
Abstract
Purpose
To describe an innovative technique to occlude distal backflow into a false lumen aneurysm by controlled rupture of the dissection membrane after stent-graft implantation.
Technique
The “Knickerbocker technique” involves relining the true lumen in the descending aorta with an oversized thoracic tubular endograft, followed by controlled rupture of the dissection membrane using a large compliant balloon within the graft's midsection. This maneuver, which allows expansion of the stent-graft's midsection into the false lumen, was developed in order to occlude the large false lumen distally and thus prevent continued false lumen perfusion through distal abdominal entry tears. The technique has been successfully used in 3 patients with ruptured or symptomatic chronic false lumen aneurysm in type B aortic dissection. There was no short-term mortality associated with the procedure. After a mean follow-up of 8 months, the false lumen aneurysm remained thrombosed, with no mortality after a mean clinical follow-up of 22 months.
Conclusion
The Knickerbocker technique appears to be feasible and effective in inducing false lumen thrombosis in selected patients who undergo stent-grafting for chronic type B aortic dissection.
Keywords
Since its introduction in 1999, 1 thoracic endovascular aortic repair (TEVAR) has become the mainstay of operative treatment for complicated type B aortic dissection, offering clear benefits of lower mortality and morbidity compared to open surgical repair.2–4 TEVAR in aortic dissection is based on the implantation of tubular thoracic stent-grafts to cover the proximal entry tear and thereby redirect flow into the true lumen. 2 Although this strategy can depressurize the false lumen and promote false lumen thrombosis and aortic remodeling in the majority of acute aortic dissections,2,5 the response is limited in chronic dissections, which have a reduced capacity for remodeling due to the thickened and fibrotic degenerated intimal flap.5,6 This limited response to endovascular treatment in chronic aortic dissection is caused by the continued pressurization from persistent retrograde false lumen flow to the intercostal and bronchial arteries from downstream entry tears. 7 Retrograde filling and pressurization leads to late aortic expansion in 35% of patients treated with TEVAR for chronic type B dissection. 8 The lack of aortic remodeling and development of a false lumen aneurysm due to continued perfusion causes late death, as Mani et al. 9 have recently shown. In patients with ruptured chronic false lumen aneurysm after aortic dissection, the persistent retrograde filling may lead to continued bleeding despite TEVAR down to the celiac artery to cover the descending aortic entry tears.
We describe a novel technique of paving the descending thoracic aorta with an oversized stent-graft in the true lumen and tearing the dissection membrane to expand the graft into the false lumen and prevent retrograde flow into the thoracic false lumen. This technique has been developed to prevent further bleeding in ruptured chronic aortic dissection and prevent late aortic expansion in non-ruptured chronic aortic dissection. The resulting shape of the stent-graft is similar to Knickerbocker trousers, after which it was named. We describe the technique and our initial experience in 3 patients with ruptured or symptomatic chronic false lumen aneurysm.
TECHNIQUE
The technique is illustrated in a type B aortic dissection with a large proximal entry tear (Fig. 1A). All procedures were performed in a hybrid operating room with a fixed imaging system under general anesthesia and systemic heparinization (50 U/kg). Following bilateral percutaneous femoral access, the true lumen was catheterized under repeat angiography to ensure true lumen position, then an extra-stiff Lunderquist wire (Cook Medical, Bjaeverskov, Denmark) was positioned in the ascending aorta. A proximal thoracic endograft ∼150 mm long was deployed in the true lumen covering the ostium of the left subclavian artery (LSA) and extending into the thoracic aorta (Fig. 1B) to occlude the proximal entry tear and redirect flow into the true lumen. Coverage of the true lumen was distally extended to the level of the celiac artery (Fig. 1C) using an oversized stent-graft with a diameter sufficient to cover the complete aortic diameter according to pre-procedure planning; the presence of such a landing zone is a prerequisite for treatment with this technique. A large compliant balloon (40-mm Coda; Cook Medical) was delivered to the midsection of the oversized distal stent-graft and inflated with up to 90 mL of dilute contrast until the dissection membrane ruptured and the stent-graft expanded into the false lumen (Fig. 1D) to occlude distal backflow (Fig. 1E), preventing bleeding in the setting of ruptured false lumen aneurysm. A chest tube is inserted if required.
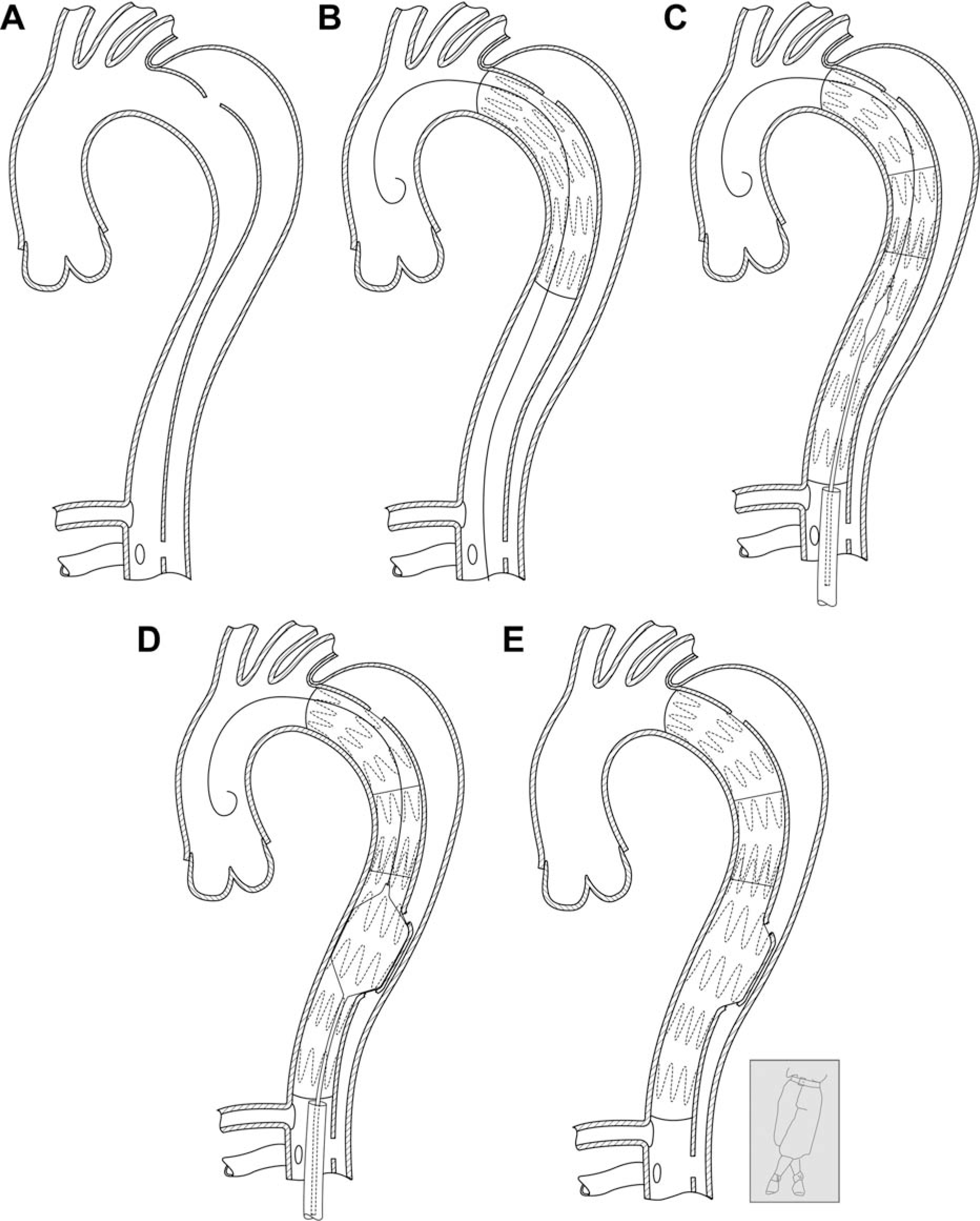
Illustration of the Knickerbocker technique in a (
The technique was first used when treating a 39-year-old morbidly obese patient with chronic type B aortic dissection who presented with a ruptured 12-cm false lumen aneurysm. Emergency TEVAR was performed with proximal deployment of a 42×216-mm Zenith TX2 ProForm (Cook Medical) covering the LSA followed by extension to the level of the celiac artery with a 46×209-mm Relay NBS thoracic endograft (Bolton Medical, Barcelona, Spain). Computed tomographic angiography (CTA) on the first postoperative day showed continued false lumen perfusion and an open LSA. After initial stabilization, the patient started bleeding from the pleural drain and was taken to the hybrid operating room. DSA showed massive distal false lumen backflow into the ruptured false lumen aneurysm. A 16-mm Amplatzer vascular plug II (AGA Medical Corporation, Plymouth, MN, USA) was placed in the proximal LSA and a 40-mm Coda balloon (Cook Medical) was used to dilate the midsection of the previously deployed distal 46-mm endograft, which had expanded to only 40 mm measured on CTA. The balloon maneuver opened the endograft to its full diameter at its midsection, with a rapid diameter “jump,” suggesting the dissection membrane had been ruptured. Digital subtraction angiography (DSA) showed no further backflow into the false lumen with patent visceral arteries. The patient became hemodynamically stable, and no further bleeding was noted from the thoracic tube. The patient made a slow recovery due to acute on chronic renal failure requiring hemodialysis and was transferred to a rehabilitation unit 4 weeks later. He was discharged home 10 weeks after the initial procedure with chronic renal failure but was mobile and self-caring. At 36 months postoperatively, the patient is clinically well but refuses a follow-up CT.
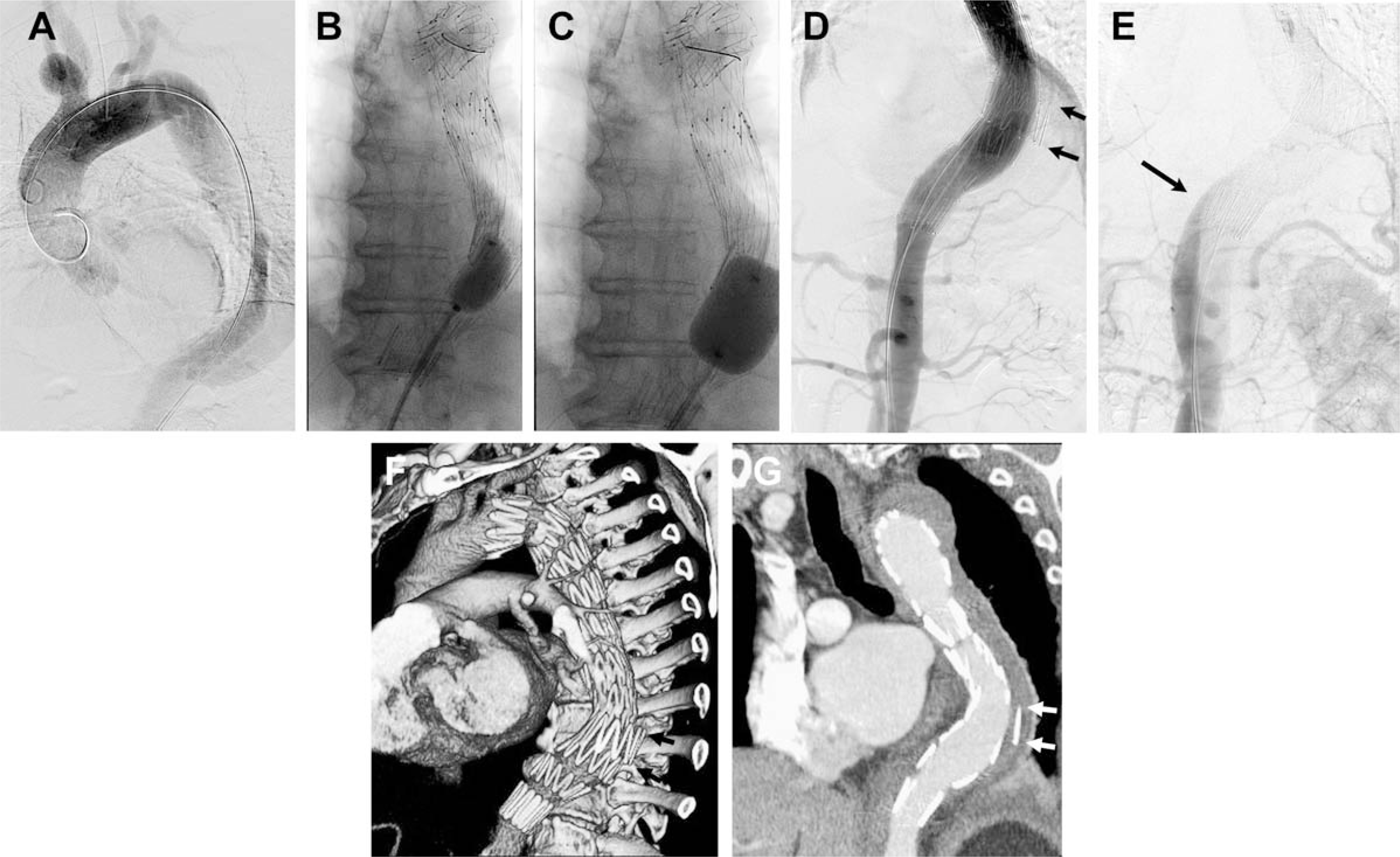
In the second case, a 77-year-old man with a medical history of hypertension, stroke, aortic and mitral valve insufficiency, and atrial fibrillation was treated conservatively with antihypertensive therapy for an acute type B aortic dissection. Six weeks after the initial dissection, he complained of chest pain. CTA showed rapid expansion of the aortic diameter from an initial 4.2-cm diameter at presentation to 5.3 cm and persistent false lumen perfusion. He was treated by TEVAR with two Zenith TX2 ProForm stent-grafts (Cook Medical) measuring 38×202 mm for the proximal device and 42×158 mm for the distal stent-graft. The Knickerbocker technique was used to completely cover the false lumen at the site of the torn dissection membrane (Fig. 2A–E). The postoperative course was uneventful, and the patient was discharged home on the 8th postoperative day. Initial CTA on postoperative day 4 and at 3 weeks (Fig. 2F,G) showed complete sealing of the expanded graft with false lumen thrombosis. Follow-up CTA at 16 months showed complete regression of the false lumen aneurysm over the entire length of the covered aorta. The patient is doing well 24 months after the initial procedure.
(
In the third case, a 65-year-old woman was transferred to our service because of a ruptured chronic thoracic false lumen aneurysm with bilateral paraplegia. She had a history of type A dissection, which was managed with an ascending and hemi-arch repair 13 months earlier; this procedure was complicated by a stroke with left-sided hemiplegia. Two months following the initial procedure, she underwent TEVAR covering the LSA down to the mid descending thoracic aorta. At the admission for rupture, a Zenith TX2 ProForm stent-graft (Cook Medical) measuring 42×216 mm was deployed from the previous stent-graft to the celiac artery. The Knickerbocker technique was used to successfully occlude flow in the thoracic false lumen. Postoperative CTA at 6 months confirmed complete thrombosis of the proximal false lumen and no further bleeding.
DISCUSSION
In chronic aortic dissection, TEVAR aims to reduce or abolish flow in the false lumen and prevent aorta-related death. TEVAR is technically feasible and associated with low perioperative morbidity and mortality. However, there are serious concerns about the efficacy of TEVAR in managing chronic aortic dissections both in the short and long-term. The key problem is poor remodeling of the chronically dissected aorta following endovascular therapy due to a fibrotic and stiff dissection flap. A significant proportion of patients have persistent and significant false lumen flow even after long lengths of the thoracic aorta have been covered with a stent-graft. 10 Large reentry tears at the level of the visceral aorta (or further distally) are particularly responsible for persistent false lumen flow.
The technique described herein was developed to occlude false lumen flow that could be associated with significant early complications, particularly in patients who receive a stent-graft for a ruptured thoracic aorta due to a chronic dissection. Roselli et al. 11 described a surgical technique to prevent distal false lumen flow. Twenty-four patients with type A aortic dissection received a proximal elephant trunk arch repair and a fenestration of the distal landing zone through a sternotomy to create a non-dissected aortic segment in the distal descending aorta. In a second procedure, TEVAR was performed landing the distal end of a stent-graft in the fenestrated segment, where seal could be achieved by expansion into the false lumen, abolishing backflow. Konings et al. 12 described a similar technique to create distal seal in the supraceliac aorta using a subxiphoid incision for open fenestration in one patient with chronic type B aortic dissection. Both strategies efficiently address the problem of false lumen flow by creating an aortic segment in which the stent-graft can open into the false lumen and thereby occlude it. The disadvantage of both strategies is that they require open surgery and aortic cross clamping.
Seal of the distal false lumen can also be achieved by endovascular techniques, such as fenestrated stent-grafts that can cover an even longer segment of the aorta to occlude more distal entries13,14 or by deployment of large vascular plugs, coils, or glue into the false lumen.15,16 The Knickerbocker technique allows for immediate distal false lumen occlusion in patients with chronic aortic dissection and favorable anatomy. Although balloon dilation appears counterintuitive and is generally not recommended in aortic dissection because of the risk for rupture and bleeding, the Knickerbocker technique was safe in the 3 cases treated so far.
Another significant difference between the Knickerbocker technique and the other methods11,12 is that the open fenestration techniques direct blood flow into both lumens distal to the stent-graft due to landing in the fenestrated segment. There is therefore a risk of distal false lumen aneurysm and branch vessel ischemia. The Knickerbocker technique aims to confine the distal stent-graft opening to only the true lumen to direct the blood flow into it. This strategy of landing the distal end of the stent-graft in the true lumen only could easily be transferred to the techniques of Roselli 11 and Konings 12 by creating the fenestrated segment a distance above the celiac artery and then landing distally to this fenestrated segment.
In our experience, balloon dilation to rupture the dissection membrane was not complicated. Alternatively, a fenestrated segment can be created by endovascular techniques prior to deployment of the oversized graft. Potential limitations of the described technique include the risk of aortic perforation and hemorrhage, subsequent dilatation, and further disruption of the dissection flap due to significant oversizing of the stent-graft. Moreover, the Knickerbocker technique does not prevent further distal false lumen perfusion in the visceral and infrarenal aortic segment.
Conclusion
The Knickerbocker technique appeared to induce false lumen thrombosis in these few selected patients who had undergone stent-grafting of chronic type B aortic dissection with complications due to false lumen backflow. Whether intentional oversizing of the stent-graft in the distal true lumen is acceptable and will be tolerated remains unclear. Future endografts designed for the Knickerbocker technique may include a tapered or double-tapered configuration to address this issue. Further studies are required to confirm whether these results can be replicated and to ensure the durability of false lumen thrombosis.