
Abstract
Purpose
To describe advanced retrograde access (transmetatarsal or transplantar arch) for endovascular treatment of critical limb ischemia (CLI) and foot salvage.
Methods
From September 2011 to March 2012, 28 CLI patients (24 men; mean age 71.9±10.6 years) being treated for foot salvage had failed antegrade recanalization, and percutaneous retrograde access at the pedal or plantar artery was unavailable. Advanced retrograde access techniques were required to recanalize the target vessel to restore blood flow to the compromised tissue. After local administration of verapamil to control spasm, the first dorsal metatarsal artery was preferentially accessed with a 21-G needle. When the first metatarsal artery was occluded and not fluoroscopically viewable, the plantar arch was punctured directly. After puncture, a 0.018- or 0.014-inch guidewire and microsheath were inserted for retrograde recanalization of the foot and tibial arteries with balloons sized to the target vessels.
Results
Retrograde transmetatarsal artery access was performed in 25 cases and direct transplantar arch access in 3. Technical success (ability to deliver the balloon across the lesion and inflate it at nominal pressure) was achieved in 24 (86%) cases, with <50% residual stenosis and no complications. The 4 technical failures were due to spasm or no true lumen re-entry after successful transmetatarsal (n=3) and transplantar arch access. During a mean 5-month follow-up (range 1–8), clinical improvement was obtained in the patients having technically successful tibial and foot artery recanalization; the transcutaneous pressure improved from 12.5±6.7 to 49.8±9.5 mmHg. There were no major and only 8 minor amputations. Amputation-free survival estimated by Kaplan-Meier analysis was 71% at 6 months. In patients with failed advanced access, the clinical condition did not improve.
Conclusion
The advanced retrograde access technique appears feasible and beneficial as a rescue strategy in challenging patients with a failed antegrade approach who are unsuitable for retrograde pedal/plantar access.
Keywords
Revascularization is the first-line treatment of critical limb ischemia (CLI) to relieve rest pain and improve wound healing. 1 In recent years, there has been growing acceptance of endovascular therapy as a primary therapeutic strategy for infrapopliteal lesions and CLI, especially in patients at high risk for or with contraindications to surgical revascularization.2–7 In daily interventional practice, challenging cases are encountered in which innovative technical strategies are required to restore blood flow to the foot when standard technical solutions fail. In our experience, 8 when antegrade recanalization fails, retrograde revascularization and the SAFARI (subintimal arterial flossing with antegrade-retrograde intervention) technique are considered.9–12 However, in a few cases, the pedal or plantar arteries13,14 are not available or feasible for puncture due to chronic occlusion. In this situation, an advanced retrograde access can help achieve both technical and clinical success. In a recent article, we described the retrograde transmetatarsal access. 15 We now evaluate this advanced access technique for foot salvage in the setting of CLI.
See commentary page 812
METHODS
Patient Population
From September 2011 to March 2012, 507 consecutive patients with lower limb CLI (Rutherford category 5/6, TcPO2 ≤30 mmHg 1 ) due to atherosclerosis underwent endovascular recanalization at our center. Of these, 28 (5%) patients (24 men; mean age 71.9±10.6 years) had failed antegrade recanalization, and percutaneous retrograde access at the pedal or plantar artery was unavailable. Advanced retrograde access techniques were required to recanalize the target vessel identified according to the wound-related artery concept 16 to restore direct blood flow to the compromised tissue. All patients gave written informed consent, and the retrospective study was conducted in accord with the local ethics committee rules. Demographics, comorbidities, and clinical conditions are summarized in Table 1.
Demographics, Comorbidities, and Clinical Conditions of 28 Patients
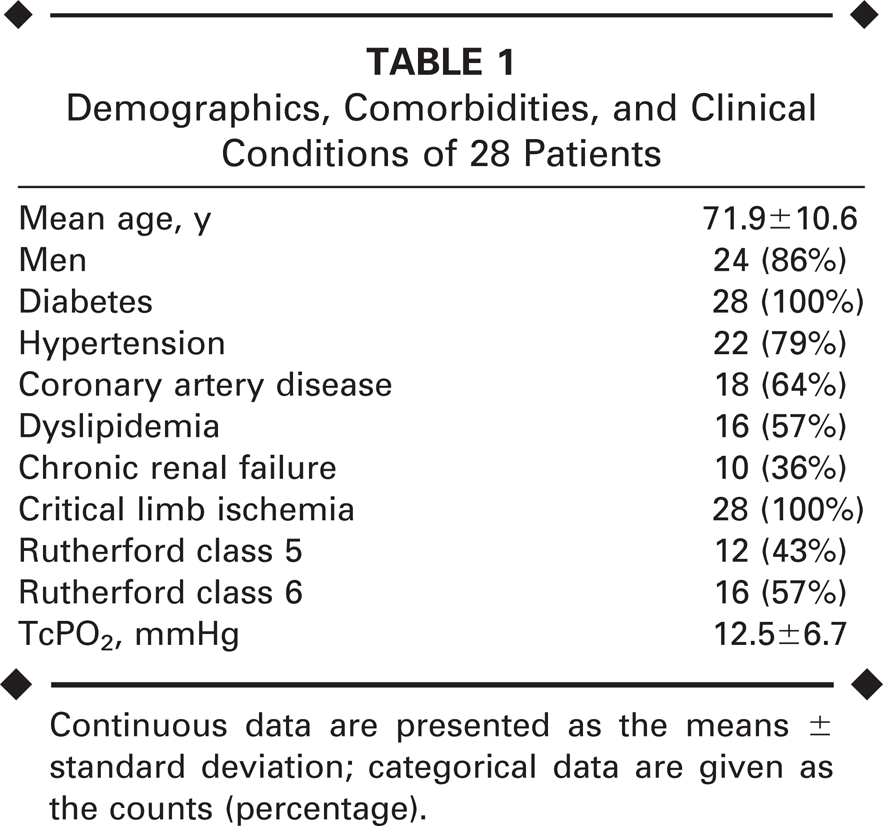
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
Endovascular Treatment
All patients have a noninvasive diagnostic study prior the invasive procedure to exclude any aortic or iliac inflow disease. Three days before of the procedure, the patients are pre-treated with aspirin (75 to 160 mg), ticlopidine (500 mg), or clopidogrel (300 mg).
With the patient under local anesthesia, an antegrade access to a common femoral artery is obtained under ultrasound guidance (7.5-MHz linear probe), and a 5-F, 10-cm-long sheath is deployed. Five thousand units of unfractionated heparin are administered. Angiography is performed to document infrapopliteal occlusive disease. If attempts to recanalize the tibial and foot arteries via the antegrade access are unsuccessful and the anterior and posterior tibial arteries and/or pedal/plantar arteries are occluded, then the transmetatarsal (Fig. 1) or transplantar arch (Fig. 2) access route is considered.
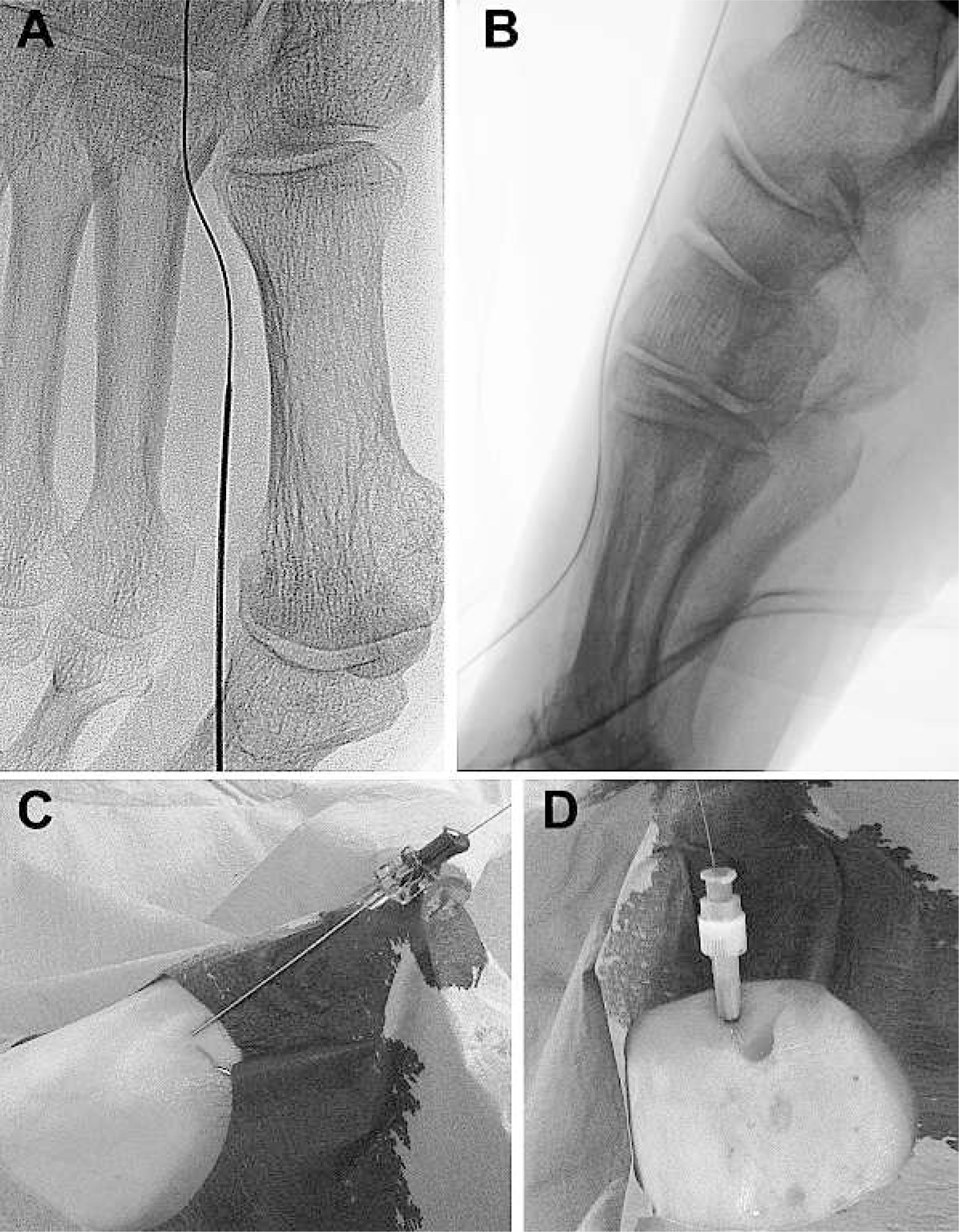
Retrograde percutaneous transmetatarsal (digital) artery access in the
anteroposterior (
Retrograde transplantar arch puncture in the anteroposterior
(
In this approach, pharmacological support is mandatory to avoid spasm that can compromise the puncture and navigation of these small vessels. For this, 5 mg/2 mL of verapamil (Isoptin; Abbott S.p.A, Campoverde, Italy) is diluted to 10 mL with saline, and 9 mL of this solution is injected intra-arterially as distal as possible, close to the foot. Local anesthesia is administered close to the target area, and 1 mL of the diluted verapamil together with lidocaine is injected into the subcutaneous tissue to avoid spasm. This pharmacological support guarantees good preparation of the puncture site.
In selecting the access vessel, if the first dorsal metatarsal artery is patent or has wall calcification visualized on fluoroscopy if occluded, it is the preferred option for retrograde access in our experience. Via this access, it is usually possible to reach the plantar arch or loop, through which the pedal artery or lateral plantar artery can be recanalized. When the first metatarsal artery is occluded and not viewable, the second possible access site is through direct puncture of the plantar arch under fluoroscopic guidance with contrast injection and at maximum magnification to identify the target vessel. When the access vessel is occluded or without flow, puncture can be performed using the wall calcification as a guide.
For either route, a micropuncture introducer set (Cook Medical, Bloomington, IN, USA) composed of a long 21-G needle, a dedicated torque-flex 0.018-inch guidewire, and microsheath is useful for gaining access and minimizing wall vessel trauma. If the target vessel is smaller than usual, a 0.014-inch guidewire [Pilot 200 (Abbott) or Approach Hydro ST (Cook)] can be used.
After access creation and sheath deployment in the target vessel, retrograde recanalization of the foot and tibial arteries is performed, usually using a 0.018-inch guidewire (V18; Boston Scientific Corp., Natick, MA, USA) and support catheter (CXI; Cook). For dilation, the balloons are sized by visually estimating the distal reference vessel diameter, as well as the target lesion; as a general rule, the balloons used for metatarsal branch recanalization are 1.5 or 2.0 mm in diameter; for the plantar arch, the diameter is 2.0 or 2.5 mm. They are delivered via the antegrade access and inflated for 1 minute at nominal pressure.
After the procedure, aspirin is continued indefinitely 8 and ticlopidine or clopidogrel is continued for 3 months. After discharge, clinical follow-up is routinely performed at 1 month and then at 3-month intervals.
RESULTS
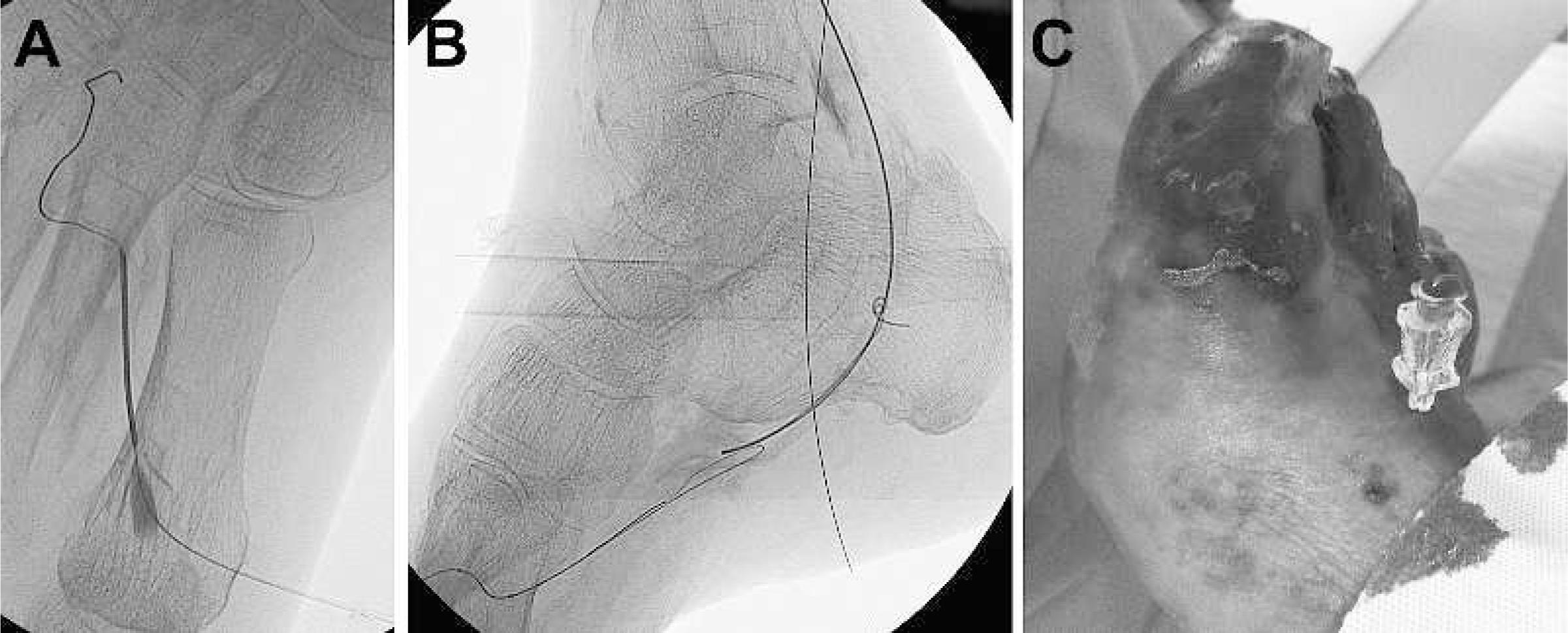
Retrograde transmetatarsal artery access was performed in 25 cases and direct transplantar arch access in 3 patients in whom the first dorsal metatarsal artery was occluded and not calcified. Technical success (ability to deliver the balloon across the lesion and inflate it at nominal pressure) was achieved in 24 (86%) of 28 cases, with adequate angiographic results (<50% residual diameter stenosis) and no complications (Figs. 3 and 4). The 4 technical failures were due to spasm or no true lumen re-entry after successful transmetatarsal (n=3) and transplantar arch (n=1) access. Technical results and lesion location are summarized in Table 2.
Technical Results
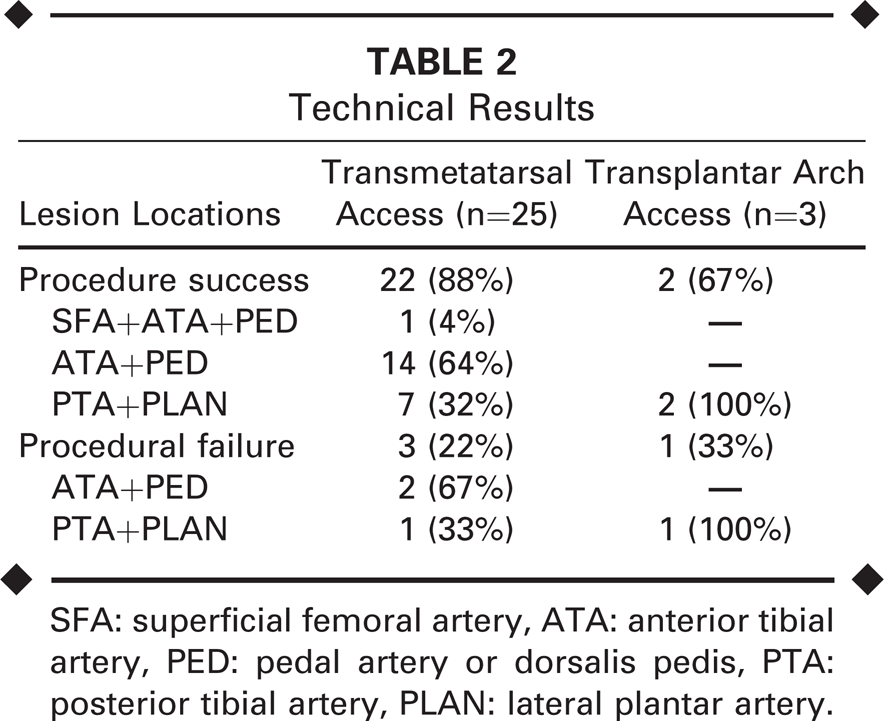
SFA: superficial femoral artery, ATA: anterior tibial artery, PED: pedal artery or dorsalis pedis, PTA: posterior tibial artery, PLAN: lateral plantar artery.

(
During a mean 5.3±1.9-month follow-up (range 1–8), clinical improvement was obtained in the patients having technically successful tibial and foot artery recanalization, with a significant TcPO2 improvement from 12.5±6.7 to 49.8±9.5 mmHg. In this population at high risk of amputation, 2 patients underwent transmetatarsal amputation after endovascular treatment, with good clinical results in terms of surgical incision healing; 6 patients had phalange or toe amputations. No major amputations were performed in the entire cohort (limb salvage 100%); healed lesions and plantar stand were maintained despite the minor tarsal-metatarsal amputations. 17 Amputation-free survival estimated by Kaplan-Meier analysis was 71% at 6 months (Fig. 5). The patients with technical failure did not have clinical improvement and underwent minor amputations.
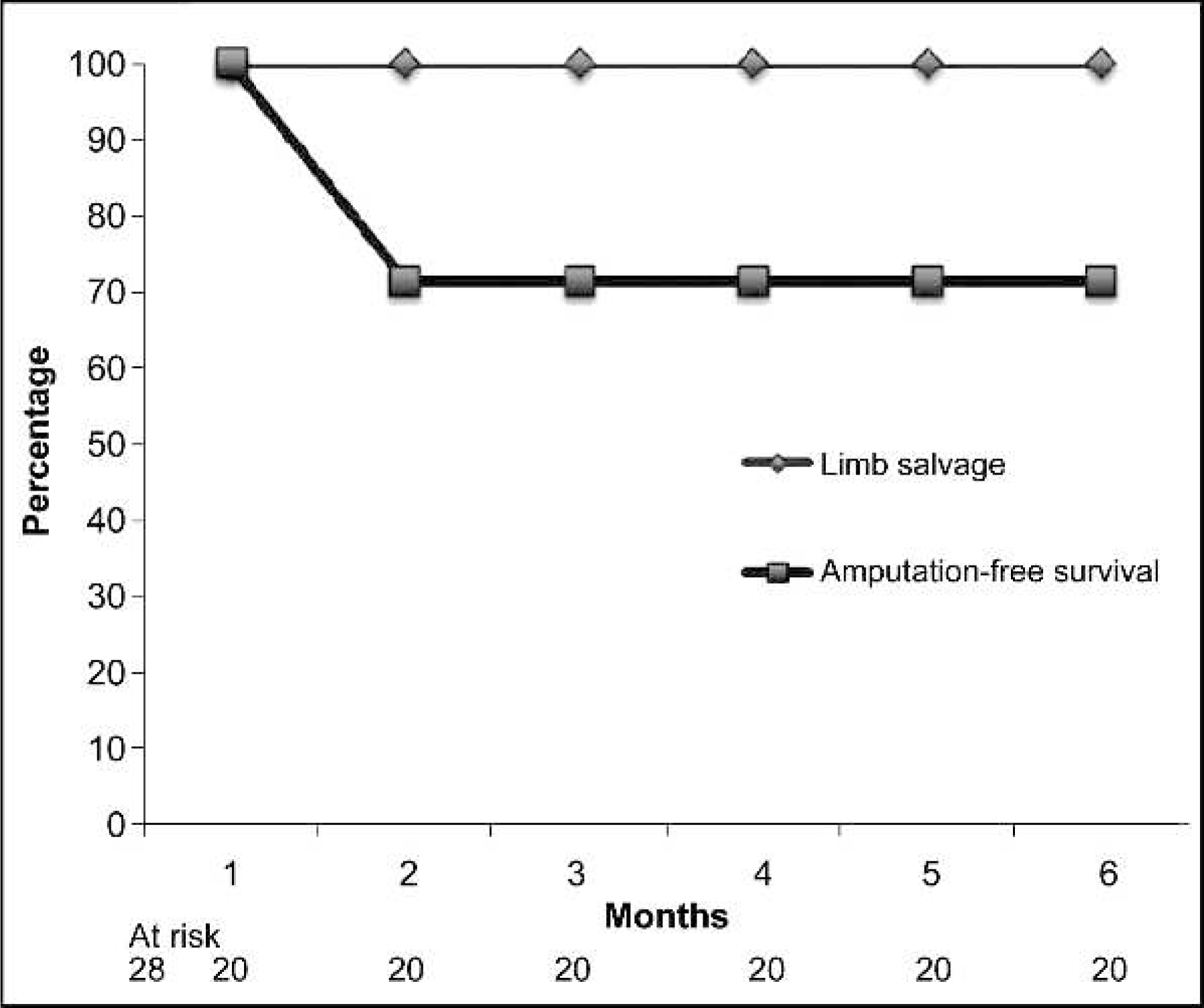
Limb salvage and amputation-free survival rates estimated by Kaplan-Meier analysis.

In the patient from Figure
3, percutaneous retrograde access in the first metatarsal artery
with (
DISCUSSION
Since its initial application, endovascular recanalization of tibial and foot arteries has become particularly useful in diabetic patients with CLI.2–5,8,15,18–20 Nevertheless, a small percentage of cases conclude with poor technical results or failure to cross the lesion or re-enter the true lumen during subintimal recanalization. In these cases in which surgical revascularization is not feasible, it is necessary to find new solutions to guarantee successful recanalization. 15 Retrograde percutaneous access has been described as a solution for re-entry in cases of subintimal recanalization.9–14
When the tibial or pedal arteries are not available for puncture, retrograde percutaneous transmetatarsal artery access or direct puncture of the plantar arch are useful alternatives to retrograde recanalization of foot and tibial vessels. These maneuvers can improve both technical and clinical results for nonsurgical candidates in whom all other percutaneous access routes have failed or are unavailable. 15
Our results show that advanced access may be of particular value as a rescue technique in cases in which retrograde percutaneous puncture leads to dissection and acute occlusion. A case in point was one of our transmetatarsal artery access cases. The patient had occluded anterior and posterior tibial arteries with a patent pedal artery. Subintimal recanalization of the anterior tibial artery was attempted but re-entry to the pedal artery failed. Subsequently, retrograde recanalization was attempted via a very thin pedal artery. In the process of accessing the vessel, dissection and acute occlusion occurred. The last technical solution was transmetatarsal artery access, which solved the access problem and facilitated recanalization of the target vessel, with good technical and clinical results.
This approach strategy is minimally invasive, and the risks to the patient are very low. In our opinion, this strategy should also be considered in cases in which foot perfusion is maintained by very slow flow through thin pedal or plantar arteries. Attempts to puncture these tiny vessels could carry a high risk of dissection and worsening of ischemia. The risk of retrograde transmetatarsal artery access is lower because acute occlusion of the metatarsal artery involves only one toe and not the entire foot. In our experience, dissection never occurred during access of the metatarsal artery.
Despite the usefulness of this retrograde advanced access technique, it is not free from the risk of failure or complications. In this small cohort, almost 15% of the retrograde advanced accesses failed due to spasm or no re-entry in the true lumen. In our first case, for example, after guidewire deployment through the first metatarsal artery and the plantar arch, it proved impossible to advance or retrieve the guidewire; it was necessary to wait 20 minutes to remove it. Another challenge for the interventionist is the radiation exposure. 21
Conclusion
In our experience, retrograde percutaneous transmetatarsal or transplantar arch access is feasible and safe for retrograde recanalization. These access routes are reserved for extremely challenging cases in which surgical revascularization is infeasible or contraindicated, endovascular antegrade access has failed, and retrograde access into the pedal or plantar artery is not possible.