
Abstract
Purpose
To describe our experience with a novel technique to decompress abdominal compartment syndrome after endovascular aneurysm repair (EVAR) of ruptured abdominal aortic aneurysm (rAAA).
Method
From January 2003 to April 2010, 13 patients (12 men; mean age 75 years) treated for rAAA with EVAR underwent tissue plasminogen activator (tPA)–assisted decompression for intra-abdominal hypertension. All of the patients but one had intra-abdominal pressure >20 mmHg, with signs of multiple organ failure or abdominal perfusion pressure <60 mmHg. With computed tomography guidance, a drain was inserted into the retroperitoneal hematoma, and tPA solution was injected to facilitate evacuation of the coagulated hematoma and decrease the abdominal pressure.
Results
In the 13 patients, the mean intra-abdominal pressure decreased from 23.5 mmHg (range 12–35) to 16 mmHg (range 10–28.5). A mean 1520 mL (range 170–2900) of blood was evacuated. Urine production (mean 130 mL/h, range 50–270) increased in 7 patients at 24 hours after tPA-assisted decompression; among the 5 patients in which urine output did not increase, 3 underwent hemodialysis by the 30-day follow-up. One patient did not respond with clinical improvement and required laparotomy. The 30-day, 90-day, and 1-year mortality was 38% (5/13 patients); none of the deaths was related to the decompression technique.
Conclusion
tPA-assisted decompression of abdominal compartment syndrome after EVAR can decrease the intra-abdominal pressure and could be useful in preventing multiple organ failure. It is a minimally invasive technique that can be used in selected cases but does not replace laparotomy or retroperitoneal surgical procedures as the gold standard treatments.
Keywords
Endovascular aneurysm repair was introduced >10 years ago for treatment of ruptured abdominal aortic aneurysms (AAA). Over the last decade, the use of endovascular aneurysm repair (EVAR) has increased, and major centers have reported significant decrease in mortality.1,2 A major cause of morbidity and mortality after EVAR for ruptured AAA is abdominal compartment syndrome (ACS), which is estimated to develop in —20% of the patients. 3 ACS is defined as intra-abdominal pressure (IAP) >20 mmHg in combination with organ dysfunction, though an abdominal pressure >12 mmHg (IAH) is considered abnormal. 4 Early conservative treatment with analgesics, diuretics, colloids, and neuromuscular blockade might be useful in treating ACS,5,6 but oftentimes a laparotomy (or retroperitoneal surgical approach) is needed to clinically inspect the abdominal organs, to evacuate the hematoma and decompress the abdominal compartment, and to relieve the pressure from the swollen intestines.7,8
See commentary page 149
We report our experience of a novel method to decompress abdominal hypertension after EVAR for ruptured AAA assisted by injection of a thrombolytic agent into the retroperitoneal hematoma to augment catheter drainage.
METHODS
A decompression technique was devised in which tissue plasminogen activator (tPA) was delivered to the retroperitoneal hematoma via a catheter inserted into the abdomen under computed tomography (CT) guidance. A naturally occurring fibrinolytic agent, tPA is used widely in vascular, cardiovascular, and neurovascular interventions to facilitate clot dissolution through the conversion of plasminogen to plasmin. 9
All patients with ruptured AAA who were treated by EVAR were monitored in the intensive care unit (ICU) hourly for IAH with a Foley Manometer (Holtech Medical, Charlottenlund, Denmark). When signs of deterioration appeared, which included IAP >20 mmHg and multiple organ failure (MOF) or abdominal perfusion pressure <60 mmHg, a decision was made to perform a laparotomy or lytic-assisted decompression based on the clinical status, as well as vital signs, laboratory parameters, and abdominal CT imaging.
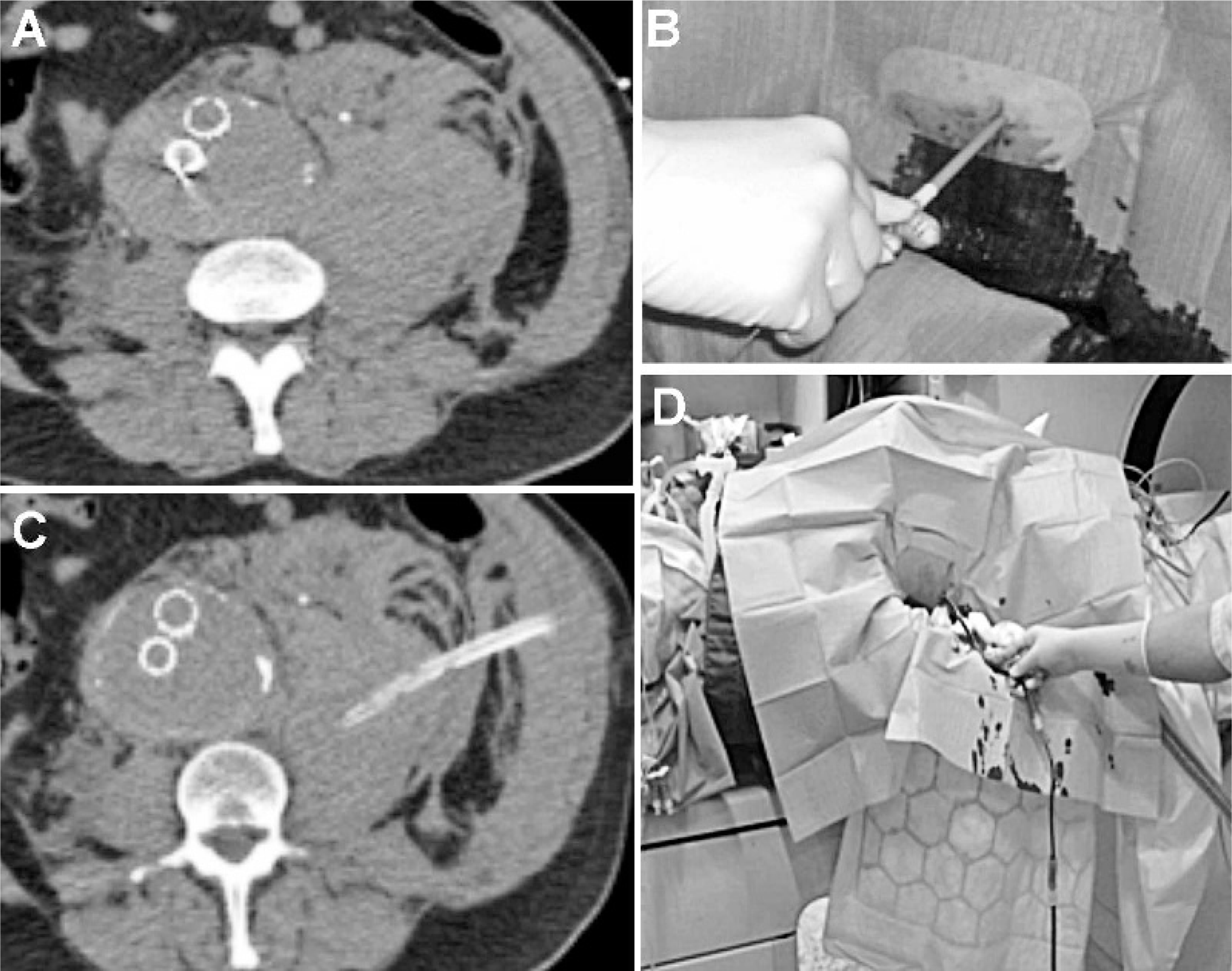
For lytic-assisted decompression, the patient was transferred to the imaging suite, where acute CT was performed to locate the retroperitoneal hematoma (Figure, A). The estimated puncture site was marked on the skin, and the distance to the hematoma from the skin was determined. Local anesthetic was injected if needed, and a small incision was made with a scalpel. Sterile puncture was done using a 14-G needle; a soft guidewire was inserted followed by sequential dilatation to facilitate delivery of a 20-F Thal-Quick catheter (Cook Medical, Bloomington, IN, USA). The catheter was positioned toward the center of the hematoma, fixed to the skin, and connected to a urinary bag to collect spontaneous blood coming through the drainage catheter (Figure, B–D). IAP was not monitored during the procedure. The patient was transferred back to the ICU. When spontaneous blood flow from the drainage catheter ceased, a solution of 20 mg tPA (Alteplase; Boehringer Ingelheim, Germany) dissolved in 200 mL of saline solution was injected into the drainage catheter, which was then clamped for 20 minutes. The evacuated blood was then collected into the bag. The catheter was removed only when blood flow ceased. The patients were followed closely with repeated measurements of abdominal pressure and urine production. If there were no signs of improvement during the following hours, a laparotomy was considered.
Between January 2003 and April 2010, 13 patients (12 men; mean age 75 years) with IAH and suspected ACS were treated with this decompression technique in our department.
RESULTS
Before the procedure, all the patients had urine production <30 mL/h (Table). The mean time to decompression was 9 hours (range 2–17). The mean IAP at the end of EVAR before decompression was 23.5 mmHg (range 12–35). At 1 hour after decompression, the mean IAP was 14 mmHg (range 11–27.5) and at 3 hours 17.7 mmHg (range 12–26). Twenty-four hours after tPA-assisted decompression, the IAP decreased to a mean value of 16 mmHg (range 10–28.5). The mean volume of blood evacuated by the catheter before tPA injection was 370 mL (range 5–1000). A mean 1520 mL (range 170–2900) of blood in total was evacuated using the tPA-assisted decompression procedure. The mean catheter time was 31 hours (range 4–72).
Outcome in 13 Patients With Abdominal Compartment Syndrome Undergoing tPA-Assisted Decompression
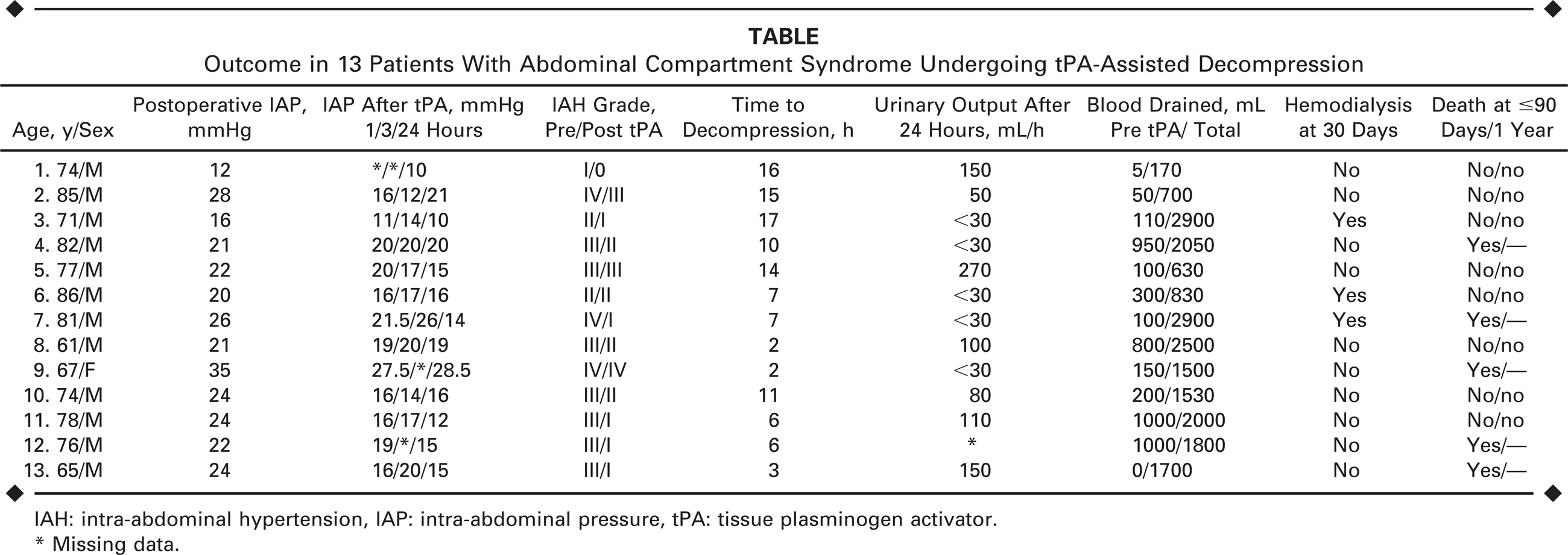
IAH: intra-abdominal hypertension, IAP: intra-abdominal pressure, tPA: tissue plasminogen activator.
Missing data.
Of the 13 patients, 7 had a documented increase in urine production (mean 130 mL/h, range 50–270) at 24 hours after tPA-assisted decompression and all survived. There were 5 patients who did not show any signs of improved urinary production; 3 of these patients received temporary hemodialysis within the 30-day follow-up period. One patient who did not improve clinically [the IAP remained very high (28.5 mmHg), and the blood lactate level increased] was taken to the operating room for a laparotomy. A colectomy was performed due to intestinal ischemia, but the patient died several days later despite these efforts. None of the other patients underwent a laparotomy. The first patient had a grade I ACS but with a distended abdomen and sharp decrease in urinary production was clinically evaluated to benefit from decompression. The 30-day, 90-day, and 1-year mortality rate was 38% (5 of 13 patients). There were no deaths or signs of internal bleeding related to the tPA-assisted decompression treatment.
DISCUSSION
Abdominal compartment syndrome is a severe complication of EVAR for ruptured AAA and is associated with increased mortality.3,6 Laparotomy (or a retroperitoneal surgical approach) has been the gold standard to immediately decrease IAH, which can be the result of residual hematoma in the abdominal cavity or swollen intestines. A laparotomy with or without a delayed abdominal closure is, however, a major surgical procedure with high morbidity that demands long postoperative intensive care.
EVAR is a minimally invasive approach to treating ruptured AAA, but in the face of ACS, it has the potential to become a major surgical intervention with prolonged hospital stay. While it is possible to drain a hematoma with a catheter, there is a limit to how much and how fast that can be done. By combining catheter drainage and tPA injection, a more effective evacuation of the hematoma can be achieved. 10 Continuous re-evaluation and clinical observation is important when making the decision to do an open procedure, tPA-assisted decompression, or to treat the patient conservatively.
The major advantage with this novel method is that it is a minimally invasive technique that can be performed under local anesthesia. It is possible to evacuate large amounts of blood and decrease the IAP, thus avoiding a laparotomy. However, tPA-assisted decompression does not allow inspection of the abdominal cavity and the intestines or reduction of the pressure from swollen intestines. The full effect of tPA-assisted decompression might take several hours or even days to manifest. We observed only a mild effect in the first hours, which should be taken into consideration when rapid decompression is indicated. It is important to be sure that there is no type I endoleak on the completion angiogram, as catheter decompression can accelerate existing bleeding.
CONCLUSION
The tPA-assisted decompression technique is a feasible, minimally invasive tool to decompress ACS or at least relieve the IAH in selected patients in whom a retroperitoneal hematoma is the major component. This method does not replace direct laparotomy or a retroperitoneal approach, and the main challenge is to identify the patients who will benefit from this procedure.
Footnotes
Acknowledgments
We would like to thank Mrs. Suzan Prince-Swartz and Ms. Robin Quell for help with language revision.