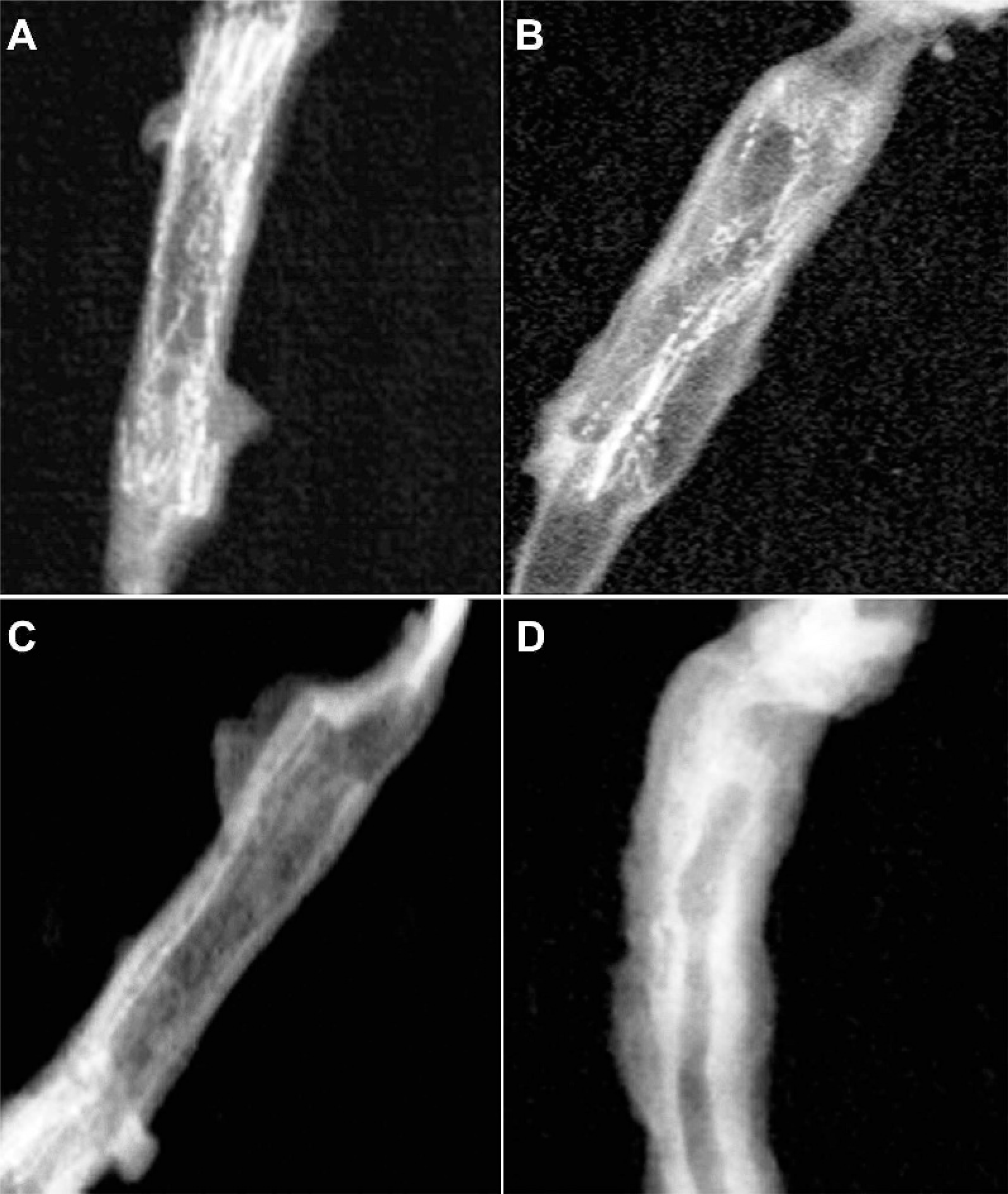
(
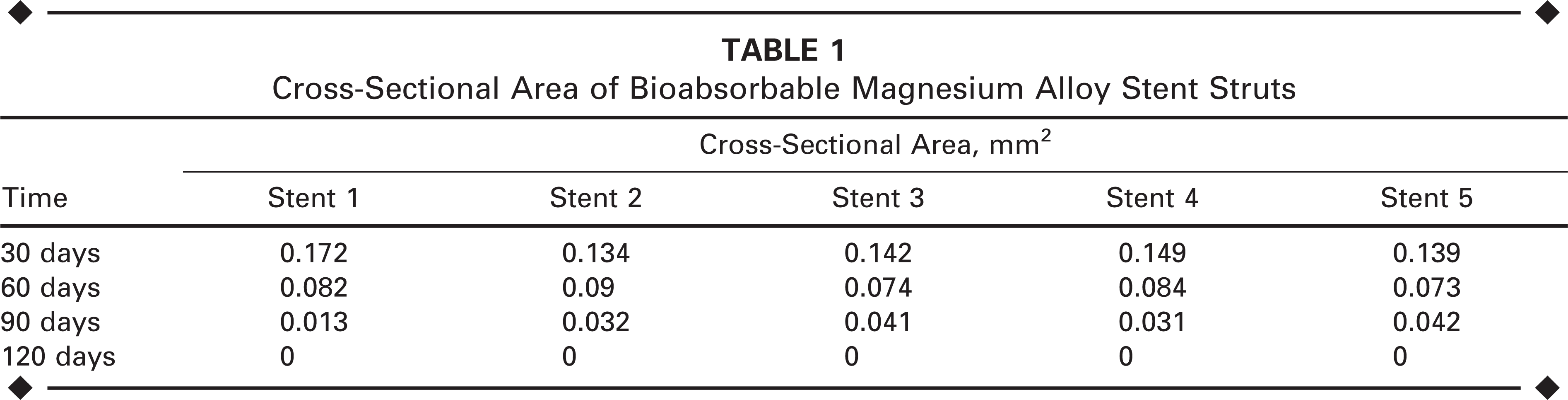
Neointima formation and inflammatory cell infiltration were seen in all groups on stained sections. The cross-sectional areas of the stent struts became smaller and smaller in direct relation to the time after implantation; by 120 days, the stent struts appeared to be absorbed since they were not evident in the cross sections (Fig. 3).
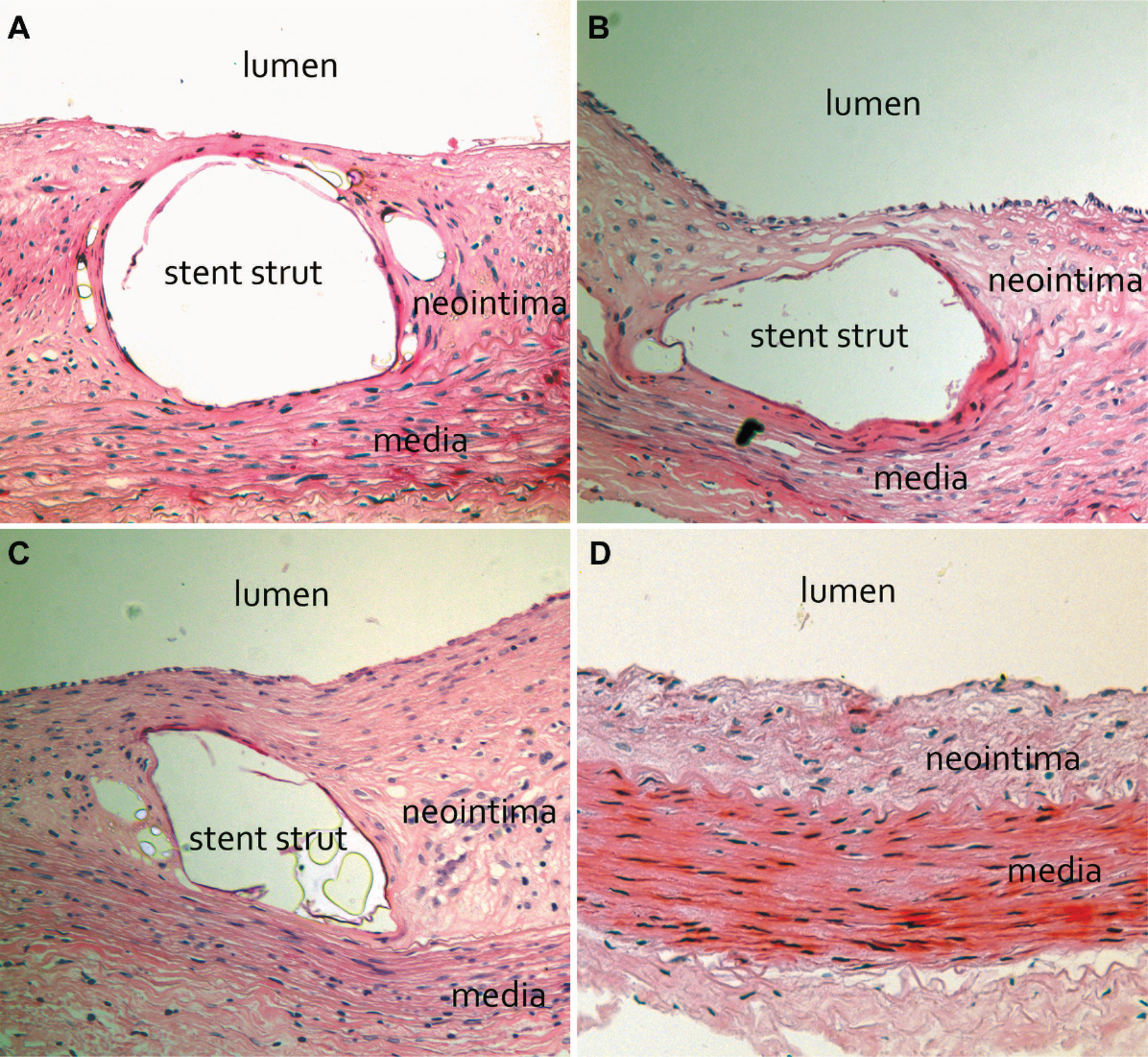
Cross sections of BMAS-stented aorta at (
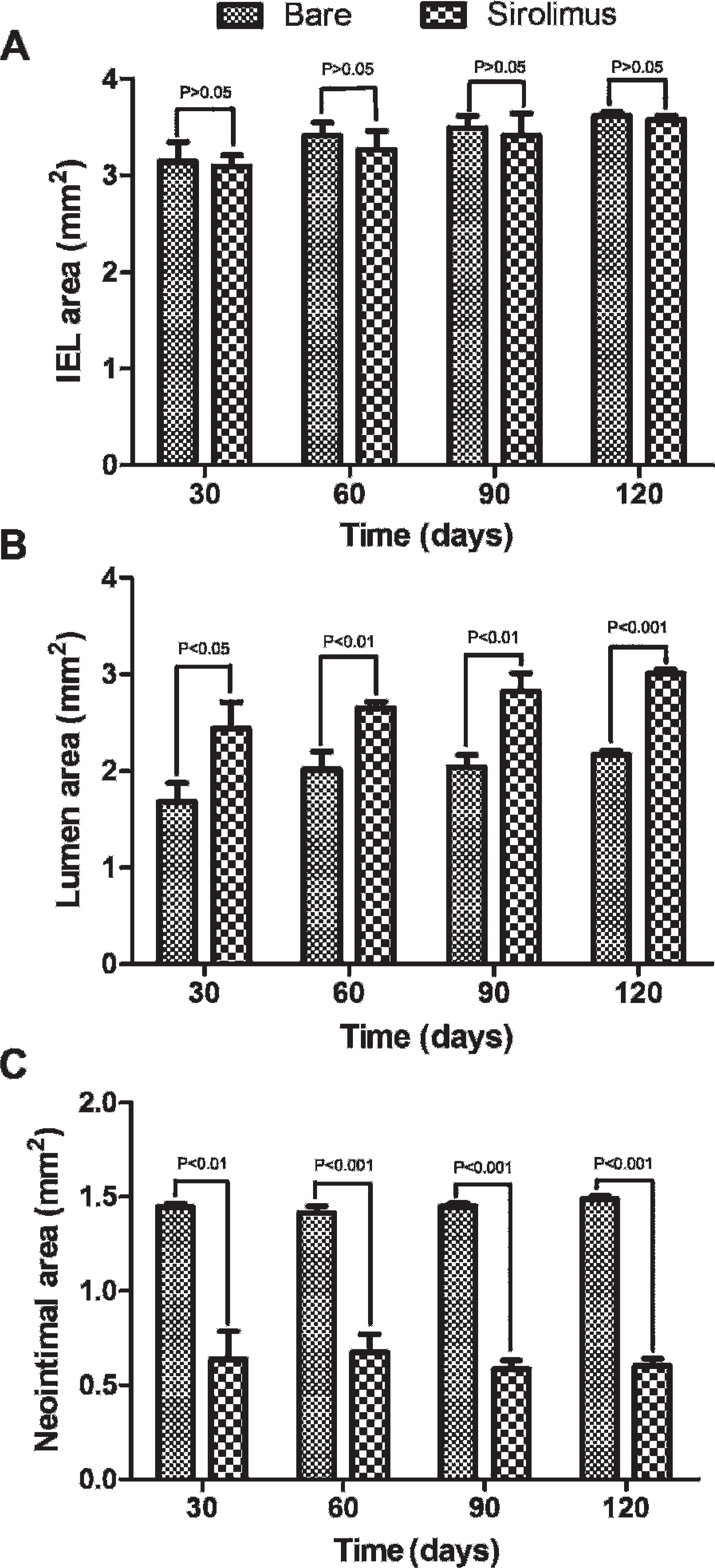
There was no significant difference of IEL area between BMAS and SEBMAS groups at any time point after implantation (Table 2 and Fig. 4A). The lumen area was larger in the SEBMAS group at 30 (p<0.05), 60 (p<0.01), 90 (p<0.01), and 120 days (p<0.001) after implantation (Fig. 4B). On the other hand, the neointimal area was smaller in the SEBMAS group at 30 (p<0.01), 60 (p<0.001), 90 (p<0.001), and 120 days (p<0.001) after implantation (Fig. 4C).
Cross-Sectional Area of Bioabsorbable Magnesium Alloy Stent Struts
Areas of the BMAS and SEBMAS Groups at Different Time Points
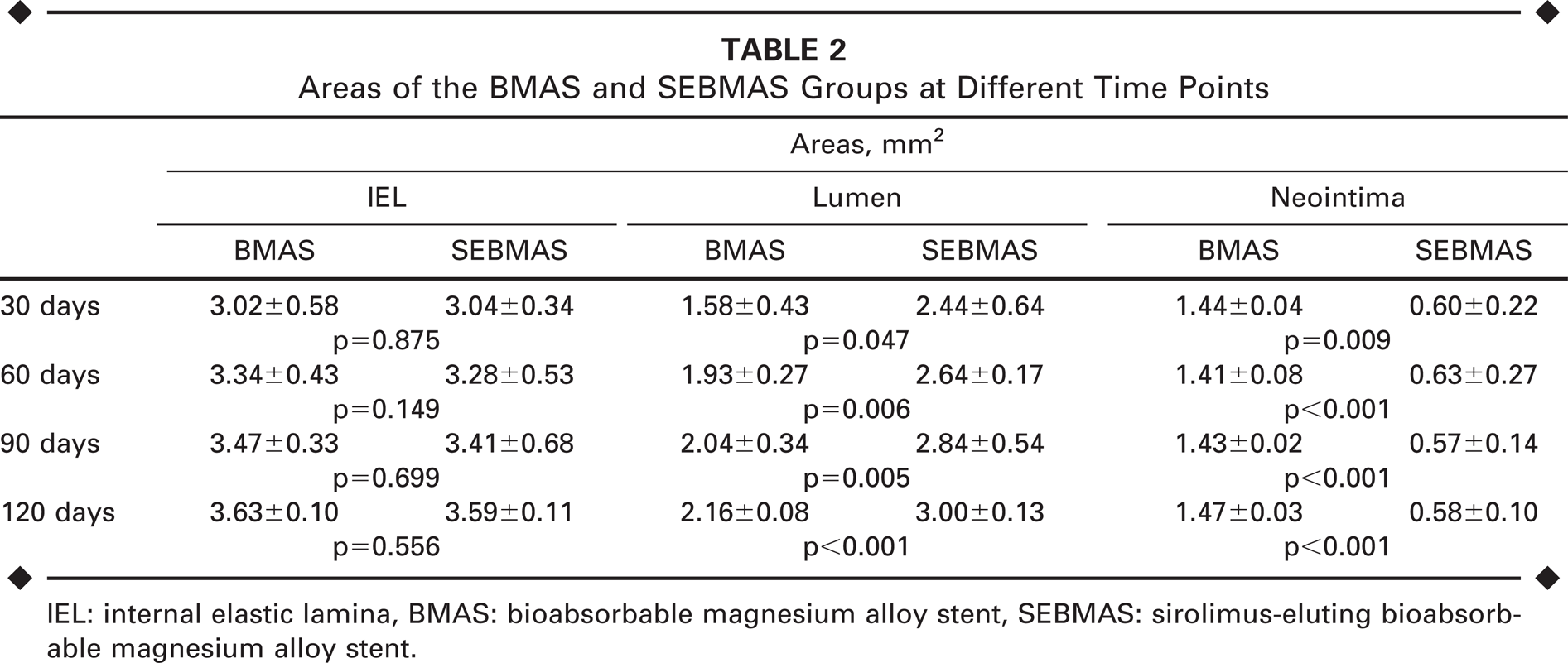
IEL: internal elastic lamina, BMAS: bioabsorbable magnesium alloy stent, SEBMAS: sirolimus-eluting bioabsorbable magnesium alloy stent.
(
The vessel injury and stent strut inflammation scores were not significantly different between the 2 groups at any time point (Fig. 5A,B). The stent endothelialization score was significantly lower in the SEBMAS group compared with the BMAS group at 30 days after stent implantation (1.0±0.21 vs. 2.45±0.35, p<0.01). However, with time, the stent endothelialization scores became similar in both groups at 60 through 120 days (Fig. 5C).
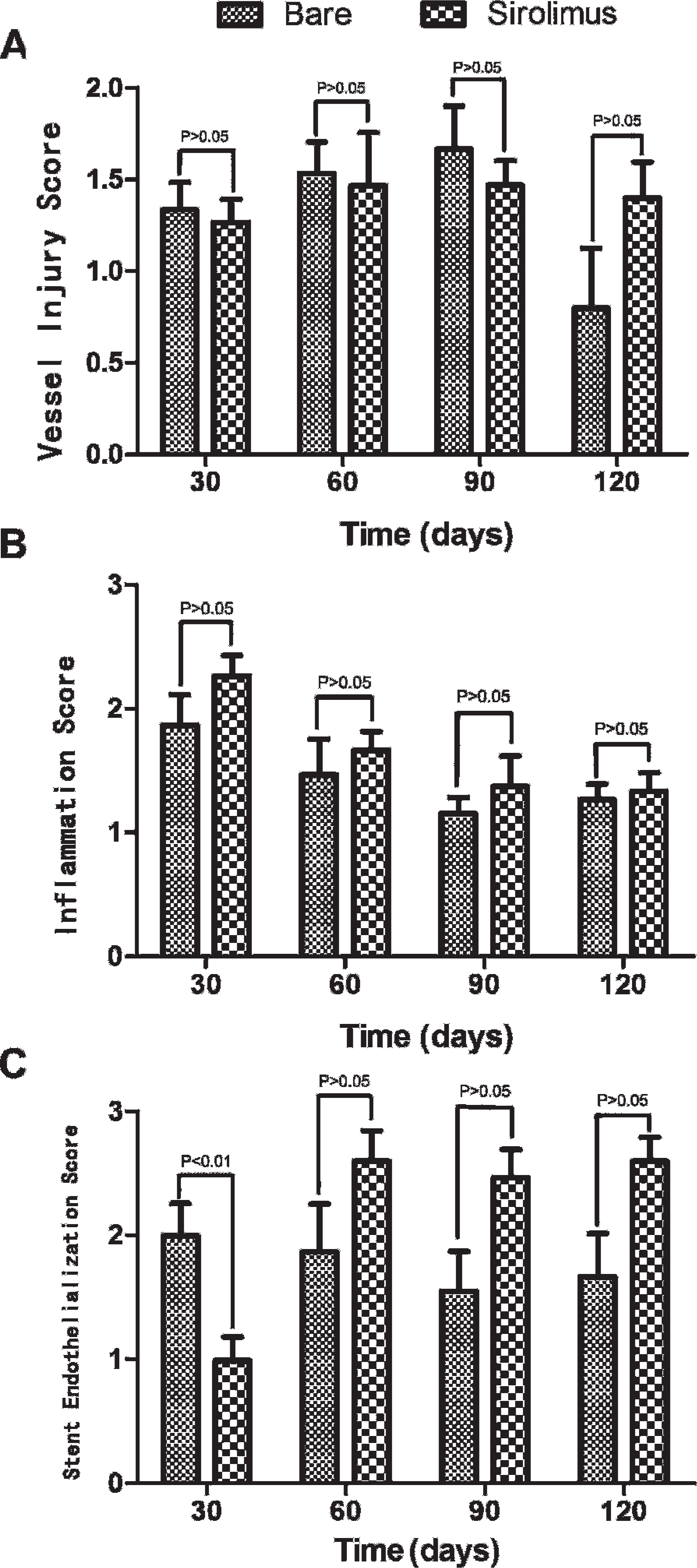
Vessel injury (
There was a linear correlation between the time after implantation and degradation of the bioabsorbable magnesium alloy stent (r=−0.98, slope −0.002). According to this slope, the estimated time for complete degradation of bioabsorbable magnesium stents was ∼105 days.
DISCUSSION
Degradable implants offer several advantages over permanent metallic implants,6,8,9 but negative remodeling due to the loss of mechanical strength and scaffolding ability after degradation of the stent has raised concerns. 13 In this study, the corrosion period of phosphorized AZ31B magnesium alloy stents coated with sirolimus-impregnated P(LA-TMC) was prolonged to ∼100 days, which may help avoid late recoil and remodeling. It was not surprising that there was no significant difference in the injury scores between the bare and drug-eluting groups because the devices had the same composition, shape, deployment pressure, and vessel-to-stent diameter ratio.
As we know, inflammation and neointima formation after stent implantation are related to regional vessel injury. However, sirolimus-eluting stents have shown little evidence of inflammation when compared with bare 14 or polymer-coated 15 stents. According to previous reports, many biodegradable coating materials, such as PLGA 16 and gelatin,17,18 will act as a matrix for inflammatory cell infiltration and angiogenesis. In our study, however, no severe inflammation was revealed, so we assumed that the lower inflammation response was due to sirolimus elution and not the polymer.
The advantage of sirolimus-coated stents may be due to its immunosuppressive properties. In our group, vessel injury scores and inflammation scores were similar between the 2 groups, indicating that the P(LA-TMC) coating and sirolimus elution were safe. On the other hand, the neointimal area was much smaller in the SEBMAS group in comparison to the uncoated BMAS group, confirming that sirolimus-coated stents can reduce neointima formation and enlarge the lumen area by impeding smooth muscle cell proliferation and migration, properties that have been well documented.1–3,19–21
The disadvantages of sirolimus-eluting stents are delayed healing and endothelialization, as well as late stent thrombosis. 22 Delayed healing and endothelialization were also found at 30 days after SEBMAS implantation in our study. However, no thrombus was found in any stented vessel, so late stent thrombosis was prevented by the prolonged antiplatelet therapy used in this experiment. At no time was there a significant difference in endothelialization between the groups, indicating that after the drug elution was complete, delayed healing and endothelialization were reversible.
Limitations
First, this assessment of SEBMAS was performed in a small animal model with normal (non-atherosclerotic) arteries, which might not accurately represent the responses in humans. Furthermore, humans have a longer endothelialization process compared to rabbits. In future studies, an atherosclerotic rabbit model should be used. Second, further research on the mechanisms of late recoil and remodeling are warranted using muscular arteries of a larger animal model so that intravascular ultrasound can be used to evaluate negative remodeling.
Conclusion
Bioabsorbable phosphorized AZ31B magnesium alloy stents coated with P(LA-TMC) are suitable for carrying sirolimus and can be safely implanted in the rabbit aorta. SEBMAS can improve the lumen area by reducing neointimal hyperplasia compared with uncoated magnesium alloy stents. However, SEBMAS leads to delayed healing and endothelialization that can result in thrombus formation during the early stage after stent implantation.