
Abstract
Purpose
To report early and midterm outcomes after open or endovascular repair of primary mycotic aortic aneurysms treated over a 10-year period in a single center.
Methods
The records of all 12 patients (10 men; 72.9 years, range 59–83) treated for primary mycotic aortic aneurysms from September 2001 to December 2010 were retrospectively reviewed. The aneurysms were located in the abdominal aorta in 10 cases and in the thoracic aorta in 2. Preoperative signs of infection, such as leukocytosis or elevated C-reactive protein, were found in all patients, and fever was apparent in 7. Three patients had primary open surgery with extensive debridement and extra-anatomical bypass, while 9 patients underwent endovascular aneurysm repair. At the time of operation, 10 mycotic aneurysms were already ruptured. All patients were prescribed lifelong antibiotics after discharge.
Results
Positive microbial cultures were found in 8 patients, including Salmonella species in 2, S. aureus in 3, E. coli in 1, and Streptococcus in 1. Mean follow-up was 29.9 months (range 1–98). Five patients took lifelong oral antibiotics after discharge with a mean medication duration of 17 months (range 1–65). Two of the 3 open surgery patients died (1 early). In the 9 endovascular repair patients, there was no early mortality, but 1 patient died at 6 months of an unknown cause. Additionally, 6 patients had a late relapse and underwent either secondary open surgical debridement (n=2) or computed tomography–guided drainage and antibiotic flush; 3 of the 6 died.
Conclusion
Endovascular aneurysm repair is a reasonable short-term management for patients with hemodynamic instability or high surgical risk. However, the late relapse rate after endovascular repair was very high in this series, despite adjunctive drainage and aggressive antibiotic treatment.
Keywords
Primary mycotic aortic aneurysm (PMAA) is a rare but life-threatening disease, comprising about 0.65% to 2% of all aortic aneurysms.1,2 The disease has a very poor prognosis because these aneurysms have a greater tendency to grow rapidly and to rupture. Also, patients with PMAA often have severe comorbidities and co-existing sepsis.3,4
See commentary page 311
Conventional open surgical treatment, which consists of a radical operation with resection of the aneurysm, extensive local debridement, and revascularization by in situ reconstruction or extra-anatomical bypass, is the gold standard but carries a high mortality due to the severe medical comorbidities, the magnitude of the surgery, and patient instability because of systemic sepsis or rupture.2,3 Endovascular aneurysm repair (EVAR) is a relative new modality for PMAA treatment, and compared with open repair, EVAR is less invasive and offers obvious advantages in terms of reduced perioperative morbidity and mortality in high-risk patients.5–8 However, a major disadvantage is that the infected tissue, including the aneurysm itself, is not resected, which may lead to recurrent sepsis and infection of the endoprosthesis.9,10
The aim of this study was to examine the contemporary management of PMAA, including open debridement and EVAR, in a single center over a 10-year period.
METHODS
Patient Population
A review was conducted of a prospectively maintained computerized database of all aneurysm patients at the Chinese PLA General Hospital between September 2001 and December 2010. During the period, 633 aortic aneurysms were treated, including 546 abdominal aortic aneurysms (AAA) and 87 thoracic aortic aneurysms (TAA). Among these patients, 12 (1.9%) with PMAA were identified (10 men; 72.9 years, range 59–83).
Patient demographics, medical history, symptoms, results of microbiologic cultures, aneurysm characteristics, treatment methods, early and late complications, and survival were recorded and are presented in the Table.
Demographics, Presentations, and Outcomes in 12 Patients Treated for Primary Mycotic Aortic Aneurysm
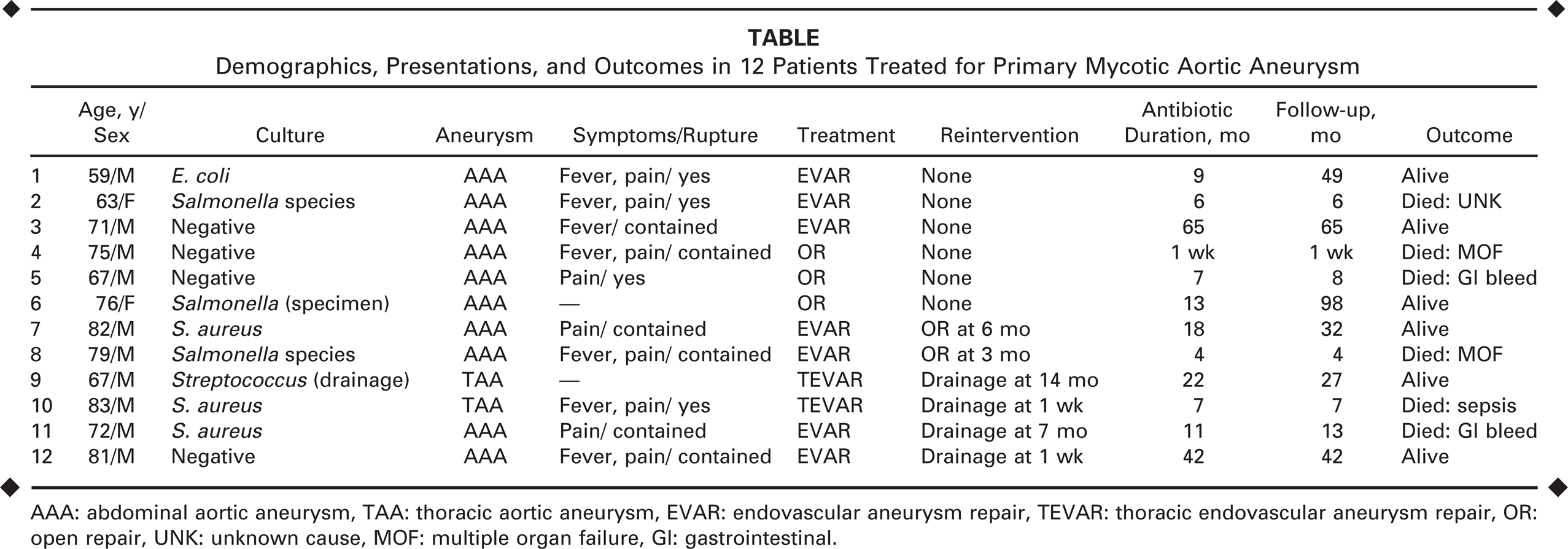
AAA: abdominal aortic aneurysm, TAA: thoracic aortic aneurysm, EVAR: endovascular aneurysm repair, TEVAR: thoracic endovascular aneurysm repair, OR: open repair, UNK: unknown cause, MOF: multiple organ failure, GI: gastrointestinal.
The aneurysms were located in the abdominal aorta in 10 cases and in thoracic aorta in 2. Comorbidities were prevalent and included hypertension (n=7), chronic obstructive pulmonary disease (n=5), coronary artery disease (n=7), diabetes mellitus (n=7), and a history of tobacco use (n=8). Two patients had previous vascular operations including femoropopliteal bypass with autogenic saphenous vein and prior aortic valve replacement.
The diagnosis of PMAA was based on a combination of clinical presentation, results of hematologic tests and cultures, and the presence on computed tomography (CT) of the saccular multi-lobular aneurysm, rapid expansion, peri-aortic gas within the aneurysm thrombus, or a soft tissue mass surrounding the non-dilated or aneurysmal aorta (often accompanied by a fractured, calcified atherosclerotic plaque).
All patients had elevated blood levels of inflammatory markers (leukocytosis and/or C-reactive protein) as well as the typical radiologic findings for PMAA. Seven patients had fever at presentation, and 6 had miscellaneous other symptoms, including weight loss, diarrhea, and dysphagia. At the time of operation, 4 cases were ruptured with hemodynamic instability; 6 patients had a contained rupture. Positive microbial cultures were identified in 8 patients, including Salmonella species in 3, S. aureus in 3, E. coli in 1, and Streptococcus in 1.
Medical Treatment
All patients were given antibiotics preoperatively and postoperatively, initially with broad-spectrum antibiotics intravenously and later guided by culture results, when available. Patients with negative cultures received broad-spectrum antibiotic therapy based on clinical suspicion of an infective agent. The preoperative antibiotic was given for at least 1 week if the patient's vital signs were stable and fever status was controlled. When discharged from the hospital, all patients were required to take lifelong oral antibiotics.
Surgical Treatment
Three AAA patients (4, 5, and 6 in the Table) had open surgery as the primary treatment. The procedure included extensive debridement of the infected aorta and extra-anatomical bilateral axillofemoral bypass with an 8-mm expanded polytetrafluoroethylene graft (W.L. Gore & Associates, Flagstaff, AZ, USA). Patient 4 had a juxtarenal AAA; both renal arteries had to be reconstructed with saphenous vein grafts due to the severe infection involving the proximal aorta. All the reconstructed vessels and aortic stump were covered with omentum as much as possible.
Endovascular Treatment
Nine patients had an endovascular repair as the primary treatment. Seven infrarenal AAAs were treated with a bifurcated Talent stent-graft (Medtronic, Santa Rosa, CA, USA; n=2), a bifurcated Zenith device (Cook, Bloomington, IN, USA; n=2), or a tubular Hercules stent-graft (Microport Medical, Shanghai, China; n=3). The 2 TAAs were treated with a Hercules tubular stent-graft.
When required in follow-up, CT-guided percutaneous drainage of the aneurysm sac was performed using a posterolateral approach. With the patient in the prone position, a 21-G Yeuh needle (Cook) was inserted into the aortic aneurysm sac, and a wire was then advanced. Following tract dilation, a 14-F locking-loop drainage catheter (Cook) was advanced and secured using sutures. Aspiration of the sac contents was sent for microbial analysis. The catheter was attached to a Jackson-Pratt drain for later antibiotic flush. For each patient, at least 2 catheters were placed in the aneurysm sac, one as the entry channel and the other as the exit channel for continuous flush. Perfusion was performed at least twice every day using at least 1000 mL of saline containing antibiotics each time.
Follow-up
Patients were reassessed postoperatively with a clinical examination, hematologic tests, and imaging at 1, 6, and 12 months, and then annually thereafter. Postoperative imaging was primarily performed with CT, but ultrasound imaging was sometimes substituted in infrarenal aneurysms.
RESULTS
Mean follow-up (from first operation until data were retrieved in October 2012) was 29.9 months (range 1–98). No patient was lost to follow-up. In this series, the 30-day mortality was 8% (1/12) and the late mortality was 50% (6/12). Among the 3 patients who underwent primary open surgery, 2 died. Patient 4 succumbed to multiorgan failure 1 week after the operation, while patient 5 expired 8 months after the operation from gastrointestinal bleeding, which was found at autopsy to be caused by an aortoenteric fistula.
Among the 9 patients who underwent endovascular repair, patient 2 died suddenly 6 months after the procedure of unknown causes. Four patients (patients 9–12) underwent CT-guided percutaneous drainage and antibiotic flush as described above (Fig. 1). Patients 9 and 11 received the drainage procedure for relapse, while patients 10 and 12 received the drainage prophylactically at 1 week after the repair. Patient 11 died 13 months later secondary to gastrointestinal bleeding, and patient 10 died 7 months later from uncontrolled sepsis.
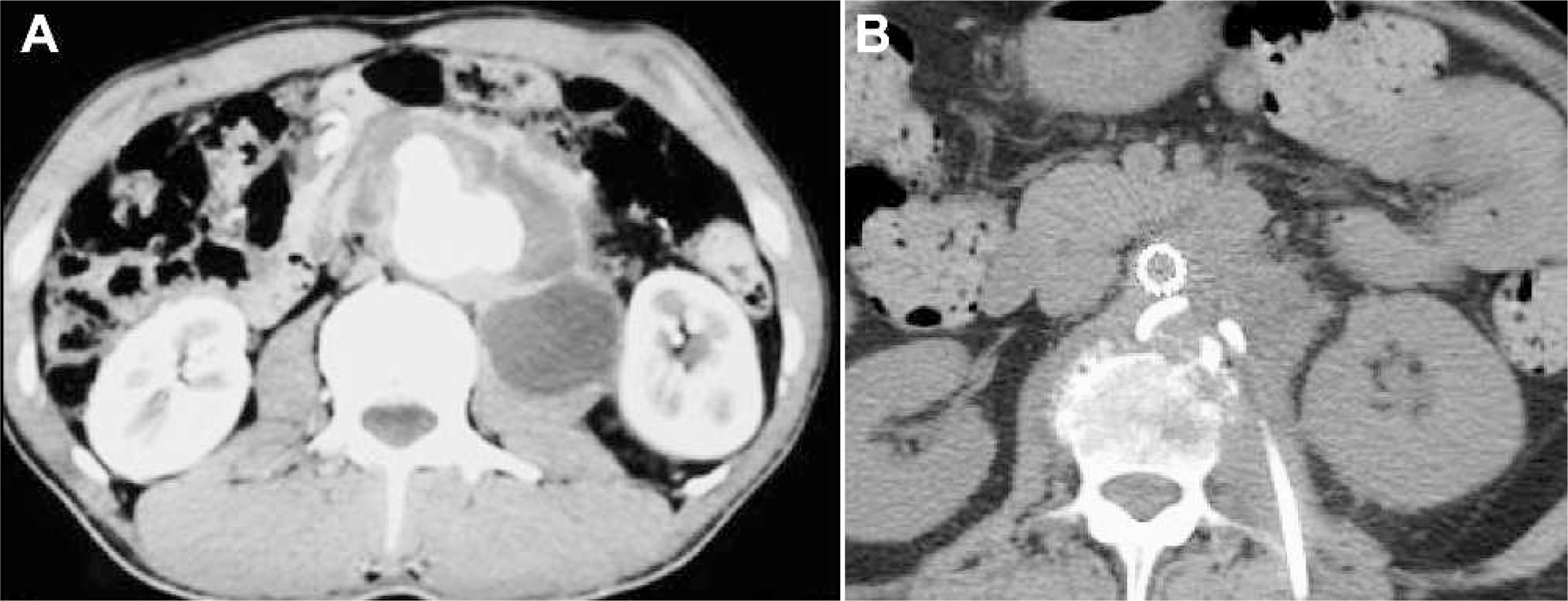
CT scans from patient 12 (
Patients 7 and 8 suffered from late relapse and underwent rigorous debridement of all infected tissue and explantation of the stent-grafts. In both cases, the suprarenal aorta was severely affected by infection, so the renal arteries were reconstructed using autogenic saphenous vein graft. The aorta and iliac arteries were reconstructed using polytetrafluoroethylene bifurcated graft intentionally placed in the right retroperitoneum (beneath the ascending colon) to stay away from the infectious area (Fig. 2). Patient 8 died within 30 days from multiorgan failure. Thus, the late mortality in this group was 44% (4/9).
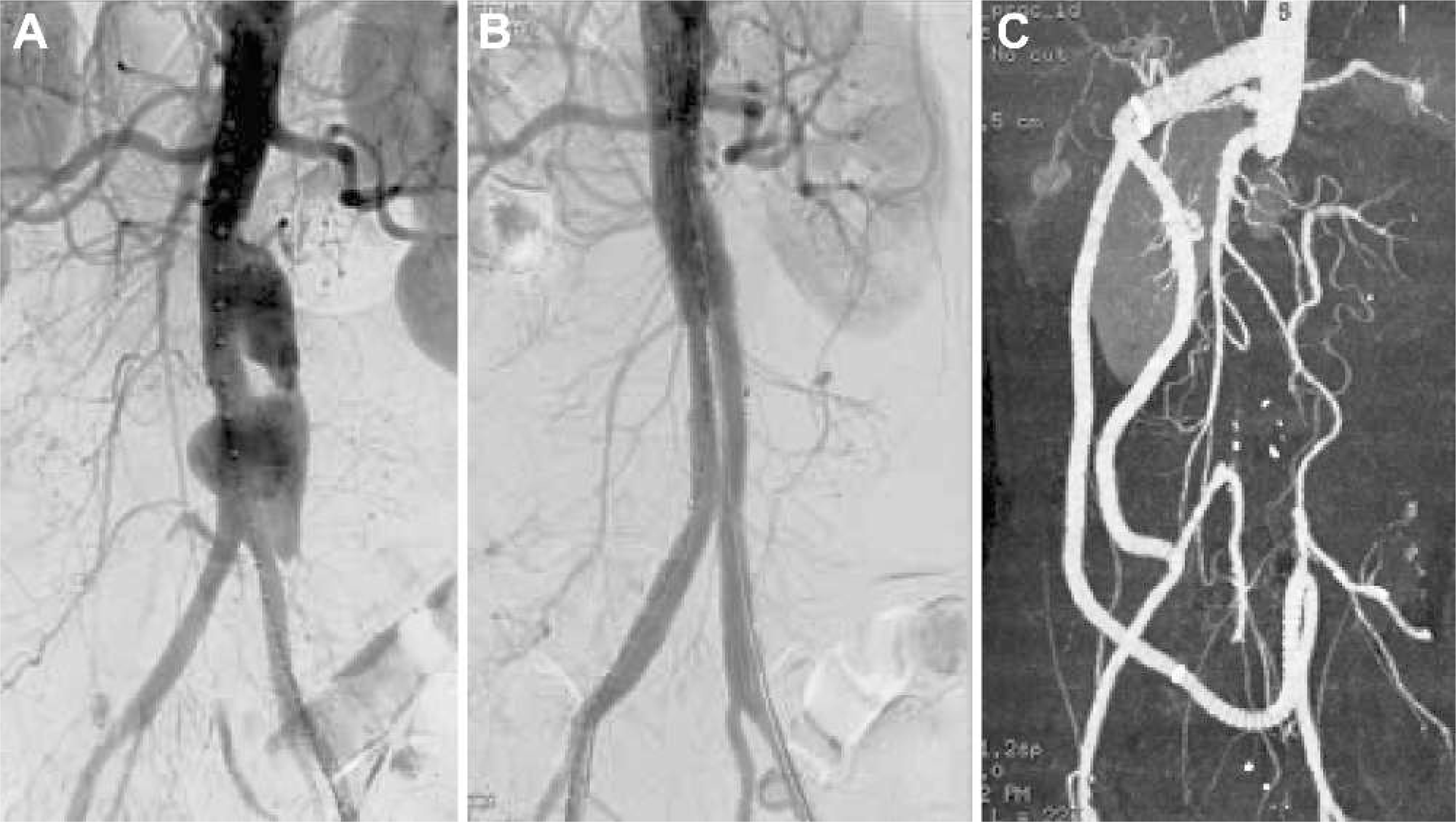
Angiography from patient 7 (
The mean duration of antibiotic therapy was 17 months (range 1–65); only 5 patients strictly complied with the medication protocol. Of these, patient 3 had intermittent fever and raised levels of inflammatory markers during follow-up but no other symptom. Patient 2 died suddenly of an unknown cause; patients 8 and 10 suffered relapse and expired later from complications. The mortality in this subgroup was 60% (3/5). In the 6 patients who stopped the medication automatically, patients 1 and 6 had elevated levels of inflammatory markers but were asymptomatic. Patient 5 died after open surgery 8 months later, and patient 11 relapsed, was treated, and expired. The mortality was 33% (2/6) in this subgroup.
Four of the 8 culture-positive patients expired, as did 2 of the 4 culture-negative patients. Autopsy was performed only in 2 cases owing to gastrointestinal bleeding and local culture and customs. In both cases, the autopsy proved that the cause of death was aortoenteric fistula. Postmortem tests for bacterial colonization of the endografts were not performed in these patients.
DISCUSSION
The most conservative treatment of PMAA consists of debridement of infected tissue; in situ or extra-anatomical bypass can be used depending on the severity of infection. In 1999, Soravia-Dumand et al. 2 put together one of the largest reviews involving 136 cases of PMAA treated over the prior 50 years. In 52 patients, treatment consisted of antibiotic therapy alone; the overall mortality was 96% vs. 38% in the other 84 patients who were treated with open surgery and antibiotics. However, treatment of aortic aneurysms has evolved over the past 2 decades, and EVAR has become the treatment of choice in many settings, including PMAA. In a systematic review of EVAR experience in PMAA, Kan et al. 11 analyzed 48 patients from 22 reports. The overall mortality was 25%: 10% 30-day and 15% late mortality over an average follow-up of 20 months.
Encouraged by the good results with the endovascular approach to treatment of PMAAs in the literature,11–14 we have changed the treatment protocols in our center. This study dated back to 2001 when we first established the patient database. In the next 10 years, only 12 cases of PMAA were identified, an incidence similar to the literature. Open debridement used to be our first choice for PMAA, and the postoperative results were sobering. In this series, 2 of 3 mycotic AAA patients who underwent primary open surgery expired. In comparison to the current literature, the mortality in our small series was higher than the reported rates of 11% to 36% and 17% to 58% for early and late death, respectively.1–4 One possible explanation was that our patients were older (median age 75 years), in severely poor condition, and had ruptured aneurysms.
In recent years, we chose EVAR for high-risk PMAA patients. Encouragingly, there was no perioperative mortality or severe complication in our endovascular group. However, the late mortality was 44%, which was also relatively high compared with the 20% to 50% range from the literature.11–13 This might be due to the high relapse rate (67%) after EVAR; 5 of the 6 relapses occurred within 7 months. Kan et al. 11 found that those PMAA patients with persistent infection had a 12-month mortality of 61%. One explanation for the high mortality in this series might be the low conformity of patients to the medication protocols. Although all the 11 patients who survived to discharge were required to take lifelong oral antibiotics, only 5 followed the prescription protocol strictly. However, the mortality in those who took lifelong oral antibiotics (60%, 3/5) was surprisingly higher than those who did not (33%, 2/6) in our series.
Aneurysm sac drainage after EVAR has been proposed by some authors to diminish the infectious content of the aneurysm sac and effectively prevent late relapse.6,7 Four of our EVAR patients had CT-guided percutaneous drainage and antibiotic flush (2 prophylactically), but there were still 2 late deaths. The possible reason could be that the remnant infection inside the sac could not be eliminated by regional drainage and flush; on these occasions, more extensive surgical debridement might still be the best solution to eradicate the infectious tissues. In our series, 2 patients underwent secondary open debridement. The one who did not survive was treated only after severe relapse; the final result might have been improved if the debridement was performed earlier when the patient was more stable and the infection was under control.
Conclusion
Comparing outcome results from PMAA treatment between EVAR and open surgery can be difficult due to the variability in presentation, etiology of infection, and comorbidities of the patients. Based on our single-center experience, the treatment protocol for PMAA should be individualized. EVAR is a reasonable short-term management technique for hemodynamically unstable patients with ruptured PMAA or those with high surgical risk. However, as seen in our series, the late relapse rate after EVAR was very high. Despite the adjunctive drainage and antibiotic flush, bacterial contamination of the aneurysm sac could be refractory and difficult to eradicate in some patients.