
Abstract
Purpose
To investigate serological predictors of risk for cerebral embolism after carotid artery stenting (CAS).
Methods
Twenty consecutive symptomatic and asymptomatic patients (13 men; mean age 74 years) with carotid artery stenosis undergoing standardized filter-protected CAS (Wallstent) were preoperatively evaluated to identify unstable plaque (duplex ultrasound), complicated aortic plaque (transesophageal echocardiography), and inflammatory status [high-sensitivity C-reactive protein (hs-CRP) and serum amyloid-A protein (SAA) serum levels]. Aortic arch type, carotid tortuosity, and complexity of the procedure were considered. Cerebral embolism was evaluated by comparing the number, volume, and side (ipsilateral and non-ipsilateral) of preoperative and postoperative cerebral lesions detected on diffusion-weighted resonance magnetic imaging (DW-MRI) and through light and scanning electron microscopy analysis of cerebral protection filters obtained from CAS.
Results
All CAS procedures were completed with no complications. All patients had a negative preoperative DW-MRI, but at least 1 asymptomatic cerebral lesion appeared on DW-MRI after the procedure in 18 (90%) patients. Female gender was associated with a higher number of cerebral lesions (18.2±10.9 vs. 8.3±8.8 for men, p=0.03). Carotid plaque morphology, supra-aortic vessel anatomy, and procedure complexity did not correlate with number or volume of new cerebral lesions. Complicated aortic plaque was associated with a higher volume of non-ipsilateral cerebral lesions than uncomplicated plaque (235.0±259.3 vs. 63.6±63.2 mm3, respectively; p=0.02). Hs-CRP ≥5 mg/L and SAA ≥10 mg/L were significantly associated with a higher number of new cerebral lesions [16.2±10.7 vs. 4.3±3.4 for hs-CRP <5 mg/L (p=0.02) and 14.8±10.3 vs. 2.8±3.4 for SAA <10 mg/L (p=0.006), respectively]. Hs-CRP ≥5 mg/L and SAA ≥10 mg/L also correlated with greater surface involvement by embolic materials in the protection filters at microscopic analysis [37.0% (5.1%) vs. 26.9% (2.5%) for hs-CRP <5 mg/L, p=0.004; 35.9% (13.5%) vs. 22.2% (6.9%) for SAA <10 mg/L, p=0.02].
Conclusion
In addition to female gender and the presence of complicated aortic plaque, inflammatory status can be a predictor of cerebral embolism in CAS.
Keywords
Carotid artery stenting (CAS) is a valid alternative to carotid endarterectomy in selected patients needing revascularization. 1 However, CAS is associated with higher cerebral embolic potential compared with endarterectomy due to several anatomical and technical factors: the presence of atherosclerotic plaque in the aortic arch, common carotid artery (CCA) tortuosity, the complexity of the procedures (predilation or multiple guide changes), and the carotid plaque structure.2–4 In addition to these, several serological markers of atherosclerotic instability, such as C-reactive protein (CRP) and serum amyloid A (SAA) protein,5,6 are considered potential risk factors for embolism in CAS.
See commentary page 695
The cerebral emboli in CAS can be assessed quite well using cerebral diffusion-weighted resonance magnetic imaging (DW-MRI), but there are no accepted methods for evaluating the nature of the embolic material. The cerebral protection filter used during CAS captures the embolic debris detached during the procedure; therefore, the analysis of its surface can be a useful indicator of emboli composition.7–9 Data on the association between the nature and amount of debris captured by the filter and new cerebral lesion detected by DW-MRI are sparse in the literature. The aim of the present study was to evaluate the relationships among clinical and anatomical characteristics, serum concentrations of CRP and SAA, composition of the embolic debris, and new cerebral lesion onset by DW-MRI.
METHODS
Study Design and Patients
Twenty consecutive patients (13 men; mean age 74 years) with carotid artery stenosis submitted to CAS from January to December 2011 in our institution were asked to participate in this prospective study, which was approved by the appropriate institutional review board. Exclusion criteria were preexisting inflammatory status (neoplasia, other inflammatory disease); carotid stenosis due to other than atherosclerosis; recent (<30 days) endovascular procedures or cardiovascular events in different anatomical regions; and refusal to participate in the study.
Clinical and anatomical characteristics were recorded in a database for statistical analysis. Relevant clinical characteristics considered in the analysis were hypertension (blood pressure >140/90 mmHg or under antihypertensive medication); dyslipidemia (total cholesterol >200 mg/dL, low density lipoprotein >120 mg/dL, or specific therapy); diabetes mellitus (under treatment with insulin or oral hypoglycemic drugs); and current smoking. Preoperative ischemic neurological symptoms were considered any hemispheric event (stroke, transient ischemic attack, amaurosis fugax) ipsilateral with the carotid stenosis occurring within 6 months before revascularization.
Anatomical characteristics were aortic arch type dichotomized as “simple” (type I or II) or “difficult” (type III and “bovine,” as described previously 10 ); CCA tortuosity (the sum of all CCA angles >150°) represented as the tortuosity index 3 (TI) >150°; carotid plaque echogenic structure evaluated as hypo-echogenic, iso-echogenic, or hyper-echogenic/calcified according to the Tromso classification 11 (types I, II, and III/IV), with “unstable” carotid plaques considered as type I and “stable” carotid plaques as types II, III, and IV.
Serological Evaluation
Blood samples were collected 24 hours prior to CAS and centrifuged at 1800 rpm for 10 minutes at room temperature. Serum high-sensitivity CRP (hs-CRP) and SAA levels were analyzed through nephelometric analysis (Immage Immunochemistry System; Beckman Coulter, Brea, CA, USA). Patients were divided into 2 groups based on a hs-CRP <5 or ≥5 mg/L. The 5-mg/L threshold was chosen because serum hs-CRP levels higher than this were previously associated with vulnerable inflammatory plaque at histological evaluation 5 and with complication risk during CAS. 12 A threshold of 10 mg/L was used for serum SAA levels according to the standard clinical reference range; higher values are associated to chronic inflammatory disease. 13
Transesophageal Echocardiography (TEE)
TEE aortic examinations were conducted 1 to 3 days before CAS using a Sonos 5500 sonograph (Hewlett-Packard, Philips, NJ, USA) with a multiplane transesophageal probe (patients received oropharyngeal local anesthetic and mild sedation with intravenous midazolam) as previously described. 10 Atherosclerotic plaques of the aortic arch seen at TEE were categorized as “complicated” when mobile debris or an endoluminal protrusion >0.5 mm was present; other types of plaque were considered “uncomplicated.”
CAS Procedure
All CAS procedures were performed by the same surgeon (G.F.) with an experience of >600 procedures, according to the European Society of Vascular Surgery guidelines. 14 The CAS procedure was conducted as described previously. 10 Briefly, patients were medicated with aspirin (100 mg/d) and clopidogrel (75 mg/d) for 3 days before the procedure. On the day of the procedure, they were taken to the angiographic suite, where local anesthesia was administered. Systemic unfractionated heparin was given to achieve an appropriate activated clotting time, and an 8-F introducer was placed via a groin access. CCA cannulation was achieved with 40° HS I or II catheters (Boston Scientific, Natick, MA, USA or Medtronic Cardiovascular, Santa Rosa, CA, USA) over a Terumo stiff guidewire (Terumo, Tokyo, Japan). When cannulation was not achievable by these means, several different alternative techniques were used (i.e., buddy wire, coaxial); such procedures were considered as “complex” for purposes of the analysis. Brachial or carotid access was not attempted in any case. Routine cerebral protection was provided by a Filterwire EZ (Boston Scientific); closed-cell stents (Wallstent, Boston Scientific) were used exclusively. Hemostasis at the access site was achieved with a vascular closure device (Angio-Seal; St. Jude Medical Inc., St. Paul, MN, USA) or manual and elastic groin compression.
Technical success was defined as the ability to treat the stenosis with <30% residual stenosis. Neurological outcome was evaluated both at the end of the procedure and in the following 24 hours by a neurologist according to the National Institutes of Health Stroke Scale and the modified Rankin scale. Clopidogrel therapy was maintained for 1 month.
Filter Evaluation
At the end of the CAS procedure, the filters were recovered, gently washed in physiological solution, and immediately fixed in 10% neutral buffered formalin (pH 6.9). Macro photographs of the entire device were taken under a stereomicroscope. The filter was cut into two equal areas for light microscopy and scanning electron microscopy (SEM) examination, as previously described. 15 Thirty fields per filter were digitalized and processed with ImageJ software ( http://rsb.info.nih.gov/ij/ ). The total area for each filter was 0.12 mm2 at magnification ×10. The membrane surface occupied by debris was expressed by the number of pores occluded by thromboembolic debris (minimum mean size of 40 μm) and presented as a percentage. Color images were converted to stacks composed of 6 fields each, transformed in montage, converted to 8-bit grayscale (0.41 pixel/μm). The boundary of the filters was delineated to calculate the total area for each stack (13.2 mm2), and then the lower and upper threshold values were set to obtain the percentage of the covered area.
SEM was performed to characterize the type of embolic debris adherent to the filter's inner surface and to confirm the results from the light microscopy analysis. Filters were embedded in ashless paper filters, washed with 0.15M phosphate buffer, and post-fixed in 1% osmium tetroxide for 15 minutes at room temperature. Then the filters were washed for 15 minutes in distilled water, dehydrated with graded steps of absolute ethanol, and dried with hexamethyldisilazene (Fluka, Steinheim, Germany) for 30 minutes at room temperature. The dried filters were accurately flattened and mounted on 0.5-inch aluminum stubs (Multilab, Surrey, UK), and sputter-coated with a 10-nm-thick layer of gold in a Balzers MED 010 sputtering device (FL 9496; Balzers Union, Furstenstum, Liechtenstein). The samples were observed using a Philips 505 Scanning Electron Microscope (Koninklijke Philips NV, Amsterdam, The Netherlands) at 15 kV. Images were processed with ImageJ.
DW-MRI Analysis
Scans were performed both 1 to 3 days before CAS and during the first 24 hours after the procedure using a 1.5T Signa Horizon LX whole-body scanner (GE Medical Systems, Milwaukee, WI, USA) with a quadrature birdcage headcoil. A fluid-attenuated inversion recovery (FLAIR) sequence was performed in the oblique-axial plane [8002-millisecond repetition time; 116-millisecond echo time; 2000-second inversion time; 24×24-cm field of view (FOV); 5-mm thickness; 0-mm inter-slice gap; 256×224-pixel matrix]. Axial DW images were obtained (5-mm thickness; 0-mm inter-slice gap) using a single-shot echo planar imaging (EPI) sequence (192×192-pixel matrix; 32×32-cm FOV; 3 next), as previously reported. 16 Inplane spatial resolution was 2.77 mm2. Diffusion encoding gradients were applied in 3 orthogonal directions, with gradient strength corresponding to b-values of 900 mm2/s. Images were additionally acquired without diffusion weighting (corresponding to b=0 mm2/s and exhibiting a T2-contrast).
Pre-CAS DW-MRI images were automatically mapped onto the post-CAS images by rigid body registration [flexible image registration toolbox (FLIRT) in the fMRIB (functional MRI of the brain) software library (FSL); Oxford Center for Functional MRI of the Brain, Oxford, UK 17 ]. Hyperintense lesions were visually identified on the post-CAS DW-MRI images and confirmed by the absence of hyperintensity on the corresponding pre-CAS DW-MRI images.
The volume and the number of lesions were assessed semi-automatically, with final revision by one of the specialized physicians involved in the study (C.T.). The volume of the lesions was quantified by defining a threshold for the difference between pre-CAS and post-CAS image intensities and counting the number of pixels where the difference was greater than this threshold. Classification of new brain lesions was based on the vascular territory in which they occurred. New lesions were defined “ipsilateral” if located in the hemisphere ipsilateral to the side of the treated carotid bifurcation or “non-ipsilateral” if located in the hemisphere contralateral to it, in the posterior territory, or in both the ipsilateral and contralateral hemispheres.
Endpoints and Statistical Analysis
The primary outcome of the present study was to evaluate the influence of the clinical (classical risk factors); anatomical (aortic arch type, TI >150°, and unstable carotid plaques); technical (complex procedures); and serological (hs-CRP ≥5 mg/L and SAA ≥10 mg/L) factors in the development of new cerebral lesions (in terms of number and volume) detected by DW-MRI after CAS. Moreover, any relationship between new cerebral lesions detected by DW-MRI after CAS and the percentage of embolic debris occluding the pores in the cerebral filter used during CAS was sought. A power calculation to determine the sample size needed to evaluate a significant difference between numbers of post-CAS cerebral lesions based on 2 groups of patients with high (10±5) or low (5±5) numbers of lesions returned a sample size of 18 patients. 18
Continuous variables were expressed as medians (interquartile range, IQR) and categorical variables by relative and absolute frequencies. Analyses of differences between 2 groups were performed with the Fisher exact test for categorical variables and the Mann-Whitney U test for continuous variables. The unadjusted odds ratios (OR) for new cerebral lesions at DW-MRI were evaluated in a regression analysis, arbitrarily setting the categorical response variable as “high (≥5) number” or “high (≥100.0 mm3) volume” of cerebral lesions. These thresholds were chosen on the basis of the upper IQR of these variables determined from a previous study (data not shown). 10
The independent influence of different variables on the total number and total volume of post-CAS cerebral lesions was investigated with a Kruskal-Wallis analysis of variance incorporating factors achieving p<0.20 in a univariate analysis. Differences were considered significant at p<0.05. Statistical tests were performed using SPSS 13.0 for Windows (IBM Corporation, Somers, NY, USA) and Prism 5 software (GraphPad Software, Inc., San Diego, CA, USA).
RESULTS
All procedures were technically successful, with no residual stenosis >30% and no death, procedure-related stroke, or other cerebral event. All patients had a negative preoperative DW-MRI, but at least 1 asymptomatic cerebral lesion appeared on DW-MRI after the procedure in 18 (90%) patients (Table 1). As shown in Tables 2 and 3, female gender was associated with a higher total number (p=0.03) and a greater total volume (p=0.03) of cerebral lesions on DW-MRI; the presence of a complicated aortic plaque was associated with a higher volume of non-ipsilateral cerebral lesions (p=0.02). Hs-CRP ≥5 mg/L and SAA ≥10 mg/L were associated with a higher number [total (p=0.02 and p=0.006, respectively); ipsilateral (p=0.003 and p=0.006, respectively); and non-ipsilateral (p=0.02 and p=0.007, respectively)] and volume [total (p=0.02 and p=0.01, respectively)] of postoperative cerebral DW-MRI lesions. No other clinical, anatomical, or technical characteristics were significantly associated with post-CAS cerebral lesions.
Patient Characteristics and Cerebral Lesions Detected After CAS
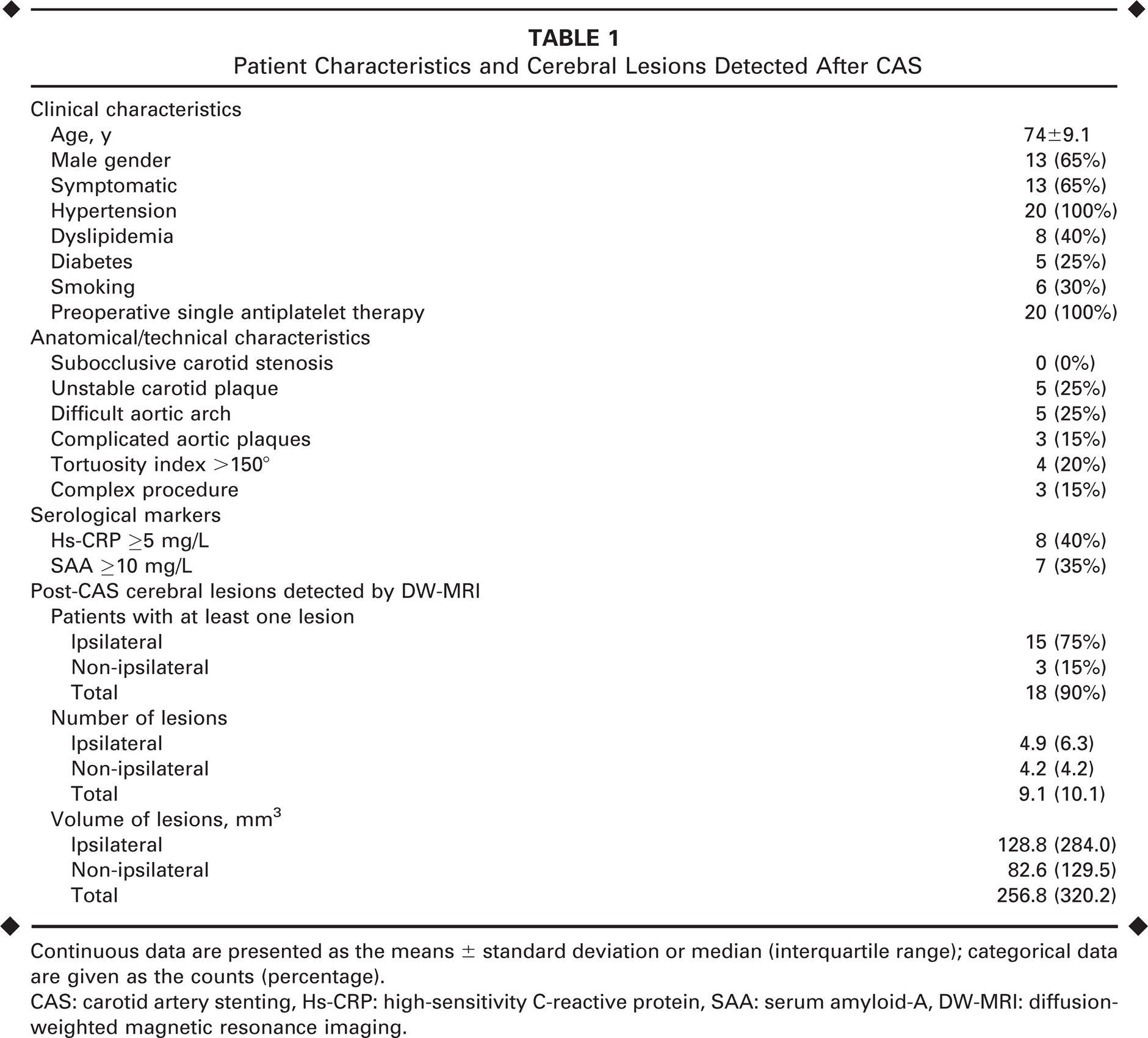
Continuous data are presented as the means ± standard deviation or median (interquartile range); categorical data are given as the counts (percentage).
CAS: carotid artery stenting, Hs-CRP: high-sensitivity C-reactive protein, SAA: serum amyloid-A, DW-MRI: diffusion-weighted magnetic resonance imaging.
Number of Post-CAS Cerebral Lesions in Relation to Clinical, Anatomical, Technical, and Serological Characteristics
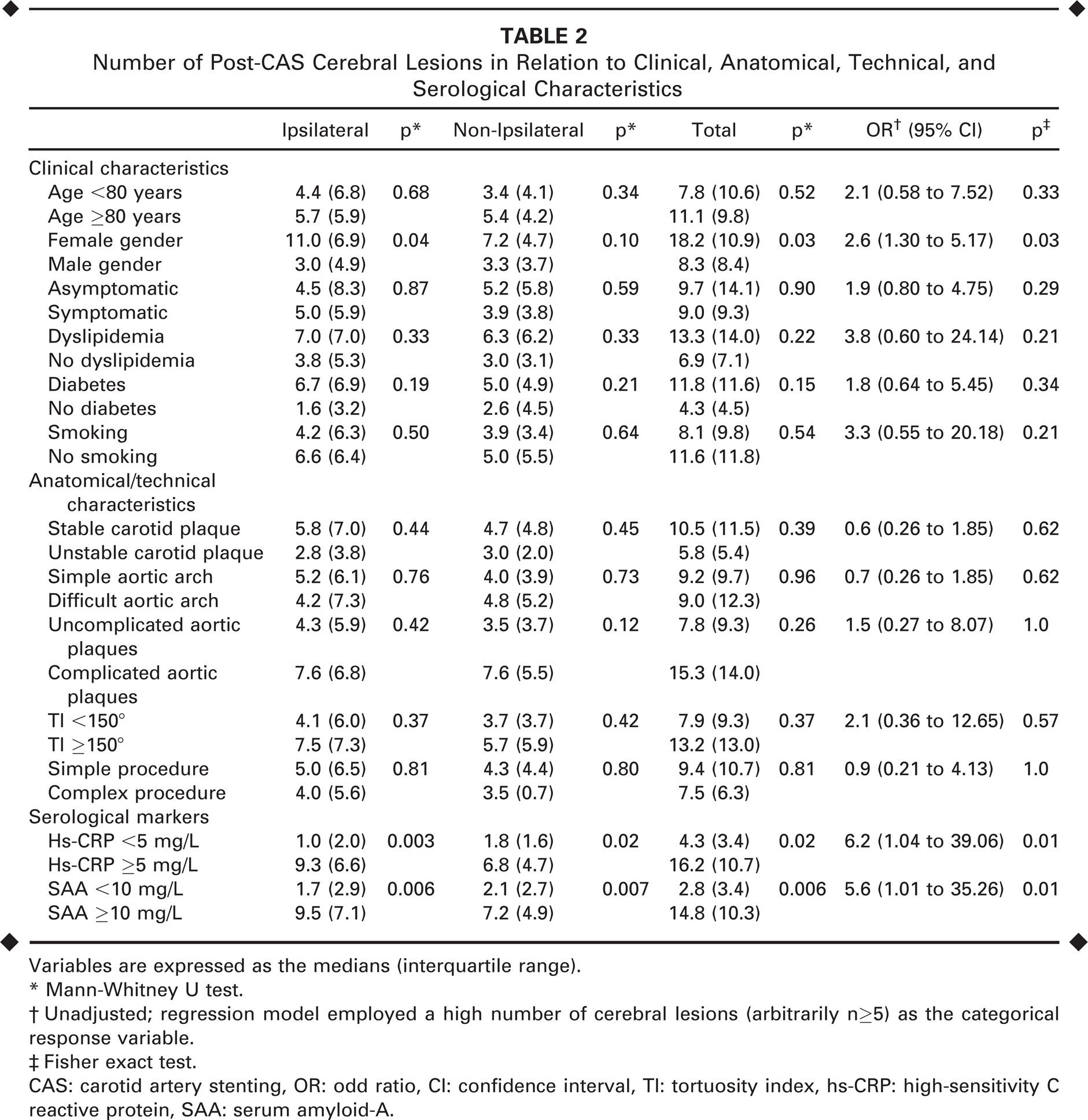
Variables are expressed as the medians (interquartile range).
Mann-Whitney U test.
Unadjusted; regression model employed a high number of cerebral lesions (arbitrarily n≥5) as the categorical response variable.
Fisher exact test.
CAS: carotid artery stenting, OR: odd ratio, CI: confidence interval, TI: tortuosity index, hs-CRP: high-sensitivity C reactive protein, SAA: serum amyloid-A.
Volume of Post-CAS Cerebral Lesions in Relation to Clinical, Anatomical, Technical, and Serological Characteristics
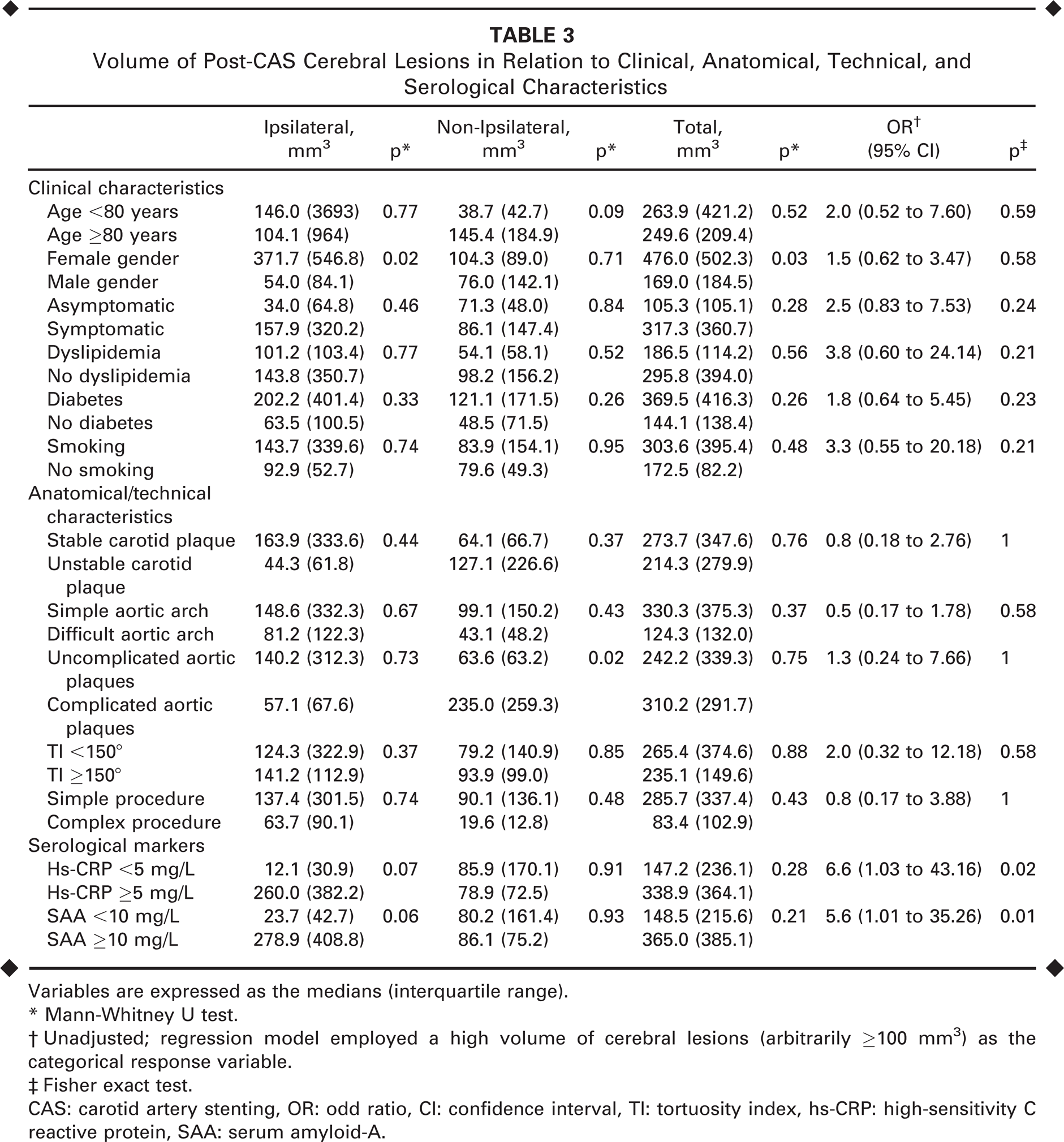
Variables are expressed as the medians (interquartile range).
Mann-Whitney U test.
Unadjusted; regression model employed a high volume of cerebral lesions (arbitrarily ≥100 mm3) as the categorical response variable.
Fisher exact test.
CAS: carotid artery stenting, OR: odd ratio, CI: confidence interval, Tl: tortuosity index, hs-CRP: high-sensitivity C reactive protein, SAA: serum amyloid-A.
The Kruskal-Wallis analysis evaluated interactions between new post-CAS lesions and hs-CRP ≥5 mg/L, SAA ≥10 mg/L, age ≥80 years, gender, symptomatic status, and complicated aortic plaques. The analysis showed significant correlations between hs-CRP ≥5 mg/L and the total number of cerebral lesions (p=0.04) and between female gender and the total volume of cerebral lesions (p=0.04); a relationship between hs-CRP ≥5 mg/L and total volume did not achieve significance (p=0.07).
All the cerebral protection filters retrieved were suitable for evaluation of surface involvement and showed a certain amount of debris captured. By SEM analysis, all filters were covered with an amorphous film, i.e., biofilm, of protein composition typical for all biomaterial. Pores of 100-μm diameter were occluded by clumps of red blood cells and embolic and plaque fragments. SEM (Figure) also revealed the presence of activated platelets with dendritic and spread morphologies.
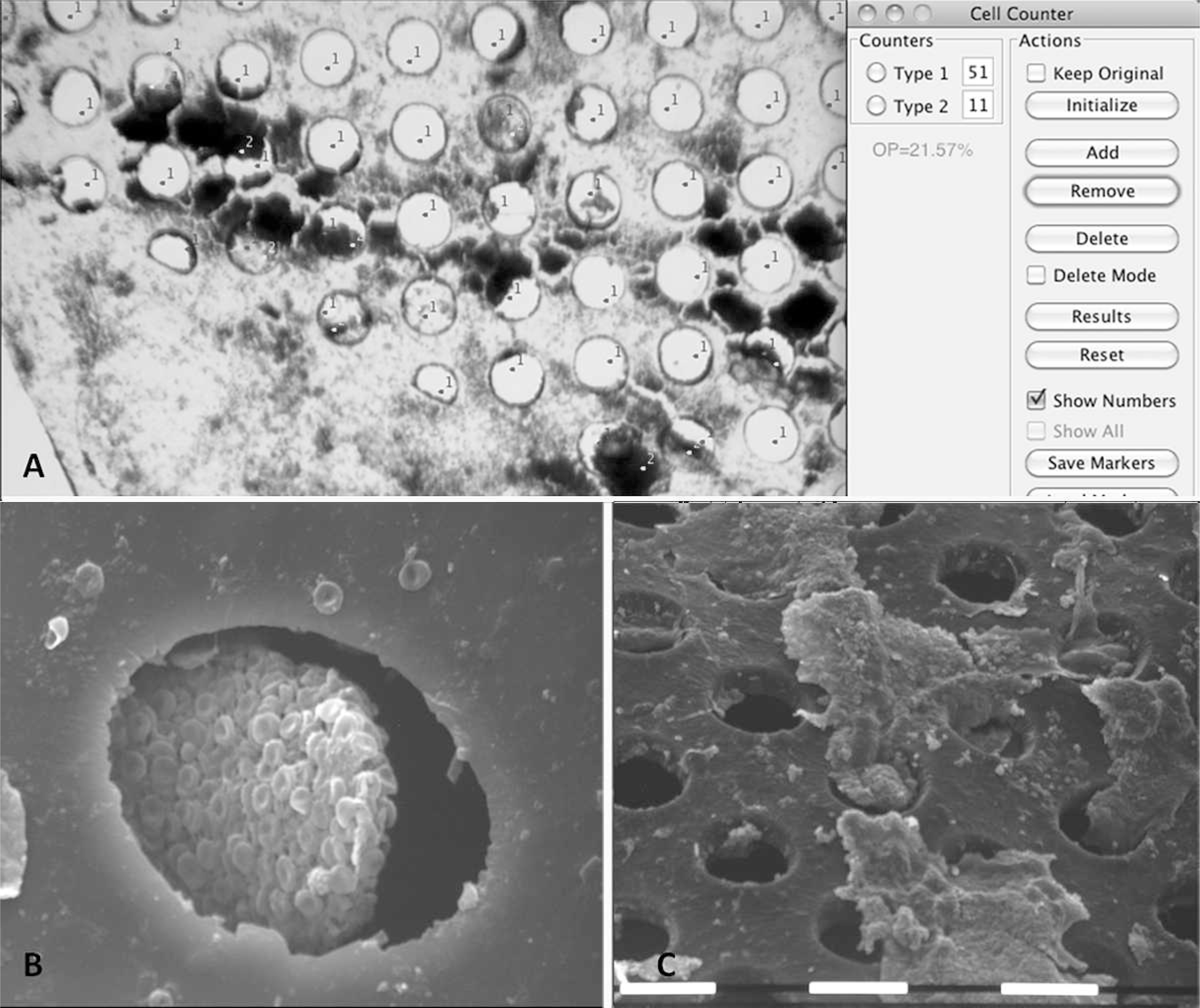
(
The correlation of percentage of filter pore occlusion and preoperative characteristics is shown in Table 4. High levels of hs-CRP and SAA were significantly associated with a higher filter surface involvement after CAS (p=0.004 and p=0.02, respectively). Greater percentages of pore occlusion were associated with a higher number of ipsilateral cerebral lesions at DW-MRI (p=0.02) but not with a difference in their volume (Table 5).
Comparison of Percentage Pore Occlusion in Cerebral Protection Filters After CAS
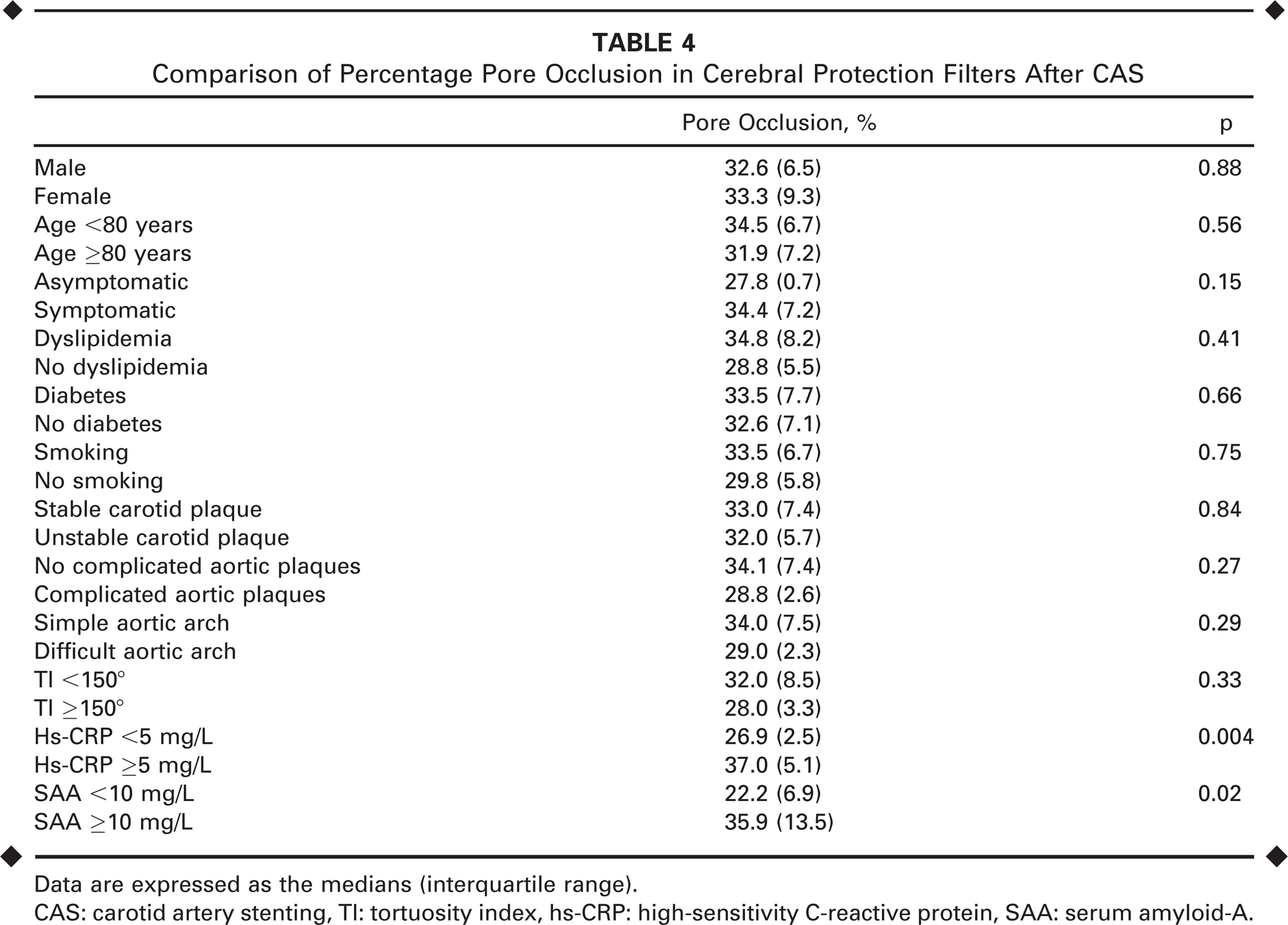
Data are expressed as the medians (interquartile range).
CAS: carotid artery stenting, TI: tortuosity index, hs-CRP: high-sensitivity C-reactive protein, SAA: serum amyloid-A.
Numbers and Volumes of Post-CAS Cerebral Lesions Detected at DW-MRI According to the Pore Occlusion Percentage
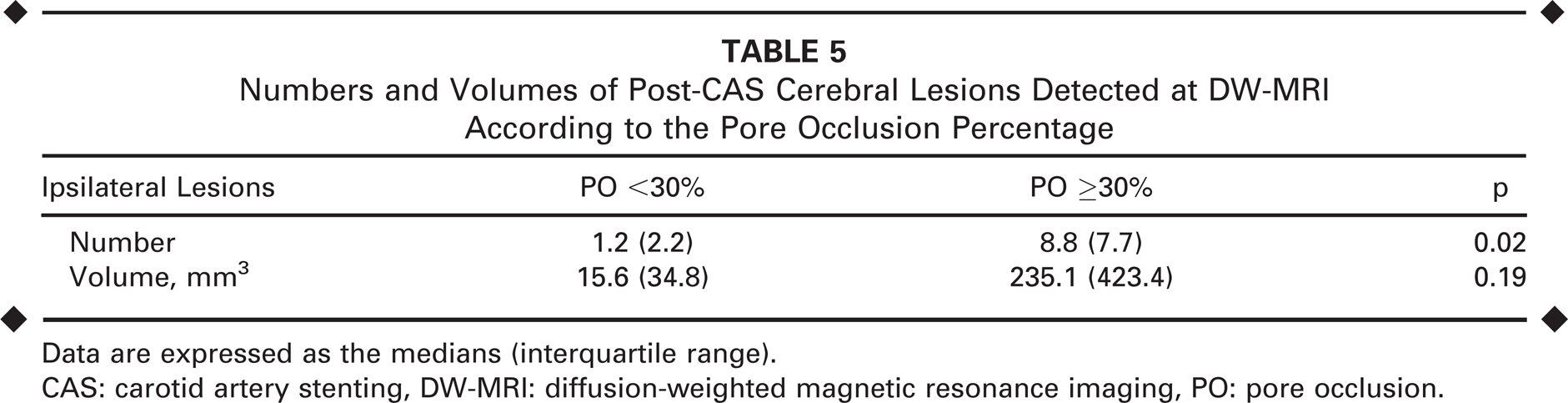
Data are expressed as the medians (interquartile range).
CAS: carotid artery stenting, DW-MRI: diffusion-weighted magnetic resonance imaging, PO: pore occlusion.
DISCUSSION
The present study confirmed that asymptomatic cerebral lesions are frequent after CAS, both in the ipsilateral (75%) and non-ipsilateral (15%) hemispheres. There are a number of variables associated with the onset of these lesions: female gender is correlated with a higher number and a greater volume of new cerebral lesions; presence of a complicated aortic plaque is related to a high volume of non-ipsilateral lesions, and the high levels of hs-CRP and SAA increase the risk of new lesion onset (number and volume) after CAS. Moreover, the hs-CRP level was independently associated with a high number of post-CAS cerebral lesions.
We have previously described that although tortuosity and difficult arch anatomy are risk factors for stroke in CAS, anatomical characteristics have a weak correlation with the onset of new asymptomatic cerebral lesions at DW-MRI. 10 Hs-CRP and SAA are serological inflammatory markers indicative of cardiovascular risk and are associated with a higher complication rate in a number of endovascular procedures. 6 In CAS they have been scarcely investigated. Only Groschel et al. 12 evaluated preoperative CRP levels and CAS outcome, resulting in an independent association between CRP levels >5 mg/L and the risk of postoperative stroke/death.
The association between CRP and SAA and cerebral microembolism during CAS has a possible biological background in the inflammatory status correlated with unstable atherosclerosis,19–22 since high serum CRP levels and leukocyte counts were associated with atherosclerotic plaque instability, a leading factor in plaque rupture and embolism.23–25 In the present study, female gender was a risk factor for new cerebral lesions on DW-MRI. This finding is consistent with the article by den Hartog et al., 26 wherein women had a higher risk for cerebral microembolization and neurological complications after carotid endarterectomy. However, other authors 27 did not confirm this association, so further studies are necessary on that matter.
The embolic lesions seen on DW-MRI are caused by fragmentation of the carotid plaque. The microscopic analysis of the debris captured in the CAS filters confirms their atherosclerotic nature. Most importantly, the clinical, anatomical, and technical factors examined were not correlated with filter involvement, meaning that the embolic material captured by filters occurs mainly as a consequence of carotid plaque disruption either during stent deployment or subsequent postdilation. Hs-CRP and SAA values were the only variables associated with the degree of filter surface involvement in our study. The fact that filters with higher surface involvement were significantly associated with more ipsilateral cerebral lesions (both number and volume) suggests that the function of these protection devices should be improved. Only a portion of the emboli released during CAS are captured by the filter, leaving pre and post filter deployment phases of the procedure vulnerable to embolic dispersal. In this study, only one kind of cerebral filter was used; however, different experiences have shown similar incidences of microembolization with other types of filter protection.9,28 The use of reverse flow balloon occlusion could be a valid alternative to reducing cerebral microembolization, but at present their use has not been shown to provide a significant reduction in the embolic potential in any of the CAS phases.29,30
Limitations
The sample size of this prospective study is small, which could have an effect on the analysis, specifically in the Kruskal-Wallis analysis. Also, the clinical influence of new post-CAS cerebral lesions detected on DW-MRI is doubtful, since no patient had clinical symptoms, even if the number and volume of the cerebral lesion was significant. While the microembolization seen on DW-MRI can be considered indicative of the overall embolic potential of the procedure, its clinical consequences are largely unknown. In the long term, cognitive decline or dementia is a possible effect. 31
Conclusion
The present work represents the completion of our studies in this area of interest. In our 2010 article, 10 the analysis of the anatomical characteristics of 59 patients and the onset of post-CAS cerebral lesions showed no influence of any single anatomical characteristic on new lesion occurrence. A subsequent preliminary study 15 on the embolic potential associated with high levels of hs-CRP in CAS patients found that this marker was significantly associated with the amount of embolic debris captured by the filters. The present study confirms the hypothesis regarding the influence of the inflammatory status, as represented by these evaluable serological markers, on the cerebral embolic potential of CAS.