
Abstract

To the Editors:
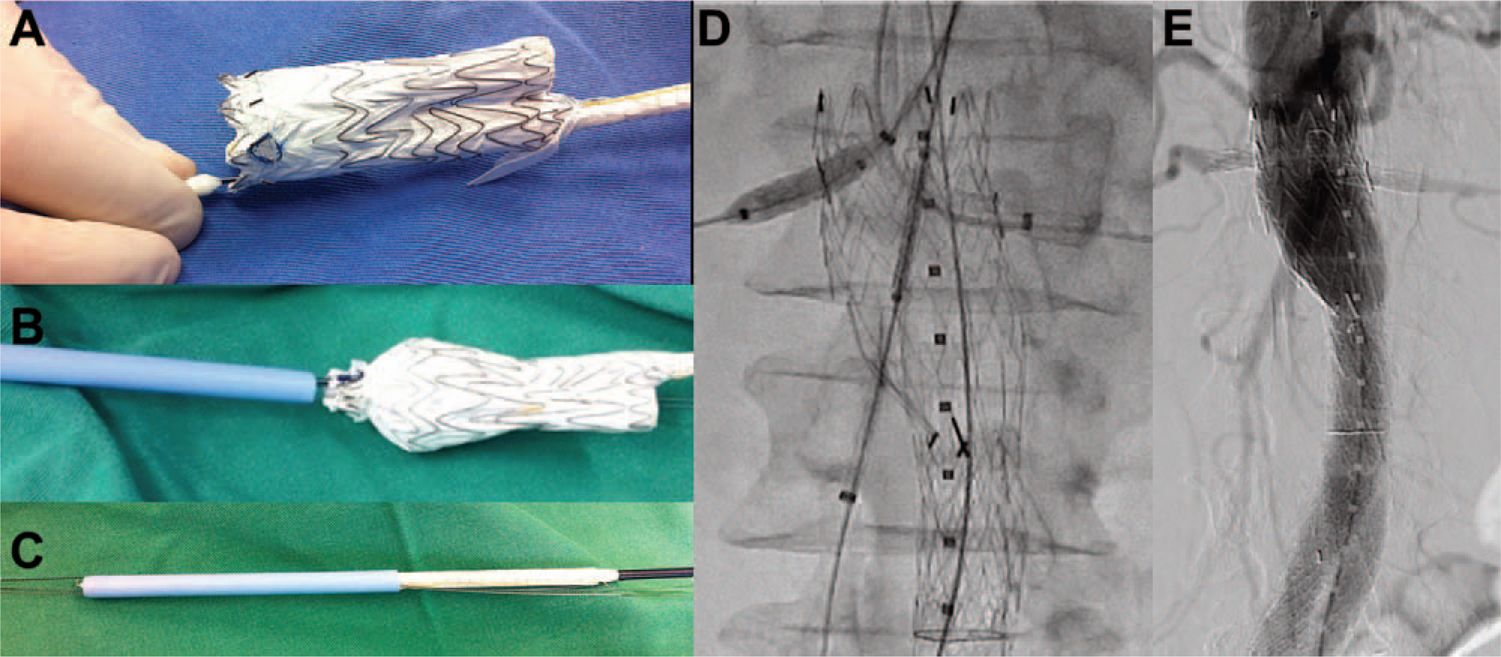
The article by Stephen and colleagues 1 shows a novel cautery instrument for on-site fenestration of Dacron endografts, but we believe that fenestration techniques may be applied to polytetrafluoroethylene (PTFE) endografts as well. Our group has developed a new technique using a physician-customized fenestrated C3 Excluder (W.L. Gore & Associates, Flagstaff, AZ, USA) to treat aortic aneurysms with unsuitable necks. On a back table, the bifurcated Excluder is released until the contralateral leg is entirely liberated (Figure, A). Five-millimeter fenestrations are constructed with a circular object cutter (punch). The edges of the fenestrations are reinforced with a radiopaque wire from a snare (Covidien, Mansfield, MA, USA); the wire is anchored to the graft with CV6 PTFE suture (W.L. Gore & Associates). Next, the fenestrations are pre-cannulated with 0.018-inch guidewires. After that, the opened main body and contralateral leg of the endograft are manually constricted and re-sheathed into a 22-F tube segment detached from a 22-F Dryseal introducer flow valve (Figure, B and C). This tube segment containing the re-sheathed endoprosthesis is inserted in a 22-F Dryseal sheath. Once delivered to the target site, the Dryseal is partially retracted using a “pin and pull” mechanism until the main body is completely exposed outside the sheath, positioning the fenestration at the level of the visceral vessels. Next, the target visceral arteries are selectively cannulated and balloon-expandable covered stents (Advanta V12; Atrium Medical Corporation, Hudson, NH, USA) are deployed (Figure, D and E).
(
This technique using a repositionable endograft, which we have applied in 24 patients thus far, has several advantages, such as precise deployment and simplicity, and it requires only a short time to accomplish the on-site customization. We believe that a fenestrated PTFE endoprosthesis may represent an alternative in patients who are unable to wait for a custom-made device.