
Abstract
Purpose
To review all available literature on catheter-directed ultrasound-accelerated thrombolysis for peripheral artery occlusions, stroke, deep venous thrombosis, and pulmonary embolism.
Methods
A systematic literature search was performed, using MEDLINE, EMBASE and Cochrane databases. A total of 77 reports focusing on catheter-delivered ultrasound-accelerated thrombolysis were identified.
Results
Experimental studies show that high intensity ultrasound may induce thrombolysis, with and without the addition of plasminogen activators, mainly by acoustic cavitation and mechanical disruption, while low intensity, high frequency ultrasound waves may actually enhance plasmin-mediated thrombolysis. In a total of 340 clinical cases of various thromboembolic conditions, catheter-directed ultrasound-accelerated thrombolysis was related to rapid revascularization and a reduction in treatment time, drug dosage, hospitalization time, and possibly major bleeding complications compared to standard thrombolysis. Reported complication rates, including bleeding and embolization, were low.
Conclusion
Ultrasound enhanced thrombolysis seems to be a promising concept in the treatment of various thromboembolic conditions. The technique has shown to be safe and efficacious in vitro, in vivo, and in clinical studies. Randomized controlled trials are warranted and should be awaited before considering catheter-directed ultrasound-accelerated thrombolysis as a new standard treatment.
Keywords
In recent years, pharmacological catheter-directed thrombolysis (CDT) has become an accepted treatment modality for a variety of thromboembolic conditions, including infrainguinal artery thromboemboli, stroke, and deep venous thrombosis (DVT). Acute infrainguinal artery thrombosis is related to significant morbidity and mortality. Traditional therapy consists of surgical thrombectomy, which is associated with incomplete thrombus removal, a high rate of rethrombosis, perforation, pseudoaneurysm formation, and intimal hyperplasia.1–3 Advantages of CDT are its minimally invasive character, gentler clot removal, and the opportunity to immediately treat an underlying cause endovascularly. Potential drawbacks of this technique include high costs, an extended time needed for revascularization, hemorrhagic complications, and renal dysfunction related to repeated angiography.4–7
Stroke and stroke-related death are an increasing cause of concern in the Western world, where stroke is the third most common cause of death.8,9 In 2008, the American College of Chest Physicians (ACCP) stated that the preferred treatment of acute ischemic stroke is the intravenous administration of recombinant tissue plasminogen activator (rtPA), provided that treatment is initiated within 3 hours of clearly defined symptom onset. Additionally, the use of catheter-delivered thrombolytic therapy may be indicated in selected patients with acute middle cerebral artery or acute basilar artery thrombosis in specialized centers, although this indication is still a matter of dispute. Limitations of the technique (e.g., contraindications to thrombolytic drugs and side effects such as intracranial hemorrhage) emphasize the need to develop adjunctive therapies that increase efficacy and minimize the administered dose of thrombolytic drugs. 3
The two major manifestations of venous thromboembolic events are DVT and pulmonary embolism (PE). Over 90% of acute PEs are caused by emboli originating from proximal veins of the extremities; it is the most significant complication of DVT, with a mortality rate of 12%. 10 The vast majority of patients with DVT are treated with low-molecular-weight heparin and warfarin derivatives. Before the introduction of these agents, 80% of patients with DVT developed a severe form of post-thrombotic syndrome (PTS), 11 which is associated with a reduced quality of life 12 and chronic venous ulceration. 13 The use of heparin and warfarin derivatives has reduced the incidence of PTS to 20% to 50% within 1 to 2 years after the symptomatic episode of DVT. 14 However, anticoagulation therapy only prevents propagation of thrombus; it does not resolve existing thrombus. 3 Catheter-delivered thrombolysis may offer a valid alternative in patients with extensive acute DVT as it might shorten treatment time, reduce acute symptoms, and, most importantly, reduce the incidence of PTS.15,16 Interventional catheterization techniques of PE may also be indicated in compromised patients who are unsuitable to receive prolonged systemic thrombolytic therapy due to bleeding risk. 3
Numerous in vitro studies have suggested a role for ultrasound in accelerating thrombolysis.17–57 In addition, in vivo studies have shown that transcutaneously applied ultrasound waves, either alone or in combination with thrombolytic agents, are capable of enhancing thrombolysis in peripheral artery occlusions (PAO), DVT,27,45,58–68 stroke, 69 and myocardial infarction.63,70–72 However, adverse effects of transcutaneous ultrasound application, including interstitial edema, internal and external tissue damage,45,65,66,73–75 and the disruption of the blood-brain barrier, causing brain edema and infarction,76,77 have limited its applicability in common clinical practice.
Recently, catheter-directed thrombolysis has been combined with catheter-delivered high frequency, low intensity ultrasound in order to accelerate clot dissolution, thereby reducing treatment time and the incidence of thrombolysis-related complications. Ultrasound waves may increase clot permeability by affecting the fibrin strands, thereby facilitating the delivery of therapeutic agents into the clot.78–83 A rapid restoration of complete blood flow is likely to reduce the risks of treatment and costs.84,85 The aim of the present study was to summarize all available evidence on catheter-delivered ultrasound-accelerated thrombolysis.
METHODS
A systematic literature search was conducted to identify reports on the application of catheter-delivered ultrasound-accelerated thrombolysis published up to September 1, 2010, using the MEDLINE, EMBASE, and Cochrane databases. The following MeSH search terms were used: ultrasonography, ultrasonic therapy, thrombolytic therapy, stroke, pulmonary embolism, venous thrombosis, and arterial occlusive diseases. Other non-MeSH terms, such as catheter-delivered ultrasound, peripheral artery occlusions, thrombolysis, and ultrasound enhanced/accelerated thrombolysis, were also used. These terms were applied in various combinations in addition to the use of the “related articles” and “citing articles” function. Fulltext articles were studied without language restriction, and manual cross-referencing was performed. Reports were classified as in vitro studies, in vivo studies, and clinical trials. Experimental studies focusing on transcutaneously applied ultrasound were excluded.
A total of 77 reports on catheter-delivered ultrasound-accelerated thrombolysis were identified; 51 reports presented data from in-vitro studies, 11 reports described results from in vivo studies and 15 reports described clinical results of catheter-delivered ultrasound-accelerated thrombolysis in case series. To date, no randomized controlled trials have been published in this area.
RESULTS
In Vitro Studies
In 1976, Truebestein et al. 17 were the first to demonstrate that ultrasound waves could disrupt clots. Additional animal studies suggested that this approach had the potential for peripheral artery clot dissolution. Since then, two fundamentally different approaches have evolved in the use of ultrasound for thrombolysis. In the first concept, high-intensity ultrasound is applied to mechanically disrupt the clot, while in the second concept a lower intensity ultrasound is used to augment enzymatic fibrinolysis by breaking linkage of fibrin strands. 86
High-intensity ultrasound. In the early studies of Truebestein et al.,17,18 high-intensity ultrasound was used to disrupt clots. Later studies showed that a simultaneous application of thrombolytic drugs, such as urokinase and tPA, had a synergistic effect on clot resolution. 28 Several other studies have confirmed the observation that catheter-delivered ultrasound at different intensities (10–150 W, 20 kHz) could mechanically disrupt clots with87–89 or without19–24 the administration of plasminogen activators.
Siegel et al. 22 were the first to demonstrate the effectiveness of catheter-delivered ultrasound in atherosclerotic clot ablation. Treatment, however, was limited by vessel perforation, thermal heating, and the generation of microscopic debris. These adverse effects were considered to be related to the thermal heating, the use of continuous wave energy at an intensity >20 W, the application of the probe perpendicular to longitudinally opened segments, and the use of ultrasound for at least 30 seconds. In addition, other researchers observed that the effects of ultrasound on dissolution rates were inversely related to its intensity.20,23 Hong et al. 19 observed that ultrasound waves could disrupt human blood clots by both mechanical and cavitational mechanisms, rather than by fibrinolysis. In contrast, Rosenschein et al. 21 have shown that high-intensity, focused ultrasound provided a safe and effective means to induce thrombolysis.
Low-intensity ultrasound. Various experimental studies have shown that low-intensity, high-frequency ultrasound waves may actually enhance plasminogen activator mediated thrombolysis.25–38 According to Blinc et al., 25 the degree of thrombolysis depends on the plasminogen activator concentration, the intensity of ultrasound waves, the duty cycles, and the frequency. A successful thrombolytic effect has been reported for urokinase,25,26,28 rtPA,25,48 tPA, 27 reteplase, 35 and streptokinase25,28,34,36 at intensities ranging from 0.125 to 4 W/cm2. The lytic effect of streptokinase and reteplase, however, disappeared at intensity levels of ≥4 W/cm2, indicating that the balance between ultrasound waves and pharmacological treatment is crucial.34–36 In addition, Soltani et al. 90 demonstrated that ultrasound with a frequency of 1 MHz and intensities of 2.5 to 3.1 W/cm2 had no statistically significant effect on the enzymatic activity of the plasminogen activators urokinase, reteplase, alteplase, and streptokinase. Nevertheless, only limited data is available on the ideal concentrations of plasminogen activators necessary for optimal ultrasound-enhanced thrombolysis. The highest lytic rates of rtPA have been reported using a dose of 1 to 3 μg/mL. 47
Importantly, a variation in the ultrasound waves may affect its thrombolytic efficacy. The use of low-frequency ultrasound has repeatedly been shown to accelerate fibrinolysis, reducing side effects caused by thermal heating.39–41,43–47,49 The use of a pulsed mode ultrasound29,33 significantly enhanced thrombolysis when compared to continuous waves; a rise in duty cycles resulted in increased clot lysis. 48 Moreover, traveling waves significantly 38 accelerated thrombolysis, either in a pulsed 37 or continuous wave mode, when compared to standing waves. 38
An addition of microbubbles to ultrasound therapy may further increase the thrombolytic effect of ultrasound-accelerated thrombolysis.55,91–100 Several in vitro studies have been focusing on the use of catheter-delivered ultrasound in the endovascular area. According to Tachibana et al.,26,53 the use of catheter-delivered ultrasound at 225 kHz and 1.3 MHz, combined with urokinase, accelerated thrombolysis. Similar results were described by the group of Shlansky-Goldberg 54 using a 640-kHz catheter-mounted transducer with urokinase. In addition, the use of albumin microbubbles in combination with urokinase and pulse-waved ultrasound catheter (170 kHz, 0.5 W/cm2, 60 seconds) significantly enhanced the fibrinolytic effect. 55
Hartnell et al. 56 evaluated an ultrasonic thrombolysis device for intracoronary use and reported rapid clot lysis, less local heating, and little debris release during clot ablation. These results were confirmed by the studies of Muller-Leisse et al. 57 In addition, Fischell et al. 42 showed a dose-dependent, reversible vasorelaxant effect of catheter-delivered ultrasound at moderate power outputs effective for clot ablation in rabbit thoracic aortas; the effect was not related to thermal heating or irreversible smooth muscle cell injury. They suggested that this vasorelaxation effect could further enhance the safety and efficacy of catheter-directed ultrasound thrombolysis.
In Vivo Studies
Animal studies using a catheter-delivered external ultrasound transducer for clot dissolution are relatively rare. Rosenschein et al. 21 found that a pulsed mode ultrasound (20 kHz) significantly reduced obstruction in canine femoral arteries. Histological examination showed no damage to the media or adventitia. Applying the same pulse mode ultrasound, a rapid disruption of occluded arteries, without thermal or cavitation injury, embolization, or perforation, was found in canine femoral artery models20,101 and in xenografts. 101 In addition, an arterial relaxation effect of catheter-delivered external ultrasound was found ex vivo and in vivo in occluded canine femoral arteries. Histological examination revealed no evidence of perforation, thermal damage, blast injury, rethrombosis, or vessel damage. 42 In a case controlled study, Steffen et al. 87 showed that an activated ultrasound probe was able to completely disrupt a coronary thrombus in 13 of 15 dogs and partially in 2 of 15 dogs, while there was no clot lysis in the control group without ultrasound. Again, there was no histological evidence of ultrasound-mediated vessel damage or residual thrombus.
A relatively new concept is the catheter-delivered transducer-tipped ultrasound. Experiments in rabbit aortas using a continuous ultrasound exposure of 10 minutes demonstrated no endothelial damage due to thermal or mechanical factors. 102 Atar et al.103–105 tested a prototype of a transducer-tipped ultrasound catheter with a local drug delivery capability in 16 bilateral occluded superficial femoral arteries in dogs. Significantly more partial or complete reperfusion (p=0.0007), widely patent artery segments (p=0.0002), and lower distal embolization rates (p=0.05) were found in the ultrasound (1.1 MHz, 0.6 W/cm2) plus low-dose urokinase group compared to urokinase treatment alone. In a similarly designed study, Atar et al. 106 and Mitchell et al. 107 confirmed these results using the same catheter. These first comparative studies showed significantly more complete perfusion in the combined ultrasound and urokinase-treated arteries when compared to controls.103–107
Clinical Data
Peripheral artery occlusions. The first clinical results using ultrasound-accelerated thrombolysis with the EKOS Ultrasound Infusion System (EKOS Corporation, Bothell, WA, USA) were published by Greenberg et al. 108 in 1999 (Table). In a small series of 9 patients with acute lower extremity ischemia, the authors described technical difficulties in 3 patients in which the procedure had to be discontinued. The technical success rate of the 6 remaining cases was 100% after changing the study design. Revascularization was seen in 5 of the 6 cases. In addition, Link et al. 109 reported a technical success rate of 80% using the same system in 5 patients with acute leg ischemia over a mean treatment time of 5.75 hours with 8.5 mg rtPA. Complete lysis was achieved in 3 patients.
Clinical Data on Catheter-Directed Ultrasound-Enhanced Thrombolysis in Arterial and Venous Occlusions of the Extremities
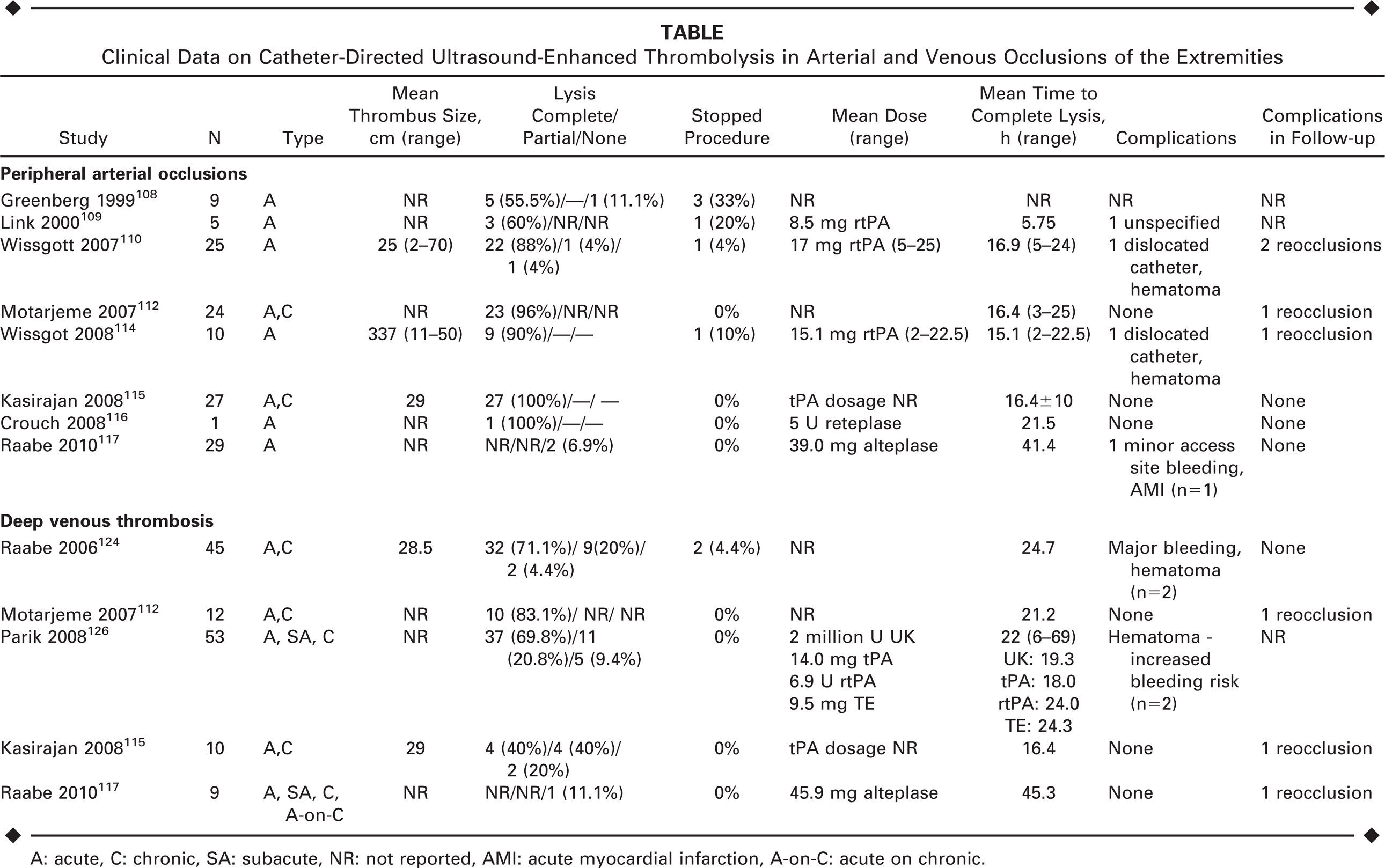
A: acute, C: chronic, SA: subacute, NR: not reported, AMI: acute myocardial infarction, A-on-C: acute on chronic.
In 2007, Wissgot et al. 110 published a retrospective nonrandomized trial designed to evaluate the efficacy and safety of the EKOS Peripheral Infusion System (Fig. 1) in 25 patients with acute thrombotic occlusions of the lower limb. The inclusion and exclusion criteria were matched to the TOPAS protocol to allow comparison to a control group. 111 Early recanalization (>50% thrombus resolving after 6 hours of treatment) occurred in 23 (92%) patients, with complete lysis achieved in 8 (32%). Complete lysis, defined angiographically as >95% clot removal and <30% residual stenosis, was achieved in 22 (88%) patients after 16 hours of treatment. Partial lysis had been realized in 1 patient and no lysis in another. In 1 case, treatment had to be stopped due to a dislocation of the introducer sheath. Additional treatment, such as percutaneous transluminal angioplasty, stent placement, thrombectomy, and vascular repair, was performed in 12 (48%) patients. The technical success rate, defined as placement of the tip of the catheter distal to the thrombus and simultaneous delivery of ultrasound with lytic infusion, was 100%; no adverse events were attributable to the EKOS Peripheral Infusion System. The mean time to discharge was 4 days (range 1–6). During 1-month follow-up, 2 reocclusions occurred. No amputations or deaths were reported. The authors concluded that the use of ultrasound-accelerated thrombolysis is a safe, effective, and time-saving treatment, achieving rapid recanalization and higher rates of complete lysis.
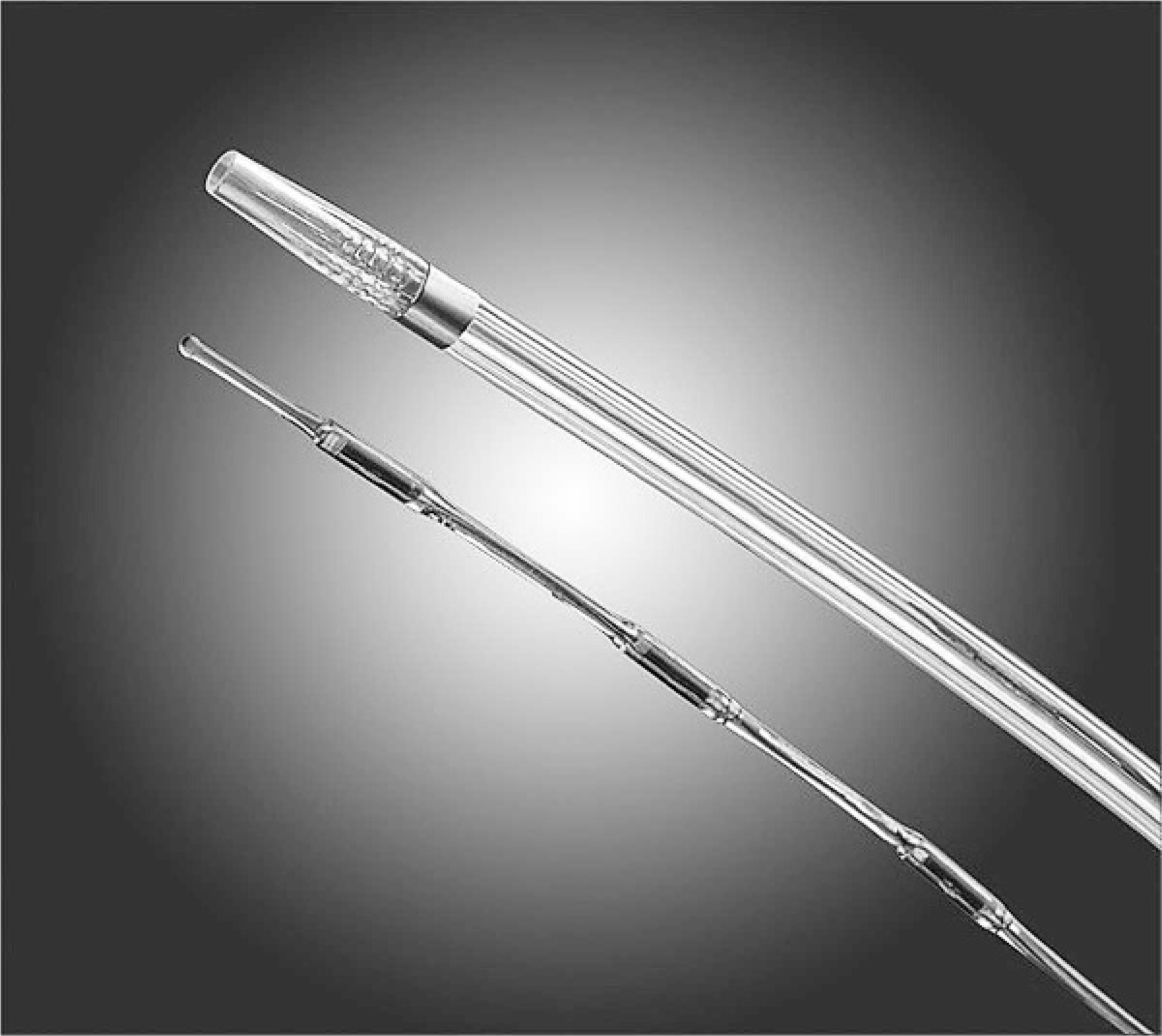
The transducer tipped ultrasound probe of the EKOS EndoWave Endovascular Device. (Kindly provided by EKOS Corporation, Bothell, WA, USA).
Similar results were obtained by Motarjeme, 112 who reported a complete lysis rate of 96% with a mean treatment time of 16.4 hours in a group of 24 patients with an occlusion in the iliac, femoral, or popliteal artery. They reported a shorter infusion time and higher rate of complete lysis using the Lysis Infusion System (EKOS Corporation) compared to the TOPAS 111 and RELAX 113 trials. There were no procedure-related complications, and during a 12-month follow-up, reocclusion occurred in only 1 patient.
In a prospective trial, Wissgott et al. 114 compared the EKOS Lysis Peripheral Catheter System with a rotational mechanical thrombectomy device (Rotarex; Straub Medical, Wangs, Switzerland) in 20 patients with an acute occlusion of a femoropopliteal bypass graft. The mean time to achieve complete lysis was significantly lower (p<0.05) in the mechanical thrombectomy group, i.e., 1 hour compared to 15 hours in the lysis group. The technical success rate was 100% in the thrombectomy group and 90% in the ultrasound-accelerated thrombolysis group, due to a dislocation of the introducer sheath, which was successfully treated by open surgery. Additional treatment was performed in both groups (60% in the thrombectomy group compared to 70% in the lysis group). No major complications were reported. The mean hospitalization time was 2.3 days in the mechanical thrombectomy group and 8.5 days in the lysis group. During follow-up, reintervention was necessary in 1 patient in the lysis group because of a reocclusion. The authors concluded that both techniques were very safe and effective in the treatment of acute arterial occlusions.
In 2008, Kasirajan 115 presented data from 37 patients with arterial and venous occlusions treated with the EKOS EndoWave Endovascular System. Complete lysis was achieved in all arterial patients without any complication related to the EKOS device. In addition, Crouch et al. 116 used the EKOS EndoWave Endovascular System in a 66-year-old woman with a right femoral-tibial peroneal bypass graft occlusion. After 1 hour of treatment, pulses in the dorsalis pedis returned, and a patent bypass with minimal residual thrombus had been achieved in 21.5 hours of infusion with in total 5 U reteplase. Angioplasty was performed to treat the underlying atherosclerotic irregularity. The patient was discharged the 4th day post treatment without complications.
Very recently, Raabe 117 studied the EKOS EndoWave Endovascular System in combination with alteplase in 29 patients with peripheral artery occlusion. Twenty-seven of 29 patients achieved either complete or partial lysis without an unusual decline in fibrinogen levels. No major complications were reported. These data suggest that shorter infusion times and lower administered drug doses related to the use of ultrasound-accelerated thrombolysis may limit fibrinogenolysis, thereby minimizing fibrinogen depletion and reducing the likelihood of bleeding complications.
Stroke. The first clinical experience with the EKOS MicroLysUS Infusion Catheter for acute embolic stroke was published in 2003 by Mahon et al. 118 They studied 14 patients with an occlusion of the anterior (n=10) or posterior (n=4) cerebral circulation and symptoms of cerebral ischemia. At the end of ultrasound-accelerated thrombolysis using either tPA or reteplase, complete perfusion was achieved in 36% of patients (n=5), partial perfusion in 29% (n=4), and 5 patients died. Three patients died within 24 hours after treatment due to cerebral edema (n=1) and intracranial hemorrhage (n=2). In another patient, the thrombolysis had to be terminated due to bradycardia and hypotension, followed by cerebral edema, which required neurosurgical intervention; the patient died within 4 days because of non-hemorrhagic herniation. A fifth patient died from an intracranial hemorrhage 1 month after treatment. No adverse events attributable to manipulation of the catheter, such as perforation, dissection, vasospasm, or vessel occlusion, were seen. During follow-up, improvement was noted in all major standardized stroke scores. The group with posterior occlusions performed better on average standard stroke score scales than those with anterior occlusions. It was concluded that ultrasound-accelerated thrombolysis is associated with a similar or slightly better rate of recanalization and neurological outcome compared to the historical controls using standard thrombolytic therapy.119–121
The Interventional Management of Stroke II (IMS II) trial 122 was developed to determine if microcatheter technology using the EKOS MicroInfusion System in combination with intravenous (IV) and/or intraarterial (IA) administration of thrombolytic drugs is safe and effective in patients with ischemic stroke. Eighty-one patients were enrolled in the study, of which 26 patients received only IV rtPA. A combined IV/IA therapy was applied in 55 patients; 36 of them had occlusions accessible for the infusion catheter. Any subject with etiology of arterial occlusion that prevented safe passage of a guidewire through the occlusive lesion was not accepted for treatment with the EKOS catheter. Additionally, patients with thrombus identified in the anterior cerebral artery, posterior cerebral artery, superior cerebellar artery, posterior inferior cerebellar artery, and anterior inferior cerebellar artery could not be treated with the EKOS MicroInfusion System. In total, 33 patients were treated with the EKOS MicroInfusion System; 3 subjects received rtPA infusion without ultrasound activation, with a mean drug dose of 56 mg rtPA. A complete or partial perfusion was achieved in 46% of the EKOS-treated patients within the first hour of treatment and in 73% at the end of procedure. Procedure-related complications, such as dissections and vasospasm, were reported in 3 cases, and 2 major bleeding complications required transfusion. The overall mortality rate at 3 months was 16% for the entire IMS II population. Significantly better 3-month outcomes were reported at all endpoints when compared to both the placebo-treated subjects and the rtPA-treated group of the National Institute of Neurological Disorders and Stroke rtPA Stroke Trial. 123 A randomized IMS III trial was started in 2006 and included the EKOS MicroInfusion System as part of the investigation to further elucidate the role of this technique in ischemic stroke.
Deep venous thrombosis. In an open enrollment registry across 7 centers in the US, Raabe et al. 124 studied 40 patients with 45 acute and chronic occlusions of the upper and lower extremity and hepatic veins (Table). Using various thrombolytic agents, including reteplase, alteplase, urokinase, and tenecteplase, in combination with the EKOS LysUs System, they achieved complete lysis in 71% and partial lysis in 20%; no lysis occured in only 9%. The average time to achieve complete clot clearance was 25 hours, and 2 (4.4%) major bleeding complications occurred. The technical success rate, defined as catheter positioning within the clot and simultaneous delivery of ultrasound with lytic infusion, was 100%. It was concluded that the EKOS LysUs System offers a rapid initiation of thrombolytic therapy with lower lytic drug dosage and shorter infusion time compared to traditional catheter-directed thrombolysis as reported in the literature. 125 Similar results were reported by Motarjeme et al., 112 who had 83% complete lysis in a mixed group of patients, including venous thrombosis, with a mean duration for complete lysis of 21 hours, without major complications. Compared to the National Venous Registry, 125 shorter average infusion times and higher rates of complete lysis were seen using the EKOS LysUs Infusion System. During a 12-month follow-up, reocclusion occurred in 1 patient. In a retrospective study, Parikh et al. 126 investigated the success of lysis and clinical outcomes in patients treated for DVT. Forty-seven patients with 53 occlusions in the upper and lower extremity and hepatic veins were treated with the EKOS EndoWave System. In 37 (70%) patients, complete lysis, defined as ≥90%, was achieved. Partial lysis was noted for 11 (21%) patients, and in 5 patients no lysis occurred. Additional treatment, such as angioplasty, stent placement, mechanical thrombectomy, and surgery, was necessary in 40 cases. Two major bleeding complications occurred in patients with relative contraindications to thrombolytic therapy. Both patients successfully completed thrombolysis followed by a surgical evacuation of the hematoma. These results showed better efficacy rates, a 3.4 times lower urokinase drug dosage, and half of the infusion time used in the National Venous Registry. 125 Similar results were found when compared to the study of Grunwald and Hofmann. 127 The authors concluded that ultrasound-accelerated thrombolysis appeared to be safe and effective in the treatment of DVT, and it had the potential benefit of complete thrombus resolving behind valves to prevent PTS.
Additionally, Kasirajan 115 reported 10 cases of venous occlusions treated with the EKOS EndoWave System. In that study, complete lysis occurred in only 40% of the DVT group; partial lysis was noted in 4 (40%) patients, and 2 patients had no changes. Mean duration of tPA infusion was 16 hours. After a 6-month follow-up, 1 patient developed an asymptomatic reocclusion. Recently, Raabe 117 published the results of 9 patients with venous occlusions of the upper and lower extremities who were treated with the EKOS EndoWave System in combination with alteplase. Treatment was successful in 8 of 9 patients; during follow-up, 1 reocclusion occurred 2 months after treatment. Fibrinogen depletion was more pronounced among patients with venous occlusions (26.4% from baseline) than those with arterial occlusions (15.8% from baseline), but no major hemorrhagic complications occurred.
Pulmonary embolism. Publications focusing on ultrasound-accelerated thrombolysis for PE are rare. In 2008, Chamsuddin et al. 128 evaluated the efficacy of thrombolysis in 10 patients with 17 massive PEs. The EKOS EndoWave System was used in combination with urokinase, tPA, or reteplase. Complete lysis, defined as >90% thrombus removal, was achieved in 13 (76%) patients. Near complete thrombolysis, defined as 75% to 90% thrombus clearance, was achieved in 18% (n=3), and partial thrombolysis, defined as 50% to 75% thrombus removal, was achieved in 6% (n=1). The average treatment time was 25 hours. Two minor complications, a small right groin hematoma and nonfatal hemoptysis, were seen. During follow-up over a period of 3 days to 1 year, no reocclusions were seen.
Stambo and Montague 129 used the EKOS EndoWave System in a hemodynamically unstable patient with bilateral massive pulmonary embolism. Bilateral infusion of tPA (0.5 mg/h for 8 hours) resulted in complete lysis of both emboli at control angiography, without any complication. This is a fraction of the total amount of 100 mg IV tPA recommended by the ACCP. 3 The patients' hemodynamic status improved, and the patient was discharged home after 9 days. Further, Lin et al. 130 evaluated the outcome of acute massive PE in patients treated with ultrasound-accelerated thrombolysis using the EKOS EkoSonic Endovascular System (n=15) or CDT (n=18). The EKOS-treated group had a significantly (p<0.02) better outcome in complete thrombus dissolution compared to the CDT group (100% vs. 50%). The time to achieve thrombolysis was significant shorter in the EKOS group (p<0.03), with a mean duration of 17.4±5.2 hours. The mean total dosage of tPA was 17.2±2.4 mg for the EKOS-treated group and 25.4±5.3 mg for the CDT group. Comparative analysis showed a significant reduction in treatment time and drug dosage in the EKOS group compared to CDT (p<0.001). No treatment-related hemorrhagic complications were seen with the EkoSonic Endovascular System compared to 21.4% for CDT (p<0.02). The authors concluded that, compared to CDT, treatment with the EKOS EkoSonic Endovascular System has the same efficacy but provided faster recanalization and less treatment-related complications.
DISCUSSION
In the present review we have shown that ultrasound-accelerated thrombolysis is a promising concept in the treatment of various thromboembolic conditions. This technique has repeatedly been associated with rapid revascularization without increased complication rates (Fig. 2). It must be stressed, however, that all the available clinical data are complicated by reporting bias, which may be one of the reasons for the positive results. Moreover, the EKOS catheter has undergone significant modifications since 1999, which may have affected outcome of different studies. Randomized trials have not been performed to date. Due to the wide variance in study design of publications concerning ultrasound-enhanced thrombolysis, a comparison with results from either the TOPAS or STILE study may not be reliable.131,133 Additionally, since the publication of these trials, treatment protocols have changed, indicating the need for prospective randomized trials.
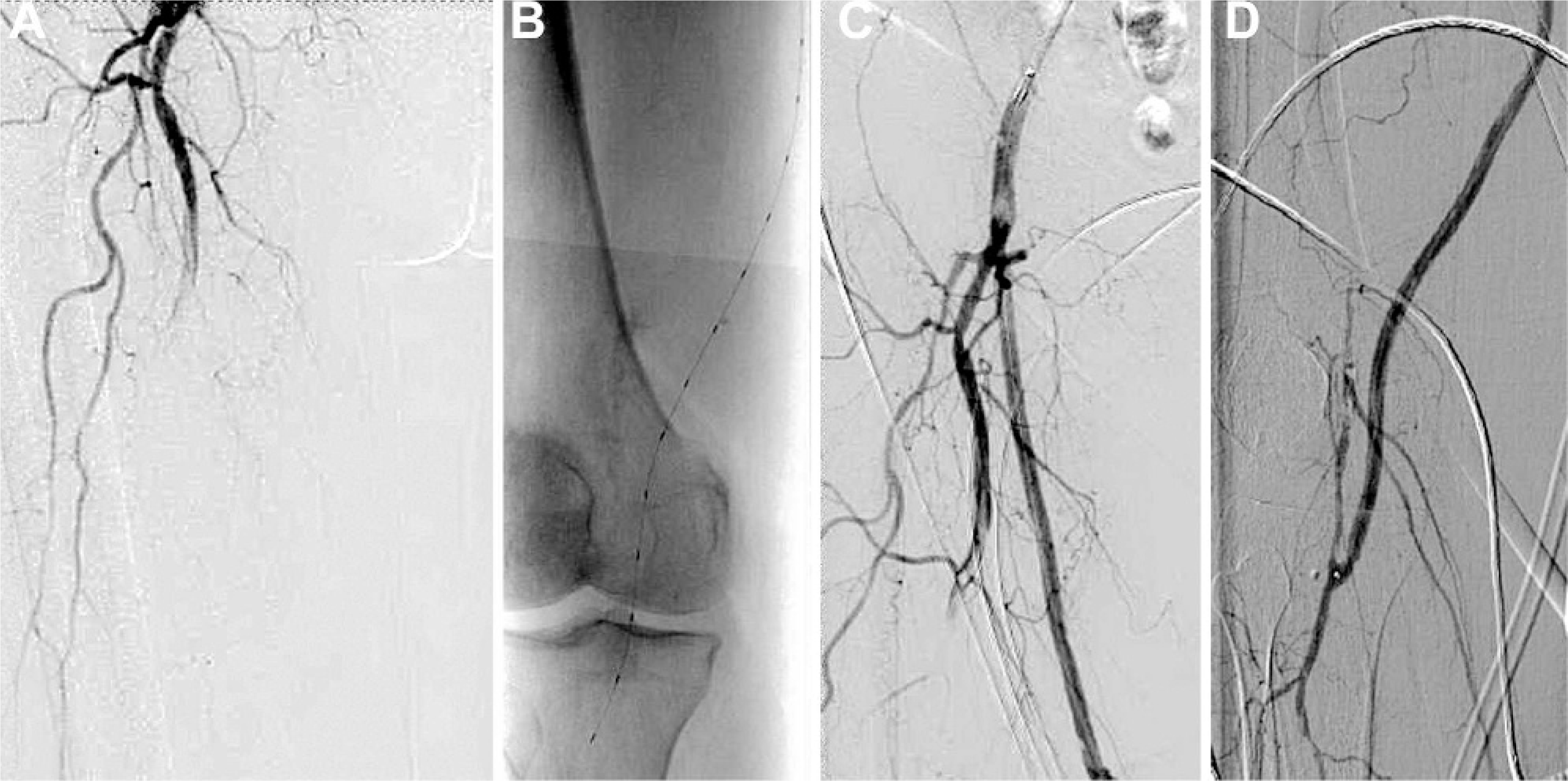
(
Catheter-directed thrombolysis is an accepted therapy in different thromboembolic conditions. When compared to surgical thrombectomy, however, the technique is associated with higher costs, longer time to revascularization, hemorrhagic complications, a small but significant incidence of stroke, and renal dysfunction related to repeated angiography. The incidence of complications appears to be related to the length of treatment, since extended infusion times are associated with increased fibrinogen depletion.131–134 For this reason, a reduction in thrombolytic therapy time would be indispensable. Various reports included in this study note rapid lysis when using ultrasound-accelerated thrombolysis.
In the present review, a total of 340 patients were treated with catheter-delivered transducer-tipped ultrasound-accelerated thrombolysis for various indications. Complete lysis (>90% thrombus removal) or partial lysis (<90% thrombus removal) was achieved in 87.9% compared to no lysis in 8.2%. In 4 cases, it was not clear if there was lysis or not, and 2.6% of the procedures had to be discontinued before thrombolysis was achieved. The time to complete lysis differed among indications, partly caused by differences in definitions of lysis time (e.g., time to complete lysis, median lysis time, and early recanalization).
Moreover, the lysis time may have been influenced by the anatomical substrate of the occlusion (arterial or venous), the time of onset of the occlusion (acute, subacute, or chronic), the length of the occlusion, the use of different plasminogen activators, and the interval of control angiography. The mean drug dosage was lower compared to conventional thrombolytic treatment. The overall complication rates are low (7.1%). Bleeding occurred in 4.1%, and distal embolization was not described. Procedure-related complications, including technical failure, occurred in 1.2% of the cases. In some studies, a shorter hospitalization time was reported. During follow-up, reocclusion occurred in 2.1% of the cases. None of the studies included in this review had a proper control group.
The development of an algorithm for treatment of acute thromboembolic events may be hampered by advances in percutaneous thrombomechanical devices, which are a promising alternative to catheter-delivered pharmacological thrombolytic therapy and surgical thrombectomy. Combinations of these techniques may prove to be useful in the near future. Current limitations of percutaneous mechanical thrombectomy devices, however, are incomplete thrombus removal, high costs, embolization risks, hemolysis, vessel wall and valve injury, design complexity, labor intensiveness, effectiveness in fresh thrombi only, and the lack of prospective data.4–6 Randomized studies focusing on different techniques and indications are indicated to elucidate this subject.
Various authors have reported the efficacy of ultrasound-accelerated thrombolysis in the dissolution of chronic clots. A chronic thrombus is less receptive for lytic drugs 25 because thrombus composition changes over time as a well organized fibrin cap develops around the thrombus. 135 The application of high-frequency ultrasound may facilitate permeation of the lytic drug into the fibrin cap due to ultrasound-mediated changes in fibrin structure. This mechanism may account for the complete lysis seen in patients with chronic arterial and venous occlusions. 112 The possibility to clear thrombus behind venous valves, thereby preserving their function, may lead to better long-term patency rates and a reduced incidence of PTS.124,126 Long-term follow-up of patients, however, has not been published to date.
The reported incidence of complications using ultrasound-accelerated thrombolysis is low. Systemic thrombolysis is associated with a significant increase in major bleeding complications. 85 A reduced lysis time and dose might lower the incidence of bleeding complications. The reported rate of distal embolization is also low. The absence of mechanical fracturing of the thrombus by the EKOS EndoWave Endovascular System may prevent distal embolization during the procedure. 124 Several devices for arterial revascularization have been reported to cause vasoconstriction or spasm,136,137 which could result in turbulent blood flow and high shear rates that promote platelet aggregation and thrombus formation.138,139 In vitro, ex vivo, in vivo, and clinical experiments have shown a dose-dependent, reversible vasorelaxant effect of catheter-delivered ultrasound. This finding may further enhance the safety and efficacy of ultrasound-accelerated thrombolysis, especially when the device is used in the coronary or cerebral circulation.42,140
The mechanism of action of ultrasound-accelerated thrombolysis is not completely clear. The effects of ultrasound on clot dissolution are thought to be based on multiple factors including (1) acoustic cavitation, (2) microstreaming, (3) mechanical effects, (4) intracellular microcurrents, (5) thermal warming, and (6) increased clot permeability. The chemical effect of ultrasound on thrombus dissolution is most likely based on the cavitation phenomenon: the formation, growth, and implosive collapse of cavities in liquids that release large amounts of localized energy.78,141
Acoustic cavitation results in the formation of microscopic bubbles when ultrasound waves pass with an alternating pressure and may be either stable or transient. Both the oscillation of microbubbles and their rapid collapse in the acoustic field result in high local pressure changes, 78 localized thermal heating, acoustic (micro)streaming (liquid micro circulations), and local turbulences.142–145 An intense shear stress may occur in tissues in the immediate vicinity of the collapsing bubble, which could alter the erythrocyte membrane, causing reversible disaggregation of fibrin fibers and affect platelets. Acoustic (micro)streaming and local turbulences may improve transport processes,143,145 leading to better penetration of enzyme into the thrombus78,79 and increasing the total amount and depth of penetration, 80 finally leading to thrombus disruption.78–83
The effect of ultrasound-accelerated thrombolysis may be further increased by the addition of various substances (chemical microbubbles), including perfluorocarbon-filled polymer biospheres, perfluorocarbon-exposed sonicated dextrose albumin, and galactose-based microbubbles.94–96 The addition of a glycoprotein IIb/IIIa receptor antagonist to microbubbles may improve binding of the microbubble at the surface of platelet thrombi.97,146 Recent studies have demonstrated that tPA-incorporated echogenic liposomes may also enhance thrombolysis.98,99 These observations warrant further experimental studies in order to optimize thrombolytic treatment.
CONCLUSION
Catheter-directed ultrasound-accelerated thrombolysis seems to be a promising concept in the treatment of various thromboembolic conditions. However, ultimately, this issue can be resolved only by randomized controlled trials. Comparative studies with conventional thrombolysis and other available techniques are indicated before considering ultrasound-accelerated thrombolysis as the new standard treatment. To this end, the Dutch Ultrasound accElerated Trial (DUET), comparing standard catheter-directed thrombolysis with ultrasound-accelerated catheter-directed thrombolysis in infrainguinal artery occlusion, is designed to provide level 1 evidence.