
Abstract
Purpose
To report 1-year results from the first subgroup of patients treated with the Multilayer Flow Modulator (MFM) stent for aortic aneurysm and dissection.
Methods
Up to December 2012, 243 patients have been treated worldwide for aortic aneurysm and dissection with the Cardiatis MFM under the established indications for use. This retrospective review encompasses the first 55 of these patients (41 men; mean age 64.5±18 years), who were treated on a compassionate basis in 11 countries. There were 31 thoracoabdominal aortic aneurysms (8 Crawford type I, 3 type II, 9 type III, and 11 type IV), 7 arch aneurysms, 3 infrarenal abdominal aortic aneurysms, 8 suprarenal aortic aneurysms, and 6 type B dissections. Mean aneurysm diameter was 6.04±1.66 cm, and the mean length was 11.58±7.62 cm. The primary endpoint at 1 year was a composite of rupture and aneurysm-related death. The secondary endpoints were all-cause mortality, visceral branch occlusion, adverse events (i.e., stroke and paraplegia), and reintervention.
Results
Technical success was 98.2%; there was no paraplegia or perioperative visceral or renal insult. The mean number of side branches covered was 3.7±1.3 per case (range 0–6); 108 stents were deployed (range 1–5). At 1 year, aneurysm-related survival was 93.7%, all-cause survival was 84.8%, intervention-free survival was 92.4%, and all of the 202 side branches were patent. There were no stent fractures. At 6 months, the mean rate of sac volume increase was 0.36% per month, resulting in a mean volume increase of 2.14%. At 12 months, the rate of increase had slowed to 0.28% per month, resulting in a total average increase in sac volume of 3.26%. The ratio of thrombus to total volume stayed almost constant over the 12 months at 0.48, while the ratio of flow to total volume fell from 0.21 to 0.12 at 12 months.
Conclusion
MFM implantation instigates a process of aortic remodeling involving initial thrombus deposition, which slowed between 6 and 12 months. Increasing sac size did not herald rupture, and the MFM was not associated with loss of native side branches. With physiological modulation of the aneurysm, the MFM offers promise for resolution of complex thoracoabdominal pathology with off-the-shelf availability, but this disruptive technology requires further development and technical refinement. Long-term follow-up of the registry patients is mandatory before establishing a randomized controlled study.
Keywords
Patients with thoracoabdominal aortic aneurysm (TAAA) have been classically managed by open surgical repair, but despite surgical advances and the introduction of newer less-invasive techniques, such as hybrid repair or branched endografts, these patients remain a surgical challenge. The high incidence and severity of complications and failure to reproduce acceptable outcomes outside of high volume centers has fueled the drive for a less invasive, more efficacious, and more universally reproducible solution for TAAA repair.
See commentary page 378
Disruptive technology with Multilayer Flow Modulator (MFM) stents is emerging as an alternative to abrupt aneurysm exclusion and is an unorthodox concept for the management of aneurysmal disease. The MFM stents are self-expanding mesh constructs of cobalt alloy wires interconnected in 5 layers (Fig. 1). They are extremely flexible devices with high kinking and fatigue resistance and low total porosity due to their interlocking layers. The construct channels blood flow to native side branches and slows the flow vortices within the aneurysm sac, thus laminating blood flow. Through this mechanism of flow modulation, the MFM device treats the aneurysm rather than excluding it. The MFM has the advantage of being simple and easy to deploy, and its minimal invasiveness allows for negligible impact on patients' comorbid status, rendering it ideal for use in high-risk polymorbid patients.
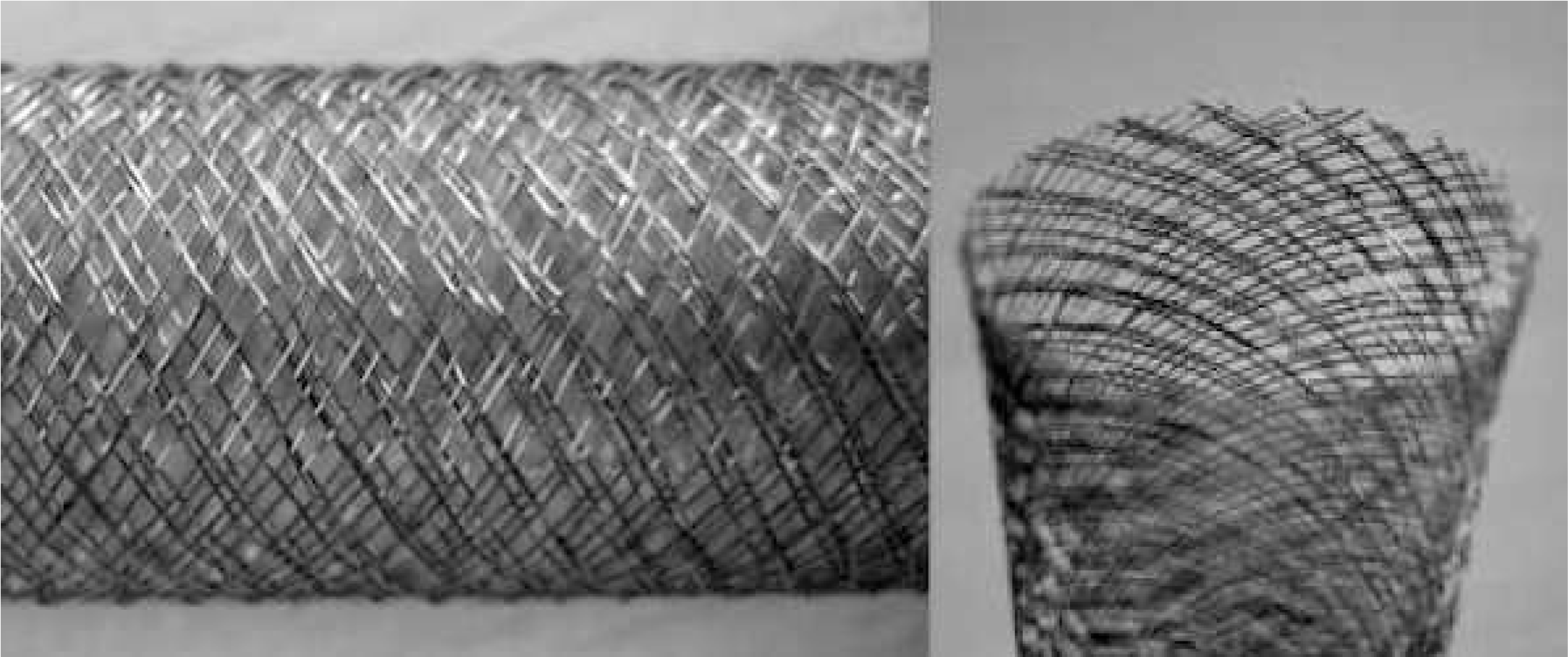
Longitudinal and transverse images of the Multilayer Flow Modulator stent.
The aims of this study are to examine the null hypothesis that the MFM is a safe technology that can be utilized in managing complex aortic pathologies.
METHODS
Study Design
Between August 2010 and December 2012, 243 patients worldwide were treated for aortic aneurysm or dissection under the indications for use of the MFM stent (Cardiatis, Isnes, Belgium) and enrolled in an independent registry. This retrospective review examines the first 55 patients treated according to established indications, i.e., aortic aneurysm (ascending, arch, descending thoracic, thoracoabdominal, and pararenal) or Stanford type B dissection. Patients were not eligible for treatment with the flow-modulating technology if they had ruptured aneurysm; a contained leaking aneurysm; stenotic branches (visceral, great vessels of the head and neck, iliac, coronary); occluded aortoiliac segment; infection associated with previously inserted grafts or endografts; mycotic aneurysms; myoproliferative blood disorders; coagulopathy; or a life expectancy <6 months. Written informed consent was obtained from all patients, and ethics board approval was granted as required in each of the individual clinical institutions where the procedures were performed.
Study Sample
Fifty-five patients (41 men; mean age 64.5±18 years) were treated on a compassionate basis in 11 countries between August 2010 and May 2012. The majority of the patients (80%) were American Society of Anesthesiologists (ASA) class IV, while 14.5% were ASA III. The pathologies included 31 TAAA (8 Crawford type I, 3 type II, 9 type III, and 11 type IV), 7 arch aneurysms, 3 infrarenal abdominal aortic aneurysms (AAA), 8 suprarenal aortic aneurysms, and 6 type B dissections. In the aneurysm cases, the indications for intervention were aneurysm diameter >5.5 cm unless the aneurysm was saccular, embolizing, and/or tender (n=10, 20.4%). The dissections were all chronic, but they were complicated by false lumen sac expansion >5.5 cm. There were no cases of rupture. Mean aneurysm diameter was 6.04±1.66 cm (median 5.76 cm), and the mean length was 11.58±7.62 cm (median 9.2 cm). All cases were fully analyzed through the MFM registry.
Treatment Protocol
Patients were treated at the discretion of the interventionist according to the Instructions for Use. Notably, the landing zone at the proximal and distal ends of the treatment zone had to have at least 1 cm of normal arterial wall into which the MFM stent was positioned. The MFM had to be oversized by 12% to 18% in comparison to the outer diameter of the normal arterial wall at the landing zones. Multiple MFM stents had to overlap by 4 to 6 cm, and the smaller diameter stent had to be deployed first and the larger diameter stent within the smaller one. Postoperative clopidogrel (75 mg/d) was recommended for at least 12 weeks. Follow-up consisted of clinical examination, abdominal radiography (anteroposterior and lateral views), and computed tomographic angiography (CT) at 3-month intervals.
Morphology, Image Analysis, and Clinical Endpoints
Aneurysm sac morphology was assessed by two independent, blinded operators based on CTA images from baseline, prior to MFM implantation, and at 3-month intervals post intervention. The CTA images were examined using 3-mensio software (3mensio Medical Imaging, Bilthoven, The Netherlands) to measure the maximum sac diameter, total sac volume, and thrombus volume, the latter defined as the difference between the total sac volume and the lumen volume.
Clinical endpoints were assessed and reported according to the Society for Vascular Surgery guidelines. 1 The primary endpoint at 1 year was a composite of rupture and aneurysm-related death. The secondary endpoints were all-cause mortality, visceral branch occlusion, adverse events (i.e., stroke and paraplegia), and reintervention. Other outcome measures evaluated were technical success and the rates of change in total sac, thrombus, and flow volumes.
Statistical Analysis
Survival was analyzed using Kaplan-Meier curves and reported up to the time point just before the standard error exceeded 10%. Diameters and volumes were presented as both mean ± standard deviation and median. Interval changes were compared using a Student t test for continuous variables or a chi-square test for discrete variables. Statistical significance was defined at the p<0.05 threshold. Statistical analysis was performed using SPSS software (version 5; IBM Corporation, Somers, NY, USA).
RESULTS
Initial Results
Technical success was 98.2%. The only technical failure involved a patient with a type III TAAA in whom the distal portion of the most caudal MFM failed to fully expand. When attempting to balloon dilate the stent, the balloon burst at below nominal pressure. Two subsequent balloons also burst and because the stent was not flow-restricting, a decision was made to do no further intervention. A CTA at 3 months showed that the stent had intrinsically expanded.
There were no conversions to open repair or admissions to the intensive care unit. No perioperative paraplegia or visceral or renal insult occurred. There was no major blood loss (defined as loss of >20% of blood volume), and there was no indication for blood transfusion. The 30-day mortality was 0%.
The mean number of side branches covered was 3.7±1.3 per case (median 4, range 0–6) for a total number of 202 branches. The total number of stents used was 108 (mean 1.96±1.09, median 2, range 1–5). A single MFM was used in a 77-year-old patient with a saccular AAA in whom no side branch was covered. The patient was not fit for an open repair, and an endovascular repair using a MFM treated the aneurysm with the minimum amount of synthetic material. There were no pre-existing side branch stenoses in the current population, so there was no indication for adjuvant angioplasty or stenting.
Follow-up
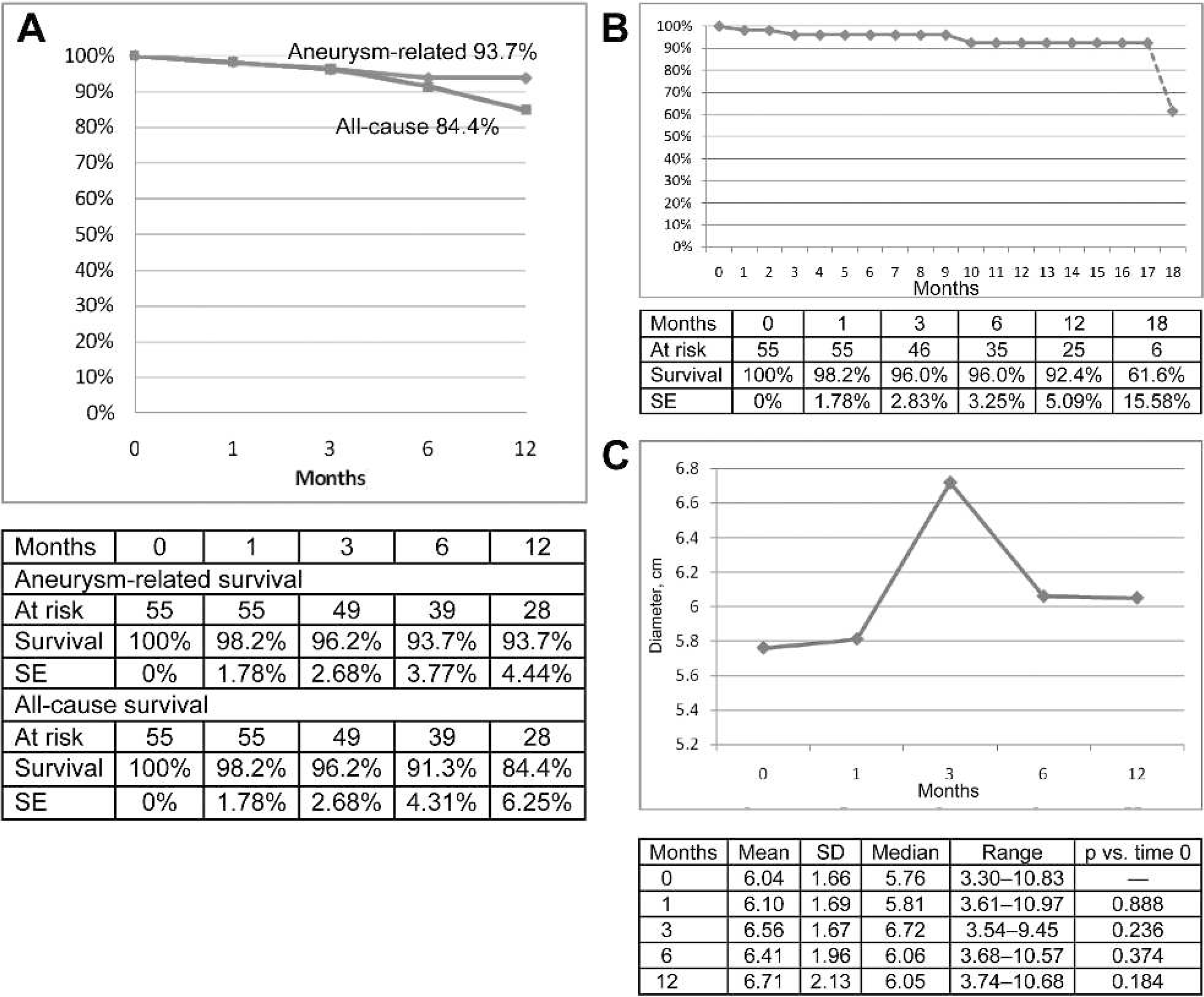
Mean follow-up was 8.2±5.3 months (median 6, range 3–18). No patients in this sample were lost to follow-up. Almost three quarters (39, 71.9%) of the patients were available for 6-month follow-up, and 28 (50.9%) were available at 12-month follow-up. Aneurysm-related survival was 93.7% at 1 year (Fig. 2A); no rupture occurred. At 12 months, all of the 202 side branches were patent. There were no stent fractures.
(
One-year all-cause survival was 84.8% (Fig. 2A). Four cases of bleeding were observed; two of these patients, a 76-year-old woman and a 60-year-old man, died from hemorrhagic stroke at day 36 and after 6 months, respectively. The incidence of stroke was thus 3.6%. Another death was recorded within the first 6 months in a 65-year-old Jehovah's Witness who had gastrointestinal bleeding and refused a blood transfusion. The fourth case of spontaneous hemorrhage occurred in a 77-year-old woman at day 31 post reintervention (20 months after primary intervention). She presented with hematuria and bleeding from her left ear, which subsequently resolved.
Diagnostic workup was available for only two of the cases of unexplained bleeding. The 76-year-old stroke victim had a platelet count <50×10 9 /L and the 77-year-old with hematuria and bleeding from her ear had fibrinogen levels <100 mg/dL. These patients had International Society on Thrombosis and Hemostasis disseminated intravascular coagulopathy (DIC) scores <5, so DIC was ruled out. 2 A consultant hematologist involved in the diagnostic workup of both cases found no underlying cause of hemorrhage and attributed the hemorrhages to the MFM implantation.
One-year intervention free survival was 92.4% (Fig. 2B). There were 4 reinterventions due to stent foreshortening with retraction of the stent back into the aneurysm sac. The reinterventions all involved deployment of a further MFM with 6-cm overlap within the primary stent, one within the first month, one at 10 months, and two at 18 months after the initial implantation. There were no complications associated with the reinterventions, and the patients were discharged from the hospital within 24 hours. One patient required a femorofemoral crossover graft within the first 6 months after MFM implantation due to progression of atherosclerotic disease distal to his MFM. This reintervention was also uncomplicated, but the patient died during follow-up from intracerebral hemorrhage as noted above.
Sac Diameter and Volume Changes
The mean maximum sac diameters at 6 months (6.56±1.67 cm) or at 12 months (6.71±2.13 cm) did not vary significantly from baseline (6.04±1.66 cm; p=0.236 and p=0.184, respectively). Following an initial increase in the median maximum diameter (Fig. 2C) at 3 months to 6.72 cm, the median fell again at 6 months (6.06 cm) and remained reduced at 12 months (6.05 cm).
The mean absolute volume of the aneurysm sac (Table) increased over time (309.84±259.62 cm3 at time 0 vs. 355.39±328.56 cm3 at 12 months, p=0.605), as did the absolute volume of thrombus. In both, the greatest increase occurred between 6 and 12 months (Table), but this was not statistically significant. The mean flow volume varied little over 12 months. The median total and flow volumes both started to decrease between 6 and 12 months, while the median thrombus volume increased over this period. The ratio of thrombus to total volume (Table) stayed almost constant over the 12 months at 0.49±0.26 (p=0.743), while the ratio of flow to total volume fell from 0.21±0.15 to 0.12±0.10 at 12 months (p=0.069).
Changes in Sac, Thrombus, and Flow Volumes Over a 12-Month Period
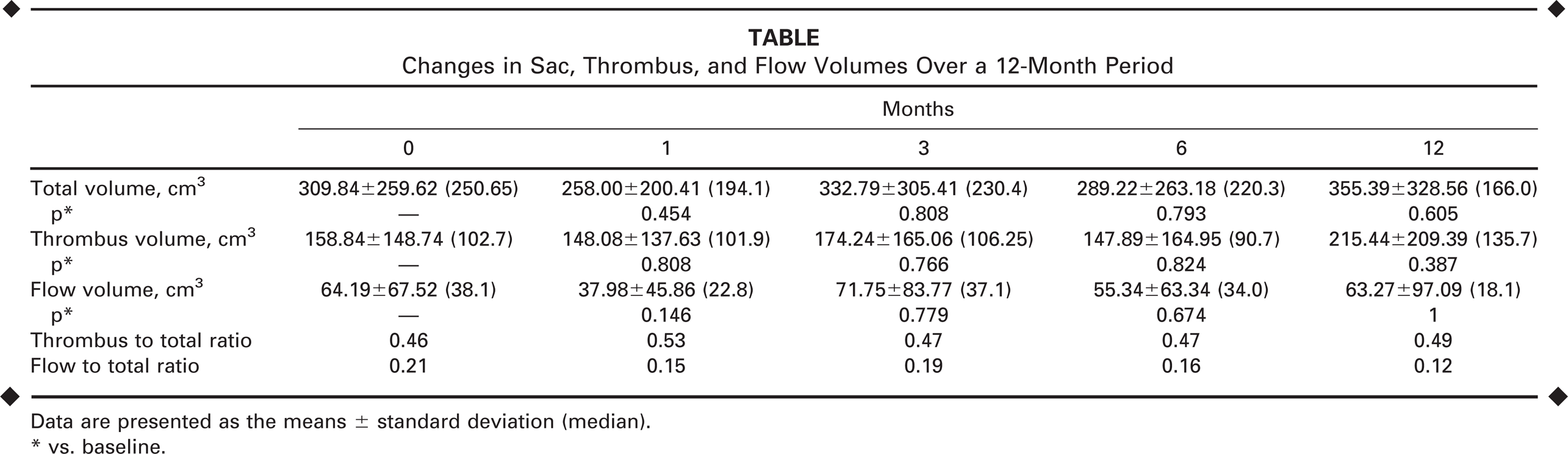
Data are presented as the means ± standard deviation (median).
vs. baseline.
At 6 months, the mean rate of sac volume increase was 0.36% per month, resulting in a mean volume increase of 2.14%. At 12 months, the rate of increase had slowed to 0.28% per month, resulting in a total average increase in sac volume of 3.26%, but the reduction in sac volume increase was not significantly different between 6 and 12 months (p=0.460).
DISCUSSION
In the search for ever-decreasing invasiveness in the treatment of aortic diseases, the evolution of fenestrated and branched technology was initially promising. However, realistic assessment of fenestrated and branched technologies demonstrates that, just as in open and hybrid techniques, acceptable outcomes are only achievable in high volume specialist centers.3–5 Furthermore, even in such specialist centers, mortality and spinal cord ischemia risks are still considerable with this technique and offer no real advantage over open surgical techniques. Greenberg et al. 6 reported a series of 633 patients undergoing endovascular repair (ER) who were matched according to the anatomical extent of disease with those having contemporary surgery. The mortality was similar at 30 days (5.7% for ER vs. 8.3% open, p=0.2) and at 12 months (15.6% ER vs. 15.9% open, p=0.9). Paraplegia rates were also similar between the groups (4.3% ER vs. 7.5% open, p=0.08).
Other issues with fenestrated and branched technologies are the time delays from design to implantation and the prohibitively high cost. Even the more recent availability of “off-the-shelf” branched devices has failed to provide more general applicability or ease of use because the diversity in aneurysm morphology and multiple permutations of device configuration means that off-the-shelf branched or fenestrated endografts are not a feasible or practical option. 7 However, the main concern that prohibits the use of these devices is the profound systemic inflammatory reaction that patients are subjected to post implantation. 8
In an 8-year experience with fenestrated endografts, Verhoeven et al. 9 highlighted renal function deterioration as a major concern even when treating juxtarenal AAA. In the context of almost uniformly high comorbid burden in patients with aortic disease, such an intense systemic inflammatory reaction is all the more difficult to tolerate. So, although proponents of endovascular repair prophesized a minimally invasive solution for even the most high-risk of TAAA patients, its use, alone or in combination with open techniques, has failed to deliver even in the most expert of hands. An explanation for this could be that the technology itself is fundamentally flawed.
Regardless of the mode of repair, the main issues with TAAA repair remain mortality, spinal cord blood supply, and visceral hemodynamic compromise. There are specific issues with contemporary endovascular repair relating to the adverse effect on aortic wall compliance, shear stresses, and pressures within the aneurysm sac caused by exclusion with relatively stiff covered endografts, which in turn not only increase rupture risk but also compromise spinal artery perfusion.10,11
There is mounting evidence to suggest that exclusion of aneurysms may actually subject the sac to greater pressure, inducing an iatrogenically enhanced risk of rupture and pathological loss of branch patency rather than offering the patients a safe aortic repair. Evidence from the Malmö group12–18 suggests that stiff covered endografts, which do not in any way mimic the native arterial wall, may in actual fact have seriously adverse effects on relative intrasac pressures, pulsatile wall motion, and spinal perfusion, which can essentially cause more harm than good and enhance rather than decrease the risk of aneurysm rupture and spinal cord ischemia.
Contrary to popular belief, persistent flow between the stent and native wall, i.e., endoleak, may in reality be beneficial rather than an adverse prognostic factor in terms of sac expansion. In fact, recognition of the limitations of contemporary endografts has forced investigators to try to overcome such adverse side effects. Lioupis et al. 19 reported the successful investigational use of “paraplegia prevention branches,” which intentionally produce temporary endoleak to allow spinal cord perfusion after aneurysm exclusion as an adjuvant to permissive hypertension or spinal fluid drainage. This is a cumbersome approach that requires three separate trips to the operating theatre and prolonged stay in a high dependency unit during two separate hospital admissions, placing unrealistic demands on the individual patients and on hospital resources. However, this technique did augment spinal cord perfusion and serves as a proof of concept for the undesirable effects of acute aneurysm exclusion.
Diverse therapeutic options are offered with the primary aim of preventing aneurysm rupture without compromising branch vessel patency and thus preserving distal end organ perfusion. Although there are no studies that provide direct and objective comparison of the clinical efficacy and/or relative failing of these different modalities, trials addressing the individual treatment options are universally disappointing in terms of morbidity and mortality. Currently, clinical practice guidelines do not exist to define the indications for determining which type of intervention is most efficacious or which treatment best suits various patient and/or anatomical characteristics.
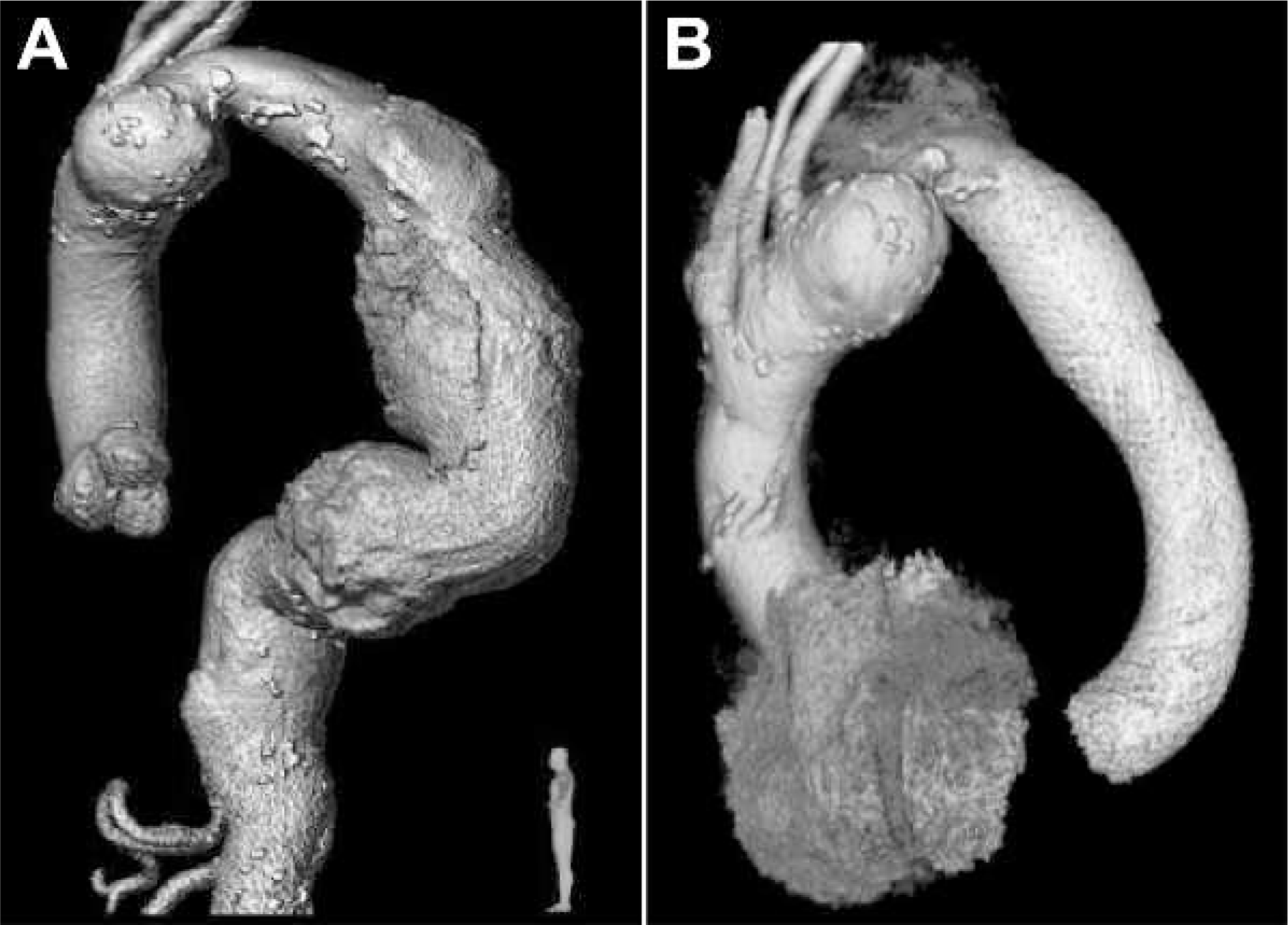
Flow-diverting stents were originally developed for endovascular treatment of intracranial aneurysms, but the technology has been adapted to higher caliber arteries. The Cardiatis MFM has received a Conformité Européenne mark and been approved for management in all aneurysms. Preliminary case reports 20 and reviews 21 involving this device offered great promise for extended use in aortic pathologies, and the preliminary data from our global registry strengthen the case for this technology. 22 The MFM technology has even been successfully deployed in type A and B aortic dissection; Figure 3 shows a patient with complicated type I aortic dissection and 9 cm TAAA, in whom a MFM was smoothly deployed 1 cm from the aortic valve. Compatibility with magnetic resonance imaging modalities without using enhancement dye is an added advantage of this stent.
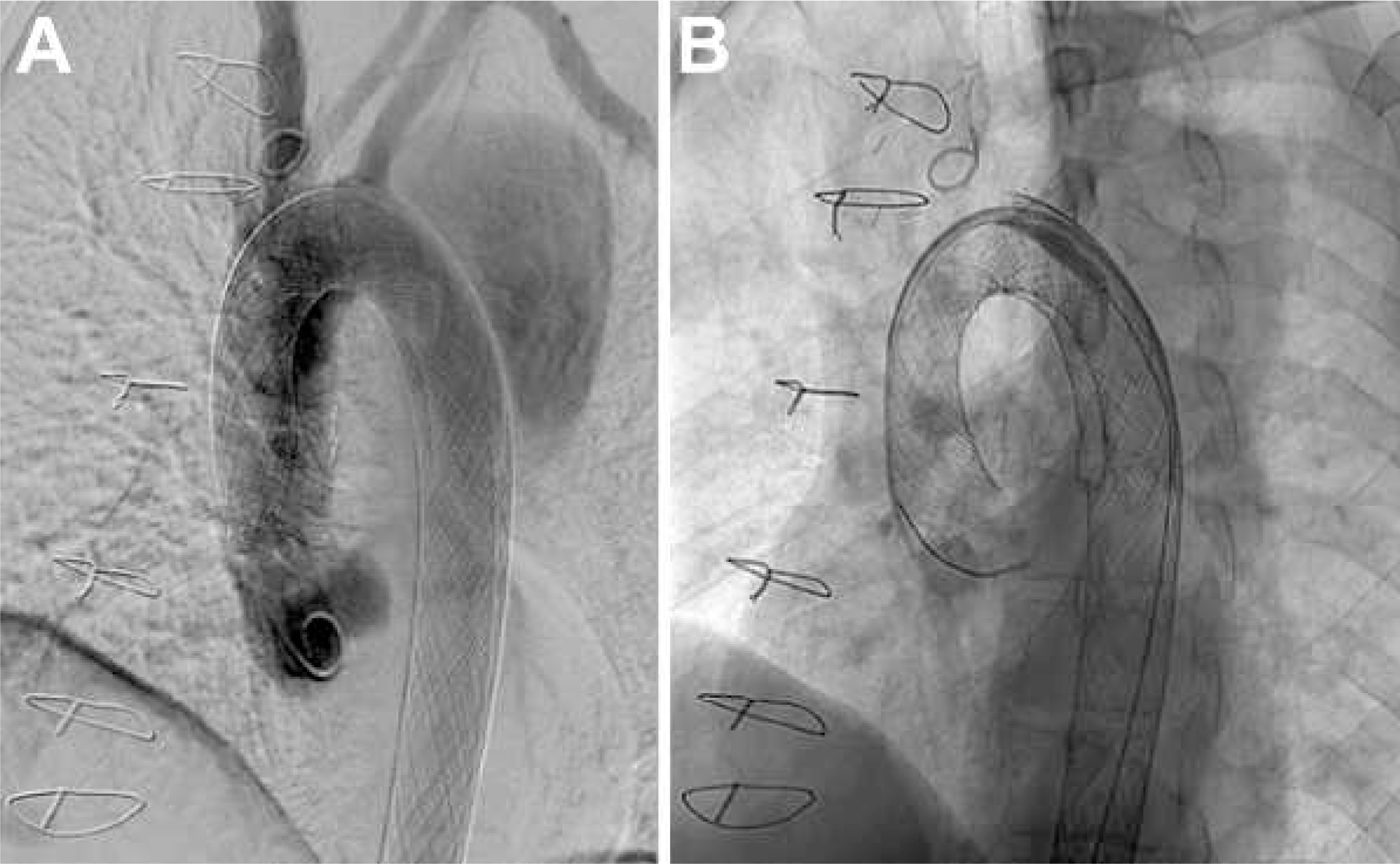
Management of acute type A ascending aortic dissection. The MFM is deployed at the level of the aortic sinus and lies just above the aortic valve.
Aneurysm “exclusion” is not the modus operandi of this device; rather, it acts as a scaffold to allow thrombus deposition, endothelialization, and flow pattern modulation, while maintaining side vessel patency. In our series, the sac volume increased due to thrombus deposition, with the greatest increase occurring in the first 6 months and slowing thereafter. Aneurysm sac remodeling was evident from the relative changes in sac composition, flow volume, and thrombus volume over time. One year after implantation of the MFM, there has been no aneurysm rupture reported in this initial subset of registry patients.
TAAA repair is tempered by the high-risk patient population in whom this specific aneurysmal pathology most commonly occurs. Most TAAA patients are elderly, with a high surgical risk profile. Even in contemporary series of open TAAA repair, the rate of paraparesis or paraplegia can still be as high as 13.2%, and renal failure requiring dialysis rates range to 5.6%. Overall 30-day mortality is as high as 19.0%, and 1-year mortality can reach 31%.23–28 Furthermore, open surgical techniques are confined to high-volume centers. Utilizing the National Inpatient Sample, Cowan et al. 29 reported a 23.8% mortality in patients treated by low-volume surgeons compared to 11% for high-volume surgeons, reinforcing the notion that thoracoabdominal aortic surgery outcomes are volume-dependent and not universal. Notably, TAAA repair complications, such as paraplegia and renal failure, were not evident in our series of patients treated with a MFM.
Chandra and coworkers 30 were the first to report the use of a bare metal stent for AAA exclusion in a patient with severe aortoiliac disease, deploying 2 overlapping Wallstents and coils through an 8-F system. Two years later, Achari and Krajcer 31 reported similar success using an 11-F system without coils in a high-surgical-risk patient with severe concomitant iliac disease. They reproduced these results in 2000 32 in a 60-year-old man with an inflammatory AAA; 2-year follow-up showed aortic sac shrinkage, stabilization of thrombus, and regression of periaortitis. In each of these studies, the authors enthused that the advantages of the bare metal stents included their low profile, which allows deployment through small iliac vessels, and increased stent trackability and flexibility, which made stent deployment feasible in tortuous vessels. The authors postulated that uncovered stents significantly reduce the size of the AAAs, providing a framework for neointimal growth without occluding side branches.
The mechanism of aneurysm closure by bare stents is the induction of shear forces by the wires across the opening of the aneurysm, which leads to a reduction in laminar flow and, subsequently, thromboses the aneurysm sac. This redirection of flow toward the lumen and away from the dilated aortic wall promotes healing and contraction of the dilated aorta. Endothelialization of bare metal stents occurs via three mechanisms: migration of endothelial cells through the stent struts, migration of endothelial and fibroblastic cells from the adjacent aorta at the margins of the stent, and circulating myofibroblasts. The continued laminar flow into major side branches inhibits this process and maintains patency of the side branches.
Preliminary clinical experiences with bare metal stents were promising,33,34 and subsequent studies that showed less favorable results were most certainly undermined by the use of embolization coils, which adversely interfered with intrasac pressures. 35 Canic et al. 36 used mathematical modeling to compare bare metal stents to covered endografts and showed that a single bare metal stent is 10 times more flexible and elastic than the wall of the aneurysmal abdominal aorta. Changes in the diameter and length of the stent when exposed to a range of internal and external pressures demonstrate that if the aorta is axially stiff and resists length change, a force as large as 1 kg can act in the axial direction on the aortic wall, but if the stent is not firmly anchored, it will migrate.
A fabric-covered, fully supported stent-graft is significantly less compliantthan the aorta or a bare metal stent. During each cardiac cycle, the stent frame tends to move, while the fabric resists movement, which can break the sutures that join the fabric to the frame. Elevated local transmural pressure, detected along the prosthetic graft, can contribute to material fatigue. Therefore, a happy medium may lie in a layered bare stent that preserves flexibility and maintains side branch patency but is not as susceptible to material fatigue or acute pathological increases in sac pressurization as the contemporary covered endografts. In contrast to contemporary endografts, the MFM stent has been found to become adherent and readily embedded into the aortic wall, allowing minimal relative movement between the aorta and the stent.11,37
Measurements from the Canic study, 36 as with previous studies in both bare metal stents and endografts, highlight the inaccuracy of using diameter as a surrogate marker of disease progression. More attention to sac geometry and 3-dimensional parameters yields more precise predictions of sac behavior. We previously documented that the volume and length of the aortic sac are more predictable of sac progression and rupture in patients with expanding AAA than a diameter measurement, and the ratio of maximum diameter to length is the most accurate forecaster of sac rupture. 38
The MFM curtails the odds of aneurysmal rupture through dissipation of wall stress by permitting an organized thrombus to develop, initiating laminar flow in the aortic sac and maintaining vital branches. The slight increase in volume at a rate of 0.36% per month in the first 6 months, which slowed to 0.28% per month by 12 months, is the effect of modulation and management of the aortic sac and offers a more controlled manipulation of the body's innate physiological potential for auto repair than the abrupt and unnatural exclusion of the sac by covered endografts. Median total volume, median flow volume, and the ratio of flow to total volume decrease beyond 6 months, as would be expected with a change from turbulent uncontrolled flow toward a more physiological laminar flow pattern within the aneurysm sac.
Endoleak has not been reported in this study because it does not apply to the MFM device, which does not exclude the aneurysm. It is an uncovered stent and so flow will continue to occur between the stent and the aneurysm wall as thrombus is laid down and vessel wall modulation occurs. The uncovered nature of the stent means that flow is not occurring within a closed space, as happens with conventional covered endografts that exclude the aneurysm. Consequently, pressure buildup is not an issue within the MFM as it is with conventional devices, and attempts to treat endoleak post MFM can cause more harm than good. 37 Endoleak is a term that should be confined to studies involving conventional covered endografts.
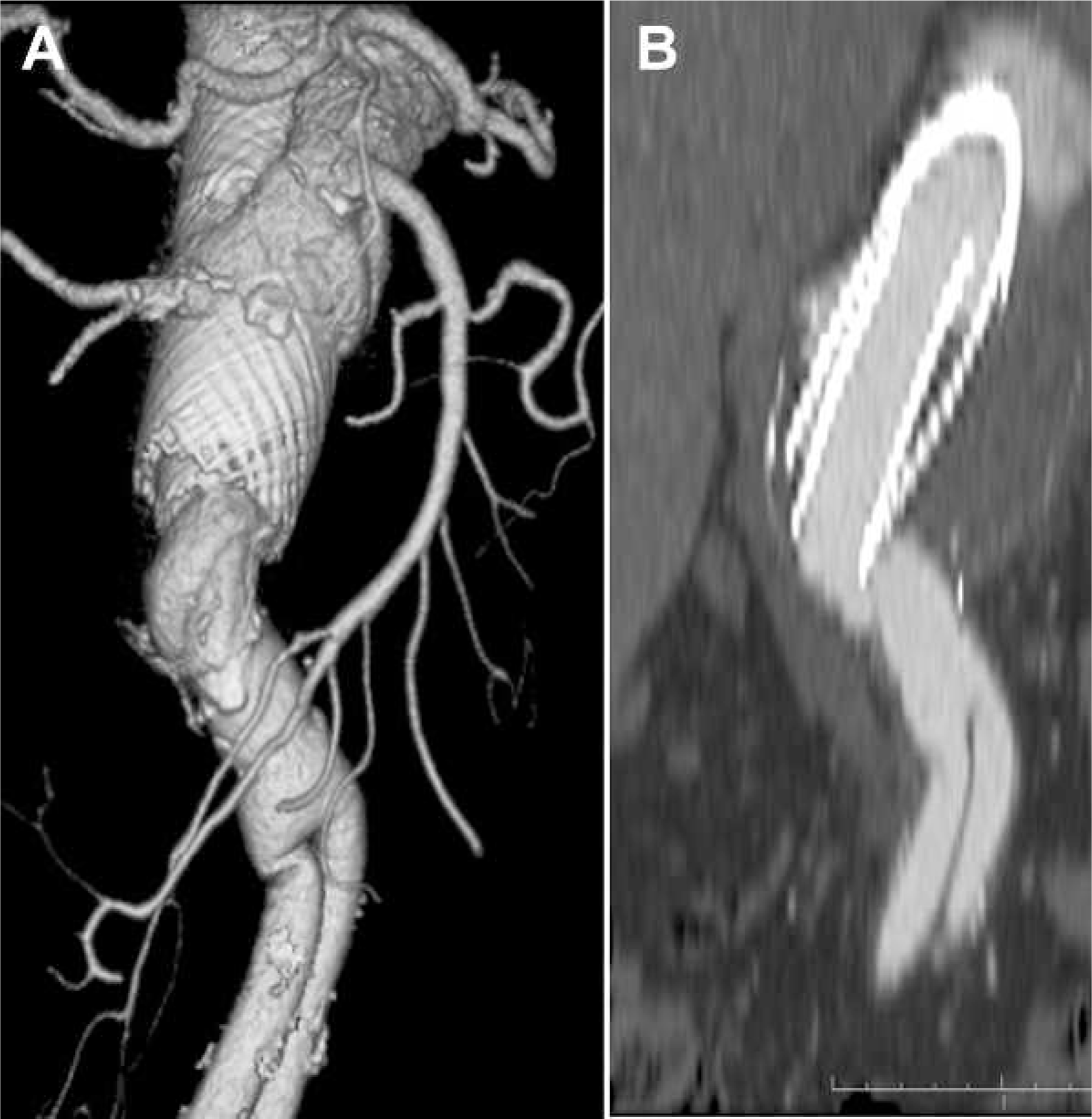
A few technical issues deserve discussion. First, the operator needs to be acutely aware of the potential for foreshortening of the MFM on deployment. In contrast to standard self-expanding nitinol stents, which are cut from a tube into an open lattice design, multilayer stents exhibit a significant shortening during deployment of up to 33% compared to its unfolded length in the delivery sheath. This is a result of its interwoven design, which makes the degree of shortening not always easy to predict. A consequence of this is that if the distal landing zone is selected too far distally, the target zone might not be completely covered, so the stent will not realign the flow and thus could lead to sac rupture. Figure 4 depicts a technical failure that resulted from not covering the proximal normal aorta (this patient was not included in the current report).
Case 98 (
If foreshortening does occur, the situation is redeemable, and the deployment of a second stent does not adversely impinge on clinical efficacy. We have had to double stent across the visceral branches, and it did not result in any loss of side branches. A caveat, however, is that it is crucial to deploy the smaller diameter stent first. Figure 5 demonstrates a technical failure that resulted from implanting a smaller diameter MFM in a bigger one, causing increased wall shear stress and vortices that led to TAAA rupture (this patient was not among the first 55 cases in the current report).
Case 145 (
Further technical difficulties can arise when attempting to deploy a MFM in a previously treated aorta. Anecdotal evidence does exist for the successful use of the MFM as a secondary intervention post previous endovascular or open thoracoabdominal aortic repairs. However, there is insufficient evidence and a lack of long-term follow-up to recommend the use of the MFM in these circumstances. Ideally, the MFM should be deployed such that both proximal and distal ends appose normal aortic tissue. Failure to do so can have devastating consequences as evidenced by Lazaris et al., 37 who published a case in which a MFM was used to treat a pseudoaneurysm at the proximal anastomosis of a previous open AAA repair. The patients presented 12 months later with a fatal rupture. The variability in compliance between the MFM and previous Dacron graft, or a previous implanted endograft, leads to misalignment and adverse flow patterns that ultimately can result in rupture, as the Lazaris experience highlights. Although the learning curve is very steep, physicians employing this technology do need to be intensely aware of the mechanical properties of the stent and have a keen understanding of the physiological processes that are being therapeutically manipulated by the MFM.
A precaution that we take in all of our patients is to manage endovascularly any side branch stenosis prior to MFM deployment on the hypothesis that such stenosis could increase the vortices in the area and affect target organ perfusion.
All of our patients are on dual antiplatelet therapy with acetylsalicylic acid and clopidogrel; however, clopidogrel is discontinued after 6 months. In our opinion, antiplatelet therapy is needed to preserve side branch patency, and patients should be placed on at least one antiplatelet drug for a minimum of 12 weeks. That said, one needs to remain cognizant that remolding of the aortic sac by the MFM does consume platelets, and this might be impeded by aggressive anticoagulation or antiplatelet medication. Although in our experience an initial drop in platelet count in the first week is not always pathological and it can spontaneously correct itself, the treating physician should remain attentive to the possibility of excessive platelet loss. This is especially true in the case of patients with suspected underlying myoproliferative disorders or potential adverse drug interactions, and it can result in serious adverse bleeding events and death, as evidenced in this series.
Current MFM Limitations and Future Design
Although the flow-diverting concept is exciting, in its current stage of development, the MFM has many shortcomings that will temper enthusiasm for its widespread use until further development is undertaken. The 1-year follow-up is very short, and although marginal increases in sac volume had begun to recede by the end of this observation period, more long-term data are required to assess the lifelong risk of rupture. Furthermore, the effects of the MFM on shear stress, pressure, and flow patterns in vivo and their subsequent effects on rupture risk need more in-depth analysis. Caution should certainly be taken when using the MFM in cases of previous aortic intervention and in aortic rupture. The MFM will require an accurate delivery deployment system. The closed-door MFM stenting design hinders postoperative visceral artery access; consequently, all stenotic visceral side branches must be dealt with preoperatively even if the patient is asymptomatic. Attention must be paid to technical issues, such as foreshortening and accurate sizing during stent overlap. Finally, due to profound platelet consumption, the MFM is contraindicated in cases of myoproliferative disorders and coagulopathies.
Limitations
This study is limited by the brevity of follow-up and the variation in the pathologies and anatomies of the patients treated. It is further limited by the issues that plague any registry. When formulating questions to collect clinical data, one is forced to strike a balance between having enough questions to gain sufficient information and not having too many so as to reduce compliance by the inputting physicians. Registry data are also dependent on the timeliness and accuracy of the individual centers when reporting primary data, follow-up information, and incidence of complications, and it is impossible to fully account for physician bias when submitting data. In addition, patient compliance with follow-up cannot be guaranteed, especially in a high-risk population who are laden with morbidities. Finally, as with any multicenter study, follow-up protocols and pharmacotherapies can vary between institutions despite recommendations being provided.
Conclusion
In this study, MFM implantation instigated a process of aortic remodeling involving initial thrombus deposition, which slowed between 6 and 12 months. The MFM was not associated with critical shuttering or loss of native side branches. With physiological modulation of the aneurysm, MFM offers promise for resolution of complex thoracoabdominal pathology with off-the-shelf availability. It is a disruptive technology that requires further development and technical refinement. Long-term follow-up of the registry patients is mandatory before establishing a randomized controlled study.
Footnotes
Acknowledgment
Our thanks to Amine Benjelloun, Sidney Chocron, Victor Costache, Edward Diethrich, Pascal Leprince, Teodoro Meloni, Vittorio Pedicini, Antonios Polydorou, Jacques Robin, Hervé Rousseau, Marc Sapoval, Thierry Unterseeh, Claude Vaislic, and Jean-Pierre Villemot.