
Abstract
Purpose
To examine long-term survival and freedom from reintervention after endovascular treatment of patients with isolated abdominal aortic dissections (IAAD).
Methods
A retrospective review was conducted of 21 patients (18 men; mean age 72±18 years, range 34–90) with an IAAD who underwent endovascular treatment between January 2000 and December 2012. Fourteen patients had spontaneous abdominal dissections, while 7 dissections were iatrogenic in origin. Thirteen patients with symptomatic acute (n=9) or subacute (n=4) lesions underwent analgesic therapy and medical management of systolic blood pressure for at least 5 days; persistent pain was an indication for endovascular treatment. Eight patients with chronic dissections were treated by endovascular means for co-existent (1) abdominal aortic aneurysm (AAA) that was >5 cm in diameter or had expanded >5 mm in 6 months (n=6) or (2) rupture-threatening penetrating aortic ulcer (PAU, n=2) even with a diameter <5 cm. Mean dissection length was 45±12 mm (range 18–98). Ten patients received tube stent-grafts, 9 had bifurcated endografts, one had an aortouni-iliac (AUI) endoprosthesis, and one patient was treated with a bare metal stent. Follow-up included computed tomographic angiography within 1 month postoperatively, duplex ultrasound at 3 and 6 months, CTA at 12 months, and then annual duplex scans.
Results
Early (30-day) mortality was 0%; no major adverse events occurred during hospitalization. Patients with co-existent AAA/PAU had complete exclusion of the aneurysm sac. The patient with an AUI graft suffered from an early stent-graft thrombosis in the abdominal aorta; flow was restored after transfemoral thrombectomy and balloon angioplasty of the common iliac artery. During a mean 73±22-month follow-up (range 19–144), 3 patients died due to unrelated causes (95% survival at a median 67 months estimated by Kaplan-Meier analysis). All patients showed full aortic remodeling over a period of 12 years. One patient with AAA underwent surgical conversion due to persistent type II endoleak (95% freedom from reintervention at a median 67 months).
Conclusion
In this series, long-term evaluation of endovascular IAAD treatment found no mortality, few complications, and rare need for secondary interventions.
Keywords
Aortic dissection involving only the abdominal aorta is a rare clinical entity, with an incidence of between 1% and 4% of all dissections in the entire aorta.1–6 The literature lacks evidence for the treatment of choice and consists mainly of small patient series. In 2009, Jonker et al. 1 conducted a review and meta-analysis of the published clinical experience consisting of 92 patients with isolated abdominal aortic dissections (IAAD). The majority of the patients were treated conservatively (27, 29%) or with conventional surgical techniques (46, 50%). Endovascular repair was performed in only 19 (21%) patients using a plethora of different stents, stent-grafts, and balloons. The heterogeneity of the series, the short-term follow-up, and the small number of treated patients did not support robust conclusions about the best therapeutic strategy for abdominal dissections.
See commentary page 329
The aim of the present study was to evaluate the utility of the less invasive catheter-based approach based on long-term outcomes of a single-center experience.
METHODS
Between January 2000 and December 2012, 2472 patients underwent endovascular stent-graft placement in the descending thoracic, visceral, and abdominal aorta at our large tertiary care center. Among them, 21 (0.8%) patients (18 men; mean age 72±18 years, range 34–90) who underwent endovascular repair of an IAAD were retrospectively evaluated. In the same period, one IAAD patient was treated surgically in 2000 before endovascular techniques were sufficiently developed to deal with his complex dissection, which involved one renal and both iliac arteries. His case was excluded from this analysis. Also in the same 12-year interval, 326 patients were diagnosed with a thoracic dissection; 199 underwent endovascular treatment.
In the IAAD cohort (Table), the lesion was localized at the level of the abdominal aorta without retrograde extension to the thoracic aorta (Fig. 1). Mean dissection length was 45±12 mm (range 18–98). More than 50% of the lesions (n=11) were detected between the renal arteries and the aortic bifurcation without involvement of the iliac arteries. The mean length between the origin of the dissection and the lowest renal artery or the aortic bifurcation was 1.9±0.3 mm and 0.5±0.2 mm, respectively. The remaining 10 cases involved the iliac arteries.
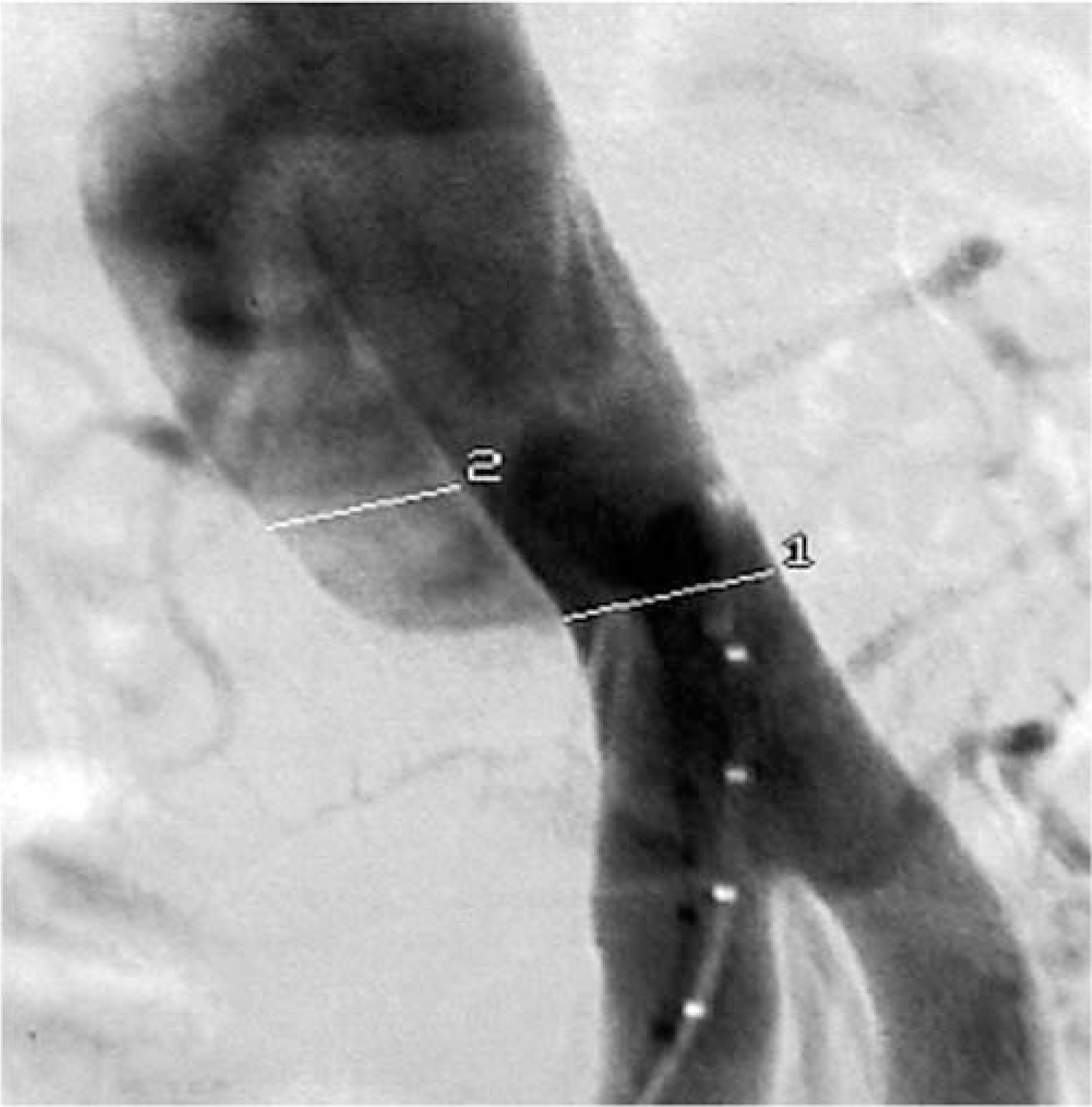
Intraoperative angiography of an infrarenal abdominal aortic dissection; 1 indicates the true lumen and 2 the false lumen.
Demographics and Characteristics of the 21 Study Patients
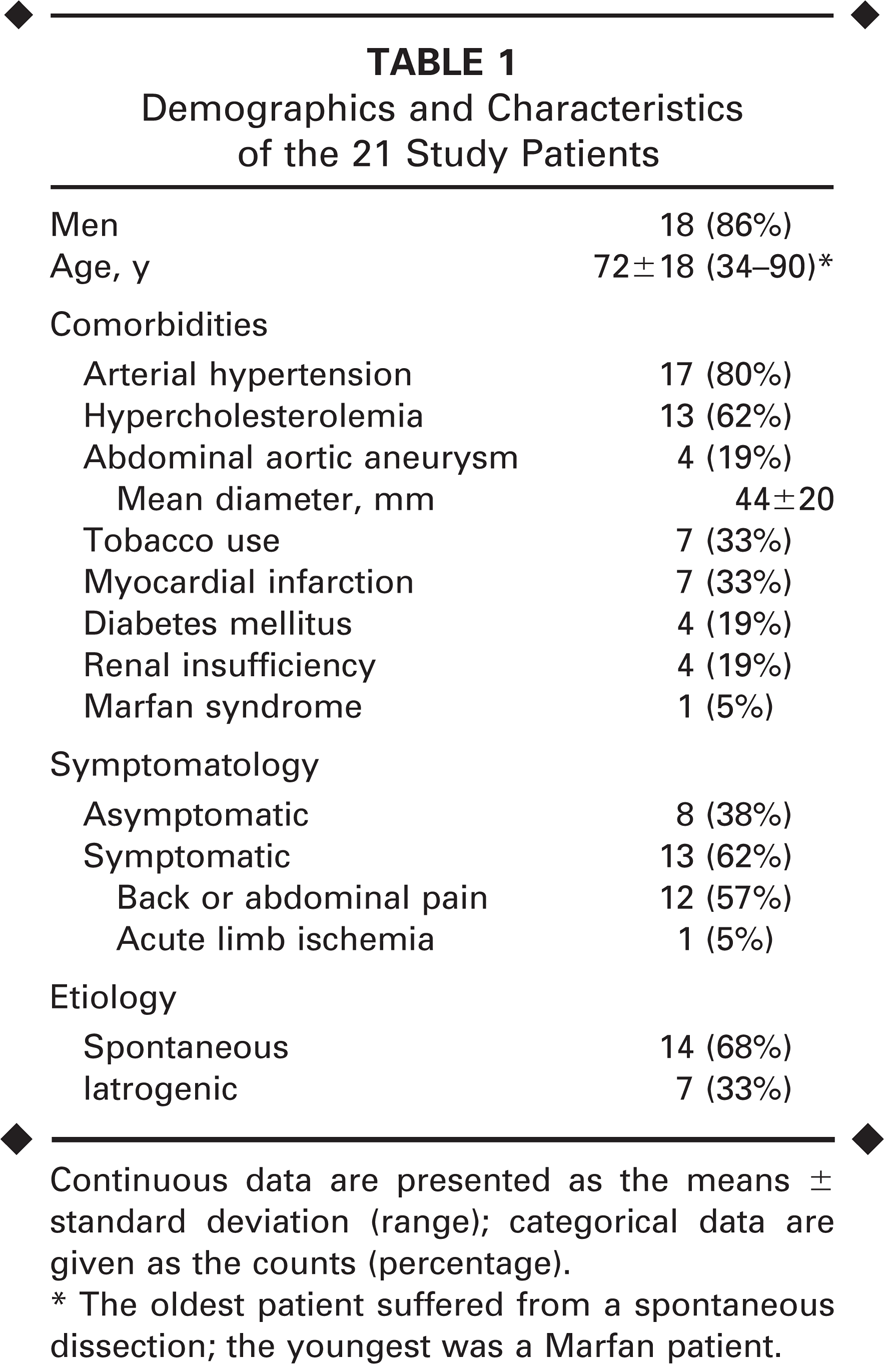
Continuous data are presented as the means ± standard deviation (range); categorical data are given as the counts (percentage).
The oldest patient suffered from a spontaneous dissection; the youngest was a Marfan patient.
The majority of abdominal dissections occurred spontaneously (n=14), while 7 dissections had an iatrogenic etiology (previous cardiac or hybrid interventions). Thirteen patients suffered from acute (n=9) or subacute (n=4) lesions accompanied by abdominal pain in 12 and acute limb ischemia caused by peripheral embolization in 1 patient. The other 8 patients had asymptomatic chronic dissections with co-existing abdominal aortic aneurysm (AAA, n=4), penetrating aortic ulcers (PAU, n=2), or an increase in aortic diameter >5 mm in 6 months (n=2) based on computed tomographic angiography (CTA).
All patients with acute symptoms underwent analgesic therapy and medical management of systolic blood pressure (target <120 mmHg) for at least 5 days. If pain persisted after this regimen, the patient was treated by endovascular means. Otherwise, the patient underwent conservative treatment with radiologic and clinical follow-up in pre-arranged examinations. If during the course of conservative treatment, PAU or aneurysm progression was detected, an aggressive approach was elected even for cases with <5-cm-diameter lesions. During the span of this study, 5 patients were treated conservatively.
All endovascular repairs were performed percutaneously with use of the Prostar XL 10-F vascular closure system (Abbott Vascular, Redwood City, CA, USA). A variety of stent-grafts (10 tube, 9 bifurcated, 1 aortouni-iliac) were used: Talent (Medtronic Vascular, Santa Rosa, CA, USA), Zenith (Cook Medical Inc., Bloomington, IN, USA), Endurant (Medtronic Vascular), Anaconda (Vascutek, a Terumo company, Inchinnan, Scotland), and Excluder (W.L. Gore & Associates, Flagstaff, AZ, USA). In one patient at low risk of peripheral embolization due to an absence of thrombus, a bare metal stent (Luminexx; Bard Peripheral Vascular, Tempe, AZ, USA) was used to cover the dissection.
Follow-up included CTA within 1 month postoperatively, duplex ultrasound at 3 and 6 months, CTA at 12 months, and then annual duplex scans. If an increase in the aortic diameter >5 mm in 6 months was detected, CT was performed to determine the cause. Duplex scans with contrast were not available in our institution.
RESULTS
Early (30-day) mortality was 0%. No major adverse events (e.g., myocardial infarction, pneumonia, or stroke) occurred during the hospital stay. The patients with co-existing AAA/PAU covered by the stent-graft had complete exclusion of the sac without evidence of type I/III endoleaks.
Two patients developed access-site pseudoaneurysm and underwent surgical restoration of the common femoral artery. One patient developed a transient increase in serum creatinine (1.2 to 1.7 mg/dL) probably caused by microembolization to the renal arteries after placement of an Anaconda tube graft; however, the values normalized before discharge. The patient with the aortouni-iliac stent-graft developed early graft thrombosis owing to residual stenosis of the common iliac artery; the occlusion was recanalized with transfemoral thrombectomy and balloon angioplasty. He also suffered from postoperative delirium, which resolved during the hospital stay.
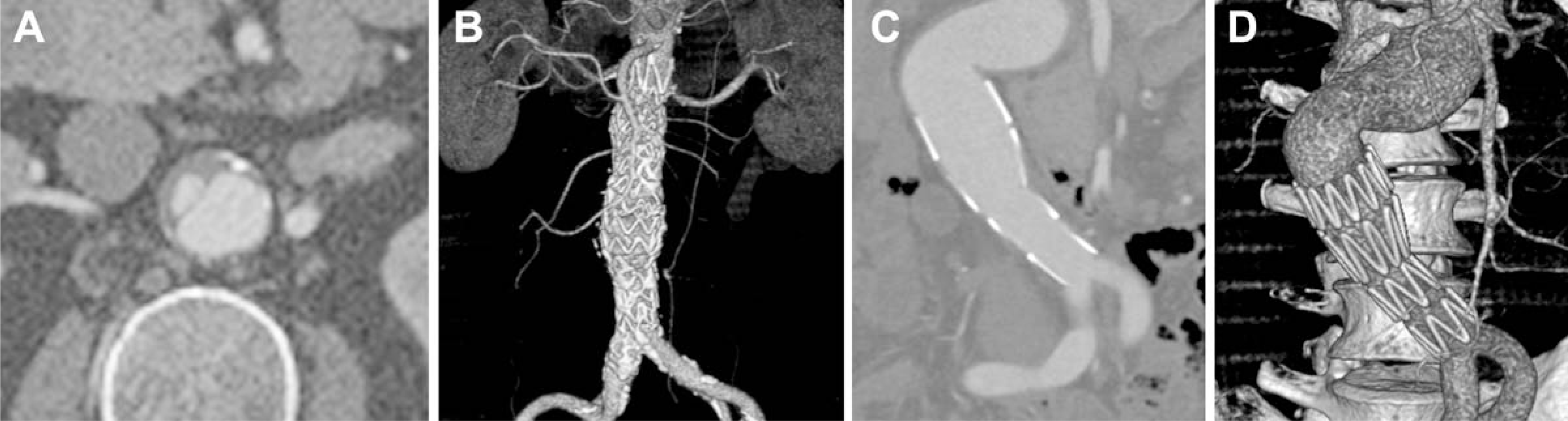
During a mean follow-up of 73±22 months (range 19–144), 3 patients died due to unrelated causes (pneumonia, intracranial aneurysm rupture, and cardiac failure, respectively). The survival rate at a median 67 months was 95% (95% CI 86% to 100%; Fig. 2A). One patient with a co-existing AAA who had a failed coil embolization of a type II endoleak underwent surgical conversion at 1 year postoperatively due to sac expansion. Freedom from reintervention was 95% (95% CI 87% to 100%; Fig. 2B) at a median 67 months. All other patients showed full aortic remodeling postoperatively without evidence of endoleak or stent-graft migration (Fig. 3).
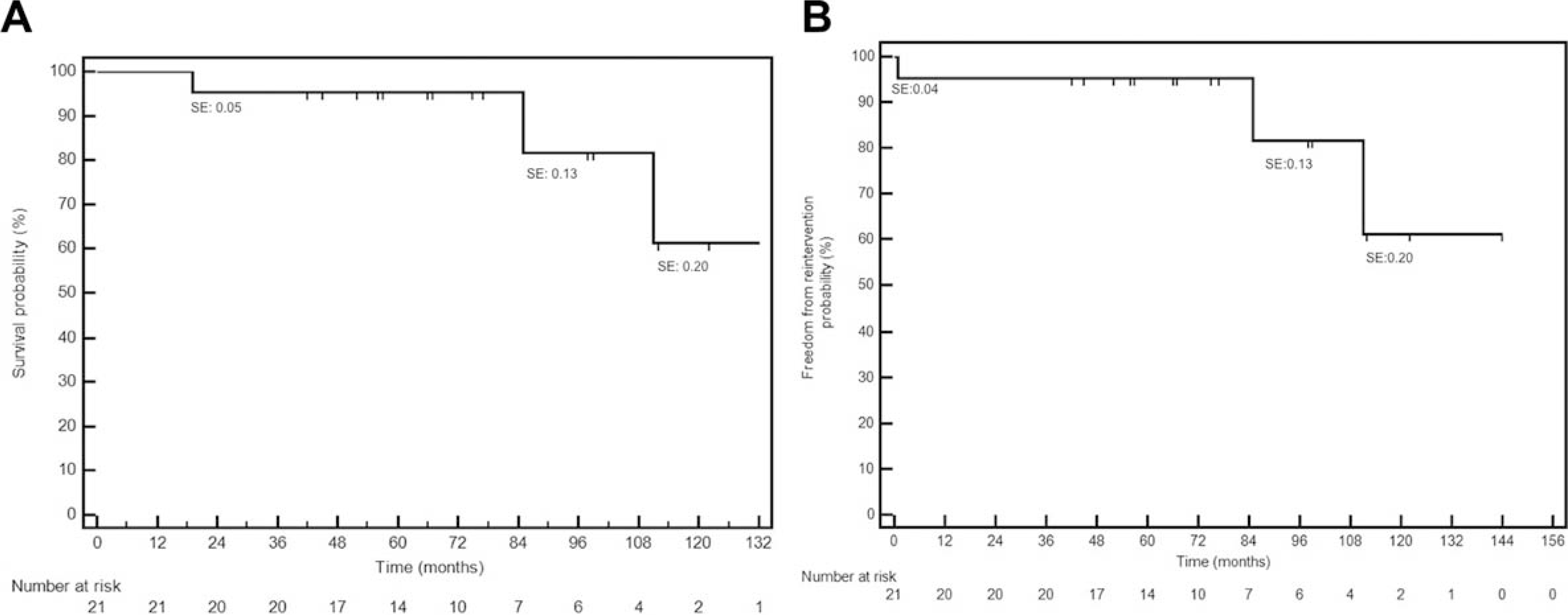
Kaplan-Meier estimates of (
(
DISCUSSION
Outcomes after endovascular treatment of IAAD are notable because surgical treatment of this rare lesion is generally associated with a considerable risk of in-hospital mortality (4%) and complications (9%). 1 Kouvelos et al. 7 recently published their results of endovascular treatment in 14 patients with IAADs. During a mean follow-up of 37±23 months (range 8–82, median 32.5), 2 patients experienced primary treatment failure and underwent reintervention that led to a successful outcome. The cumulative freedom from reintervention was 90.9% at 58 months, which is on par with our 95% freedom from reintervention at a median 67 months in 21 patients.
Management strategies for abdominal dissections are evolving. Asymptomatic IAADs should be treated conservatively under radiological and clinical surveillance. If the patient is symptomatic, medical treatment with analgesic and antihypertensive medication should be administered first. In cases of persistent pain or expanding AAA, an intervention is justified in order to restore the vessel wall.
There is little literature about the preferable invasive modality for IAAD. In the meta-analysis from Jonker et al., 1 surgical treatment was the selected approach in 50% of the 92 analyzed patients. One (2.2%) patient died during the hospital stay and 6 (13%) suffered from neurological lower limb problems (n=4), bleeding (n=1), or renal failure (n=1). The use of endovascular techniques, on the other hand, allows less invasive treatment of IAADs with little or no mortality and a low complication rate. 1 We encountered no procedure-related death or major morbidity in our series. Jonker's analysis 1 also reported a low complication rate for the endovascular approach, with only one neurological lower limb problem among 19 endovascular cases vs. 4 in the 46-patient open group.
A co-existing aneurysmal aorta makes the onset of IAADs more complex. More than a quarter of our patients had concomitant AAA or PAU. Similarly, Jonker et al. 1 reported IAAD associated with AAAs in 42% of the patients reviewed. There is scant evidence about the nature and progression of IAAD. Our clinical experience with aortic wall lesions, such as PAUs, intramural hematomas, or dissecting saccular aneurysms, has brought about an early and aggressive approach to treatment due to the progressive degeneration of the aortic wall leading to rupture. Therefore, we prefer early invasive treatment of IAADs with co-existing PAUs/AAAs even for lesions with a diameter of <5 cm.
There are no clear indications for one type of endovascular device over another. If relevant thrombus formation is absent in the true lumen, then the risk of peripheral embolization is low; in this situation, the use of bare metal stents can be considered as a first choice to ensure perfusion of collateral pathways and lumbar arteries. On the other hand, if there is a risk for peripheral embolization or a co-existing AAA, the use of stent-grafts is recommended. The location of the proximal landing zone (supra- vs. infrarenal) seems to be irrelevant based on our experience, though we almost exclusively used endoprostheses with suprarenal fixation.
Conclusion
Despite the small number of patients studied, our experience with endovascular treatment of IAADs seems to indicate that it is a safe method, with durable results over the long term. The less invasive nature of the procedure is associated with clear clinical benefits in terms of mortality and morbidity. Imaging follow-up to 12 years is very promising, with full aortic remodeling, rare need for secondary interventions, and no evidence of type I/III endoleaks in patients with concomitant AAA/PAU.