
Abstract
Purpose
To analyze the immediate and long-term outcomes of endovascular stenting vs. extrathoracic surgical bypass for subclavian steal syndrome.
Methods
From 1989 to 2010, 252 consecutive patients (173 men; mean age 62 years) with vertebrobasilar and upper extremity symptoms of subclavian steal were treated with balloon-expandable stents (n = 148) or extrathoracic surgical bypasses (n = 104: 71 axilloaxillary and 33 carotid-subclavian) using polytetrafluoroethylene grafts.
Results
The technical success rate was 97.3% in the stent group vs. 99.0% for the bypass group (p=0.605). There was no perioperative mortality or any permanent neurological deficit in either group. The overall perioperative complication rate was 6.1% in the stent group vs. 9.6% in the bypass group (p=0.295). The 10-year target vessel revascularization rate was 46.6% for stenting vs. 5.8% for bypass (p<0.001). The cumulative primary patency rates at 1, 3, 5, and 10 years were 91%, 78%, 67%, and 49% for the stent group vs. 99%, 97%, 95%, and 89% for the bypass group (p<0.001). The cumulative secondary patency rates were 95%, 91%, 86%, and 64%, respectively, for the stent group vs. 99%, 99%, 98%, and 94% for the bypass group (p=0.001). No difference was detected in overall survival curves between the groups (p=0.527).
Conclusion
Both endovascular stenting and extrathoracic surgical bypass are safe and effective treatments for subclavian steal syndrome in the short and medium term; however, extrathoracic surgical bypasses are more durable in the long term.
Keywords
The phenomenon of reversed flow in the vertebral artery in the setting of proximal subclavian artery stenosis1,2 is relatively rare and usually asymptomatic 3 due to adequate compensation by the circle of Willis and a rich brachiocephalic collateral circulation. However, symptoms can arise when these pathways are compromised by occlusive disease or anatomical variants,4,5 leading to vertebrobasilar or upper extremity ischemia or even myocardial ischemia from diminished flow through an internal mammary artery bypass graft.4,6,7 In these circumstances, surgical or endovascular intervention is indicated.
Over the past decades, endovascular therapy (angioplasty and stenting) and a variety of extrathoracic surgical approaches [carotid-subclavian bypass (CSB), axilloaxillary bypass (AAB), and subclavian-to-carotid transposition] have been advocated to treat subclavian lesions and avoid transthoracic approaches because of their greater morbidity and mortality. However, the data concerning long-term outcomes of different treatment approaches are limited, and there are only a few studies that have compared the efficacy of endovascular therapy vs. surgical approaches in this setting.8–11 The present study was undertaken to evaluate the immediate and long-term outcomes of endovascular stenting vs. extrathoracic surgical bypasses performed specifically for subclavian steal syndrome.
METHODS
Study Design and Patient Population
Under a clinical protocol approved by the Institutional Review Board of our hospital, a retrospective analysis was conducted of patients undergoing treatment for subclavian steal syndrome between January 1989 and November 2010. A search of hospital records identified 252 consecutive patients (173 men; mean age 62 years) with vertebrobasilar and upper extremity symptoms of subclavian steal who underwent primary stent implantation (n = 148) or primary extrathoracic surgical bypasses (n = 104: 71 AABs and 33 CSBs) at our institution. Data were collected on baseline characteristics, presenting clinical signs and symptoms, the location of the subclavian artery lesions, results of the pretreatment evaluation, procedure details, and the immediate and long-term outcomes. Patients in the stent group who underwent extrathoracic surgical bypasses after failed endovascular reinterventions for in-stent stenosis/occlusion were not included in the bypass group.
Symptoms included vertebrobasilar ischemia (dizziness, vertigo, diplopia, tinnitus, syncope, or ataxia), upper extremity ischemia (claudication, weakness, coldness, paresthesia, cyanosis, or trophic changes), or both. Patients with vertebrobasilar ischemia were also evaluated by a neurologist to rule out other causes of their symptoms. For upper arm complaints, most were claudication or weakness; true ischemic complaints, such as arm ulceration or gangrene, were not found in this cohort.
Preoperative pressure gradients were measured in the upper limbs. All patients had reversed vertebral flow documented with duplex ultrasound and confirmed with aortic arch aortography and extracranial vessel arteriography. The mode of treatment was at the discretion of the operating surgeon. Before September 2007, surgical bypass was preferred for complete subclavian occlusions, while stenting was preferred for stenotic lesions. Since that time, enhancements in endovascular devices and increased experience with endovascular therapy gradually have made it possible to treat more and more complete occlusions with endovascular recanalization. Currently, stenting is the first choice for all subclavian lesions; failures of endovascular therapy are treated with surgical bypass.
Stent and Bypass Procedures
Stent procedures were performed under local anesthetic. Arterial access was obtained via the common femoral and/or axillary arteries. Unfractionated heparin (80–100 U/kg) was given after arterial access to maintain an activated clotting time ≥250 seconds. A 6- or 7-F sheath was used during the procedures. The lesions were crossed using a 0.035-inch hydrophilic wire with a curved catheter providing directional control and support. The reference vessel diameter was determined with quantitative angiography, and the appropriate size of stent and balloon were selected accordingly. Balloon-expandable stents (Palmaz or Genesis; Cordis, a Johnson & Johnson company, Miami Lakes, FL, USA) were used in all patients in this study. Completion angiography was performed after stent deployment; residual stenosis <30% determined technical success.
All extrathoracic surgical bypass procedures were performed with 8-mm-diameter polytetrafluoroethylene grafts under general anesthesia. For AAB, the axillary artery was exposed bilaterally by transverse infraclavicular incisions along the lateral third of the clavicle. The pectoralis major was split along its fibers, and the axillary artery was identified just inferior to the clavicle, posterior to the deep pectoral fascia. A subcutaneous tunnel was created between the arteries, and an end-to-side anastomosis with prosthetic graft was performed bilaterally after systemic heparinization. For CSB, a transverse supraclavicular incision provided exposure for both the carotid and subclavian arteries. The platysma was divided, and the sternocleidomastoid was retracted medially. The jugular vein was dissected free and also retracted medially to expose the common carotid artery, which was encircled and mobilized sufficiently to obtain proximal and distal control. The subclavian artery was exposed by dividing the inferior insertion of the anterior scalene muscle (on the first rib). After systemic heparinization, the distal subclavian anastomosis was first performed in an end-to-side fashion to minimize the amount of time the common carotid artery was clamped. The site for the proximal anastomosis was selected on the common carotid artery so as to minimize the amount of graft material used. The carotid anastomosis was completed in end-to-side fashion. Carotid shunts were not used routinely. Lifelong aspirin (100 mg/d) therapy was prescribed after treatment in both groups.
Follow-up and Surveillance
Follow-up information was obtained from patient examination and noninvasive vascular laboratory data. Graft and stent patency were determined by the presence or absence of peripheral pulses and confirmed by duplex ultrasound performed at 1, 6, 12 months for the first year and annually thereafter. All patients with recurrent symptoms had a duplex ultrasound scan and angiography.
Definitions and Statistical Analysis
Continuous variables are expressed as the mean ± standard deviation and categorical variables are given as the count (percentage). Perioperative complications were any sequela that took place within 30 days following the procedure. Target vessel revascularization (TVR) was defined as repeat intervention (endovascular or surgical) in the target vessel driven by recurrent symptoms with angiographic documentation of >70% stenosis.
The technical success (<30% residual stenosis), perioperative complications, relief of symptoms, TVR, primary patency, secondary patency, and overall survival were compared between the stent and bypass groups. The standardized difference 12 method was used to identify baseline variables having a potential effect on long-term outcomes. Based on the formula 1.96 × √[(n1+n2)/n1(n2)] and the current sample sizes (148 stents and 104 bypasses), a standardized difference >0.251 would indicate a potential confounding effect. The influence of confounding variables was assessed using multivariable regression analysis or a Cox proportional hazards model as appropriate.
A post-hoc power calculation was performed based on a 20% absolute difference in the 10-year TVR rates between groups, assuming a 10% 10-year TVR rate for the bypass group. The current sample sizes provided >95% power.
A t test for independent samples was used to compare means of continuous variables, and a chi-square test was used to compare proportions of categorical variables between groups. The Wilcoxon test was used to compare patency and survival rates. The cumulative patency and survival rates were calculated with the life-table method; the curves were compared using the log-rank test. P<0.05 was considered statistically significant. Statistical analyses were performed using SPSS software (version 16.0; SPSS Inc, Chicago, USA) and Microsoft Office Excel 2007 (Microsoft Corporation, Redmond, WA, USA).
RESULTS
Comparison of Patient Samples
The proportion of men was higher in both groups (Table), and risk factors for atherosclerosis were prevalent. Most of the patients (203, 80.6%) were first seen with at least 2 risk factors for atherosclerosis. The left subclavian artery was more commonly involved than the right in both groups (85.8% in the stent group vs. 82.7% in the bypass group, p=0.5). The proportion of occlusions in the bypass group was higher than in the stenting group (p<0.001). The mean pretreatment arm pressure gradient in the bypass group was higher than that in the stent group (p<0.001). No difference was detected in the other baseline variables and the indications for treatment between the groups.
Baseline Patient Characteristics and Indications
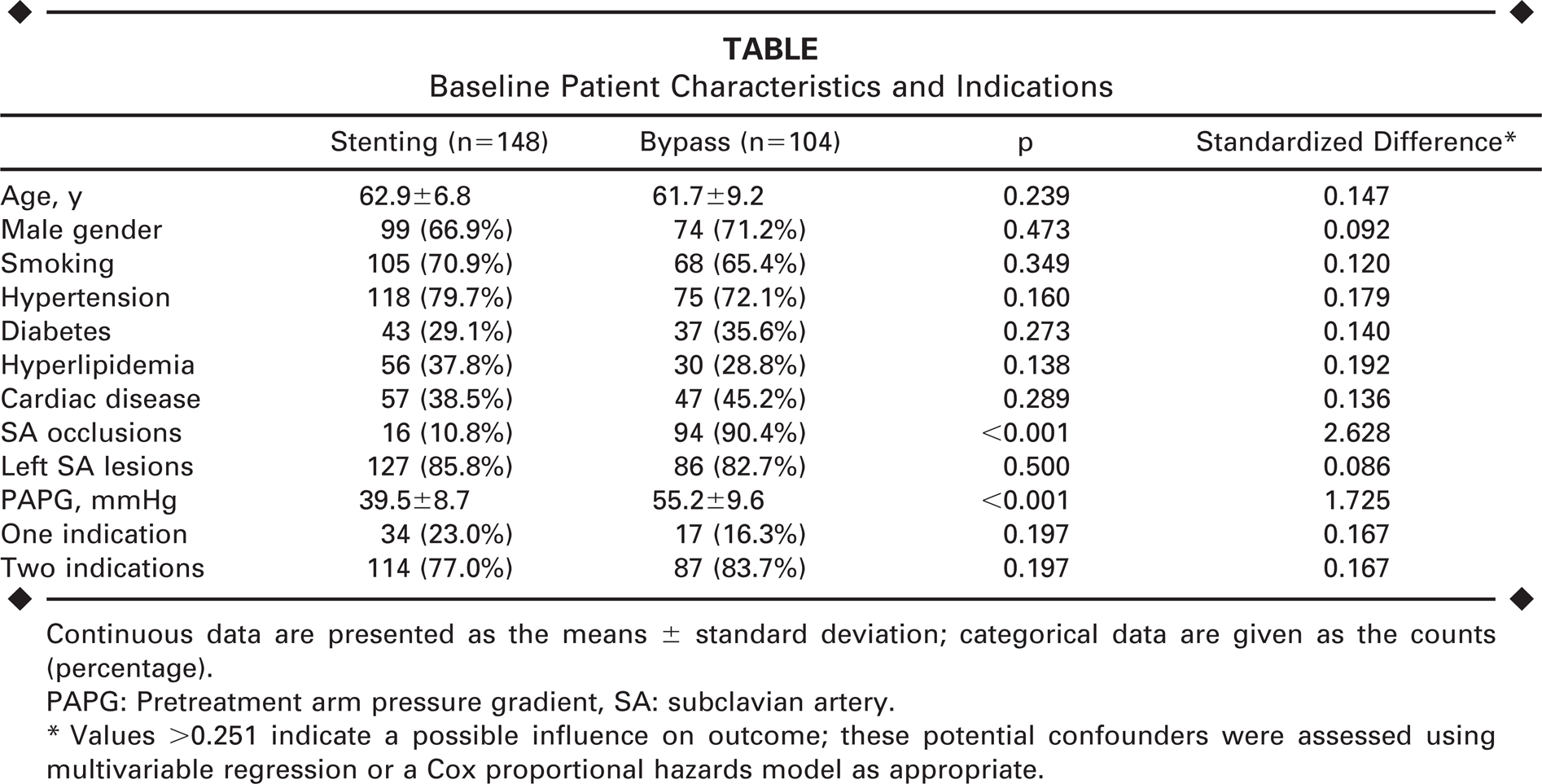
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
PAPG: Pretreatment arm pressure gradient, SA: subclavian artery.
Values >0.251 indicate a possible influence on outcome; these potential confounders were assessed using multivariable regression or a Cox proportional hazards model as appropriate.
Periprocedural Outcomes
At 30 days after treatment, the procedure success rate was 97.3% (144/148) for the stent group vs. 99.0% (103/104) for the bypass group (p=0.605). In the stent group, 3 procedures failed when total occlusions could not be crossed. There was also 1 case of in-stent stenosis at 26 days post procedure. One AAB graft failure occurred at 3 days in a Takayasu arteritis patient. No perioperative mortality or any permanent neurological deficit occurred in either group.
The overall perioperative complication rate was 6.1% in the stent group vs. 9.6% in the bypass group (p=0.295). There were 3 major complications (myocardial infarction, pseudoaneurysm, and contrast-induced nephropathy) in the stent group, and 6 minor complications (4 femoral hematomas and 2 access site infections). In the bypass group, there were 5 mild brachial plexus injuries (3 AAB and 2 CSB), 3 minor wound complications (all AAB), 1 temporary recurrent laryngeal nerve dysfunction (CSB), and 1 case of transient hemispheric symptoms (AAB). Among the brachial plexus injuries, 3 patients presented with mild numbness in 1 finger; they recovered at 2, 2, and 5 months, respectively. The other 2 patients recovered from mild numbness in 2 fingers at 3 and 11 months, respectively. Among the minor wound complications, 2 patients with seroma recovered at 5 and 8 days, respectively; the other patient developed a superficial wound infection (swelling and pain around the wound) and recovered at 10 days. The patient with recurrent laryngeal nerve dysfunction was recovered at 36 days.
Relief of vertebrobasilar ischemic complaints was achieved in 97.2% (139/143) in the stent group vs. 99.0% (102/103) in the bypass group (p=0.587). Relief of upper extremity ischemic complaints was achieved in 96.6% (113/117) in the stent group vs. 98.9% (87/88) in the bypass group (p=0.554). Reversed flow in the vertebral artery was corrected in 97.3% (144/148) in the stent group vs. 99.0% (103/104) in the bypass group (p=0.605). The arm pressure gradients decreased markedly after treatment in both groups, and no difference was detected in the post-treatment pressure gradient means (p=0.281). For the stent group, the mean pretreatment gradient of 39.5 mmHg fell to 5.8 mmHg; for the bypass group, the 55.2 mmHg pretreatment gradient declined to 6.4 mmHg.
Mid- and Long-term Outcomes
The median follow-up for the stent group was 67 months (range 2–178) vs. 101 months (range 4–202) for the bypass group. During follow-up, 4 stent patients were lost to follow-up at 29, 81, 97, and 118 months vs. only 2 AAB patients in the bypass group at 47 and 134 months. In the stent group, there were 47 in-stent occlusions and 29 in-stent stenoses during follow-up. Eighty-four revascularization procedures (16 AABs, 9 carotid-subclavian/ axillary bypasses, and 59 balloon angioplasties) were performed to relieve the recurrent symptoms.
A subanalysis was done of the 25 patients (18 men; mean age 66 years, range 57–81) with in-stent occlusion who underwent surgical intervention after unsuccessful endovascular recanalization attempts. The bypass technical success rate was 100%; 1 (4%) perioperative complication occurred. A 65-year-old man developed minor stroke due to ipsilateral carotid artery stenosis at 18 days after AAB and underwent carotid artery stenting. No vertebrobasilar ischemia, transient ischemic attack, or stroke occurred in these patients during follow-up. Over a median 53-month follow-up (range 6–126), the only graft failure was in a 74-year-old man who developed graft thrombosis and recurrent symptoms 87 months after AAB. He underwent successful thrombectomy and maintained functional graft until his last follow-up. A 79-year-old woman with a patent CSB graft died of colon cancer at 33 months after CSB. All the other patients remained asymptomatic during follow-up.
In the bypass group, 6 (8.5%) AAB patients had graft thromboses at 3 days, 47, 62, 79, 125, and 166 months, respectively; 2 (6.1%) CSB patients had graft thromboses at 39 and 92 months, respectively. One of the AAB patients with an occluded graft remained asymptomatic. For the 5 AAB patients with recurrent symptoms, revascularization procedures included graft thrombectomy in 2 and carotid-axillary bypass in 3. Two AAB patients with patent grafts had recurrent symptoms because of ipsilateral vertebral artery ostial lesions. The symptoms disappeared after stenting of the vertebral artery via a brachial artery access. For the 2 CSB patients with recurrent symptoms, revascularization procedures included graft thrombectomy and AAB, respectively.
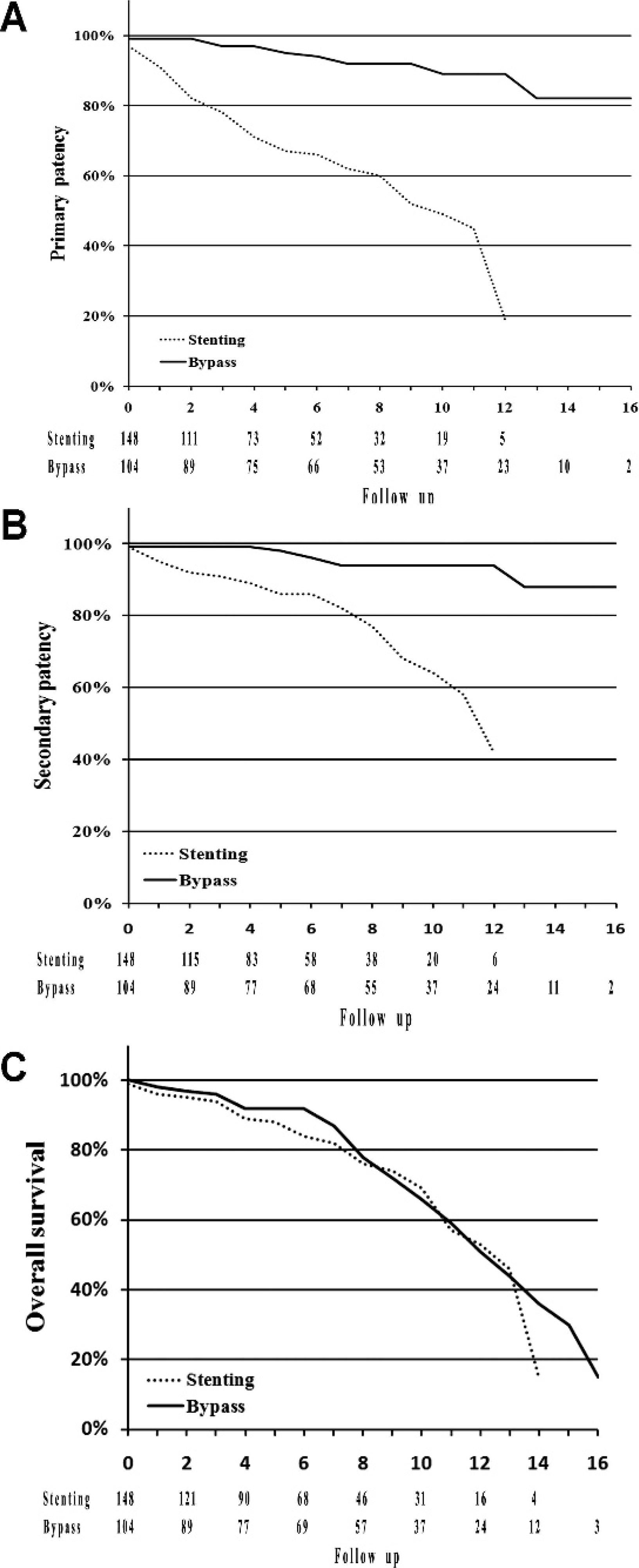
The 5-year TVR rate was 34.5% (51/148) for the stent group vs. 3.8% (4/104) for the bypass group (p<0.001); the 10-year TVR rate was 46.6% (69/148) for the stent group vs. 5.8% (6/104) for the bypass group (p<0.001). Multivariable regression analysis showed that the variables identified by the significant differences test did not exert any specific influence on TVR. Likewise, the Cox proportional hazards regression model did not show any influence on long-term patency and survival. The cumulative primary patency rates (Figure, A) at 1, 3, 5, and 10 years were 91%, 78%, 67%, and 49% for the stent group vs. 99%, 97%, 95%, and 89% for the bypass group (p<0.001). The cumulative secondary patency rates (Figure, B) at the same intervals were 95%, 91%, 86%, and 64% for the stent group vs. 99%, 99%, 98%, and 94% for the bypass group (p=0.001). The cumulative overall survival rates (Figure, C) were 96%, 94%, 88%, and 69% for the stent group vs. 98%, 96%, 92%, and 66% for the bypass group (p=0.527).
DISCUSSION
Patients with subclavian steal are relatively rare and usually asymptomatic 3 because of the rich collateral compensation.13,14 Thus, “subclavian steal” is generally a benign hemodynamic phenomenon.4,15–17 However, clinical ischemic symptoms develop when the collateral circulation to the upper extremity is unable to compensate for a decrease in blood supply as a result of anatomical variation or occlusive disease in the carotid, vertebral, or circle of Willis arteries.4,5 In these circumstances, surgical or endovascular treatment of the subclavian artery lesion is indicated.
Carotid-subclavian bypass and axilloaxillary bypass represent two of the extrathoracic surgical techniques used to treat subclavian steal, and both have excellent long-term outcomes.18–21 However, in patients with concomitant carotid lesions, graft failure is more frequent in the CSB group; 5- and 10-year estimated patency rates were 66.0% and 40.8% for the CSB group and 100% for the AAB group (p<0.05). 22 Based on this data, we usually perform CSB in patients without concomitant ipsilateral carotid diseases and AAB in patients with concomitant carotid artery diseases, especially ipsilateral.
In our study, only 5 failed AAB grafts and 2 failed CSB grafts were found after 3 years, and 1 patient with an occluded AAB graft remained asymptomatic. Theoretical concerns about graft infection and skin erosion in AAB have not been encountered in our study. Any coronary artery disease that developed during follow-up in these bypass patients could be treated with balloon angioplasty and stenting or minimally invasive coronary artery bypass graft surgery in patients receiving AAB.
Brachial plexus injuries and minor wound complications were predominant perioperative complications in AAB and CSB patients. Most of the brachial plexus injuries occurred early in our experience. The symptoms were mild numbness in 1 or 2 fingers, and no motor dysfunction occurred. To avoid brachial plexus injuries, the dissection of the axillary artery in AAB should not be carried out too laterally; in CSB, division of the anterior scalene muscle during subclavian artery exposure should be done under direct vision and without cautery as the brachial plexus is immediately adjacent to the lateral aspect of this muscle. Second, the dissection should not be carried too laterally or superiorly. Third, the lower cords of the brachial plexus are found deep to the subclavian artery and should be carefully handled during placement of retractors. Other rare complications (e.g., temporary recurrent laryngeal nerve dysfunction and transient hemispheric symptoms) did not require additional intervention, and all patients recovered without deficit. Previous studies have reported ipsilateral Horner syndrome and thoracic duct fistula in CSB, 23 but those complications did not occur in our CSB patients.
Endovascular treatment, such as angioplasty or stenting, is an alternative to bypass grafting and may have several advantages over surgical approaches, including its minimally invasive nature, avoidance of general anesthesia, greater patient acceptance, shorter length of hospital stay, and lower cost-per-unit treatment. However, angioplasty alone carries a high recurrence rate (20% at 1 to 5 years),24,25 with initial technical success rates ranging from 83% to 100% for stenoses (50% to 87% for occlusions26,27) and a risk (1%) of cerebral embolization. 24
Although primary stenting seems to have improved results over angioplasty alone, these endovascular procedures are not as durable as their surgical alternatives. In a study comparing the results of stenting and CSB for isolated subclavian artery disease, the primary patency rates at 1, 3, and 5 years were 93%, 78%, and 70% for the stent group vs. 100%, 98%, and 96% for the CSB group, respectively (p<0.001). 11 Similarly, in our study, stents were also not as durable as bypass grafts; both the 5- and 10-year TVR rates were significantly lower (p<0.001).
Although surgical bypasses had excellent long-term outcomes, their perioperative complication rate was still relatively high compared to endovascular therapy in our study. In addition, most in-stent stenoses can be treated with endovascular therapy, which suggests that endovascular management of subclavian artery stenosis may be an excellent alternative to surgical bypass with comparable long-term secondary patency if an adequate surveillance program can be established, enabling early detection and treatment of any significant recurrent stenosis. Today, we routinely select subclavian artery stenting first for subclavian steal syndrome. When endovascular therapy is unsuccessful initially or fails due to in-stent stenosis/occlusion during follow-up, surgical revascularization with a CSB or AAB using a PTFE graft can provide an effective and durable treatment option. This “stent first then surgery” algorithm has gained popularity and acceptance among patients and surgeons.
Limitations
First, the influence of potentially confounding variables on immediate outcomes (e.g., perioperative complications) was not assessed in multivariable regression analyses because of limited events. Second, this was a retrospective, nonrandomized study with relatively small sample sizes. Prospective randomized studies are needed to compare the current treatment modalities for subclavian steal syndrome.
Conclusion
Our results showed that both balloon-expandable stent implantation and extrathoracic surgical bypass using PTFE grafts are safe and effective for treating subclavian steal syndrome in the short and medium term; however, extrathoracic surgical bypasses are more durable in the long term. An adequate surveillance program for stent patients is essential because of the high risk of recurrent stenosis in long-term follow-up.
Footnotes
Acknowledgments:
The authors thank Xuefeng Li and Lixing Qi for assistance with manuscript preparation and data collection.