
Abstract
Purpose
To determine gutter size and stent-graft geometry in an in vitro juxtarenal aneurysm model using various chimney graft (CG) configurations.
Methods
Two silicone juxtarenal aortic aneurysm models were constructed combining different diameters of the aorta and renal artery. In a single-branched CG configuration, 2 sizes (23 and 28.5 mm) of Excluder stent-grafts were tested individually with 2 sizes of 2 types of CGs: Advanta balloon-expandable (BE) stent-grafts (6×59 and 12×61 mm) and Viabahn self-expanding (SE) stent-grafts (6×50 and 13×50 mm). All combinations were tested with a short (10-mm) and long (20-mm) sealing zone between the CG and main graft (total 16 configurations). Immediately after deployment, the CG configuration was scanned using a 64-slice computed tomography scanner. Gutter sizes were measured at different levels of the sealing zone.
Results
At the top of the sealing zone, the gutters were significantly larger in the BE CGs compared to SE CGs in combination with the 23-mm main graft (p=0.021). At the bottom of the sealing zone, there were no statistically significant differences (p=0.77). No significant differences were seen using the 28.5-mm main graft. Median gutter size was larger in the 6-mm CGs. The length of the sealing zone had no influence on gutter size. Significant compression of the main graft was found using 12 or 13-mm CGs compared to 6-mm CGs (p=0.001).
Conclusion
In this in vitro study, the CG configurations with BE stent-grafts show larger gutters than configurations with SE stent-grafts in small main grafts. Main graft compression is increased using wider CG stent-grafts.
Keywords
More patients are today being treated with endovascular aneurysm repair (EVAR) even when they have complex aneurysm anatomy, such as short or angulated proximal aortic necks.1–3 In juxtarenal aneurysms, fenestrated devices can preserve blood flow to renal or visceral branches, but customization, planning, and manufacturing of such stent-grafts requires time, during which the patients remain at risk of rupture. 4
The chimney (or sandwich) technique uses off-the-shelf stent-grafts parallel to the main aortic stent-graft to maintain perfusion of side branches in aneurysms with short proximal aortic necks.5–7 Early experience with the chimney technique has shown promising results.7–9 Inadequate sealing between a chimney graft (CG) and main graft leads to the formation of so-called gutters between the grafts and the aortic wall, which could lead to type I endoleaks. Several studies, however, show a high rate of spontaneously resolved type I endoleaks, possibly due to the formation of clot or poor outflow. 8
The aim of this study was to find the optimal CG configuration with the smallest gutters and acceptable main graft and CG compression (<50%).
METHODS
Experimental Model
Two double-branched silicone models of juxtarenal aortic aneurysms with the compliance of a human aorta were custom-made for this experiment (Fig. 1). Two different diameters (19 and 24 mm) of the main tube (“aorta”) and 2 diameters (5 and 11 mm) of the side branch (“renal artery) were used (Table). The model was placed in a tray containing water-gelatin with the same viscosity as blood and was kept at a constant temperature of 37°C.
Double-branched silicone juxtarenal aortic aneurysm models combining 2 diameters (19 and 24 mm) of the aorta and 2 diameters of the renal artery (side branch; 5 and 11 mm).
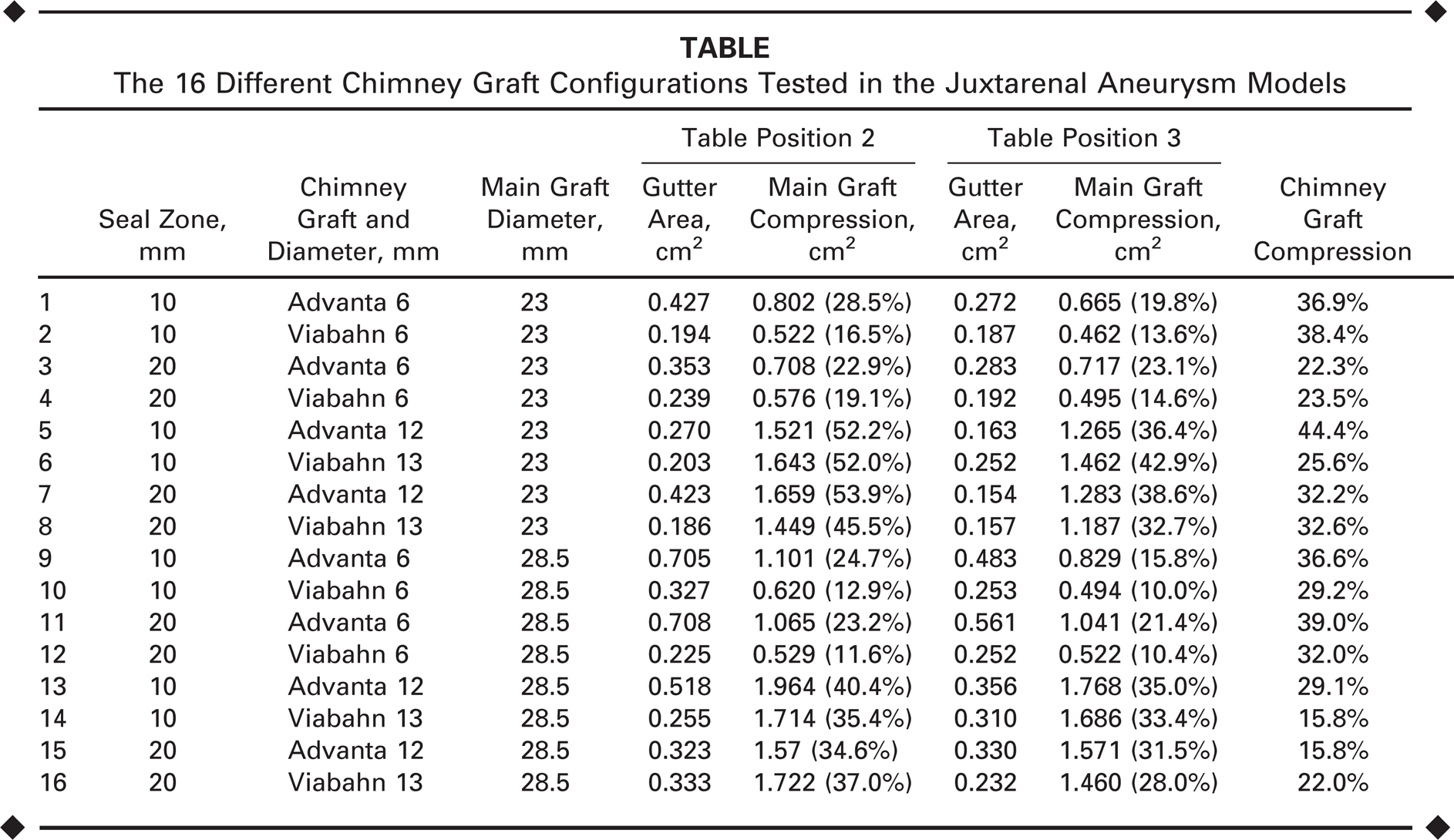
The 16 Different Chimney Graft Configurations Tested in the Juxtarenal Aneurysm Models
Stent-Graft Configurations
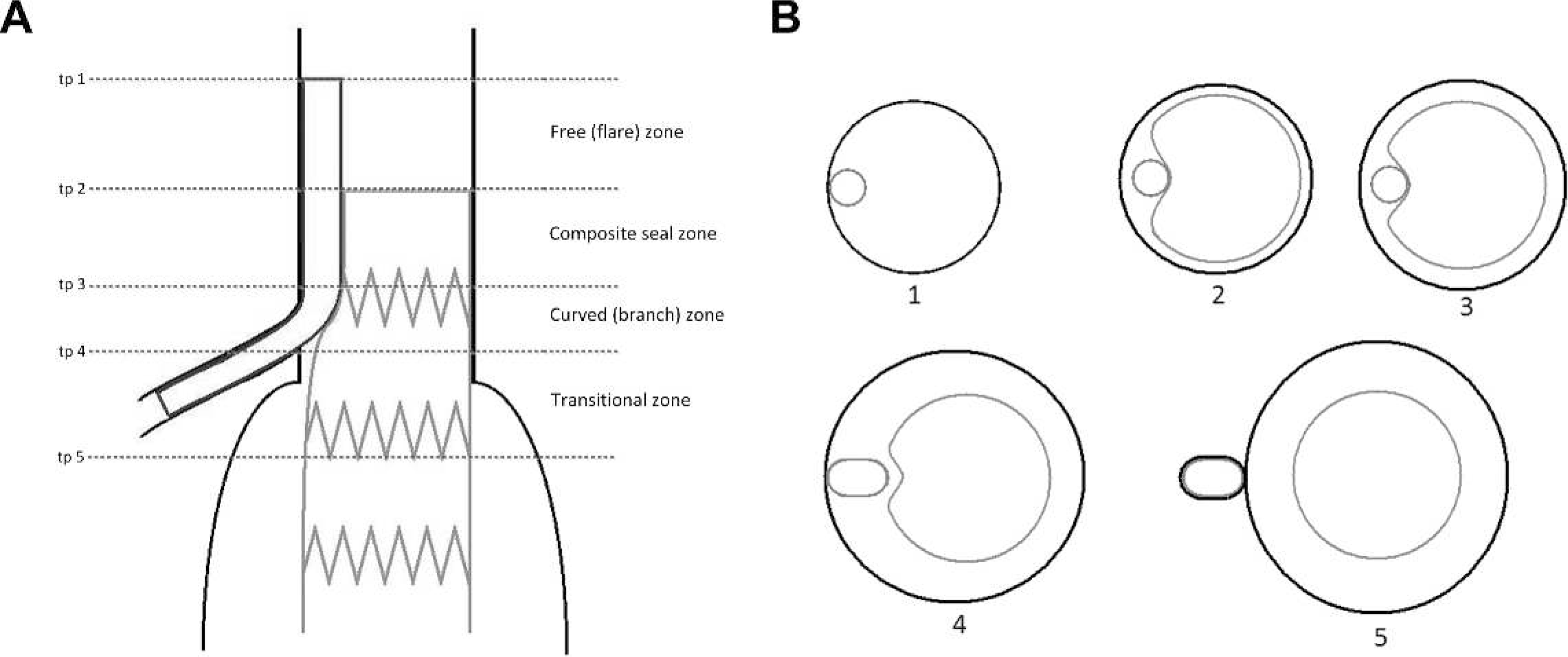
One type of main graft was tested, the Excluder (W.L. Gore & Associates, Inc. Flagstaff, AZ, USA), in combination with 2 types of CGs: the Viabahn self-expanding (SE) stent-graft (W.L. Gore & Associates, Inc.) and the Advanta V12 balloon-expandable (BE) stent-graft (Atrium Medical Corp., Hudson, NH, USA). Two sizes of the BE stent-graft were used (6×59 and 12×61 mm), as well as 2 sizes of the SE stent-graft (6×50 and 13×50 mm). In addition, 2 sizes of the Excluder were used (23 and 28.5 mm). The CG configuration was divided into 4 separate zones, a free (“flare”) zone, a composite seal zone, a curved (“branch”) zone, and a transitional zone (Fig. 2). The length of the free (“flare”) zone was 5 mm in all configurations. The various diameters of stent-grafts in combination with 2 different seal zone lengths (10 and 20 mm) led to 8 different configurations for the SE and BE stent-grafts (total 16 configurations; see the Table)
Different zones of interest including the (
Experimental Setup
For each setup, the main graft and CGs were simultaneously deployed in a single-branched CG configuration. After deployment, the CG and main graft were dilated simultaneously at a pressure of 8 bar (116 psi) for 10 seconds. A compliant balloon was used in the main graft. Immediately after stent-graft deployment, the complete tray (including the aortic model and CG configuration) was placed into a 64-slice computed tomography (CT) scanner (Philips Medical Systems, Inc., Shelton, CT, USA) to determine the geometry of the configuration.
CT Measurements
The main tube (“aorta”), CG, main graft, and gutters were scanned using 2-mm intervals starting 2 mm above the chimney graft configuration and ending 10 mm below the side branch. Cross sections of interest were named after the table positions (tp) and were used in the calculations (Fig. 2). Cross-sectional surface areas of the CGs, main grafts, and the main tubes (“aorta”) were measured at the top and bottom of the seal zone (tp 2 and tp 3) with OsiriX (Pixmeo, Geneva, Switzerland), an image processing software program (Fig. 3).
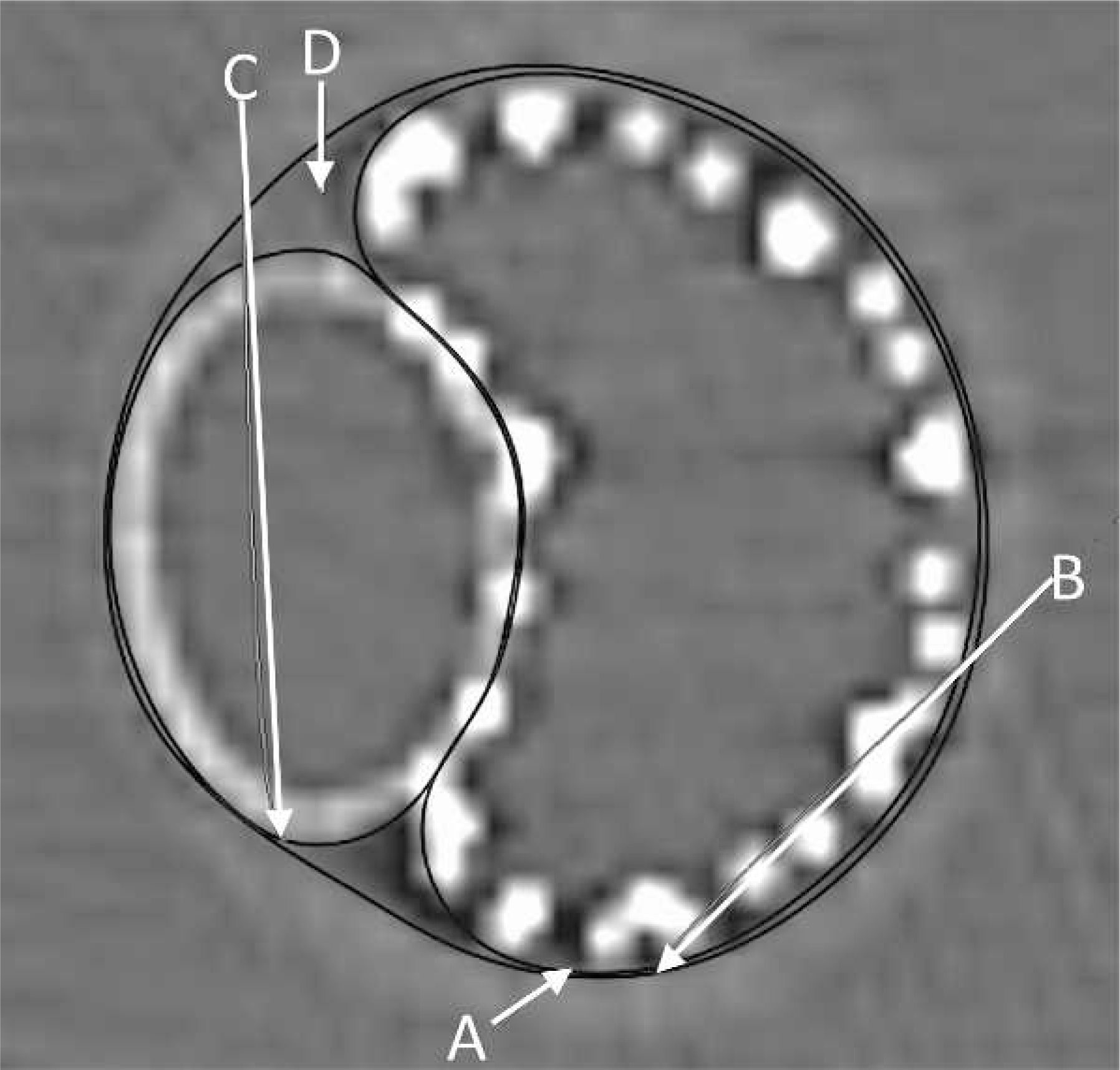
Different cross-sectional areas measured with OsiriX. A: outer perimeter of the main graft, B: inner diameter of the aorta, C: outer perimeter of the chimney graft, and D: gutter.
Measurements of each setup were used to calculate gutter size and main graft compression. Absolute gutter size was calculated by subtracting the areas of the CG and main graft from the aortic areas at tp2 and tp3. Main graft compression was calculated by subtracting the area of the main graft from the aortic area. In addition, main graft compression was calculated relative to the aortic area. To determine maximum chimney graft compression (stenosis), a centerline (Fig. 4) was drawn through the CG to measure the narrowest area and nominal area at the top of the stent (tp 1).
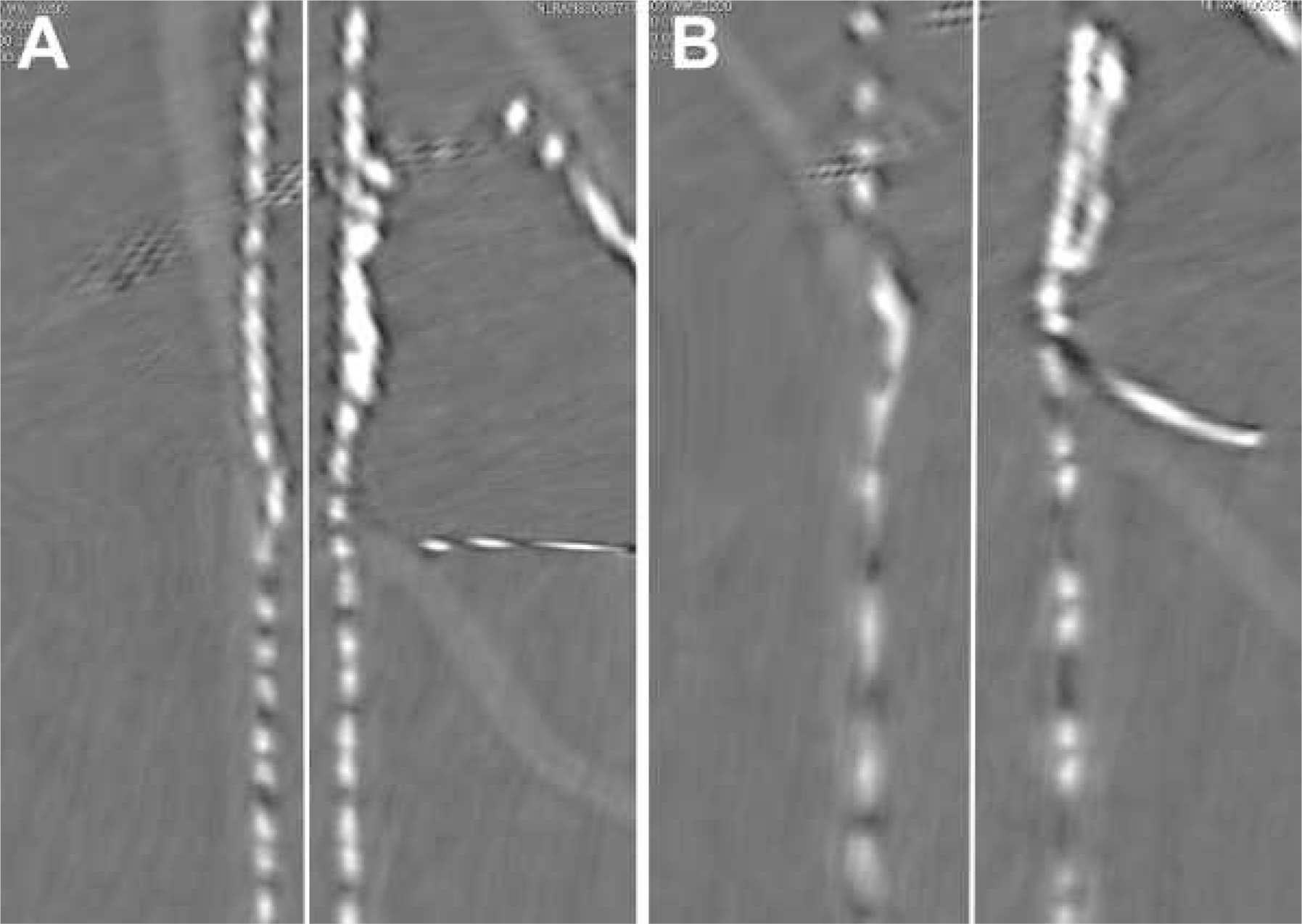
Curved multiplanar reconstructions of a centerline drawn through the
renal CG for the (
Statistical Analysis
Continuous data are presented as median with interquartile range (IQR). Differences in outcome were analyzed using the Mann-Whitney U test. All p-values were 2-sided without correction for multiple testing. P<0.05 was considered to indicate a statistically significant difference. Analyses were performed using SPSS software (version 20.0; IBM Corporation, Somers, NY, USA).
RESULTS
Absolute and relative values for gutter size and compression are enumerated in the Table. At the top of the seal zone (tp 2), the absolute cross-sectional areas of the gutters (Fig. 5) were significantly larger in the BE CG configuration compared to the SE CG configuration in combination with the 23-mm main graft: median 0.39 cm2 (IQR 0.33–0.42) vs. 0.20 cm2 (IQR 0.19–0.21), respectively (p=0.021). At the bottom of the seal zone (tp 3), no significant difference was observed between the cross-sectional areas of the gutters of both graft types (p=0.77). No significant difference in gutter size between both graft types was seen in combination with the 28.5-mm main graft (Fig. 5): SE CG median gutter area 0.29 cm2 (IQR 0.25–0.33) vs. BE CG gutter area 0.61 cm2 (IQR 0.47–0.71), respectively (p=0.083). No significant difference in gutter size existed when comparing the length of the 10 vs. 20-mm sealing zones.
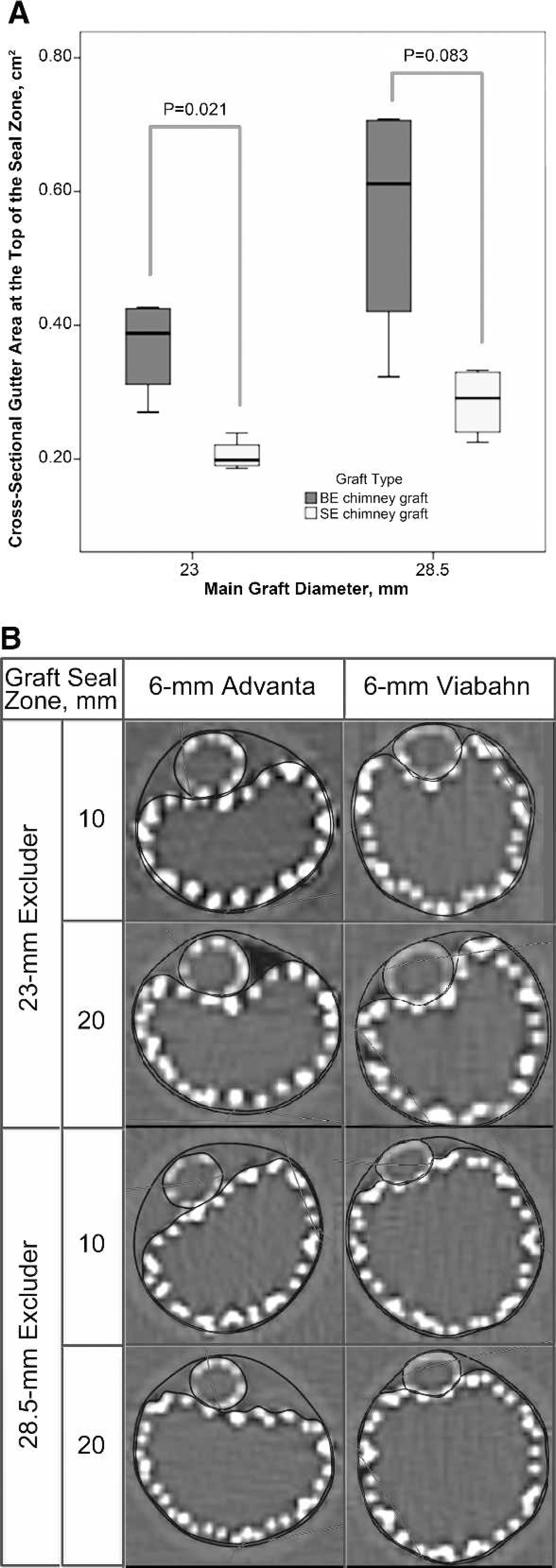
Differences in gutter size at the top of the seal zone between the 6-mm
Viabahn and Advanta stent-grafts are compared in the (
More relative compression of both main grafts was seen using 12 or 13-mm CGs as compared to 6-mm CG (p=0.001) at tp 2 (Fig. 6). The median main graft compression was 42.9% (IQR 36.6%–52.0%) vs. 21.0% (IQR 15.6%–23.6%), respectively. The same difference was seen at tp 3 (p=0.001). Graft type had no influence on relative compression of the main graft.
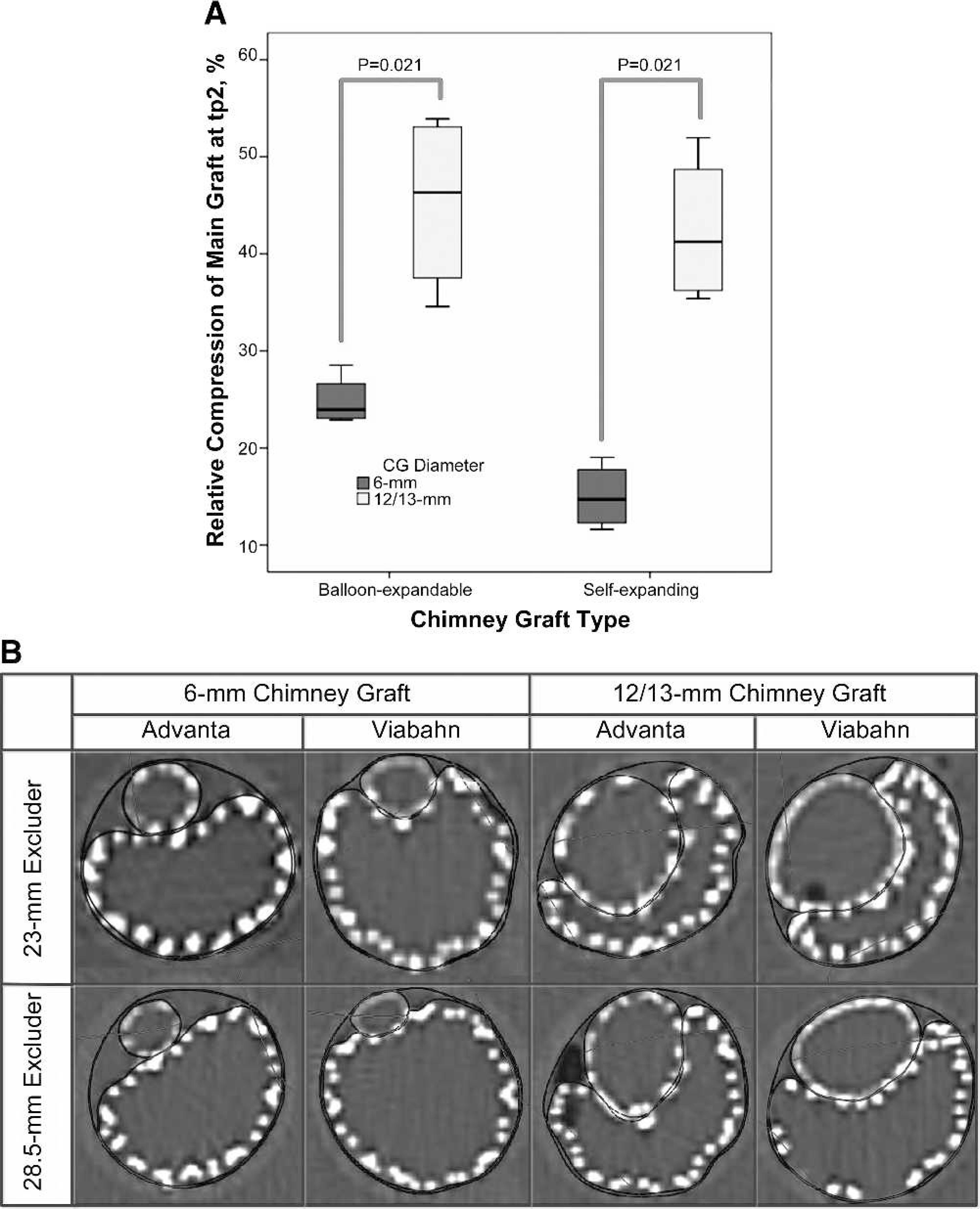
Main graft compression for the 6- and 12/13-mm chimney grafts (Advanta and
Viabahn) in the 10-mm seal zone at table position (tp2) are compared in
(
The difference in main graft compression between 6-mm and 12/13-mm grafts at tp 2 was significant for both graft types (Fig. 6): BE CG (p=0.021) and SE CG (p=0.021). The median compression of the 23-mm main graft with 12/13-mm CGs was 52.1% (IQR 50.3%–52.6%). No significant difference existed between either the BE or SE stent-grafts comparing narrowest diameter on centerline measurement of the CG (p=0.141). The median compression of the CG was 27.4% (IQR 23.1%–32.1%) and 34.4% (IQR 28.9%–37.4%) for the 6-mm and 12/13-mm grafts, respectively. Relative compression of the CG did not exceed 45%. No significant differences in main graft or CG compression existed between the 10 and 20-mm sealing zones.
DISCUSSION
Fenestrated and branched stent-grafts are now being used widely to address the problem of short infrarenal necks. While short- and midterm results show promising results,4,10 long-term renal artery patency is still a concern in a substantial number of patients. The chimney technique also deals with the problem of short infrarenal necks but can be applied in the emergency setting. This technique, also referred to as “snorkel” or “sandwich,” places stent-grafts parallel to a main aortic stent-graft to maintain perfusion to visceral or renal arteries. 7 To our knowledge, no research has been published on the optimal CG configuration in which gutters are smallest.
Results of our study showed clear differences between the two CG models. The SE stent-grafts had small gutters in every setup and were not more compressed than BE stent-grafts. The flexible properties of SE stent-grafts allowed better conformation to the Excluder, which led to the smaller gutters. The large gutters in configurations with the BE CG and small main graft do not support the use of this combination in the chimney technique. By the same token, if a small Excluder were combined with a large CG, regardless of the type, the >50% compression of the main graft renders this configuration unusable.
Limitations
One of the limitations of this study was the use of one type of main graft. There are main grafts with more radial force than the Excluder, and they could have different effects on the geometry of the CG configurations and therefore gutter size. However, in a clinical review by Moulakakis et al., 8 the Excluder stent-graft was used frequently in CG configurations.
Moreover, only 2 types of CG stent-grafts were studied. Other CGs with different physical and mechanical properties could influence the geometry of these configurations. Nonetheless, it should be taken into consideration that the use of several combinations of these stent-grafts led to small gutters and limited compression. Our report focuses on the effect of different types and sizes of CGs on gutter development. Further studies with various types of main grafts are underway.
Flow models could provide us with better insights in flow distribution and gutter leakage in CG configurations. Clot formation could not be tested properly in this in vitro study because gelatin-water was used, so animal studies are needed to analyze clot formation. In addition, research needs to be done on the occurrence of endoleak using our findings.
Conclusion
In this in vitro juxtarenal aneurysm model, self-expanding chimney grafts conformed well to 2 sizes of main grafts. Balloon-expandable chimney grafts led to large gutters when used in combination with relatively small main grafts. In addition, a small main graft in combination with a large (balloon-expandable or self-expanding) stent-graft led to ≥50% main graft compression.