
Abstract
Purpose
To assess the safety and efficacy of the sandwich technique for complex aortic aneurysms.
Methods
Between October 2008 and March 2012, 78 patients (70 men; mean age 73.3 years) undergoing complex thoracic or abdominal endovascular aneurysm repairs were treated with the sandwich technique when the aneurysm features did not fulfill the requirements for standard endovascular techniques or total aortic arch replacement. Two thirds of the population was treated for aortoiliac aneurysm (52, 66.7%). There were 15 (19.2%) thoracoabdominal aneurysms, 6 (7.7%) isolated iliac artery aneurysms, 3 (3.8%) arch aneurysms, and 2 (2.6%) abdominal aortic aneurysm with non-diseased, short common iliac arteries bilaterally. Five (6.4%) symptomatic patients were submitted to endovascular repair in the urgent setting.
Results
Technical success was 98.7%; one procedure was aborted when both renal arteries could not be cannulated. Over a mean 17-month follow-up (range 1–42), primary patency was high (96.7%) and mortality low (early: 5.1%, late: 1.3%). Overall, only 4 (5.1%) type II endoleaks persisted: 3 early with no sac increase and 1 late with sac increase that was managed conservatively on patient demand (stable at 9 months). In all other aneurysms except the 3 in the arch, there was a 5-mm reduction in size achieved by the end of the second year of follow-up, though this was significant only in the aortoiliac aneurysm group (p<0.005).
Conclusion
The sandwich technique facilitates safe and effective aneurysm exclusion and target vessel revascularization in adverse anatomical scenarios, with sustained durability in midterm follow-up.
Keywords
Aortic aneurysm disease is a world health problem of great magnitude and considerable economic burden, with rising incidence and prevalence rates. Endovascular aneurysm repair (EVAR) is currently recognized as the first-line treatment for abdominal aortic aneurysms (AAA) due to decreased operative mortality/morbidity and shorter patient recovery times. In the thoracic aorta, thoracic endovascular aortic repair (TEVAR) is also gaining acceptance as a valid treatment option for thoracic aortic aneurysm.
Despite great technical and device improvement in the last 2 decades, complex aortic aneurysm disease, as represented by aortoiliac (AIA) and isolated iliac artery aneurysms (IAA), as well as aortic arch (AcA) and thoracoabdominal aortic (TAAA) aneurysms, still presents technical challenges not completely overcome by either open surgery or currently available endovascular techniques. AIA and isolated IAA extending to the internal iliac artery (IIA) require a more demanding procedure owing to the difficulties in obtaining an adequate distal landing zone for the stent-graft limb(s), a potential site for endoleak. Another difficult scenario is AAA associated with shorter common iliac arteries (CIAs) because secure distal fixation of a bifurcated stent-graft requires a long and healthy segment of CIA. Extending the iliac limbs of the stent-graft past the IIA origin to provide a secure seal can be done in these cases, but bilateral IIA occlusion is problematic in 12% to 45% of cases. 1 Patients deemed unfit for surgical or standard endovascular management are subject to unfavorable outcomes according to their aneurysm type and size.
The sandwich technique, first introduced in 2008, 2 is an endovascular approach developed to overcome current anatomical and device constraints, expanding the limits of endovascular aneurysm repair. We review the technical steps for 4 types of complex aortic aneurysms and analyze the midterm results of our single-center experience with this technique.
METHODS
Study Design
A prospective study was conducted of all consecutive patients undergoing endovascular repair of complex aortic aneurysms with the sandwich technique at our institution between October 2008 and March 2012. Patients were eligible for the sandwich technique if the aortic aneurysm did not meet the requirements for standard EVAR or TEVAR or total aortic arch replacement. Inclusion criteria were mainly anatomical. A stepwise, fully illustrated description of the sandwich technique as applied in the treatment of these types of aneurysms is provided in the designated figures.
AcA (Fig. 1): (1) ascending aorta proximal neck at least 30 mm long with a maximal diameter not to exceed 40 mm; (2) supra-aortic trunks at least 30 mm long with a maximal diameter no larger than 12 mm.
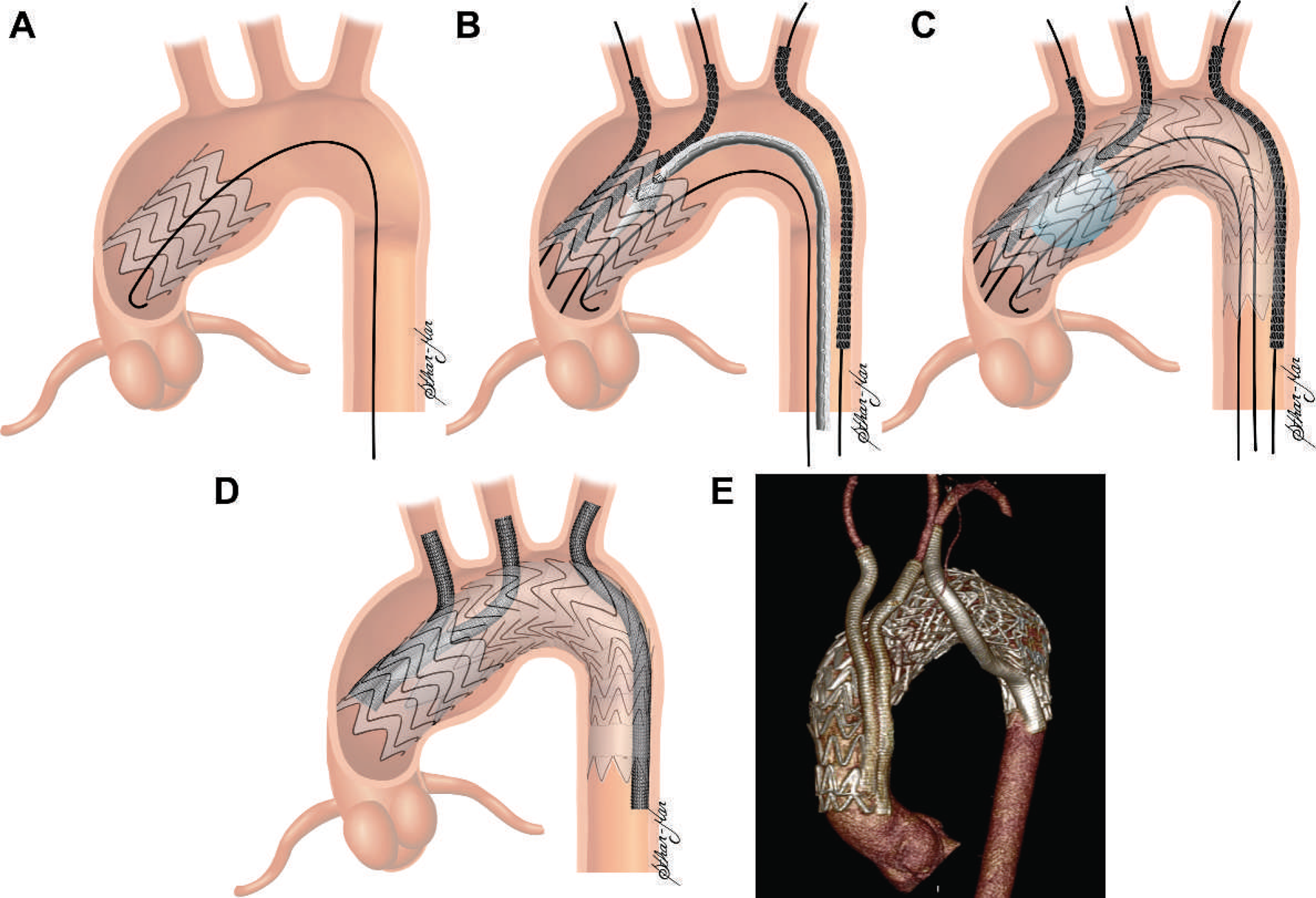
Sandwich technique for an arch aneurysm. (
TAAA (Fig. 2): (1) descending thoracic aorta proximal neck at least 20 mm long with a maximal diameter of 40 mm; (2) internal diameter of the visceral arteries at least 5 mm; (3) proximal end of the superior mesenteric artery (SMA) with at least 20 mm free of side branches.
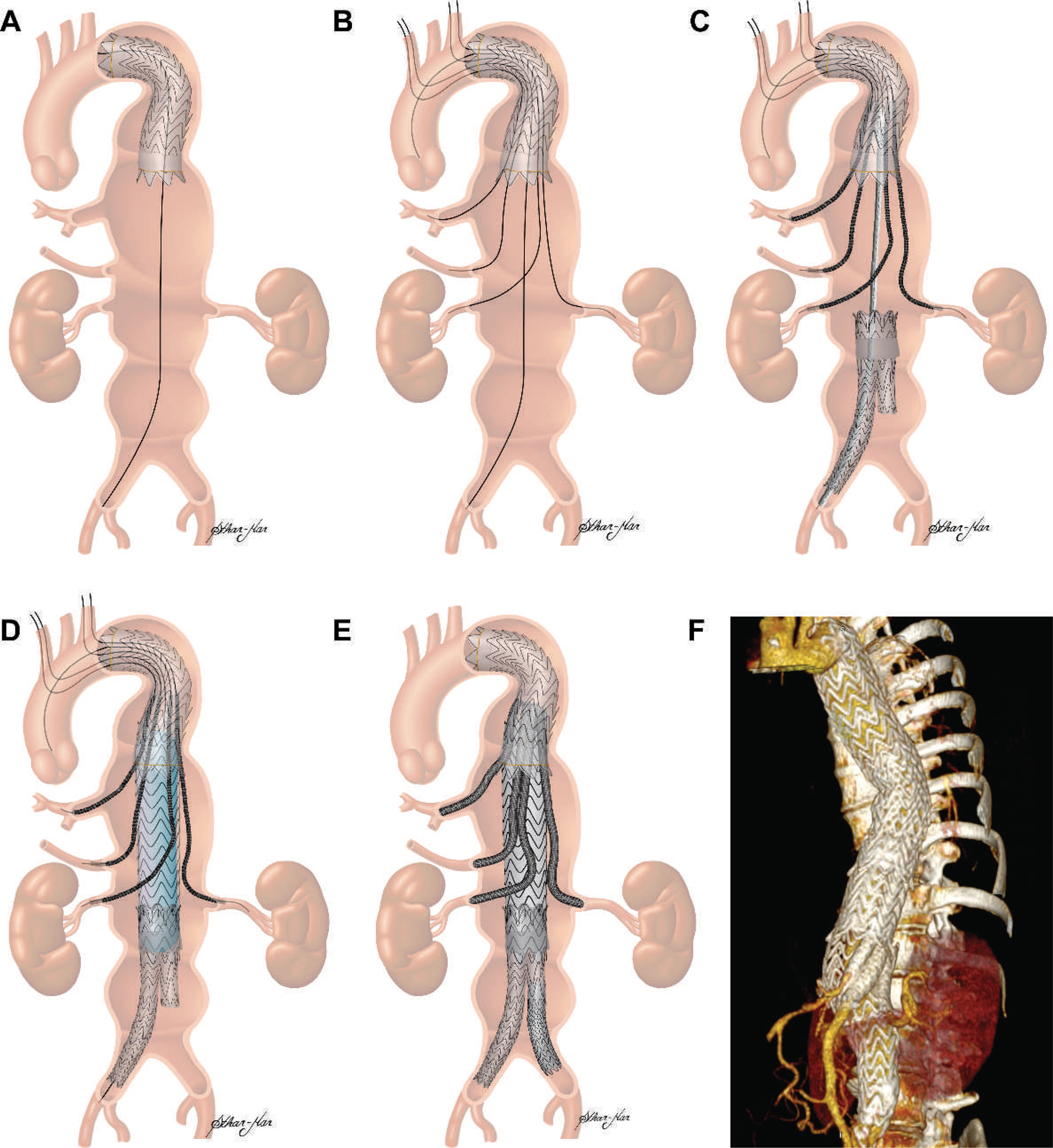
Sandwich technique for a TAAA. (
AIA (Fig. 3): (1) no distal landing zone bilaterally (CIAs); (2) no unilateral distal landing zone (CIA) plus contralateral IIA with aneurysm or previous occlusion/severe stenosis; (3) AAA with short, healthy CIAs (no distal landing zone bilaterally).
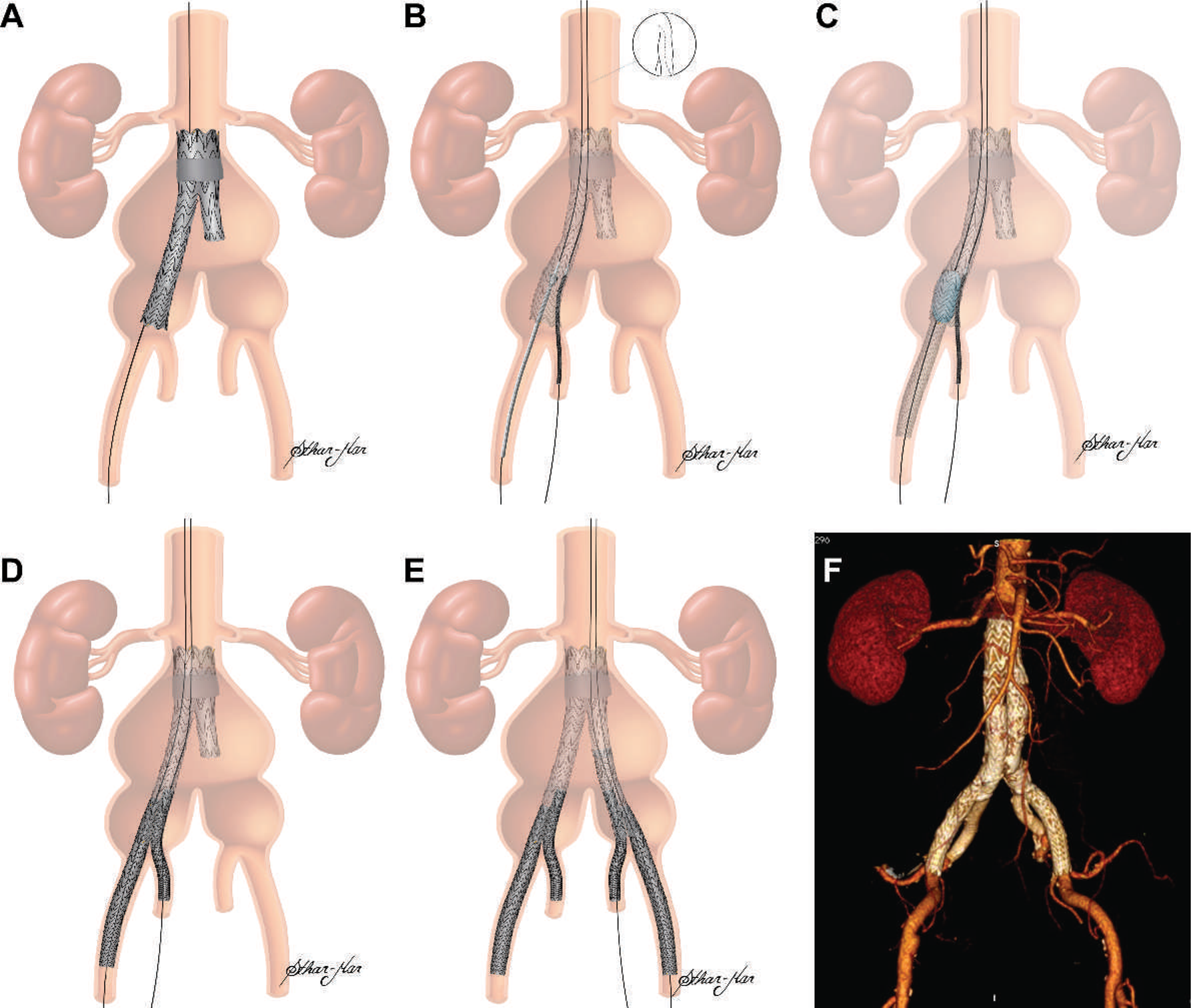
Sandwich technique for an aortoiliac aneurysm extending to the internal
iliac artery (IIA). (
Isolated IAA (Fig. 4): (1) no distal landing zone bilaterally (CIAs); (2) unilateral isolated IAA with no unilateral distal landing zone (CIA) plus a contralateral IIA with aneurysm or previous occlusion/severe stenosis.
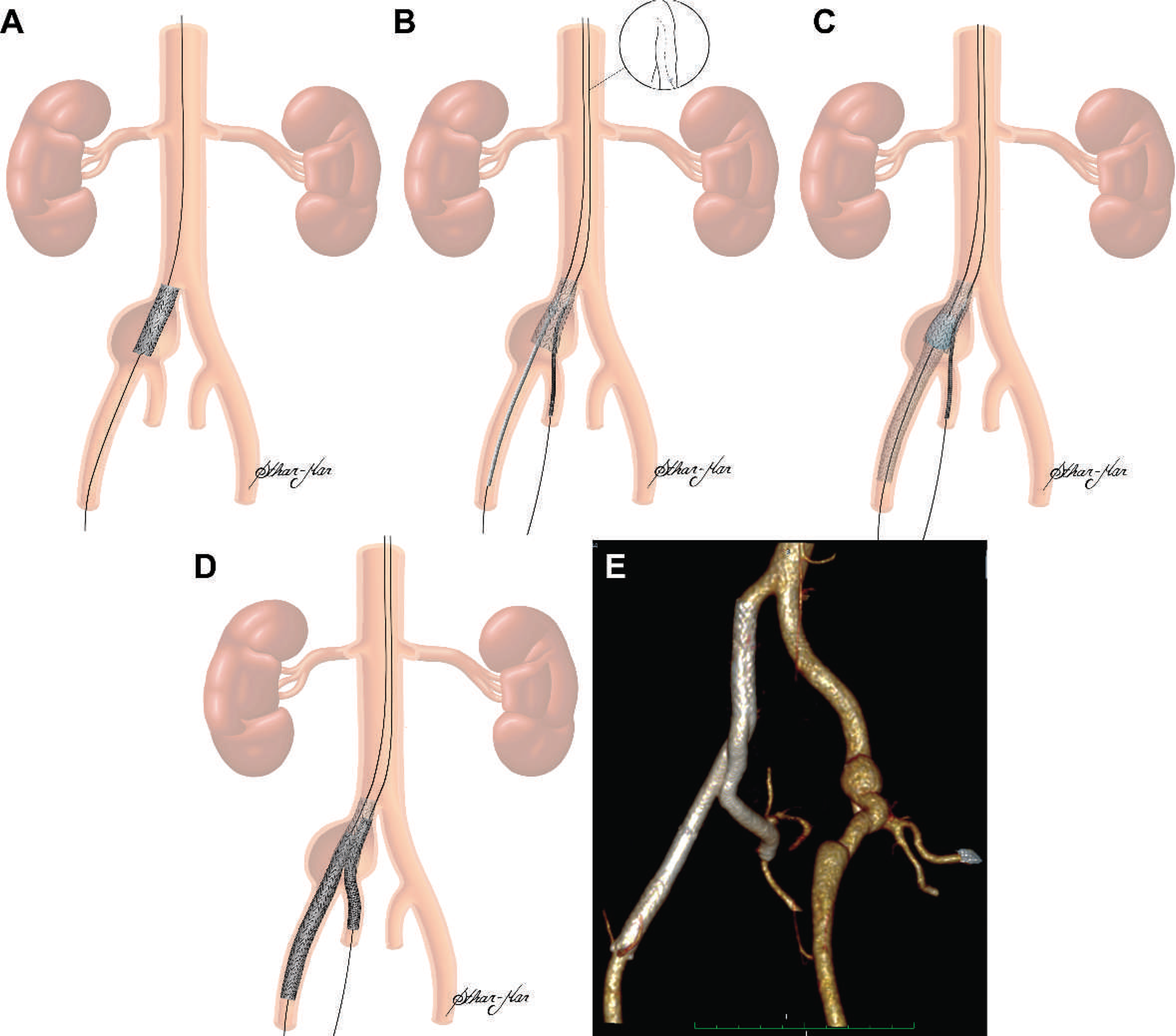
Sandwich technique for an isolated iliac artery aneurysm extending to the
internal iliac artery (IIA). (
Patient Population
In the observation period, 78 consecutive patients (70 men; mean age 73.3 years, range 61–83) undergoing endovascular repair of complex aortic aneurysms at our institution were treated using the sandwich technique under a protocol approved by the Institutional Review Board. All patients gave written informed consent to the procedure. Patient demographics and comorbidities are reported in Table 1.
Patient Demographics and Comorbidities
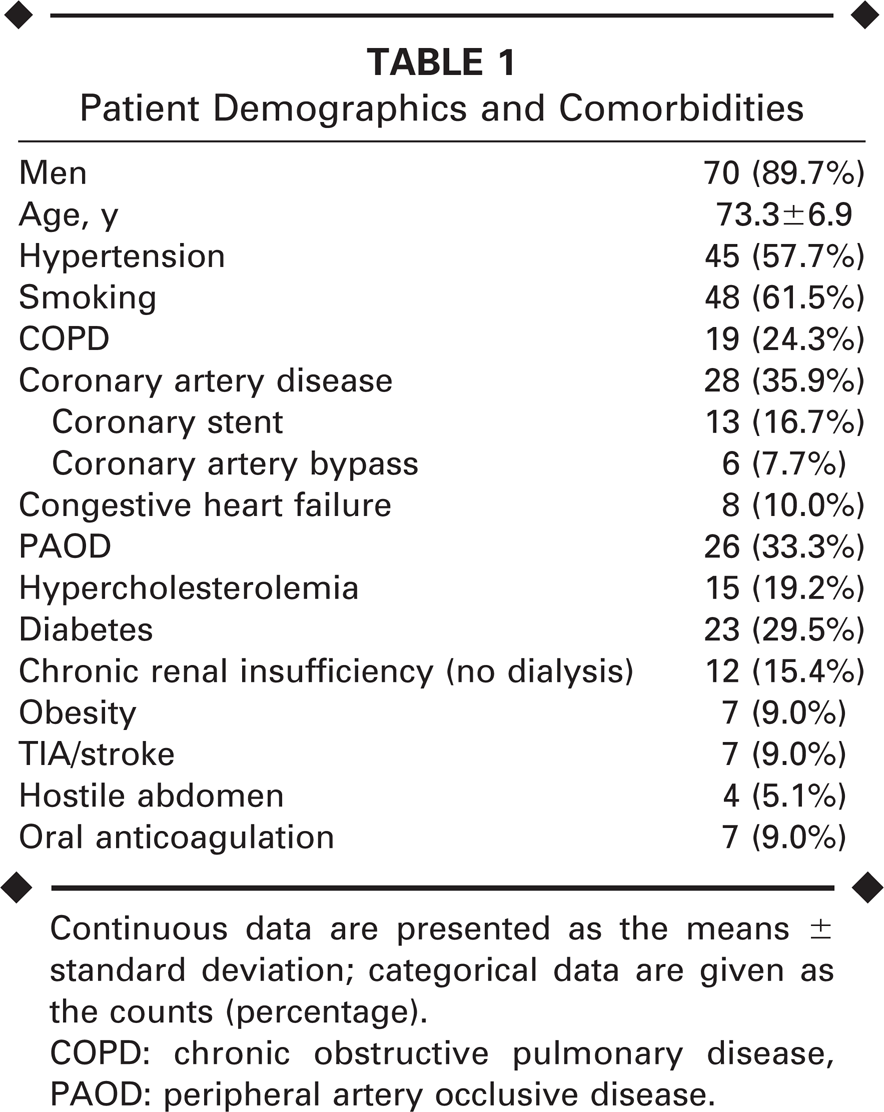
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
COPD: chronic obstructive pulmonary disease, PAOD: peripheral artery occlusive disease.
Anatomical features of the aneurysms, as well as aspects of patient history that could influence endovascular procedure indications, strategies, and planning are presented in Table 2. Two thirds of the population was treated for AIA (52, 66.7%). There were 15 (19.2%) TAAAs, 6 (7.7%) isolated IAAs, 3 (3.8%) AcAs, and 2 (2.6%) AAAs with non-diseased, short CIAs bilaterally. Five (6.4%) symptomatic patients (3 AcAs and 2 TAAAs) were submitted to endovascular repair in the urgent setting. Five (6.4%) patients had previous aortic open surgery, 32 (41.0%) were unfit for open repair, and 44 (56.4%) were not candidates for branched devices.
Preoperative Aneurysm Anatomical Features
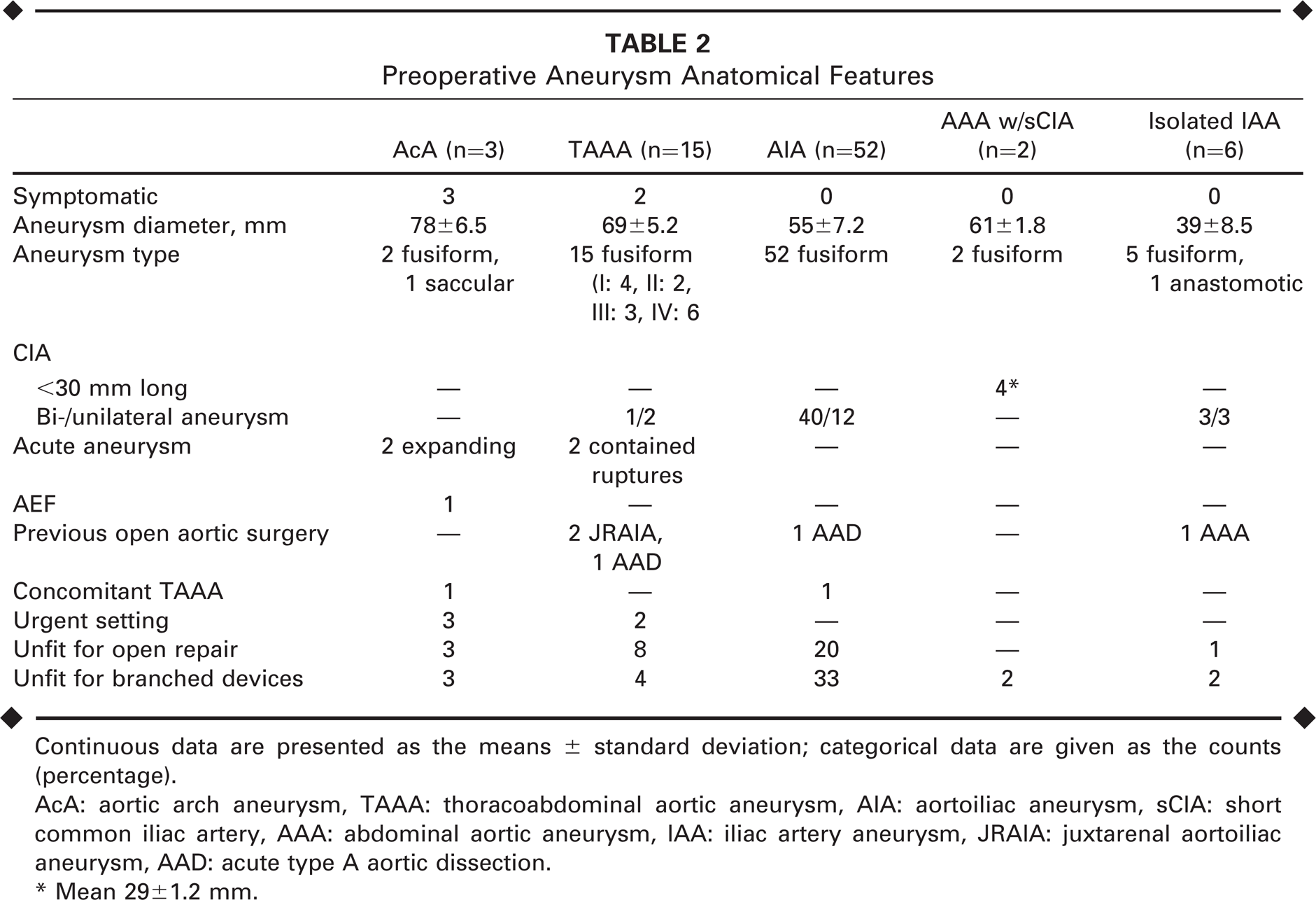
Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage).
AcA: aortic arch aneurysm, TAAA: thoracoabdominal aortic aneurysm, AIA: aortoiliac aneurysm, sCIA: short common iliac artery, AAA: abdominal aortic aneurysm, IAA: iliac artery aneurysm, JRAIA: juxtarenal aortoiliac aneurysm, AAD: acute type A aortic dissection.
Mean 29 ± 1.2 mm.
Follow-up assessment included routine office visits and imaging [computed tomographic angiography (CTA) or duplex ultrasound for patients with non-dialysis-dependent chronic renal insufficiency] performed at 1, 3, 6, and 12 months and every 6 months thereafter.
Endpoints and Statistical Analysis
Primary endpoints included patient survival and target vessel patency, as well as aneurysm sac size evolution. Patients with AIA, AAA with short CIAs, and isolated IAAs were combined in one group (hereafter referred to as the composite aortoiliac group) for analysis. Statistical analysis comprised descriptive statistics for all collected variables (procedure and fluoroscopy times; contrast and blood transfusion volumes; hospital and intensive care lengths of stay; technical success; 30-day and late (procedure-related/unrelated) mortality; endoleak; secondary intervention; device migration; end-organ complications; and aneurysm sac size change), as well as intention-to-treat analysis of survival and patency using the Kaplan-Meier method. Patients lost to follow-up were contacted, and their last CTA results were used in the analysis. Non-retrievable data were approached by the “last-observation-carried-forward” method. Student t test of the means (repeated measures) was employed to evaluate aneurysm sac size evolution over time. Continuous data are presented as the means ± standard deviation; categorical data are given as the counts (percentage). The analyses were performed using Prism statistical software (version 6; GraphPad Software Inc., San Diego, CA, USA).
RESULTS
Technical success was 98.7%; the procedure was aborted in 1 patient when both renal arteries could not be cannulated by guidewire and guide catheter. Of the 127 intended target vessels, 5 (3.9%) could not be cannulated: the 2 renal arteries in the aborted procedure and 1 additional left and 2 right renal arteries. In the last 3 cases, the sandwich procedure was carried out normally, and these vessels were occluded by the endograft. The type and number of stent-grafts, as well as the number of self-expanding covered stents used to treat target vessels, are listed in Table 3.
Aortic Stent-Graft Types and Self-Expanding Covered Stents in the Target Vessels
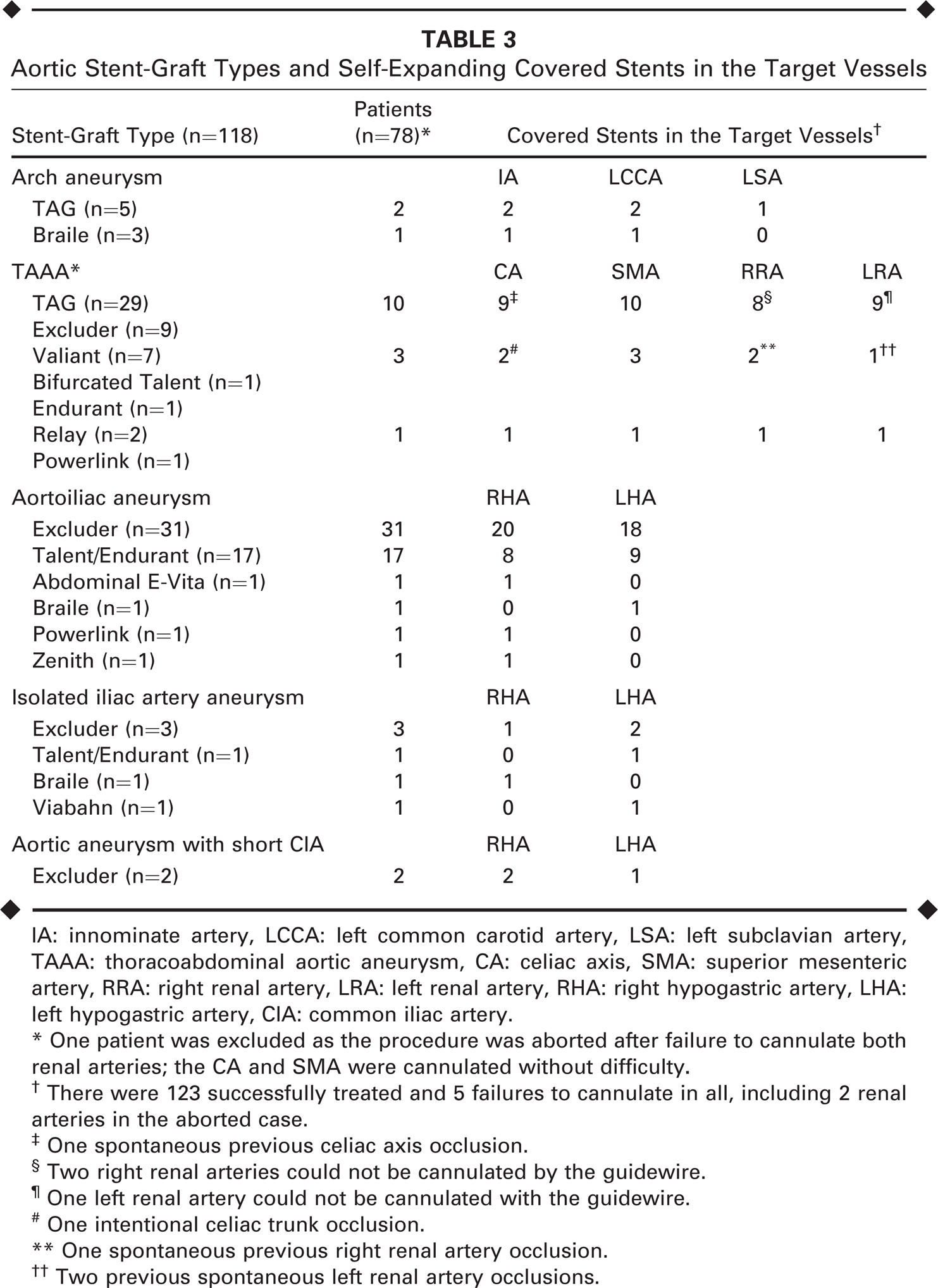
IA: innominate artery, LCCA: left common carotid artery, LSA: left subclavian artery, TAAA: thoracoabdominal aortic aneurysm, CA: celiac axis, SMA: superior mesenteric artery, RRA: right renal artery, LRA: left renal artery, RHA: right hypogastric artery, LHA: left hypogastric artery, CIA: common iliac artery.
One patient was excluded as the procedure was aborted after failure to cannulate both renal arteries; the CA and SMA were cannulated without difficulty.
There were 123 successfully treated and 5 failures to cannulate in all, including 2 renal arteries in the aborted case.
One spontaneous previous celiac axis occlusion.
Two right renal arteries could not be cannulated by the guidewire.
One left renal artery could not be cannulated with the guidewire.
One intentional celiac trunk occlusion.
One spontaneous previous right renal artery occlusion.
Two previous spontaneous left renal artery occlusions.
Performance data for the sandwich procedure for the entire study group featured a mean operating time of 154 ± 26 minutes, a mean fluoroscopy time of 31 ± 14 minutes, a mean contrast volume of 121 ± 30 mL, and a mean blood transfusion volume of 88 ± 161 mL. The mean intensive care and hospital lengths of stay were 2.5 ± 1 and 5.2 ± 2 days, respectively.
Complications
No paraplegia or paraparesis was detected (Table 4). There were 3 (3.8%) intraoperative acute myocardial infarctions (1 death, 1 coronary stenting, and 1 conservative management); 1 (1.3%) fatal pulmonary infection; 2 (2.6%) fatal cases of colonic ischemia; 1 (1.3%) case of erectile dysfunction; 2 (2.6%) patients with temporary buttock claudication; and 8 (10.2%) patients with worsening renal function (6 had existing chronic renal insufficiency). Renal function returned to the preoperative status at the 1 month in 7 patients.
Outcomes and Complications
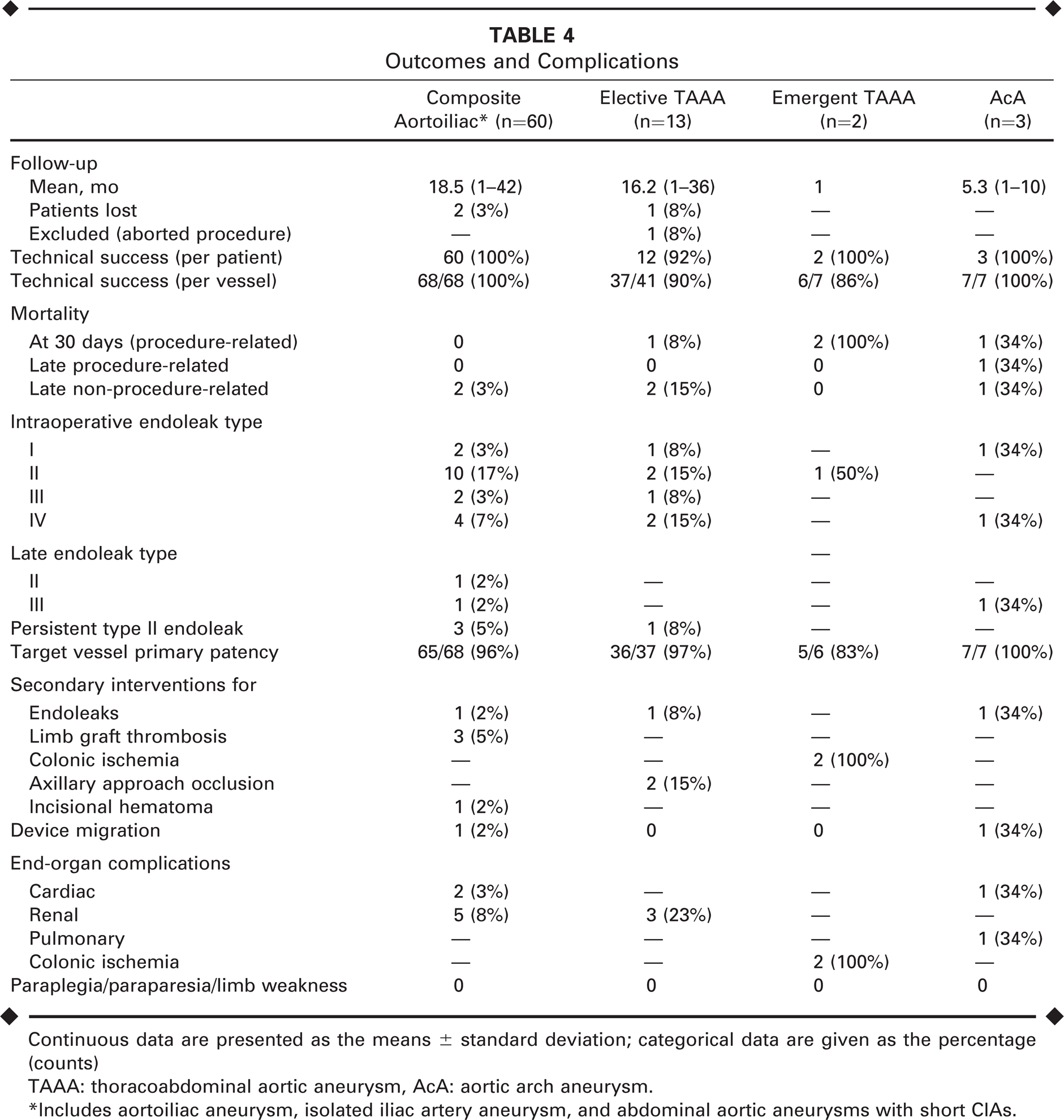
Continuous data are presented as the means ± standard deviation; categorical data are given as the percentage (counts)
TAAA: thoracoabdominal aortic aneurysm, AcA: aortic arch aneurysm.
Includes aortoiliac aneurysm, isolated iliac artery aneurysm, and abdominal aortic aneurysms with short CIAs.
Graft-related complications included 3 limb graft thromboses, 2 axillary access occlusions, 2 early brachial artery occlusions (treated medically), an inguinal hematoma, and 2 device migrations causing late type III endoleaks owing to disconnection of 2 thoracic stent-grafts in an AcA and a disconnected AIA limb.
Endoleak
Twenty-seven (34.6%) patients had endoleaks detected intraoperatively on the completion angiogram (Table 4): 4 type I, 13 type II, 3 type III, and 7 type IV. Type I endoleaks were successfully managed endovascularly during the main procedure, either with the deployment of a proximal thoracic endograft (TAAA and AcA groups) or an abdominal aortic cuff (AIA group). All early type II endoleaks were managed conservatively except one with backflow from the SMA. In the latter, a self-expanding stent-graft was successfully deployed in the SMA at the 3-month follow-up. Eight of the 13 type II endoleaks sealed spontaneously, and 1 patient died of colonic ischemia with a type II endoleak (TAAA emergency group). No aneurysm sac increase (>5 mm in diameter) was detected in the 3 persistent early type II endoleaks so far. The 3 low-flow early type III endoleaks were managed conservatively and sealed spontaneously by the time of the first CTA assessment at 1 month. All type IV endoleaks also sealed spontaneously by the time of the first CTA.
Over a mean follow-up of 17 months (range 1–42), 3 (3.8%) late endoleaks were encountered. Two type III leaks (1 AcA, 1 AIA) owing to device migration noted previously were diagnosed at 3 and 6 months, respectively; they were effectively treated with a thoracic stent-graft deployed inside the aortic arch and a stent-graft inside the right iliac limb endograft, respectively, within the first month of diagnosis.
One late type II endoleak (AIA group) associated with a 5-mm increase in the aneurysm sac was diagnosed at the 12-month assessment. This patient refused a secondary procedure and is currently being managed conservatively at 3-month intervals; no further aneurysm sac increase was observed in the last 9 months of follow-up. No late type I and IV endoleaks were detected during follow-up.
Mortality
The 30-day mortality was 5.1% (4/78). One patient died of hepatic failure after intentional celiac trunk occlusion by the endograft despite performing a recognized viability test. One arch aneurysm patient suffered a fatal myocardial infarction. Two emergency patients presenting rapid aneurysm expansion and contained TAAA rupture died of colonic infarction. All 4 deaths occurred before hospital discharge. Further investigation of factors responsible for the intestinal infarctions demonstrated that the SMA was occluded in only one of the patients.
Throughout follow-up, 6 (7.7%) patients died. Only one (1.3%) was considered procedure-related: an arch aneurysm patient with aortoesophageal fistula died of massive pulmonary infection at 6 months. The other 5 deaths, starting at 10 months of follow-up, were considered unrelated to the procedure. Their causes included a TAAA open repair in another center (AcA group), pancreatic cancer (AIA group), a hemorrhagic stroke (TAAA group), a lymphoma (TAAA group), and a myocardial infarction (isolated IAA group). The overall survival rate (Table 4, Fig. 5A) was 93.1%; the rates were 100% for the composite aortoiliac group (Fig. 5B) and 92.3% for the elective TAAA (Fig. 5C) group.
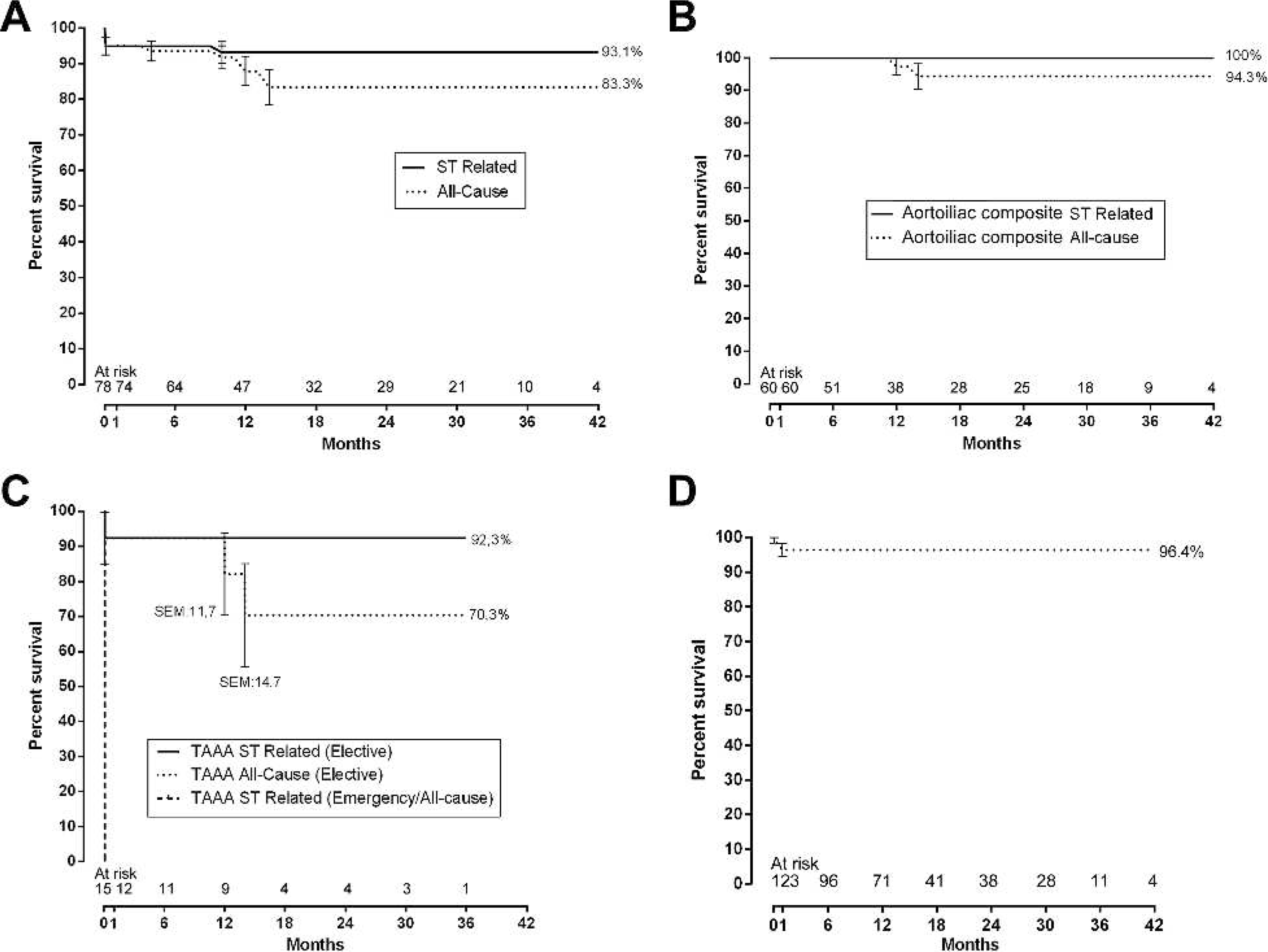
Kaplan-Meier survival curves based on intention-to-treat.
(
Target Vessel Patency
Primary patency for the 123 successfully treated target vessels was 96.4% (Fig. 5D). All 4 side branches occlusions (an SMA in the TAAA group and 3 IIAs in the AIA group) occurred in 3 patients within the first month of the study; no late occlusions were detected. Two IIA occlusions resulted from placing the covered stents too distally into the gluteal artery (<3.5 mm); the third was attributed to dissection of the distal part of the IIA by an extra-stiff guidewire. Symptoms were observed in 2 of the 3 patients, who developed buttock claudication; one of them had also erectile dysfunction, which persisted despite resolution of the buttock claudication after 6 and 10 months, respectively. The SMA occlusion also resulted from dissection of the distal part of the vessel by an extra-stiff guidewire (Table 4).
Secondary Interventions
Eleven (14.1%) secondary interventions were undertaken (Table 4): 3 (27.3%) for endoleaks as noted above, 3 (27.3%) for limb graft thrombosis, 2 (18.2%) for colonic ischemia (laparotomy and resection), 2 (18.2%) for axillary access occlusions, and 1 (9%) surgical evacuation for an incisional inguinal hematoma.
Among the graft limb complications, one ipsilateral iliac limb stent-graft with patent revascularized IIA thrombosed 12 hours after the main procedure. Patency was restored with thromboembolectomy, followed by placement of a self-expanding bare stent inside the iliac limb extension.
A contralateral iliac limb stent-graft occlusion occurred on the 29th postoperative day in a patient who had a previous unilateral CIA aneurysm and isolated IAA open repair 7 years before. A left external iliac artery dissection associated with distal clamping occurred during that procedure and was considered the cause of this event. Patency was restored through thromboembolectomy and profundaplasty, followed by self-expanding bare stent deployment to treat the previous left external iliac artery dissection.
One ipsilateral external iliac artery thrombosis with patent revascularized IIA occurred 5 months after the sandwich procedure. This patient underwent a femorofemoral crossover bypass with success.
Fate of the Aneurysm Sac
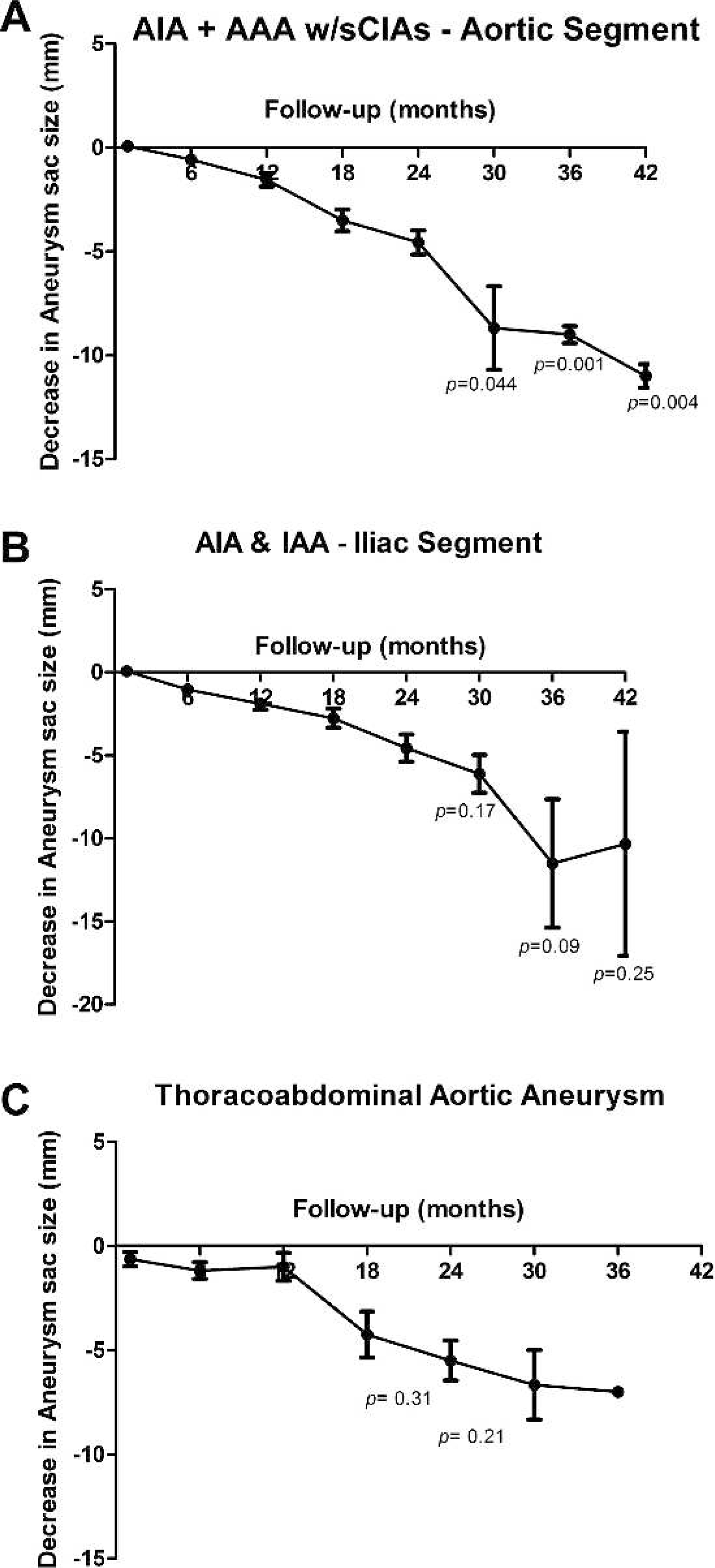
A progressive reduction in the aneurysm (AIA, isolated IAA, and TAAA) sac size (Fig. 6) was observed over the follow-up period (Table 5), reaching the mean target 5-mm reduction at the end of the second year of follow-up. Individual 5-mm reduction, though, started earlier: at 12 months for the aortic segment and at 6 months for the iliac segment of the composite aortoiliac group and at 18 months for the TAAA group. Statistical significance was reached only for the aortic segment of the AIA + AAA with short CIAs group at 30 months (p=0.044), 36 months (p=0.001), and 42 months (p=0.004).
Aneurysm Sac Size Change
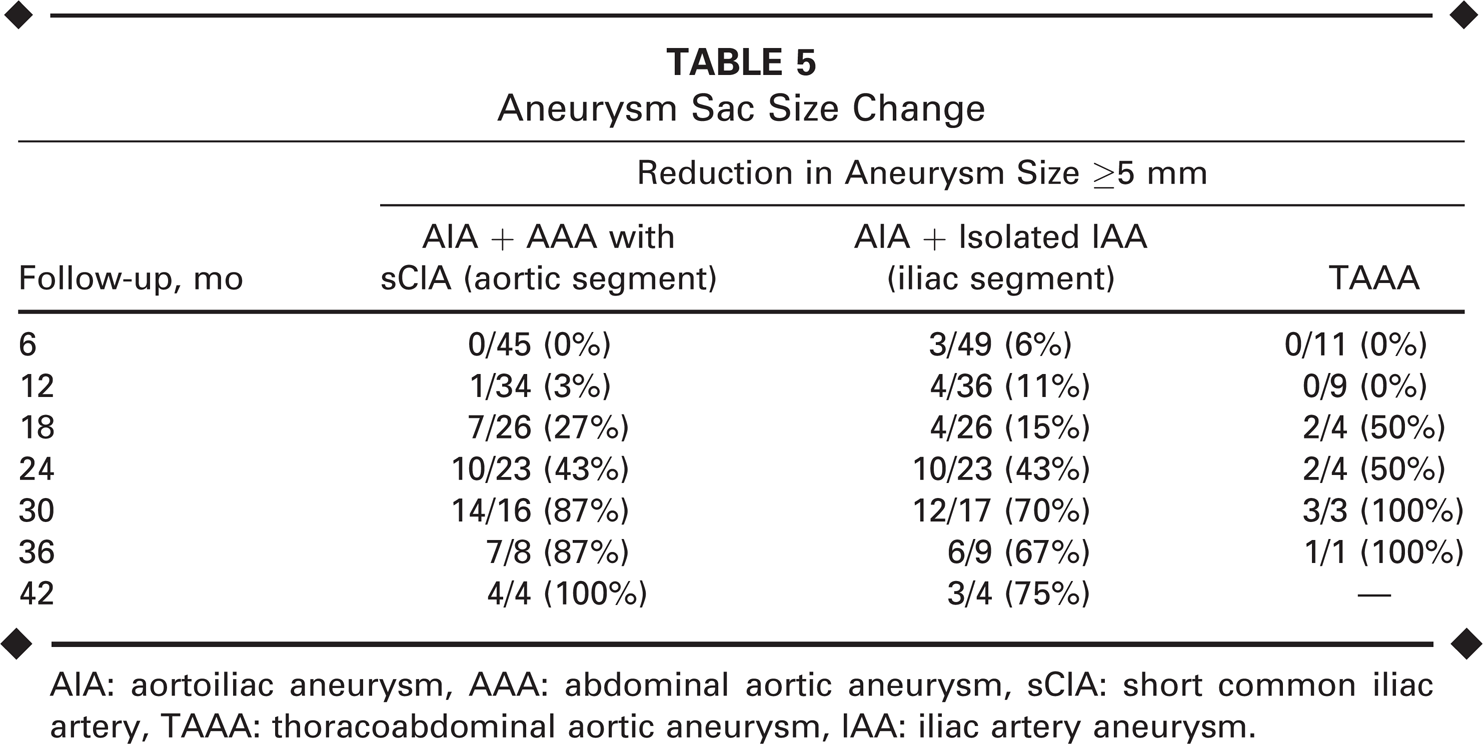
AIA: aortoiliac aneurysm, AAA: abdominal aortic aneurysm, sCIA: short common iliac artery, TAAA: thoracoabdominal aortic aneurysm, IAA: iliac artery aneurysm.
(
DISCUSSION
The sandwich technique evolved to circumvent the anatomical constraints of commercially available stent-grafts for the treatment of complex aortic aneurysms, and the midterm results are encouraging. Overall high technical success and primary patency rates, combined with progressive sac size reduction and low mortality, constitute clear-cut evidence that the sandwich technique provides safe and effective aneurysm exclusion, as well as target vessel revascularization, with sustained midterm durability in adverse anatomical scenarios not routinely addressed by other techniques.3–7 To our understanding, this derives from the use of commercially available stent-grafts familiar to the majority of endovascular surgeons, obviating the need to wait for custom-made branched devices. The outcomes reflect the technique's versatility in addressing challenging anatomical scenarios either in the emergency or elective setting (Table 6). In addition, there is no need for precise location of target vessel origins with complex image-analyzing software because the technique accommodates target vessels despite their location.
Challenging Anatomical Scenarios Appropriate for the Sandwich Technique
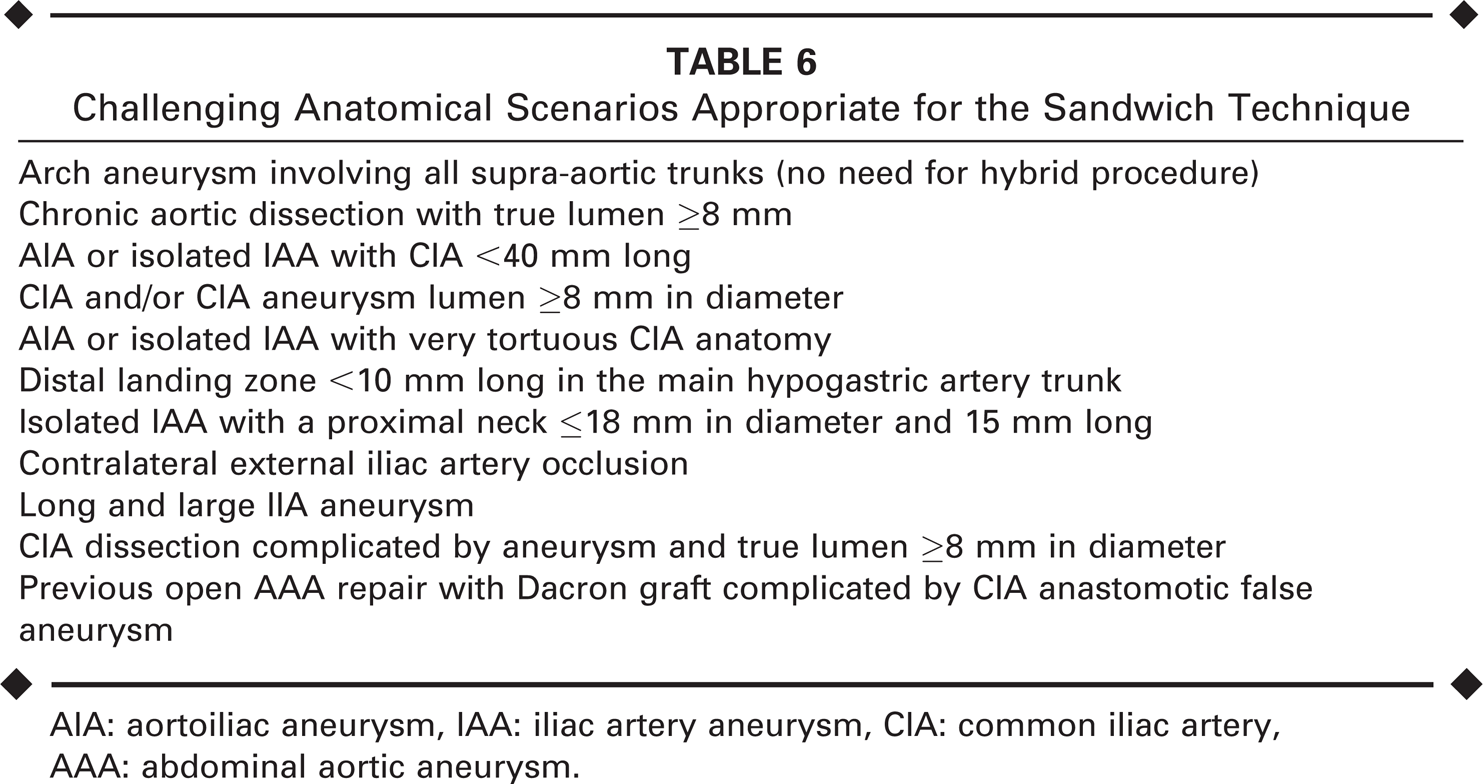
AIA: aortoiliac aneurysm, IAA: iliac artery aneurysm, CIA: common iliac artery, AAA: abdominal aortic aneurysm.
As regards branched devices, fewer than half of the study patients (43.6%: 19 AIAs, 4 isolated IAAs, and 11 TAAAs) would have been eligible for TEVAR or EVAR using a branched device. This finding is consistent with existing evidence demonstrating the low anatomical applicability (38%, 8 52% 9 ) of the commercially available iliac branched devices (IBD) for IIA preservation and/or endovascular management of aortoiliac and solitary iliac aneurysms. In the present series, patients had at least one of the following morphological factors contraindicating IBD use according to the manufacturer's Instruction for Use,10,11 as well as in other IBD series9,12–15: (1) patent CIA lumen <18 mm (free of intraluminal thrombus)9,12 in 15 (25%) patients; (2) aneurysmal IIA 9 in 13 (21.7%) patients; (3) IIA trunk length <10 mm12,14,15 in 10 (16.7%) patients; (4) CIA length <40 mm12,14,15 in 8 (13.3%) patients; (5) severe CIA tortuosity 9 in 7 (11.7%) patients; and (6) aortic bifurcation angle <40°9–11,13 in 5 (8.3%) patients. Additionally, no commercially available or custom-made branched devices can address arch aneurysm (n=3), emergency TAAA (n=2), or TAAA with previous open repair and temporary spinal cord ischemia (n=2).
Although less than half of our patients would have qualified for an IBD, it may be useful to compare the IBD results to those of the sandwich technique. Ziegler et al. 13 reported a 58% technical success rate for the first-generation device and 85% for the second-generation device when attempting to treat unilateral or bilateral CIA aneurysms combined or not with EVAR. Greenberg et al. 16 had an 86% technical success rate for CIA aneurysms and 89% for TAAAs. Other investigators have reported technical success rates varying from 91 % to 100% and primary patency rates of 74% to 100% over a 6- to 20-month follow-up for aortoiliac or isolated iliac aneurysms.14,15,17–24 We currently report 100% technical success in both arch and abdominal aneurysms and 93% for TAAAs.
Adverse outcomes, such as renal function impairment, pelvic ischemia, endoleaks, early deaths, and/or target vessel occlusions, were observed mainly in the first months of the study, suggesting the effect of a learning curve 25 or perhaps the consequence of advanced age and high comorbidities among the patients. The learning curve effect is especially evident in the TAAA group because all deaths were clustered in the first half of the study and were due to acute severe visceral ischemia caused either by intentional celiac axis occlusion, SMA occlusion, or coverage of SMA small branches. No graft-related deaths were observed in the second half of the study. The high mortality rate observed in the arch group, on the other hand, seems to reflect the patients' adverse clinical conditions. The absence of major causes of intraoperative death, such as cardiovascular and/or pulmonary complications as well as stroke in this series, may indicate that repair with the sandwich technique is well tolerated and may impose minimum operative burden to the patients.
The involvement of the visceral arteries in the aneurysm has always been of great concern during TAAA repair and has probably hindered the use of the endovascular approach in these cases. Our few instances of visceral ischemia reinforce our recommendation to revascularize all branches whenever possible to avoid end-organ ischemia.
Buttock claudication and erectile dysfunction have been reported in up to 12%12–24 of patients submitted to IBD, but these were rare (2.6% and 1.3%, respectively) for the sandwich technique. The two cases of buttock claudication in our series resolved. Endoleaks, on the other hand, were fairly common at completion angiography; however, no type I endoleak was detected thereafter. Overall, only a handful of type II endoleaks persisted, and of those, only one was associated with late sac increase.
Spinal cord ischemia (SCI) is a devastating complication that has great negative impact on health-related quality of life, lifestyle, and late survival rates. Overall, SCI (paraplegia, paraparesis, or transient lower extremity weakness) has been reported in 4% to 32% of TAAA patients undergoing surgical repair 26 and in up to 18% in TEVAR with branched devices. 27 Reilly and Chuter 26 recently proposed creating a temporary type Ib endoleak to acutely reverse neurological complications after TEVAR with branched devices by providing controlled aneurysm sac perfusion with consequent restoration of spinal cord perfusion. This idea was also adopted by Harrison et al. 27 with success in 7 of 10 cases. No SCI was observed in our patients treated with the sandwich technique, which might be owing to the use of protective measures (cerebrospinal fluid drainage) or suggest that disruption of intercostals was minimized. Indeed, the sandwich technique might provide some sort of protection against neurological adverse events by maintaining a degree of spinal cord perfusion from the unintentional low-flow type III endoleaks emanating from minimal gaps in between the two thoracic stent-grafts and the covered stents, although these endoleaks sealed within a month.
Aneurysm sac shrinkage was somewhat slower but consistent and progressive with the sandwich technique compared to IBD. Only one sac expanded and no secondary ruptures were encountered during the up to 42-month follow-up. These factors, in association with the absence of persistent types I and III endoleaks, support the efficacy and durability of this repair to completely exclude the aneurysm sac in complex aortic aneurysms.
On a technical note, we have amassed some tips to attaining better results over our 42-month-long experience with the sandwich technique. For all groups, perform targets vessel cannulation using a 0.035-inch stiff hydrophilic guidewire and 5-F catheters at least 110 cm long with VERT, MP, SIM, or IM tip curves. After cannulation, exchange the stiff hydrophilic guidewire for an extra-stiff 0.035-inch floppy tip wire no longer than 30 mm.
For the arch aneurysm group: (1) do not place more than one stent-graft and two covered stents in the aortic arch to avoid type III endoleak; instead, the third vessel should be revascularized using the periscope technique (Fig. 1). (2) Provide at least an 80-mm overlap between the first and second covered stent and the second thoracic stent-graft at the ascending thoracic aorta level to avoid type Ia endoleak. (3) Provide at least a 30-mm overlap between the third covered stent and the second thoracic stent-graft at the descending thoracic aorta level to avoid type Ib endoleak.
For the TAAA group: (1) the covered stents should be positioned not to exceed 20 mm inside the visceral arteries (distal end) and with at least a 50-mm overlap (proximal end) with the first thoracic stent-graft to avoid endoleak type III. Special attention should be given so as not to cover SMA small branches to avoid ischemic insults. (2) Place a bare self-expanding stent inside the covered stent to avoid kinking and future occlusion. (3) For type I TAAA, there is no need for the bifurcated stent-graft (Fig. 7A).
(
For the AIA group: (1) covered stents should be positioned 20 mm inside the IIA (distal end) to avoid type II endoleak and with a 50-mm overlap within the ipsilateral iliac limb of the bifurcated stent-graft (the proximal end) to avoid type III endoleak. (2) The IIA must have a minimal lumen of 3.5 mm to avoid occlusion. (3) The IIA could also be catheterized through a contralateral femoral approach when using unibody bifurcated stent-graft.
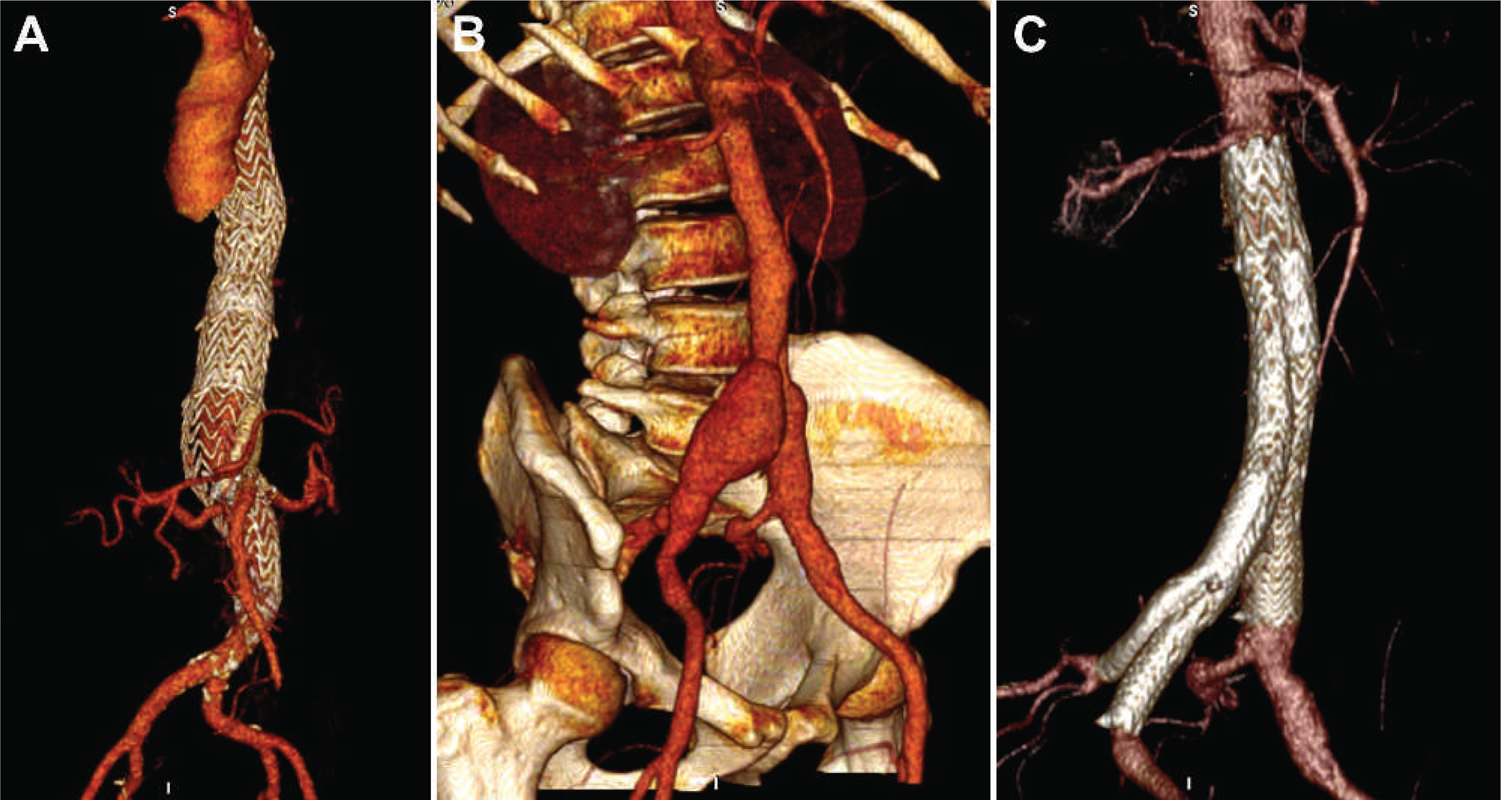
For the isolated IAA group: if the CIA aneurysm is <40 mm in length and/or has an inadequate proximal neck (Fig. 7B,C), opt for any commercially available bifurcated stent-graft instead of the iliac extension or covered stent and follow the technical steps described for the aortoiliac aneurysms.
Conclusion
The sandwich technique facilitates safe and effective aneurysm exclusion and target vessel revascularization in adverse anatomical scenarios, with sustained durability in midterm follow-up. Thus, the sandwich technique appears to be a good addition to the endovascular armamentarium for treatment of complex aortic aneurysms. More experience with the method is advisable, especially for arch aneurysms and TAAAs.