
Abstract
Endovascular stent implantation was introduced to femoropopliteal procedures almost 2 decades ago. Initial results with balloon-expandable stainless steel stents and self-expanding Elgiloy stents, however, were disappointing. In particular, recurrence rates after long-segment femoropopliteal stenting were catastrophically high, in the range of 60% to 80% at 1 year. Also, attempts to resolve the problem of in-stent restenosis (ISR) using first-generation covered stent-grafts led to unsatisfactory results, high procedural complication rates due to large introducers, and a high incidence of graft thrombosis, which did not make these devices convincing alternatives to bare metal stents. After years of stagnation, however, recent developments in femoropopliteal stent technology have been promising. Self-expanding nitinol stents have been evaluated in several prospective studies. Initial problems with stent fractures seem to be resolved using second-generation devices; for the first time, stenting has been shown to be beneficial compared to balloon angioplasty in longer femoropopliteal lesions. Nevertheless, although superior to balloon angioplasty, nitinol stenting is still associated with a considerable restenosis rate, and treatment of ISR remains problematic. Future concepts to further improve long-term patency after femoropopliteal stenting therefore are under investigation, including drug-eluting stents, biodegradable stents, and coated stent-grafts. From a current perspective, femoropopliteal stenting remains the Achilles' heel of the interventionist.
Keywords
Endovascular therapy is a minimally invasive treatment for patients suffering from intermittent claudication or critical limb ischemia (CLI) due to peripheral artery disease (PAD). The technology rapidly evolved during the last decade, and there is a growing experience in the treatment even of complex cases. The main advantages of percutaneous revascularization are a low complication rate, a high technical success rate approaching 90% even in long occlusions, and an excellent short-term clinical outcome. However, late clinical failure due to restenosis remains the major drawback of percutaneous angioplasty and limits widespread application of this minimally invasive technique. 1 Competitive surgical approaches yield better long-term results, and the indications for endovascular revascularization, therefore, remain a matter of debate.1,2
HISTORY OF FEMOROPOPLITEAL STENTING
The femoropopliteal segment is the most challenging vascular territory with respect to restenosis after endovascular treatment. The superficial femoral artery (SFA) is the longest artery in the human body and is fixed between two major flexion points: the hip and the knee. During movements such as walking or stair climbing, various forces are exerted on this vessel, including flexion, longitudinal and lateral compression, and torsion. Furthermore, the artery dives through a major muscle group at the site of Hunter's canal, leading to additional external compression during muscular work. In contrast to iliac arteries, the anatomy of the vascular wall in the femoropopliteal segment is characterized by an increased density of vascular smooth muscle cells, hence the reason this type of artery is referred to as a “muscular artery.” Response to injury by extensive scar formation leading to restenosis seems to be a specific feature of muscular arteries, making an endovascular approach prone to midterm failure. 3 Furthermore, atherosclerotic disease in long vascular segments, particularly the femoropopliteal, is usually characterized by diffuse, heavy calcification. This disease pattern is frequently associated with immediate balloon angioplasty failure in the form of elastic recoil, vascular dissection, and high-grade residual stenosis, which occur in up to ~30% of the angioplasty cases.
Endovascular stent implantation resolves these problems of elastic recoil, residual stenosis, and flow-limiting dissection, which enables treatment of long, complex, and heavily calcified lesions. The concept of stenting thus seems a logical alternative to plain balloon angioplasty in the femoropopliteal segment. Nevertheless, the aforementioned mechanical stressors in the femoropopliteal segment always were a matter of concern with respect to the durability of stents. Regardless, though, stenting was introduced to femoropopliteal procedures almost 2 decades ago, when balloon-expandable stainless steel stents were first used to treat short lesions. As always, initial reports were enthusiastic; however, 5 randomized controlled trials failed to show a beneficial effect of balloon-expandable stents compared to balloon angioplasty of short femoral lesions.4–8
The potential limitations of balloon-expandable stents in the femoropopliteal segment—the availability of only short stents and the risks associated with stent crush by external forces—led to the use of an alternative technology, namely, self-expanding Elgiloy stents (Wallstents), to treat lengthy femoropopliteal disease or lesions unresponsive to balloon angioplasty. It took several years to confirm that Wallstents yielded good immediate results, but they had low midterm patency and a relatively high rate of stent fractures.9,10 The use of Wallstents thus was abandoned for femoropopliteal treatment.
Meanwhile, several groups evaluated the concept of covered stent-graft implantation for treatment of long-segment femoropopliteal disease. 11 Again, initial results were good; however, it soon turned out that the rates of early and late thrombosis due to edge stenosis of the stent-grafts were unacceptably high. 12 Furthermore, the considerable morbidity due to the large introducers made these early femoral stent-graft implantations an inconvenient procedure for the patient. 12 Thus, stent-grafts came to be used mainly for treatment of (iatrogenic) arterial ruptures or aneurysms in the femoropopliteal segment.
For more than a decade, femoropopliteal stent implantation thus remained a bailout procedure after failed balloon angioplasty. Considering the high rates of recurrence after balloon angioplasty and the inability to offer durable endovascular alternatives, the indication for endovascular treatment of long femoropopliteal segments remained debatable and was definitively not recommended by the first TASC (TransAtlantic Inter-Society Consensus) working group. 1
The introduction of self-expanding nitinol stents once again changed the treatment of femoropopliteal disease. Self-expanding nitinol stents had improved radial strength, with shape-memory characteristics that promoted crush recoverability; they also had reduced foreshortening, which allowed precise placement. These properties led to better patency rates compared to earlier stent designs,9,10 although the underlying causes for the evident superiority of nitinol stents have yet to be determined.
CURRENT STATUS OF FEMOROPOPLITEAL STENTING
The application of nitinol stent technology seemed to improve the durability of stenting in the femoropopliteal segment. 13 One randomized trial reported only 8% restenosis within 6 months after implantation of bare nitinol stents in the SFA. 14 We observed patency rates above 80% with modern nitinol stents in non-diabetic patients, even those with long lesions >10 cm. 15 These promising results led us to initiate the first randomized controlled trial comparing primary stenting with new self-expanding nitinol stents to balloon angioplasty (BA) with provisional stenting for treatment of femoropopliteal obstructions in PAD patients. 16 In the Vienna Absolute trial (Balloon Angioplasty Versus Stenting With Nitinol Stents in the SFA), we randomly assigned 104 patients with severe claudication or chronic limb ischemia and SFA stenosis or occlusion to primary stent implantation (n=51) or BA (n=53) with optional stenting in case of residual stenosis >30%, early elastic recoil, or flow-limiting dissection. The primary study endpoint was the binary angiographic restenosis rate at 6 months; secondary endpoints were restenosis rates by duplex ultrasound at 3, 6, and 12 months and the clinical and hemodynamic outcomes. Average lengths of the treated segments were 132±71 mm and 127±55 mm in the stent and BA groups, respectively. In the BA group, secondary stenting was performed in 17/53 patients (32%) due to a suboptimal result; however, these patients were analyzed in the balloon angioplasty group as part of the intention-to-treat analysis. Restenosis rates were 23.5% and 43.4% (p=0.05) at 6 months by angiography in the stent and BA groups, respectively; at 12 months, the rates were 36.7% and 63.5% (p=0.01) by ultrasound. Clinically, patients in the stent group had a significantly higher maximum treadmill walking capacity compared to the BA group at 6 and 12 months, and ankle-brachial indexes also were significantly improved by primary stenting. We concluded from this trial that primary stenting improved 1-year morphological and clinical outcomes in these patients with a median lesion length of ~10 cm; however, larger studies and longer follow-up intervals were necessary to establish stenting as the treatment option of first choice. Soon thereafter, the 2-year results of this study were reported, 17 which confirmed a sustained benefit of primary nitinol stenting compared to BA with optional stenting. Admittedly, the rate of restenosis also in the primary stent arm (45.7% versus 69.2%) left room for improvement.
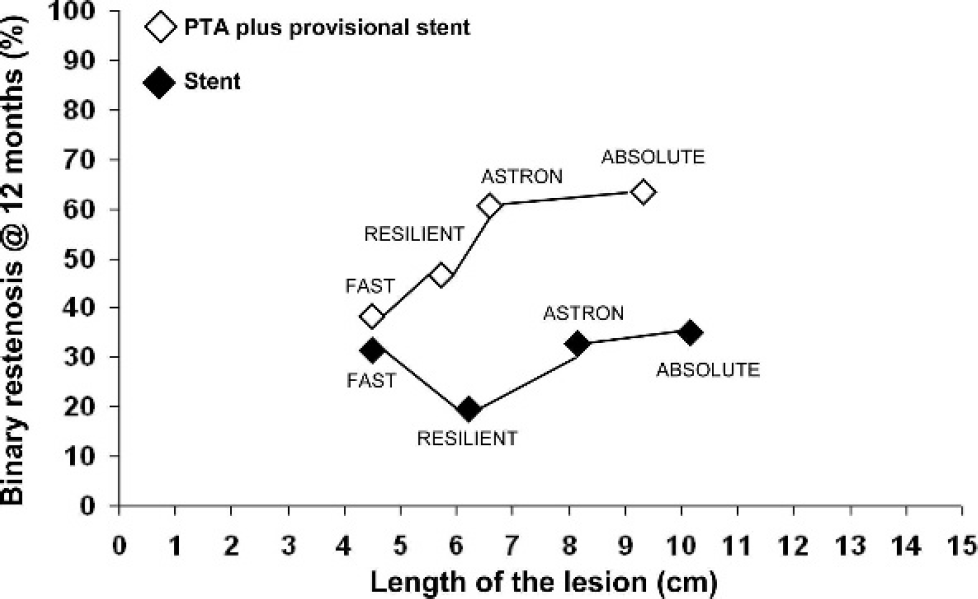
Comparison of restenosis rates at 12 months in different randomized studies comparing primary stenting to angioplasty with provisional stenting: the studies are grouped according to the length of the treated lesions.
During the time in which we were conducting the Absolute trial, other randomized studies were done (Figure). Among these, FAST (Femoral Artery Stenting Trial) included 244 patients with femoropopliteal lesions between 1 and 10 cm who were randomized to plain BA (n=121) versus primary stent implantation (n=123) with a self-expanding nitinol stent. 18 Mean lesion length was between 4 and 5 cm in both groups. Technical success rates were 95% versus 79% in favor of primary stenting. At 12 months, however, restenosis rates were 32% versus 39% in the stents versus BA groups, a difference that was not statistically significant. Remarkably, all subgroup analyses, including presence/absence of diabetes, long versus short lesions, and stenosis versus occlusions, yielded trends but no significant benefit of primary stenting. The authors concluded that primary stenting in femoropopliteal lesions <10 cm did not yield a significant benefit with respect to restenosis prevention.
Results of the RESILIENT (
ASTRON (Balloon Angioplasty vs. Primary Stenting of Femoropopliteal Arteries Using Self-Expandable Nitinol Stents) was a small randomized trial, again not yet published, of 73 patients with a mean SFA lesion length of 8.4 cm randomized to primary stenting (n=34) or BA with optional stenting (n=39). At 12 months, the restenosis rate with primary stenting (34.4%) was significantly lower compared to BA (61.1%).
Besides the problems associated with neointimal hyperplasia and in-stent restenosis (ISR), the issues of material fatigue and stent fracture have arisen during the last few years. The first systematic evaluation of stent fractures in the SFA was done in the SIROCCO I trial. 14 At 12 months in this series, fractures were found in 31% of the patients, with a mean stent length of 85 mm and a maximum of 3 stents implanted. As a consequence, a maximum of only 2 stents were allowed in the SIROCCO II trial, resulting in a marked reduction of stent fractures to 11% at a mean stented length of 82 mm. 19 However, it seemed that different stents exhibit major differences in stress resistance: we observed a <2% stent fracture rate with a mean stented segment length of 124 mm using a different type of nitinol stent. 10 Similarly, remarkable differences between various products were found in nonrandomized registries. 20 Based on these experiences with first-generation devices, stent design has been dramatically improved, and various companies have launched “fracture-free” products specifically designed for the mechanically-demanding femoropopliteal environment. So far, they have yielded fracture rates <5% even in long lesions.
Finally, the treatment of ISR in nitinol devices remains a major drawback. Recurrent restenosis after balloon angioplasty of a nitinol stent ISR occurs in up to 60% within only 6 months after re-treatment. 21 Since a rapidly increasing number of patients with SFA disease have been treated by stent implantation in the last few years, we now are confronted with more and more patients presenting with ISR, which is mainly caused by endogenic factors. Since treatment of such restenoses with balloon angioplasty alone has a very high refailure rate, different treatment modalities have been investigated to reduce the high recurrence rate. Unfortunately, the ultimate tool for treatment of ISR has not been found or invented yet, since there is no single randomized trial in patients with ISR demonstrating the superiority of one technique over the other. Alternative technologies, such as Cutting Balloon angioplasty, also were not proven effective in this context. 21 In our experience, follow-up investigations and early reinterventions are of great value. Especially after long-segment stenting, it may be very easy to treat a focal ISR, but it can be very complicated to re-open the resultant (untreated) long-segment stent thrombosis. Therefore, we recommend treating high-grade ISR—even if asymptomatic—before stent thrombosis occurs.
THE FUTURE OF FEMOROPOPLITEAL STENTING
The main obstacle of current nitinol stents remains exaggerated neointimal hyperplasia leading to ISR. Putting the findings from the available randomized trials together, bypass surgery with venous grafts must still be considered the most durable revascularization technique for patients with chronic limb ischemia and extensive disease in the SFA. 2 Nitinol stents may be an effective alternative to surgical revascularization of longer lesions in poor surgical candidates with severe cardiovascular comorbidity. Furthermore, stenting may be an option for patients without available saphenous vein grafts, as the 12-month stent patency data are comparable to those for prosthetic bypass grafts, and stenting has a considerably lower rate of complications. 1 However, the endovascular approach seems justified only as long as low complication rates are encountered and the surgical landing zone for the distal anastomosis of a potential secondary bypass operation remains unaffected by the interventional procedure. Therefore, further improvement of femoropopliteal stent technology is urgently necessary.
In the near future, drug-eluting stents (DES) may help to further improve the durability of stents in lower limb arteries. As yet, trials evaluating DES were underpowered and showed disappointing long-term outcomes.14,19 Nevertheless, the concept of combining the advantages of mechanical nitinol scaffolding with the antiproliferative action of drugs seems appealing. As yet, 2 major trials are ongoing and evaluate the different concepts of DES technology. In the STRIDES (Study to Evaluate the Safety and Performance of the Dynalink-E, Everolimus Eluting Peripheral Stent System for Treating Atherosclerotic de Novo or Restenotic Native Superficial Femoral and Proximal Popliteal Artery Lesions) study, an everolimus-coated stent is being evaluated in a nonrandomized prospective setting; the ZILVER (Evaluation of the Zilver PTX Drug-Eluting Stent in the Above-the-Knee Femoropopliteal Artery) study uses a non-polymer technology and a paclitaxel-coated device in a randomized setting. Both studies seem to be adequately powered to provide clinically important information on the future of DES technology in the femoropopliteal segment.
Drug-coated balloons may be promising alternative strategies to prevent restenosis, as shown by the first randomized trial of the paclitaxel-coated balloon. 22 This stentless approach seems appealing in light of the problems associated with stent fractures; however, the problems of elastic recoil, heavy calcification, and residual stenosis after balloon angioplasty of long and complex lesions likely cannot be resolved by the drug-coated balloon approach.
Biodegradable stents seem a concept worth further investigation. However, the main problems are currently the unsatisfactory mechanical properties both of metallic (magnesium-based) or polymeric-based biodegradable materials. Radial force of the tested devices seems to be insufficient for the femoropopliteal segment, and true self-expanding properties can hardly be achieved using the current investigational devices.
Finally, stent-grafts may have a renaissance because lower profile introducer sizes have dramatically decreased the complication rates. Kedora et al.
23
performed a randomized prospective study comparing the treatment of SFA occlusive disease with the Viabahn stent-graft (n=50) to surgical femoropopliteal above-knee bypass with synthetic graft material (n=50). The stent-graft, a self-expanding helical nitinol stent mounted to the outside surface of a tube of expanded polytetrafluoroethylene, was implanted over a mean 25.6 cm total length of artery, which is much longer than in the studies with bare nitinol stents. Primary patency at 12 months was not statistically different between the stent-graft group and the surgical group (73.5% versus 74.2%, respectively). Nevertheless, it remains to be determined whether the mechanical properties of these devices can withstand the forces exerted in the femoropopliteal segment and whether the problem of stent-graft thrombosis can be resolved by an active (heparin) coating of the devices. The ongoing VIBRANT (
CONCLUSION
Endovascular treatment of the femoropopliteal segment remains challenging with respect to mid- and long-term outcomes. The use of nitinol stents improves patency rates in longer lesions, but restenosis remains a major concern. The indication for endovascular treatment has to be critically discussed with respect to surgical options and conservative medical treatment depending on patient symptoms and comorbidities.