
Abstract
Purpose
To investigate the quality of stent-graft fenestrations created in vitro using different needle puncture and balloon dilation angles in different commercial endografts.
Methods
Fenestrations were made in a standardized fashion in 3 different endograft types: Talent monofilament twill woven polyester, Zenith multifilament tubular woven polyester, and Endofit thin-walled expanded polytetrafluoroethylene (PTFE). Punctures were made at 30°, 60°, and 90° angles using a 20-G needle and dilated using 6-mm standard and 7-mm cutting balloons; at least 6 fenestrations were made at each angle with standard balloons and at least 6 with cutting balloons. The 137 fenestrations were examined under light microscopy; quantitative and qualitative digital image analysis was performed to determine size, shape, and fenestration quality.
Results
PTFE grafts were easier to puncture/dilate, resulting in larger, elliptical fenestrations with overall better quality than the Dacron grafts; however, the puncture/dilation angle made an impact on the shape and quality of fenestrations. A significant number of fabric tears were observed in PTFE fabric at <90° puncture/dilation angles compared to Dacron grafts. In Dacron grafts, fenestration quality was significantly higher with 90° puncture/dilation angles (higher in Talent grafts). Cutting balloon use resulted in significantly more fabric tears and poor quality fenestrations in all graft types.
Conclusion
Different endografts behave significantly differently when fenestrations are fashioned. Optimum puncture/dilation is important when considering in vivo fenestration techniques. Improvements in instrumentation, materials, and techniques are required to make this a reliable and reproducible endovascular option.
Keywords
Diseases of the aorta involving arch and visceral branch vessels require challenging therapeutic maneuvers to ensure preservation of robust arterial flow within vital branches. Custom-made fenestrated and branched stent-graft technology has shown encouraging short- and midterm results in selected patients.1,2 Despite tremendous technological advances in this field, factors such as the inherent delay in device manufacturing, anatomical and technical challenges, high degree of planning, and cost limit the uptake of this technology and render it unsuitable for urgent and emergency cases. In situ fenestration of aortic stent-grafts is an attractive alternative that eliminates the need for preoperative custom tailoring, with the potential to widen the available therapeutic options and to offer a bailout option after inadvertent side branch occlusion.
See commentary page 544
The concept of in situ fenestration involves intentionally covering aortic branches with an endograft and then re-establishing blood flow by puncturing the fabric in vivo.3–17 Once the fabric has been breached, the fabric hole can then be dilated to a desired diameter and a branch stent can be placed to maintain perfusion of the target vessel. This technique can be performed in either a retrograde3,4 (from within the lumen of the side branch, therefore requiring downstream access) or an antegrade (from within the lumen of the stent-graft)16,17 fashion and may be potentially applied to all major aortic side branches.
There is little known about the optimum method of creating fenestrations to prevent tear propagation and long-term failure; there are a number of different methods that could be used. The purpose of this experimental study was to examine and grade different methods of graft puncture and dilation to guide operators in establishing the optimal fenestration technique. Specifically, this study assesses the effect of in vitro needle perforation at different angles and sequential dilation with either standard or cutting angioplasty balloons on various commercially available stent-grafts.
METHODS
Stent-Grafts and Puncture Technique
Graft fenestration techniques were tested on 3 different commercially available endografts: Talent monofilament twill woven polyester (0.09-mm-thick Dacron; Medtronic Vascular, Santa Rosa, CA, USA); Zenith multifilament tubular woven polyester (0.15-mm-thick Dacron; William A. Cook Australia, Brisbane, Australia); and Endofit thin-walled expanded polytetrafluoroethylene (ePTFE; LeMaitre Vascular, Inc., Burlington, MA, USA).
With the grafts held between 2 clamps on the benchtop, the fabric was punctured by hand using a 20-G needle held at 30°, 60°, and 90° angles to the stent-graft material guided by a protractor. The graft puncture site was subsequently dilated using a 6-mm standard angioplasty balloon (Sterling Monorail; Boston Scientific, Natick, MA, USA) or a 7-mm cutting balloon (Boston Scientific). With each balloon, the pressure was gradually increased to 10 atmospheres or until the balloon was fully inflated, with no waist caused by the endograft material. At least 6 fenestrations were made at each angle with standard balloons and at least 6 with cutting balloons (minimum number of fenestrations per graft was therefore 24). Further fenestrations were made if there was sufficient space on the available graft material. In all, 137 fenestrations were fashioned.
Quantitative and Qualitative Assessment
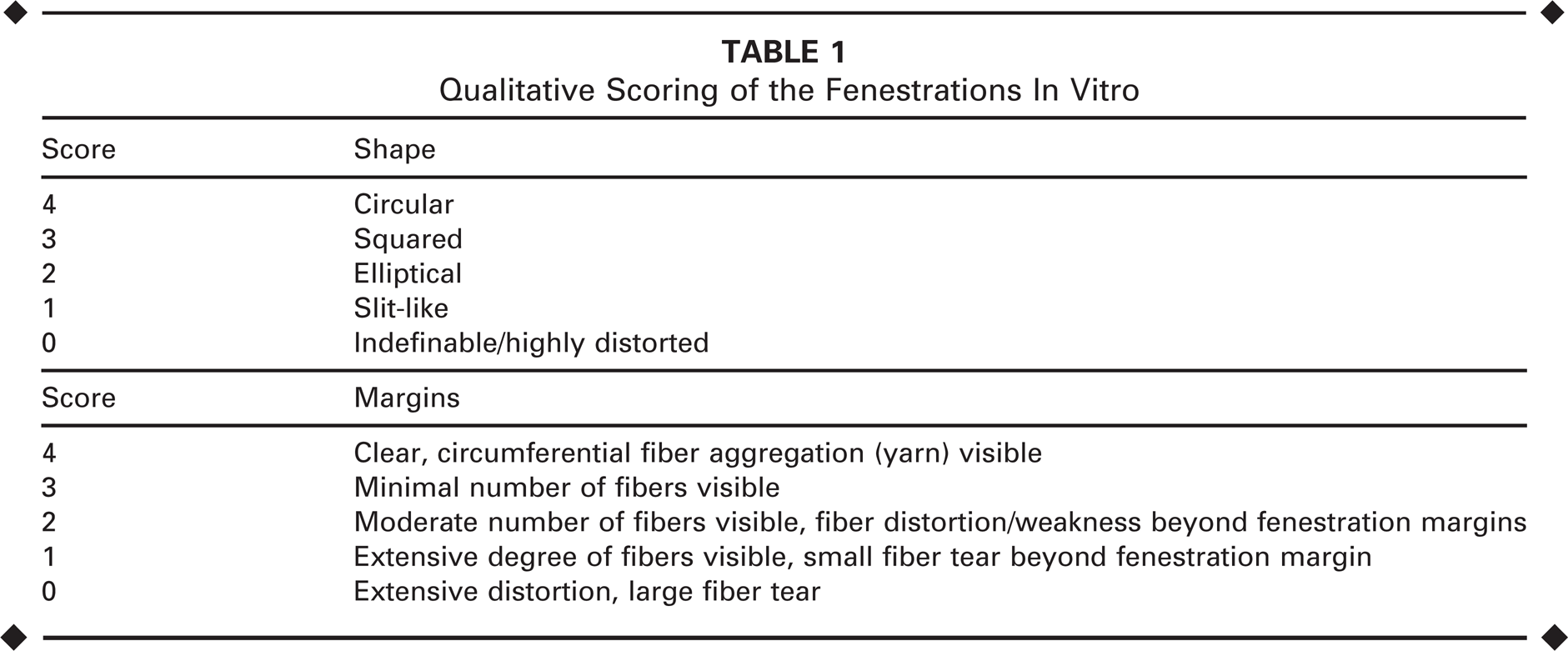
The fenestrations were evaluated using a Nikon Eclipse E400 microscope equipped with a UV light source, phase contrast, and a Nikon DXM 200 digital camera (Nikon, Tokyo, Japan). Images were captured at magnifications ranging from 2 to 100×. Four blinded observers (C.R., C.B., M.H., and N.C.) examined the digital images to determine the maximum diameter of each fenestration and qualitatively assess the shape and margins of each hole, specifically the degree of fiber tears, aggregation, and distortion, using a scoring system (Table 1). The shape of the fenestration was graded as indefinable/highly distorted, slitlike, elliptical, squared, or circular. The fenestration margins were graded between 0 (margins of poorest quality with large fiber tears) and 4 (margins of highest quality with clear circumferential fiber aggregation, i.e., yarn formation).
Qualitative Scoring of the Fenestrations In Vitro
Statistical Analysis
To analyze qualitative data on fenestration shape, the most common grade from the 4 assessors was used; for fenestration quality, the median grades (interquartile range, IQR) are presented. The non-parametrically distributed data were tested for significance using the Kruskal-Wallis test to identify differences between groups. P<0.05 was considered statistically significant. Interobserver reliability for the blinded assessors was calculated with the Cronbach's alpha test statistic. SPSS statistical software (version 18.0; IBM Corporation, Somers, NY, USA) was used for data analysis.
RESULTS
PTFE grafts were easier to puncture and dilate with standard angioplasty balloons, while both Dacron grafts resisted low-pressure dilation. The Dacron fabric of the Zenith stent-graft was the most resilient and resulted in frequent bursting of the balloon when the pressure exceeded 10 atmospheres; therefore, the balloons in this group were not inflated over this pressure, and the balloons did not generally reach 6 or 7 mm in diameter. Dilation of PTFE with standard balloons resulted in significantly larger diameter fenestrations (Fig. 1): median 5.2 (IQR 4.5–6.6) vs. 0.9 (IQR 0.5–1.5) and 0.6 mm (IQR 0.3–1.3) for Talent and Zenith Dacron grafts, respectively (p<0.001).
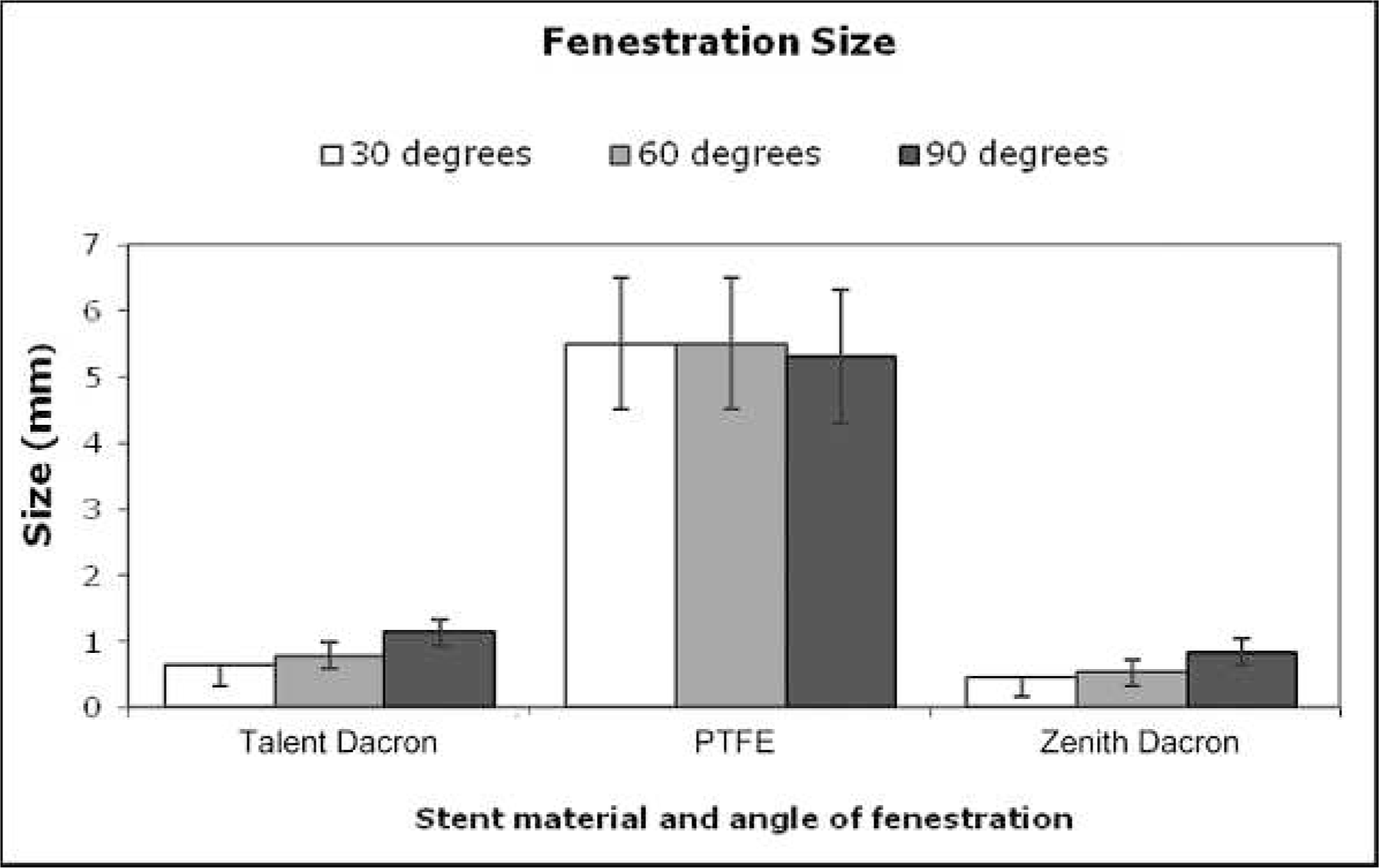
Bar chart representing mean maximum fenestration size after dilation with standard angioplasty balloons at 30°, 60°, and 90° angles. Fenestration resulted in significantly larger diameter defects in polytetrafluoroethylene (PTFE) grafts vs. Dacron fabrics (p<0.001).
There was good interobserver reliability among the assessors (Cronbach's α=0.89) for assessment of fenestration quality. PTFE graft puncture and dilation resulted in mainly elliptical fenestrations, oriented transversally along the endograft. Dacron fenestrations were mostly squared or elliptical; however, in the Talent grafts, the fenestrations appeared circular when the needle/balloon was introduced at a 90° angle (Table 2). Representative examples of fenestrations are shown in Figure 2.
Most Common Descriptive Assessment of Fenestration Shapes After Dilation With Standard Angioplasty Balloons at Various Angles
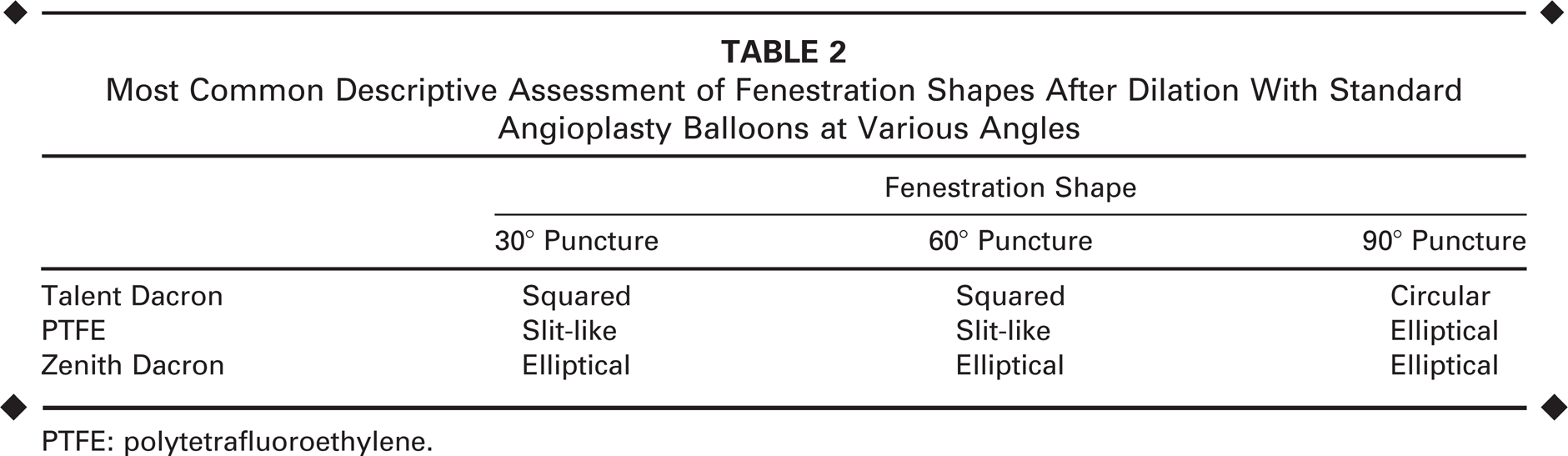
PTFE: polytetrafluoroethylene.
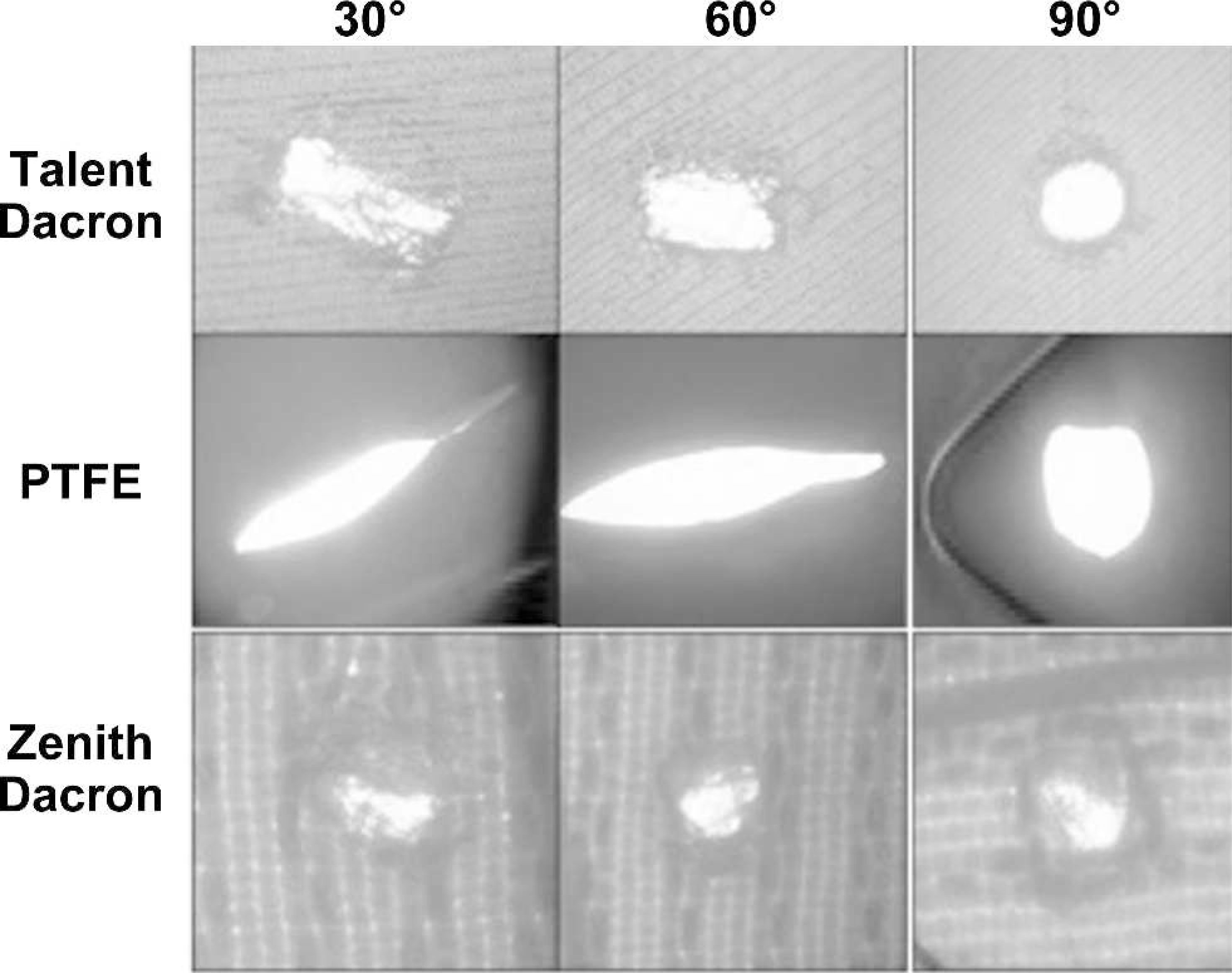
Representative microscopic images (8×) of the fenestrations in the 3 different endograft materials after dilation with standard angioplasty balloons at 30°, 60°, and 90° angles. PTFE: polytetrafluoroethylene.
The median qualitative score given to fenestration margins (Fig. 3) was highest in PTFE grafts and greatest with 90° and 60° angle needle puncture and subsequent dilation. In Talent grafts, fenestration quality improved in a stepwise fashion as the needle was introduced at steeper angles. For Zenith grafts, the median qualitative score was low for all needle puncture angles.
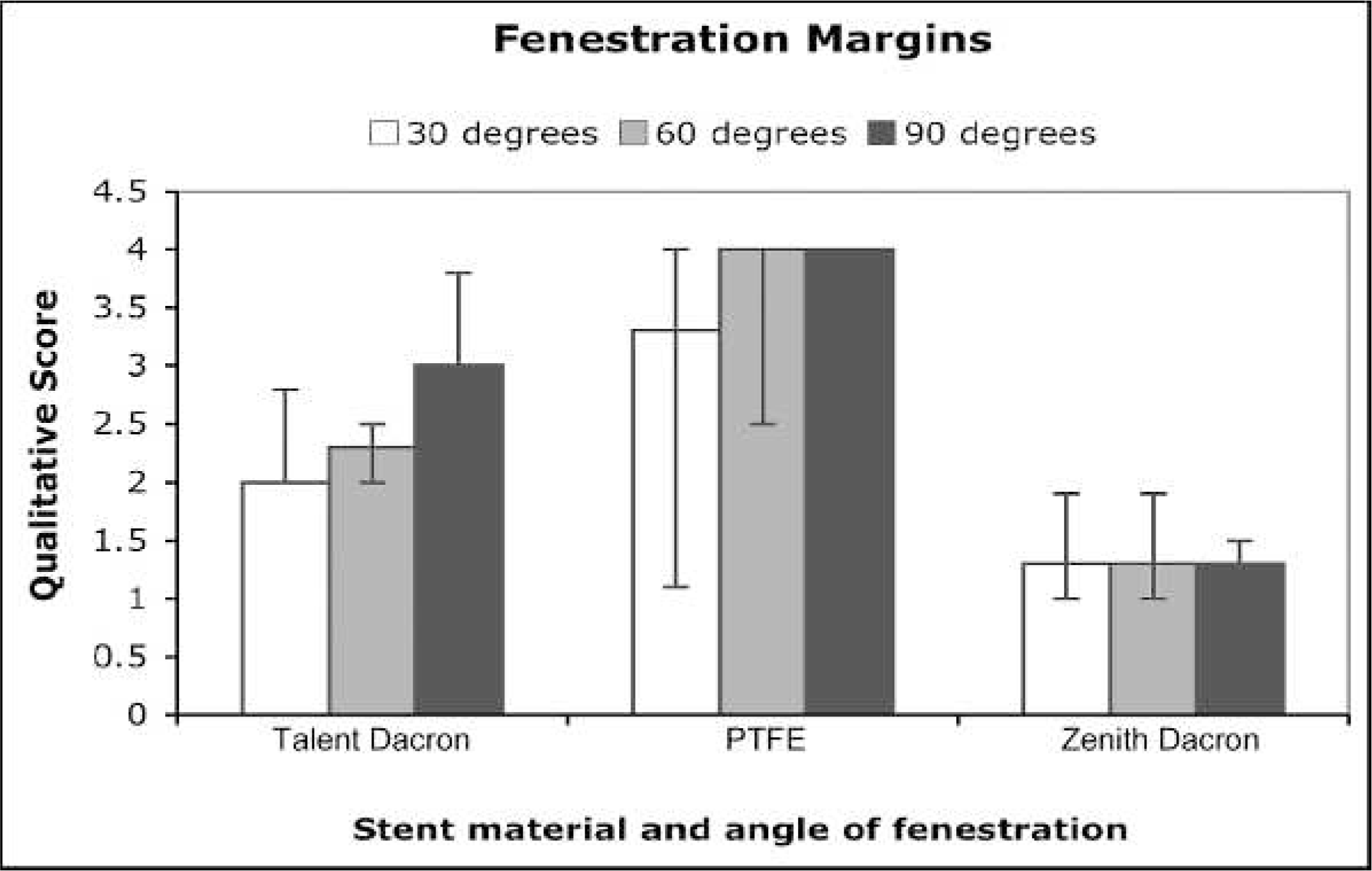
Bar chart representing mean qualitative assessment scores for fenestration margins after dilation with standard angioplasty balloons at 30°, 60°, and 90° angles, where 4 represents the maximum attainable score. PTFE: polytetrafluoroethylene.
There was variability of fenestration quality between grafts. When using standard angioplasty balloons, fenestrations with a margin score of 0 or 1 (and so showing significant tearing outside of the fenestration margins) occurred in 50% of Zenith Dacron grafts, 17% of PTFE grafts, and none in the Talent Dacron grafts. In contrast, use of cutting balloons resulted in significantly more fabric tears beyond the fenestration margins in all endograft types with extensive fiber distortion, fraying, and poor overall quality fenestrations. With cutting balloons, fenestration margin tears (fenestration margin score 1 or 0) were seen in 100% of Talent Dacron grafts, 82% of Zenith Dacron grafts, and 50% of PTFE grafts. There was no significant difference in the size of the fenestration when cutting balloons were used.
DISCUSSION
McWilliams et al. 3 first described retrograde in situ fenestration in bench and animal models, followed by the first successful clinical application in the left subclavian artery (LSA) via supraclavicular access using the back end of a 0.018-inch guidewire, a needle, and serial cutting balloons in a modified Zenith thoracic endograft. 4 A similar approach was used during aortic arch aneurysm repair to fenestrate a stent-graft from an acutely angled LSA using through and through wire access, a pre-curved semi-rigid sheath, and serial balloon dilations. 5 Retrograde puncture and balloon dilation of a thoracic endograft to fenestrate a left common carotid artery during endovascular exclusion of a descending thoracic aortic aneurysm has also been reported. 6
The feasibility of complete aortic arch reconstruction using the retrograde approach and conduit implantation with cerebral circulatory support was first demonstrated by Numan et al. 7 in cadaveric and animal models; balloon-anchored needle dilators and radiofrequency (RF) plasma electrode catheters followed by balloon dilations were used to create fenestrations. Sonesson et al. 8 applied this concept in the emergency clinical setting to treat an acute aortic arch rupture; cerebral flow was maintained using a temporary bypass from the left femoral artery to both carotid arteries. Successful laser in situ fenestration of thoracic endografts via subclavian artery access has been described by some.9,10 Later reports have demonstrated that this technique can be used to revascularize the innominate vessel for aortic arch aneurysms after carotid-carotid and carotid-subclavian bypass. 11
Retrograde in situ fenestration is difficult to apply to the abdominal aorta because of the lack of downstream branch artery access. Percutaneous access to the visceral and renal vessels is certainly challenging. Tse et al. 12 described antegrade fenestration of abdominal aortic stent-grafts in canine models under fluoroscopic guidance using intravascular ultrasound as an adjunct. Renal artery stents were inserted bilaterally prior to fenestration and used as fluoroscopic landmarks. The same group published a similar experiment in canine models, using RF probes for endograft perforation after having marked the renal arteries bilaterally with detachable coils. 13 Our group first reported the use of robotic technology for antegrade in situ fenestration in a porcine model.14,18,19 Subsequently, antegrade in situ techniques have also been used to revascularize the renal arteries during deployment of a C3 endograft above the level of the renal vessels 17 and an internal iliac artery inadvertently covered with an Excluder stent-graft. In the latter case, 6-year follow-up demonstrated maintained perfusion through the fenestration.
These clinical reports use widely varying techniques to fashion fenestrations, but it is clear that this technique is evolving, and the optimum method for fashioning the fenestrations is yet to be determined. There is ongoing interest to improve current materials and methods using advanced technology to make this exciting new concept a viable option for a wholly endovascular approach to aortic pathologies. Current endografts are not specifically designed for fabric perforation and fenestrations. The results from our study demonstrate that different fabrics react differently to perforation and subsequent dilation. Differences observed in the size of the fenestrations fashioned probably reflect the different tensile strengths of the fabrics tested. The attempted dilation of the Zenith fabric resulted in balloon bursting in many cases; the use of a high-pressure balloon may be worth exploring in subsequent studies.
The results of the preliminary in vitro experiment presented here suggest that PTFE is easier to perforate compared with Dacron; the puncture can be readily dilated with a standard angioplasty balloon resulting in larger fenestrations. It is, however, important to note that only one PTFE fabric and two Dacron grafts have been studied, and fabrics from various manufacturers are likely to react differently to fenestration formation.
In addition, there are further considerations regarding the design of current stent-grafts. The stent struts may affect the desired position of the puncture, and if the target vessel is directly adjacent to the strut, then the fenestration will be out of line. Stent design and manufacturing to provide an unsupported section for fenestration or adaptable material properties (e.g., Endologix's Ventana system) need to progress in this area also.
Another influence of stent-graft design is on end organ perfusion, which needs to be taken into account when fashioning the fenestration. Tear propagation is greatly affected by changes in yarn and fabric geometry. 20 Tearing occurs due to breakage of fabric cross-yarns as a result of laterally applied tension; in fabrics with low yarn mobility, such as the high-density fabrics used for endovascular grafts, high stress concentrations develop at the deformation or tear initiation site. 21 Consequently, following graft fenestration, one of the areas of greatest concern is longitudinal propagation of the fabric tear extending beyond the ostium of the target vessel, which may result in significant type III endoleak and aneurysm rupture. One would presume that tears arising during initial formation of a fenestration would be at risk of propagation and subsequent endoleak. One of the limitations of our study is that we have not established a long-term durability testing model. In the same way, we have assumed in this study that the highest quality fenestrations are rounded, as one would expect the branch stent to “fit” the fenestration better and have greater durability if the fenestration were shaped to fit the branch stent device. Despite an encouraging report on long-term follow-up, 16 clinical data on fenestration durability remains scarce.
In our study, the quality of the fenestration margin was affected by the graft type, angle of needle puncture, and subsequent balloon dilation of the graft. The most fenestration margin tears were seen in the Zenith Dacron grafts. PTFE dilation was more likely to result in propagating fabric tears at <90° dilation angles. Microscopic analysis of the fenestrations revealed that fenestration quality is significantly higher when the needle is introduced at 90° angles and that angle is maintained during serial balloon dilations. The highest fenestration quality in this bench experiment was achieved in the Talent Dacron stent-grafts, which showed circular fenestrations with clean margins, good fiber aggregation, and a low incidence of fabric tears. Although the median score for Talent grafts was not as high as PTFE for margin alone, the PTFE graft exhibited tears in 17% of samples studied, and most fenestrations had an elliptical shape. Presuming the fenestration can be opened and maintained by the branch stent, then the Talent graft would appear to be the most suitable among those tested in this study.
Cutting balloon use resulted in significantly more fabric tears in all endograft types, but particularly in PTFE grafts, and so should probably not be used for the in situ fenestration technique. Standard angioplasty balloons should be preferred, as the number of ruptured fibers is limited in comparison, and the risk of tear propagation should be reduced.
It seems the antegrade approach to in situ fenestration requires accurate positioning of the instruments used to ensure precise puncturing of the endograft, ideally, at a 90° angle to the graft. Modified needles have been used in many cases to perforate the endograft; these can be difficult to direct, especially through tortuous vessels. In addition, the thickness and durability of the stent-graft fabric would determine the deflection of the needle tip during puncture. The difficulties of attaining a 90° angle between the delivery sheath/catheter and graft body to deliver a stiff needle for graft puncture may be overcome using robotic catheter technology. The versatility of the robotic system, its precise positional orientation, minimum instrumentation of the vessel wall, and the ability to reproducibly and accurately return to sites of interest may facilitate in situ fenestration of aortic stent-grafts with minimal radiation exposure. 14
We have performed a series of in situ fenestrations in pigs using robotic techniques. Stent-graft puncture and target vessel cannulation with a guidewire were possible in 15/17 vessels attempted and subsequent branch-stent deployment was successful in 13/15 vessels. Other sophisticated endovascular tools, such as RF devices 13 and laser probes,10,11 have recently been tested as adjuncts to improve fenestration quality and stability during the in situ process. RF ablation catheters are capable of creating full-size circular fenestrations with fused edges. Laser technology is promising, especially with newer devices that burn a perfect circle through the wall of branch vessels using suction to hold onto the flap, preventing it from floating downstream; this technique is currently used for cerebral revascularization in neurosurgical procedures.22,23
Conclusion
The management of complex aortic pathologies remains a major challenge, particularly in the emergency setting. Extensive preoperative planning, cost of custom-made endografts, and the technical difficulties encountered in complex anatomical configurations hinder the wider applications of minimally invasive endovascular therapy. In situ fenestration is an attractive alternative and is clearly feasible. This study documents the variability of fenestrations that can be produced in some of the popular graft types and has shown that the angle and choice of angioplasty balloon for subsequent dilation of the hole is crucial for fashioning clean fenestrations without margin tears.
Footnotes
Acknowledgment
We would like to thank the companies who supplied the stent-grafts without cost for use in this study.