
Abstract
Purpose
To assess the rate of complications associated with the fascia closure technique for femoral access sites in which 18-F or 20-F sheaths were introduced during endovascular aneurysm repair (EVAR).
Methods
A retrospective analysis was done of 50 consecutive patients (41 men; median age 75 years, range 62–85) who received Excluder stent-grafts in planned percutaneous EVAR procedures from May 2006 until December 2009. The fascia closure technique was routinely used for all femoral access sites in which large bore (18-F and 20-F) introducers were employed. One patient with extremely calcified and narrowed vessels was converted to primary cutdown bilaterally after percutaneous access failed. In the 49 remaining patients, 81 femoral access sites were closed with the fascia closure technique; 17 sites with smaller 12-F introducers were closed using other techniques. Computed tomographic angiography (CTA) was performed within 30 days, at 6 months, and at 1, 2, and 3 years.
Results
Of the 81 femoral access sites closed with the fascia closure technique, only 1 patient had persistent bleeding that required an immediate cutdown and suture repair of the deep femoral artery (99.0% technical success rate). In the immediate postoperative period, 5 patients required additional interventions for bleeding (n = 2), occlusion (n = 2), or a pseudoaneurysm [92.6% 30-day technical success]. At 30 days, 11 (13.9%) of 79 access sites had pseudoaneurysms, all of which resolved within a year; none required a secondary intervention. Later surveillance scans did not detect pseudoaneurysms.
Conclusion
The fascia closure technique during EVAR is safe and has few complications. The low frequencies of pseudoaneurysms and other access site complications make the femoral closure technique a durable alternative.
Keywords
Endovascular aneurysm repair (EVAR) became established in the late 1990s, and randomized trials since then have indicated at least a shortterm benefit for EVAR vs. open repair.1,2 Traditionally, vascular access was obtained with a femoral artery cutdown, but a new generation of endoprostheses with smaller delivery systems have facilitated a trend toward a percutaneous approach.3–7 Haas et al. 3 were among the first to investigate a percutaneous closure device in 1999, while Torsello et al. 4 conducted a randomized trial in 2002 comparing a percutaneous suture-mediated closure device (SMCD) vs. an open cutdown. The SMCD reduced both operative time and interval to ambulation. However, heavily calcified and narrow iliac arteries,5,6 along with large bore introducers, 7 have been considered a limiting factor to the percutaneous approach.
See commentary page 397
Diethrich et al. 8 first described the fascia closure technique in 1997, and Larzon and colleagues 9 went on to evaluate the technique as a feasible alternative for closure of large femoral access sites in EVAR. In this study, we investigated the complication rate after the use of the fascia closure technique and also reviewed the incidence of pseudoaneurysms in the groin during follow-up.
METHODS
Patient Population
Our department's prospectively maintained database was interrogated to identify all consecutive patients recruited for EVAR from May 2006 to December 2009. Patients with reduced mental capacity, age <65 years, terminal illness, or chronic kidney failure were excluded, leaving 50 patients (41 men; median age 75 years, range 62–85) for retrospective analysis. All the patients had been screened for cardiovascular and pulmonary disease and were determined to be candidates based on favorable anatomy documented by computed tomographic angiography (CTA). All the patients had elective repairs of intact abdominal aortic aneurysms (AAA) except 1 patient who was treated for ruptured AAA. The fascia closure technique had been routinely used in all femoral access sites where large bore (18-F and 20-F) introducers were employed.
All patients were admitted 1 day prior to the EVAR procedure, which was performed percutaneously with the patients under general (n = 38), regional (n = 9), or local (n = 3) anesthesia. In the preoperative review of the CTAs, the location of the femoral bifurcation had been noted. At the time of access, the common femoral artery (CFA) was found by palpation, and the intended puncture site was between the inguinal ligament and the femoral bifurcation.
The Gore Excluder Endoprosthesis (W.L. Gore & Associates Inc., Flagstaff, AZ, USA) with introducer sheath sizes varying from 12-F to 20-F was used in all patients. One patient with extremely calcified and narrowed vessels was converted to primary cutdown with thromboendarterectomy (TEA) bilaterally after percutaneous access failed. In the 49 remaining patients having percutaneous CFA accesses, 81 had an 18-F or 20-F sheath introduced, and closure was achieved with the fascia closure technique. Seventeen access sites with smaller 12-F introducers were closed according to the physician's choice [9 with the femoral closure technique and 8 with an 8-F AngioSeal VIP vascular closure device (St. Jude Medical, Inc., St. Paul, MN, USA)].
Technique
After completion of the EVAR procedure, the introducer with dilator and guidewire was left in place, and the skin incision at the introducer was extended transversally to a length of between 4 and 8 cm (Fig. 1). Dissection down to but not through the femoral fascia was performed. As detailed and illustrated previously, 9 a single stitch was placed in the fascia beginning 5 to 10 mm away from the introducer sheath at the distal end of the incision using a monofilament polypropylene suture (Prolene 2–0; Ethicon, Johnson & Johnson, Europe). The stitch ran toward the other end of the incision parallel to the artery, but the arterial wall was intentionally not included. At the proximal end of the incision, the suture was taken up and over the skin to the other side of the introducer, run down the other side of the artery in the fascia, and exteriorized at the distal end of the incision. As the introducer was withdrawn, the suture was tightened with a sliding knot. If hemostasis was achieved (technical success), the guidewire was withdrawn, and the suture was further tightened. If bleeding was seen, the introducer was reinserted, allowing additional suturing. Attention was given to not tightening the suture more than required to stop bleeding so as not to cause narrowing of the vessel. If a palpable pulse was identified distal to the suture site, the skin was closed without use of external compression.

Incisional dissection in the groin showing the fascia priorto placement of the fascia suture.
Clinical Follow-up
Clinical follow-up with femoral pulse palpation, measurement of the ankle-brachial index, and routine surveillance CTAs were performed within 30 days, at 6 months, and at 1, 2, and 3 years to evaluate the stent-graft and detect access site-related complications. A groin pseudoaneurysm was defined when contrast was present outside of the true vessel lumen. A pseudoaneurysm <10 mm in maximum depth or width was defined as small, while a large pseudoaneurysm was ≥10 mm. Only the contrast lumen was measured and not the thrombus component of the pseudoaneurysm (Fig. 2). An interventional radiologist and an endovascular surgeon separately reviewed the surveillance scans for this analysis.

A pseudoaneurysm (arrow) from the common femoral artery in the left groin on a 30-day surveillance scan.
RESULTS
Of the 81 femoral access sites closed with the fascia closure technique, only 1 patient had persistent bleeding that required an immediate cutdown and suture repair of the deep femoral artery (DFA), for a 99.0% (80/81) technical success rate. The mean blood loss recorded for the 49 patients was 362 mL (range 100–4000) during procedures that lasted a mean 121 minutes (74–207). Thirty-five (70%) patients returned to the general surgical ward after 6 hours of observation on the recovery ward. Thirteen (26%) patients spent 1 night on the recovery ward, while only 1 stayed there for 2 days. The mean length of the hospital stay was 4.8 days (2–13).
The 30-day technical success rate was 92.6% (75/81). Postoperatively, 1 patient required a secondary cutdown and suture of the CFA the same day due to bleeding (Table). Several hours postoperatively, another patient required a second procedure for bilateral occlusions in the CFA, with TEA and patch angioplasty repair. A third patient required a secondary cutdown and a TEA and patch angioplasty repair due to occlusion on the third postoperative day. Another patient developed a large pseudoaneurysm measuring 3×5 cm that was treated with ultrasound-guided thrombin injection on the fifth postoperative day.
Early Complications After Fascia Closure in 5 Patients
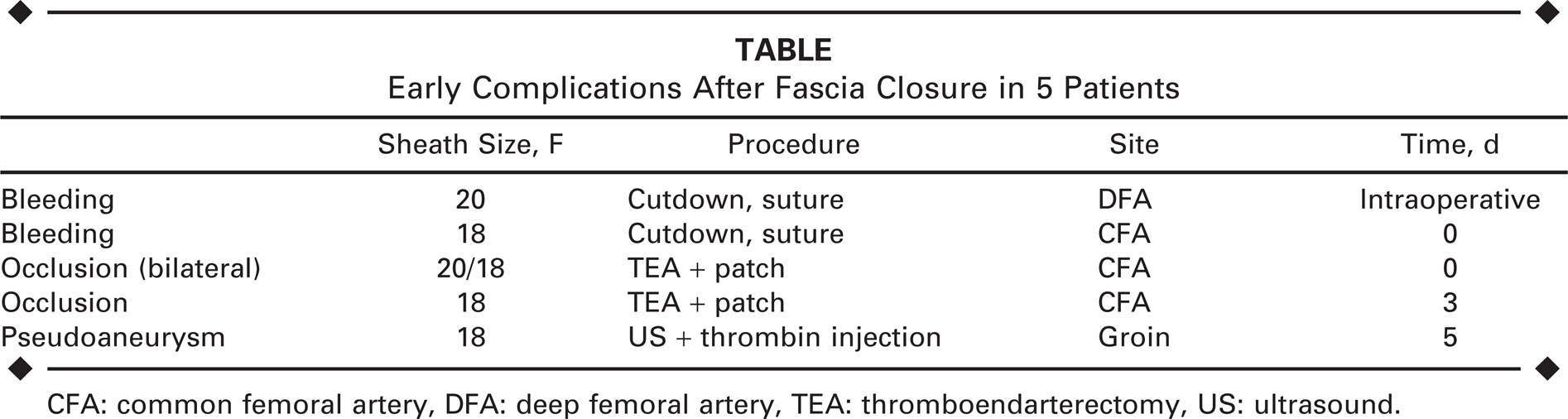
CFA: common femoral artery, DFA: deep femoral artery, TEA: thromboendarterectomy, US: ultrasound.
One patient succumbed 12 hours postoperatively due to plaque rupture of the proximal abdominal aortic neck where balloon dilation had been used to remodel the stent-graft. This left 79 access sites available for the 30-day surveillance scans. In all, 11 (13.9%) access sites had a small pseudoaneurysm. Eight of these sealed spontaneously by the 6-month examination; the remaining 3 were resolved by 1 year. None of the pseudoaneurysms detected during follow-up needed a secondary intervention. No other access-related complications were detected during the observation period. Surgical conversion with removal of an infected stent-graft and replacement with an extra-anatomical axillobifemoral bypass was performed in 1 patient after 3 months due to spondylitis. Another patient had an occluded superficial femoral artery that was not considered access-related; 1 year postoperatively, percutaneous transluminal angioplasty was attempted without success.
In addition to the early postoperative death, 6 patients died during the study period from myocardial infarction (n = 2), lung cancer, chronic obstructive pulmonary disease, acute myeloid leukemia, and an unknown cause.
DISCUSSION
Percutaneous access for endovascular AAA repair has the potential to reduce operative time, blood loss, intensive care unit stay, and length of hospitalization.4,5,10 Groin complications, such as scarring, lymphatic leakage, and wound infections, might also be reduced with a percutaneous technique.10,11 In addition, reoperations may be facilitated as a result of less scar tissue formation. 12 On the other hand, a number of vascular complications at the puncture site can occur, such as bleeding, thrombosis, and pseudoaneurysm formation. 11
Our study has confirmed the technical feasibility and high early technical success rates (86% to 91%) previously reported with the fascia closure technique.9,13,14 However, a limitation of previous studies is that they have been conducted in selected patient groups. Harrison et al. 13 reviewed their results using the fascia closure technique in patients undergoing EVAR using devices up to 24 F. Exclusion criteria were morbid obesity, high DFA bifurcation, previous groin surgery, inadvertent high puncture, arteries <5 mm in diameter, and surgeon preference. Larzon and colleagues 9 included just 51% (131/257) of the femoral arteries used for access in their EVAR cohort. Most recently, Montan et al. 14 had no anatomical exclusion criteria in their 100-patient study of the fascia closure technique, but this study was limited by the fact that 55% of the patients had an external compression system to complement hemostasis.
There are many studies of percutaneous EVAR in which SMCDs have been used, and the results compare well with the fascia closure technique. 15 However, many of these studies have reported exclusion criteria, such as vessel calcification, obesity, and scarred groins. The strength of our study is that we have included all large-bore puncture sites and used the fascia closure technique as sole treatment.
We had 2 access sites in which primary cutdown was required due to puncture problems related to extreme calcification. Otherwise, we routinely used the fascia closure technique in all femoral access sites having ≥18-F introducer sheaths. Regular surveillance scans have documented the low frequency of pseudoaneurysms, which resolved within a year in all cases. Our few late complications compare well with previous studies of this closure method.9,13,14
The fascia closure technique seals the CFA puncture site without suturing the vessel wall, which might be advantageous when the artery is heavily calcified. The fascia closure technique is also applicable in an emergency situation, such as ruptured AAA.9,14 It is an easy technique to learn; in this series, the technique was performed under direct supervision during the first 9 cases (18 accesses), which is an indication that the expected learning curve is quite short. Our team has always included an interventional radiologist and an experienced vascular surgeon, which might have had a positive effect on the outcome, even though the dissection and suture technique is rather basic.
The fascia closure technique does have some limitations. Not all patients have an anatomically distinct femoral fascia, especially on the medial side. Weakness of the femoral fascia can cause leakage and difficulty with suture sealing. It is also important to get an optimal puncture site below the inguinal ligament and above the femoral bifurcation. A puncture above the inguinal ligament will make the femoral closure less effective, as the femoral fascia does not cover the femoral artery wall, and retroperitoneal bleeding may ensue. A low puncture in the DFA might also face the same problem and cause hemorrhage in the groin. One patient in our series had persistent bleeding that required an immediate cutdown and suture repair of the DFA.
A way to improve the results of the fascia closure technique is to optimize the puncture. One way is to use a micropuncture technique and control the puncture site with angiography in a lateral oblique projection; if the approach is not good, be prepared to do another puncture. Another way is to use ultrasound to locate the optimal puncture site of the CFA. This guarantees proper anatomical placement and helps find and avoid extreme arterial wall calcification.
Economically, the fascia closure technique should be less expensive than an SMCD as long as complication rates are low level and outcome comparable with the SMCD.
Conclusion
The fascia closure technique during EVAR is safe and has few complications. The technique is applicable in all patients, even emergency procedures. The few failures that may occur due to bleeding or occlusion can easily be managed with an open surgical cutdown. The low frequencies of pseudoaneurysm formation and late adverse events make the femoral closure technique a durable alternative.