
Abstract
Purpose
To angiographically evaluate infrapopliteal arterial lesion morphology in a consecutive series of patients presenting with critical limb ischemia (CLI) and undergoing infrapopliteal angioplasty.
Methods
A prospective analysis was undertaken of a consecutive series of CLI patients undergoing endovascular therapy in a tertiary referral center in the year 2011. Morphological assessment of baseline angiograms obtained prior to revascularization included lesion length, assessment of calcification using a semi-quantitative scoring system, and reference vessel diameter (RVD) measurement. Delta RVDs were assessed subtracting distal RVDs from proximal RVDs. A total of 197 infrapopliteal lesions in 105 CLI patients (n=106 limbs) were assessed. Of these, 136 lesions were treated by endovascular means.
Results
The average length of treated lesions was 87.1±43.8 mm in stenoses and 124.0±78.3 mm in chronic occlusions (p<0.001). Mean RVD proximal to the lesions was 1.88 mm whereas it was 1.66 mm distal to the lesions (p≤0.03). Mean arterial calcification was 1.15.
Conclusion
This prospective angiographic series underlines the complex nature and extensive longitudinal involvement of infrapopliteal lesions in CLI patients. These findings should be taken into consideration for anti-restenosis concepts in this challenging subgroup of peripheral artery disease patients.
Keywords
Chronic critical limb ischemia (CLI) affects 500 to 1000 per million inhabitants per year in the Western world. 1 CLI patients not undergoing arterial revascularization face 12-month mortality and amputation rates as high as 54% and 46%, respectively. 2 In contrast, CLI patients having successful revascularization survive longer with an increased quality of life compared to patients undergoing primary amputation.3,4
Today, endovascular therapy is considered the primary treatment modality for most CLI patients. 5 Given the substantial maturation of endovascular techniques and devices, most below-the-knee (BTK) obstructions can now be treated by endovascular means. However, restenosis remains the major drawback of infrapopliteal revascularization in CLI patients despite excellent limb salvage rates up to 74% after 5 years. 6 Restenosis subsequent to plain balloon angioplasty (BA) was reported to occur in up to two thirds of CLI patients at 3 months' follow-up.7–9
Meanwhile, the application of coronary drug-eluting stents (DES) in CLI patients with infrapopliteal disease of limited longitudinal extent was associated with significantly higher patency rates as compared to bare metal stents (BMS) and BA.10–12 It is our clinical opinion, however, that the BTK lesions treated in the framework of these trials were substantially shorter than those encountered in everyday clinical practice. To explore this hypothesis, we assessed infrapopliteal lesion morphology (i.e., lesion length, vessel diameter, degree of calcification) in a consecutive all-comers series of CLI patients undergoing endovascular infrapopliteal revascularization.
See commentary page 157
METHODS
Study Design
A protocol was constructed in which all patients undergoing endovascular treatment of infrapopliteal limb arteries for chronic CLI at a tertiary referral center from January to December 2011 were eligible for inclusion; patients with acute limb ischemia were ineligible. Ethics committee approval was waived since patients were being treated on a regular clinical basis. The study was carried out according to the Declaration of Helsinki, 13 and consent forms were obtained from all patients prior to inclusion in the prospective database. The definition of chronic CLI followed current consensus,14,15 i.e., presence of ischemic rest pain for >2 weeks or ischemic tissue loss associated with (1) an absolute ankle pressure <50 mmHg or (2) great toe pressure <30 mmHg. 14
Assessed risk factors included patient age and gender, hyperlipidemia, diabetes mellitus, hypertension, coronary heart disease, renal insufficiency, cerebrovascular disease, and cigarette smoking (Table 1). The definitions for the assessed risk factors were outlined previously. 16 All patients were evaluated by a team of interventionists and vascular surgeons for optimal revascularization on a case-by-case basis.
Demographics and Risk Factors of 105 CLI Patients Undergoing Endovascular Revascularization of Below-the-Knee Arteries
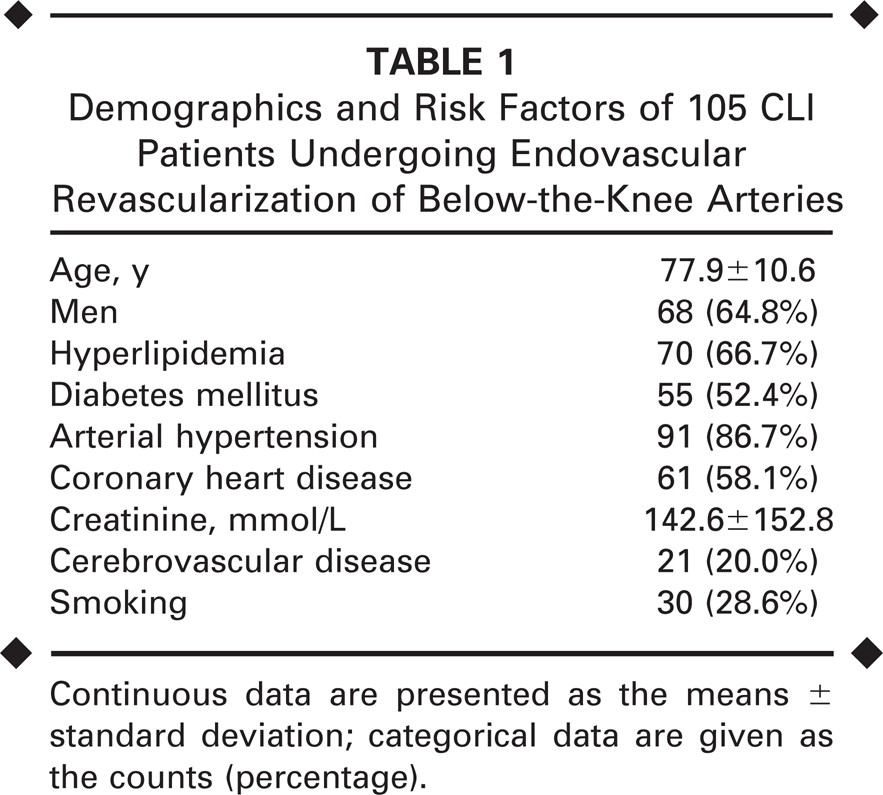
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Endovascular Revascularization
Endovascular therapy was attempted under local anesthesia after antegrade puncture and insertion of a 4-F to 6-F sheath in the ipsilateral common femoral artery whenever possible. In case of atherosclerotic involvement of the iliac and proximal superficial or deep femoral artery, a contralateral crossover approach was utilized. Recanalization of at least one infrapopliteal artery was attempted. In case of obstructions or multiple infrapopliteal arteries, the choice of which target artery to primarily address was based upon the clinical picture and the location of tissue loss. However, preference was given to those arteries exhibiting angiographically verified pedal reconstitution.
Additional inflow revascularization was performed in case of angiographically documented obstructive disease >50% affecting the ipsilateral iliac and/or femoropopliteal arteries. Baseline angiograms obtained over the intra-arterial sheath were utilized for morphological assessment. Thus, potential iatrogenic infrapopliteal obstructions secondary to iliac or femoropopliteal revascularization were excluded from the present analysis.
Biplanar angiograms were evaluated by consensus of 2 experienced readers (F.B. and N.D.) using calibrated subtracted images on PACS workstations (Siemens, Germany). The anatomical description of the affected infragenicular segment was in line with current reporting standards. 16 Obstructive disease was defined as a reduction of vessel diameter ≥50%. Accordingly, lesion length was defined as the distance over which the vessel diameter was reduced ≥50%; for occlusions, the length was determined from the level of occlusion to the point at which the artery was reconstituted by collaterals. Multifocal lesions were categorized as multiple lesions as soon as the obstructive disease was <50%.
The following infrapopliteal arterial segments were analyzed: the anterior tibial artery (ATA), tibioperoneal trunk (TPT), peroneal artery (PA), and posterior tibial artery (PTA). Data were stratified according to treated and untreated lesions. With respect to angiographically visible pedal artery reconstitution, the patency of plantar pedal arch (PPA) and dorsal pedal arch (DPA) was defined as absence of ≥50% obstruction based on digital subtraction angiography.
Delta RVDs were assessed subtracting distal RVDs from proximal RVDs (RVDp — RVDd). Given its limited anatomical length as compared to other infrapopliteal segments, the tibioperoneal trunk was not included in the calculation of mean lesion lengths and delta RVD values.
Calcification was assessed using a semi-quantitative scoring system 16 : none (0) vs. moderate (1) vs. heavy (2) calcification. Hyper-dense deposits of calcification were evaluated from baseline angiograms; no calcium deposits was defined as 0, calcification deposits <50% of lesion length as 1, and calcification deposits >50% of lesion length as 2.
Patient Population
In the 1-year period, 105 CLI patients (68 men; mean age 77.9±10.6 years) were eligible for this analysis. Patient demographics and risk factors are outlined in Table 1. Evaluation identified 196 infrapopliteal lesions in 106 limbs. Of these, 136 lesions were treated by endovascular means; 70 patients (71 limbs, 43 men) underwent primary endovascular therapy for chronic obstructions of the infrapopliteal arteries, while the remaining patients underwent repeated endovascular procedures (Table 2).
Angiographic and Technical Information on Below-the-Knee Revascularization in 106 Limbs
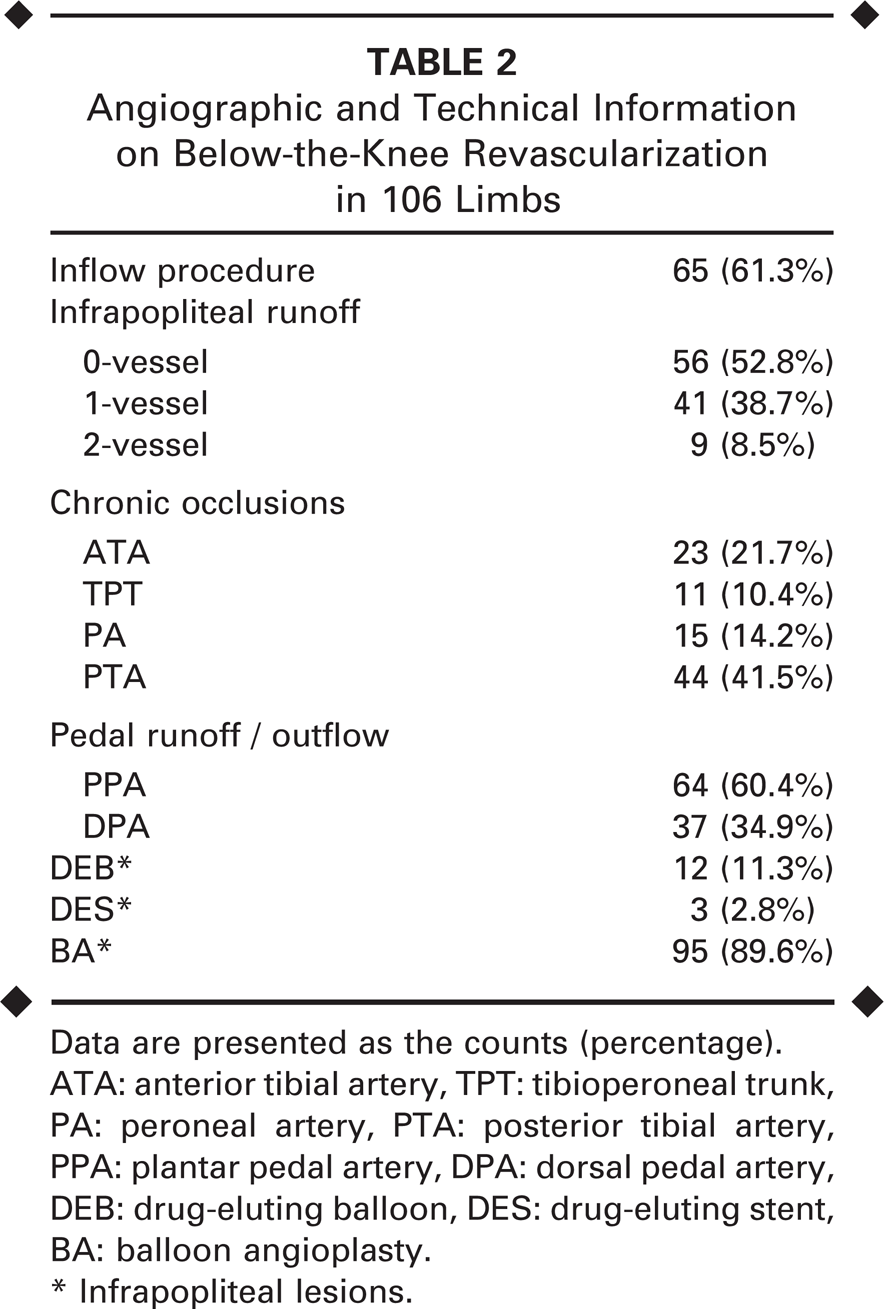
Data are presented as the counts (percentage).
ATA: anterior tibial artery, TPT: tibioperoneal trunk,
PA: peroneal artery, PTA: posterior tibial artery,
PPA: plantar pedal artery, DPA: dorsal pedal artery,
DEB: drug-eluting balloon, DES: drug-eluting stent,
BA: balloon angioplasty.
Infrapopliteal lesions.
Statistical Analysis
Demographic and clinical characteristics of the study population are reported as mean ± standard deviation for continuous variables and as number (percentage) for categorical variables. Univariate comparison analyses were performed using the Student t test for continuous variables and the Fisher exact test for discrete variables.
Regression analysis was performed to evaluate any correlation of delta RVD with lesion lengths in the infrapopliteal arteries. This correlation was analyzed using inter-reliability coefficient testing [Pearson correlation coefficient (r) with 95% confidence interval (CI)]. A coefficient <0.25 was interpreted as no correlation, 0.25 to 0.49 as minimal, 0.50 to 0.69 as intermediate, and >0.70 as a high correlation. P<0.05 was considered to indicate a statistically significant difference. Statistical analysis was performed using the MedCalc Software (version 11.2.1; Mariakerke, Belgium).
RESULTS
Mean lesion length of treated infrapopliteal arterial segments (Table 3) excluding the tibioperoneal trunk was 87.1±43.8 mm in stenotic and 124.0±78.3 mm in occlusive disease (p<0.001). Only 12 patients showed an infrapopliteal lesion length ≤35 mm; all of these lesions were treated. Of note, diabetes mellitus was not a predictor for increased lesion length (r=0.071, 95% CI −0.08 to 0.22, p=0.42).
Angiographically Determined Lesion Lengths of Infrapopliteal Lesions in 106 CLI Limbs at Baseline
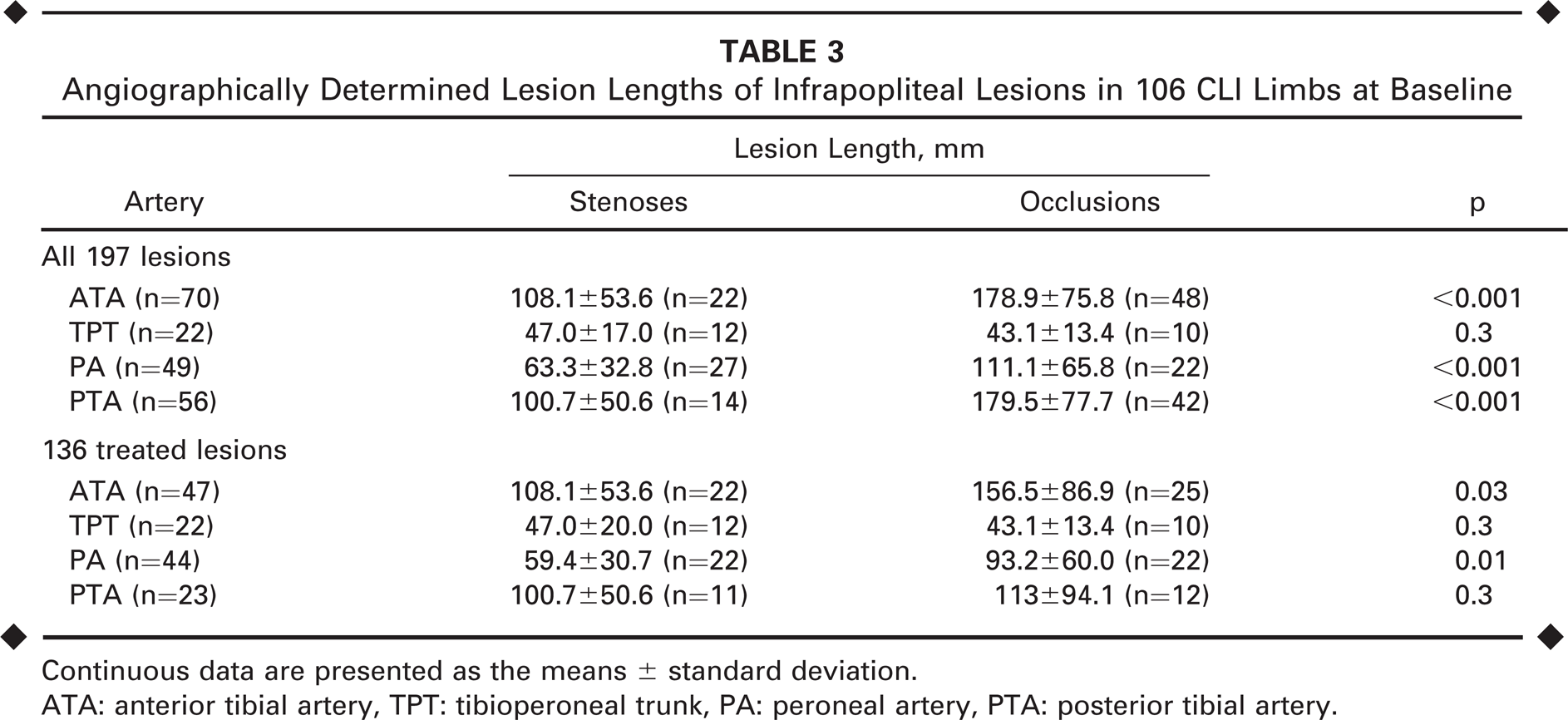
Continuous data are presented as the means ± standard deviation.
ATA: anterior tibial artery, TPT: tibioperoneal trunk, PA: peroneal artery, PTA: posterior tibial artery.
Mean reference vessel diameters (Table 4) proximal and distal to the infrapopliteal arterial lesions were 1.88 mm vs. 1.66 mm (p≤0.03). Differences between the proximal and distal RVDs (Figure) showed no significant correlation with increasing lesion length (r=0.21, p=0.03). However, a moderate correlation of delta RVD with lesion length was observed in the ATA (r=0.36, p=0.002), whereas no statistically significant correlation was observed in the PA (r=0.24, p=0.086) or the PTA (r=0.058, p=0.67) segments. The presence of diabetes mellitus had no influence on delta RVD (r=–0.008, 95% CI 0.09 to 0.07, p=0.84).
Angiographically Determined Reference Vessel Diameters Proximal and Distal to the Infrapopliteal Lesions in 106 CLI Limbs
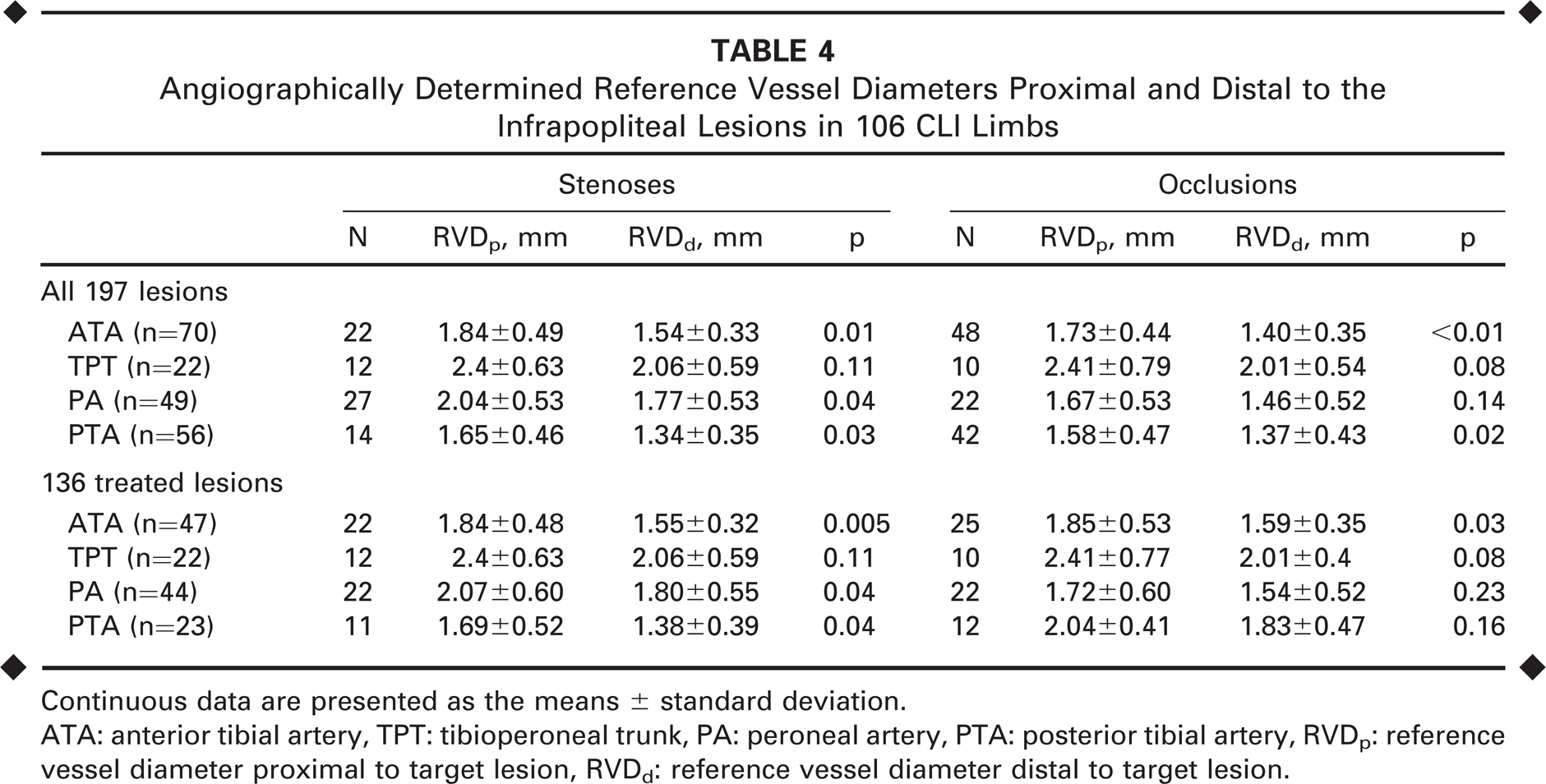
Continuous data are presented as the means ± standard deviation.
ATA: anterior tibial artery, TPT: tibioperoneal trunk, PA: peroneal artery, PTA: posterior tibial artery, RVDP: reference vessel diameter proximal to target lesion, RVDd: reference vessel diameter distal to target lesion.
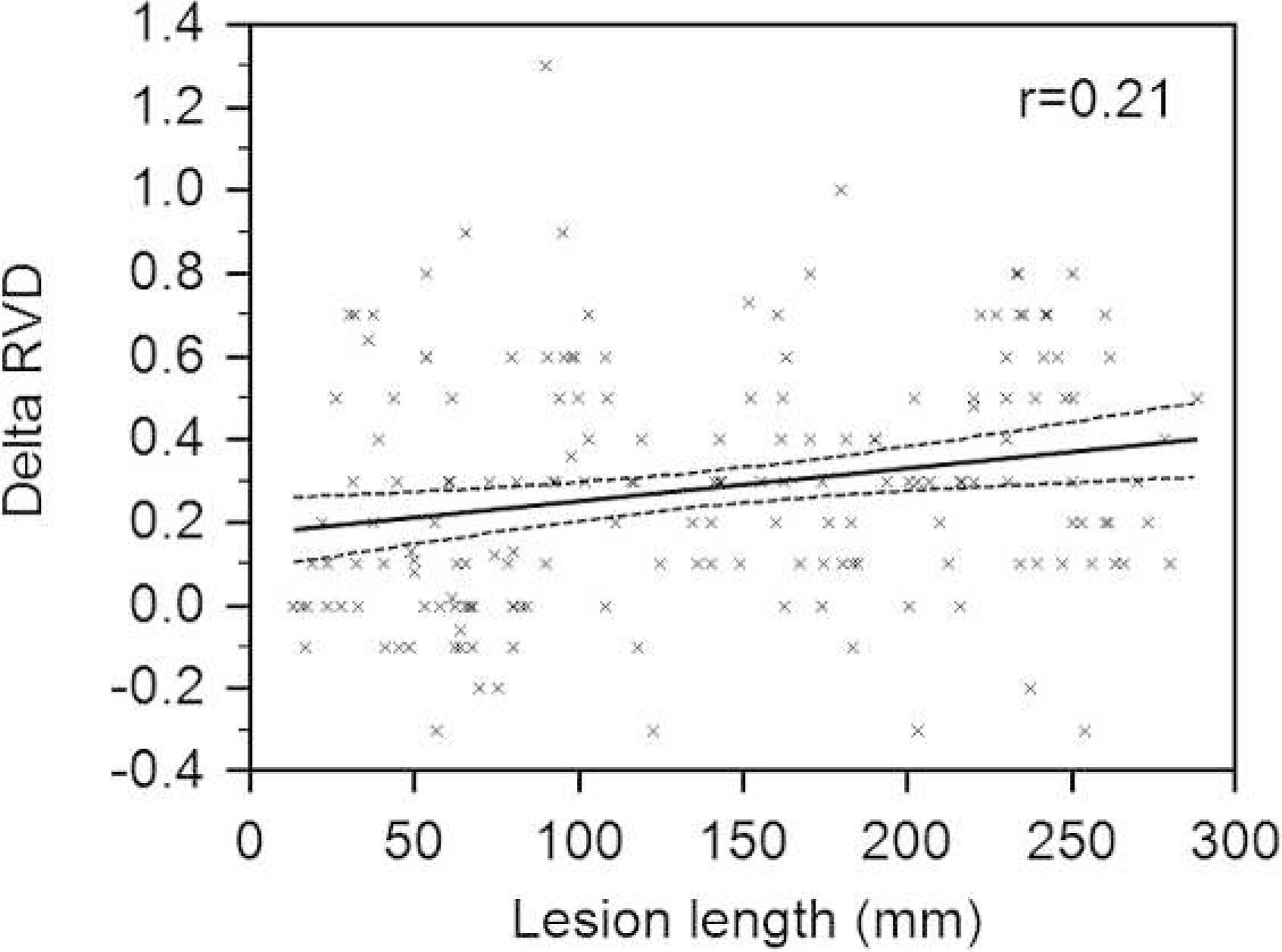
Correlation of delta reference vessel diameter (RVD) with lesion length.
Calcification was moderate to heavy in all infrapopliteal segments analyzed: the mean calcification score was 1.14±0.46 in the ATA, 1.12±0.70 in the TPT, 1.23±0.51 in the PA, and 1.09±0.49 in the PTA (p=0.45). Moreover, calcification did not differ comparing untreated with treated (p=0.08) or stenotic vs. occluded (p=0.5) segments. The presence of diabetes mellitus was not associated with a higher calcification burden (r=–0.16, 95% CI −0.27 to 0.05, p=0.004) in infrapopliteal obstructions.
DISCUSSION
Endovascular recanalization is a rapidly unfolding treatment option for patients with severe lower limb ischemia and atherosclerotic involvement of infrapopliteal arteries. While technical success rates for endovascular therapy of infrapopliteal arterial segments has increased substantially during recent years, restenosis remains the Achilles' heel of this minimally invasive treatment approach.7–9,17,18 Interestingly, in a recently published analysis of 2-year outcomes of the YUKON BTK study, 19 it was shown for the first time that long-term patency is associated with improved clinical outcomes. Thus, the tide-over concept that was deduced from earlier observations of no correlation between arterial patency and amputation rates subsequent to endovascular revascularization 20 is currently being questioned.
The present study aimed at analyzing lesion morphologies in a consecutive all-comers series of CLI patients undergoing endovascular revascularization in the infrapopliteal segment. Our findings indicate that infrapopliteal lesions in this challenging subset of patients are frequently of substantial longitudinal extent and exhibit a significant calcification burden. To date, dedicated information on infrapopliteal lesion morphology in CLI patients is very sparse. 21 In 417 diabetic CLI patients, Graziani et al. 21 observed infrapopliteal lesions to be mainly occlusions rather than stenoses, with an angiographically documented lesion length >10 cm in most cases.
Recently, different randomized10–12 and non-randomized22–28 trials have shown the advantage of coronary DES over BMS and over plain BA for the treatment of infrapopliteal lesions. In summary, a total of 501 patients were included in 3 different randomized trials analyzing the performance of DES for endovascular treatment of infrapopliteal occlusive disease.10–12 Rastan and colleagues 11 randomized 161 patients (both claudicants and CLI patients) to DES vs. BMS (YUKON BTK study) for obstructions of the infrapopliteal arteries. Similarly, a total of 140 CLI patients were randomized to either DES (n=74) or BMS (n=66) in the DESTINY trial, 10 whereas 200 CLI patients were randomized to balloon angioplasty (n=101) vs. DES (n=99) in the ACHILLES trial. 12 In all 3 studies, the application of DES was associated with higher angiographically determined patency rates at 12 months: 80.6% vs. 55.6% (p=0.004) in the YUKON trial, 85% vs. 54% (p=0.001) in the DESTINY trial, and 80.6% vs. 58.1% (p=0.006) in the ACHILLES study. In addition to these promising 1-year data, Werner et al. 26 provided follow-up data to 5 years supporting excellent outcomes subsequent to DES placement in infrapopliteal arteries.
Although these patency rates are encouraging, mean lesion lengths in the randomized trials10–12,19 were substantially shorter than those observed in the present unselected series: mean lesion length was 31±9 mm in the YUKON BTK study, 17.3±10.1 mm in the DESTINY trial, and 27.2±21.4 mm in ACHILLES. Compared to our measurements (87.1±43.8 mm in stenoses and 124.0±78.3 mm in chronic occlusions), the existing DES studies do not reflect the morphology of the majority of CLI patients in need of treatment. This finding is also corroborated by the low rate (2.8%) of stent usage for the prevention of restenosis in the present series, reflecting the described morphological observations.
Karnabatidis and coworkers 28 analyzed the application of multiple DES vs. BA and bailout BMS in infrapopliteal lesions averaging 77 mm long, closer to the lesion lengths observed in our study. Of note, lesions in the DES group were fully covered with everolimus-eluting stents. For this purpose, an average of 3.2 stents per lesion was required, for a total of 332 DES. In comparison, only 1.2 stents per lesion were deployed in the bailout BMS group. At 3-year follow-up, angiographically verified primary patency was significantly higher in the everolimus-stenting group (hazard ratio 7.98, 95% CI 3.69 to 17.25, p<0.0001) compared to BA and bailout BMS.
Katsanos et al. 29 evaluated the cost-effectiveness of coronary DES application in patients with infrapopliteal arterial obstructions. This analysis, which was based on two earlier studies,13,25 found infrapopliteal lesion lengths >10 cm to be associated with the least economically favorable scenario. This finding is reflected in the present series in which only 3 DES were applied, probably due to the longitudinal extent of the infrapopliteal lesions. Of note, infrapopliteal lesion length ≤35 mm was observed in only 12 patients within the present series. For these reasons, the application of currently available coronary stents with a maximum length of 38 mm (Abbott's XIENCE stent) cannot be considered as a first-line anti-restenosis concept for the treatment of infrapopliteal occlusive disease.
After having observed a 69% angiographically verified restenosis rate subsequent to infrapopliteal angioplasty of long lesions in CLI patients, Schmidt and colleagues 30 recently pioneered the application of drug-eluting balloons (DEB) in the infrapopliteal segment. 22 Very much in line with findings from the present study, mean lesion length in their 104 CLI patients was 176±88 mm. Follow-up angiography at 3 months revealed binary obstructive disease in 27.4% (comprising restenosis >50% in 19.1% and occlusion in 8.3%). Of note, the reobstructions were mainly focal, so angiography revealed binary restenosis / occlusion affecting the entire treated segment in only 9.5%. This non-randomized study may indicate a role for DEBs in the prevention of restenosis in the challenging infrapopliteal arteries.
Although the difference in the RVDs at the proximal and distal lesion sites was not significant within our series, probably due to limited sample size, there was a suggestion of a correlation of delta RVD with increasing lesion length (Figure). Thus, our data indicate that an ideal BTK stent has to be longer than those assessed in the DES trials10–12 and might have to accommodate diameter changes of the native artery over the length of the affected lesions.
The degree of calcification (mean score of 1.15) observed in the present series could impact upon recoil rates subsequent to infrapopliteal balloon dilation, for which infrapopliteal stenting can be advocated. Therefore, the degree of infrapopliteal calcification should be taken into consideration when deciding upon an anti-restenoses concept (DEB vs. DES).
Limitations
Our study has three major limitations. First, the number of observations is relatively small, which probably obscured any correlation of increasing RVD differences with lesion length. Second, considering that the assessment was based on angiography, a purely luminographic method, the true arterial diameters may have been underestimated in the present study. Third, the aim of this study was to describe the typical lesion pattern in CLI patients at our center. Thus, since serial angiography is not part of our institutional protocol, we have not specifically assessed clinical outcomes of patients from this study subsequent to angioplasty.
Conclusion
Our study provides important information on morphological characteristics of infrapopliteal occlusive disease in CLI patients. Infrapopliteal lesions in CLI patients are typically long, and the lesions lengths observed in everyday clinical practice are clearly beyond those treated within recent randomized DES trials.10–12,19 These findings should be taken into consideration in the development of further anti-restenosis concepts in this challenging subgroup of peripheral artery disease patients.