
Abstract
Objectives
Distraction osteogenesis has been applied to the craniofacial region. To reduce the cleft width of patients with cleft lip and palate, alveolar bones are distracted toward the cleft. However, no reports have described limitations to the amount of lengthening that can be achieved by distraction osteogenesis in this area. Therefore, we investigated the healing process following different extents of distraction osteogenesis using a canine cleft palate model.
Methods
A 10-mm bone defect was made in the palates. A bony segment including the canine was prepared and translocated into the defect area at a rate of 1 mm/d for 6 or 10 days, resulting in two groups (6- and 10-mm groups). Canine pulpal blood flow was monitored for 100 days with Doppler flowmetry. Then, the animals were sacrificed and the regenerated bone area was evaluated radiologically and histologically. Statistical significance was confirmed with the Mann-Whitney rank test.
Results
Pulpal blood flow in the 6-mm group recovered to original levels earlier than in the 10-mm group. Cortical bone density in the regenerated bone, measured by peripheral quantitative computed tomography, was significantly greater in the 6-mm group than in the 10-mm group. The amount of regenerated bone in histologic sections was also significantly greater in the 6-mm group.
Conclusion
We clearly showed that healing progress depends on the extent of distraction osteogenesis, highlighting the importance of limited distraction osteogenesis in the alveolar area.
Distraction osteogenesis (DOG) has been applied to deformities in the craniofacial region for bone correction purposes. The technique was developed originally for limb bones (Ilizarov, 1952) and then was applied to the craniofacial skeleton (Snyder et al., 1973). Because the craniofacial region contains fewer bone marrow cells than long bones, it is considered that vascularization, mineralization, and thus the overall healing process are critical.
The healing process of distracted areas in the maxillofacial region has important clinical implications for this treatment. In patients with cleft palate, large reconstructions of maxillary bones as well as major movements of teeth might be necessary in the course of treatment (Yen et al., 2001 Binger et al., 2003 Suzuki et al., 2006). In such cases, bones are distracted to different extents, depending on specific needs at a certain site, to close existing gaps or widen interdental areas to provide space for implants or for correction of malpositioned teeth. However, it is necessary to achieve sufficient remineralization of the operated sites in a short time to guarantee the long-term success of the treatment and to prevent situations in which a refracture (El-Mowafi et al., 2005) in improperly mineralized bone might occur. Given the influence of vascularization, callous formation and bone mineral density are of prime importance in providing treatment that is reproducible and reliable to patients with cleft palate.
Numerous parameters that influence the healing process after distraction osteogenesis have been examined in different model species (Djasim et al., 2007). Among the factors investigated, attention has been focused mainly on latency (days) (Aida et al., 2003), rate of distraction (mm/d) (Hasse et al., 2005), rhythm (1/24 h) (Paccione et al., 2001; Hasse et al., 2005), and duration of consolidation itself (Smith et al., 1999; Cope and Samchukov, 2001). However, only limited information is available on the final extent of the distraction process, which is commonly in the range of 5 to 20 mm. A systematic evaluation of this parameter is lacking (Swennen et al., 2001, 2002). Therefore, we investigated the impact of the extent of distraction osteogenesis in a cleft palate model. Here, by performing measurements of tooth blood flow recovery with laser Doppler flowmetry and bone mineral density analysis, we show that limited DOG is beneficial not only for shortening the duration of consolidation, but also for achieving the final mineralization. This study demonstrates the prospective limitations of bone lengthening by DOG in the alveolar area and provides a basis for considerations when a large amount of bone lengthening is warranted.
Materials and Methods
Operation Procedure and Distraction Protocol
Ten female adult beagle dogs (mean age, 14.2 months) were caged individually and kept under a 14/10 h light-dark cycle at 21±2°C. They were fed a standard diet (dog chow, DSA Oriental Yeast Co., Ltd., Tokyo, Japan) once a day in the morning, and water was given ad libitum. All dogs studied were cared for in accordance with the regulations of the Institutional Animal Care and Use Committee at Tokyo Medical and Dental University, under the supervision of licensed veterinarians. After the dogs were anesthetized by IV injection of thiopental sodium (Ravona, 0.3 mg/injection) (Tanabe Seiyaku Co., Ltd., Tokyo, Japan), the three maxillary incisors on the left side (distracted side) of each dog were extracted. Then, a 10-mm-long bone defect, mimicking a cleft palate, was made in the alveolar bone at the original location of the maxillary incisors using a carbide burr. The right side (control side) was left untreated. Then, the first and second premolars were extracted bilaterally to facilitate the subsequent operation.
The distraction device (KWA-3007, Keisei Medical Industrial Co., Ltd., Tokyo, Japan) was fixed using a bone-borne approach, as has been described elsewhere (Liou et al., 1998) (Fig. 1). After the surgery was completed, all dogs were injected with the antibiotic benzylpenicillin procaine. After the osteotomized palate had been fixed by the distraction device for 3 days (latency period), transportation of the segment into the bone defect was started. The distraction device was activated at a rate of 1 mm/d to create sufficient new bone (Ilizarov, 1989). Five dogs underwent activation for 6 days (6-mm group), and another five dogs underwent activation for 10 days (10-mm group) (Fig. 2).
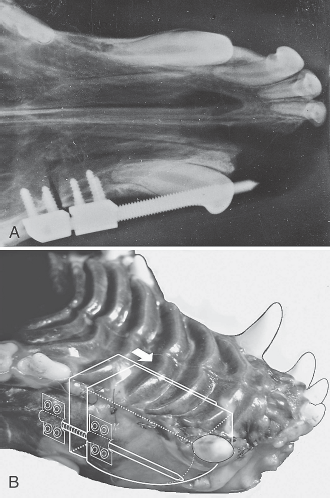
A: Occlusal view by x-ray before the distraction device was activated. B: A diagram showing the osteotomies.
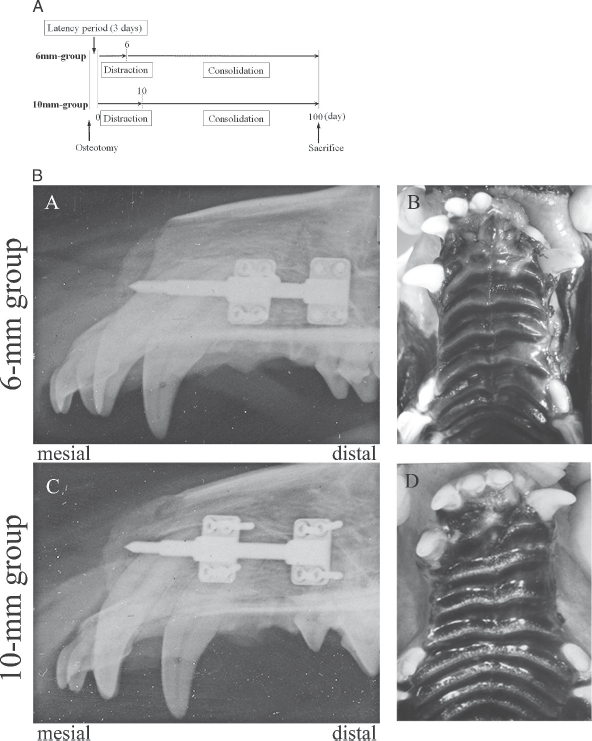
A: Experimental protocol and x-ray of the 6-mm and 10-mm groups. B: (A) Lateral view after 6 mm distraction. (B) Occlusal view from the same day. (C) Lateral view after 10 mm distraction. (D) Occlusal view from the same day.
Pulpal Blood Flow Measurements
An apparatus for monitoring tissue blood flow based on the Doppler principle has been developed (Stern, 1975; Bonner and Nossal, 1981). Recently, this method was used to study blood flow in oral tissues (Baab et al., 1986). In the present study, each dog's bilateral canine pulpal blood flow was monitored with the dog under general anesthesia from thiopental sodium, using a laser Doppler flowmeter (Periflux4001, Perimed, Stockholm, Sweden) (Roman and Smits, 1986 Grodzicki et al., 2003). Blood flow was measured on the preoperative day, every day during the distraction period, and every 10 days during the consolidation period. A cavity (1 mm in depth) for measuring pulpal blood flow was created on the buccal surface on both sides. The sensor of the laser Doppler flowmeter was placed into the cavity to monitor pulpal blood flow and was positioned with a custom-made stent (Sasano et al., 1989). Blood pressure was confirmed to be stable each time, before blood flow was measured. Blood flow recovery percentage (% blood flow) was calculated as the ratio of the mean pulpal blood flow to the preoperative value. Pulpal blood flow rates on the distracted and control sides were compared between the 6-mm and 10-mm groups.
Radiographic Observations
Plain occlusal x-rays of the head were taken using an x-ray machine (Venus Dental X-Ray, Yoshida Seiko Co., Ltd., Tokyo, Japan) immediately after the osteotomy, and every 10 days subsequently. The x-ray output voltage was set at 60 kV, 10 mA for 0.3 second. Radiographs were analyzed using gray levels (0 to 255) of the target area with an image analyzer (ImageJ, Bioarts Co., Ltd., Fukuoka, Japan). The gray level percentage was calculated as the ratio of the gray levels of the regenerated area compared with that of the canine dentin on the control side. The regenerated area was defined as the area (4 mm × 4 mm) of a site proximal to the third premolar and parallel to the distraction rod. The compared area (2 mm × 2 mm) was set at one third of the distance from the apex of the canine dentin buccal area on the control side as a standard gray level because this area consisted of a homogenous gray level. Then the percentage gray levels on days 10, 40, 70, and 100 were compared between groups.
Measurement of Bone Mineral Density by Peripheral Quantitative Computed Tomography
On day 100 after the osteotomy, each dog was sacrificed by IV injection of an overdose of thiopental sodium. After the sacrifice, bilateral palates were harvested and distraction devices removed. The palates were then cut in half along the median palatal suture. All harvested specimens were fixed in 10% buffered formalin fixative, then were dehydrated in graded ethanol and embedded in polyester resin (Rigolac, Showa Highpolymer Co., Ltd., Tokyo, Japan) in an undecalcified condition. Bone mineral density (BMD) analysis was performed on each specimen using peripheral quantitative computed tomography (pQCT) (XCT Research SA+ Stratec, Medizintechnik GmbH., Pforzheim, Germany) (Noji et al., 2000; Nonaka et al., 2006). The site proximal to the third premolar was defined as the reference line, and sequential computed tomography (CT) slices were scanned in a proximal direction from this reference line. On the distracted side, six and ten slices were taken from the 6-and 10-mm groups, respectively, with a 1-mm scanning distance. Specimens were placed in the CT scanner so that the scan planes were perpendicular to the DOG direction. On the control side in both groups, six slices were scanned from the reference line. Finally, three sequential slices representing the central area were selected: These included slices 2 to 4 on the distracted side in the 6-mm group, slices 4 to 6 on the distracted side in the 10-mm group, and slices 2 to 4 on the control side in both groups. A 10.0 (longitudinal) × 7.5 mm (transverse) area close to the nasal septum, located 2 mm below the maxillary canine pulp, was defined as a region of interest (ROI) on each CT slice. The proposed ROIs contained all of the tissue regenerated by DOG, excluding host bone, which might cause interference in the 10-mm group; the same ROI was used in the 6-mm group. A BMD of higher than 690 mg/cm3 was considered to represent the cortical range, a BMD between 395 and 690 mg/cm3 was defined as the subcortical range, and a BMD lower than 395 mg/cm3 was defined as the trabecular range, as defined in previous studies (Louis et al., 1995; Ferretti, 2000; Kudoh, 2008). The BMD, bone area, and bone mineral contents (BMC) measured in the distracted sites were statistically compared between 6-mm and 10-mm groups using the average values for each of the three slices. BMD and bone area for a certain ROI in each CT slice were automatically calculated by pQCT programs. BMC was calculated by multiplying BMD and bone area. Units for BMD, bone area, and BMC were mg/cm3, mm2, and mg/mm, respectively.
Bone Histomorphometry
After the embedded bone was scanned using pQCT, undecalcified ground sections of 50-μm thickness were prepared. Slices were prepared analogously to the pQCT sample preparation described elsewhere (Noji et al., 2000). The slices were then stained with toluidine blue (0.1%, pH 7.0) (Wako, Osaka, Japan), and light microscopic images of the undecalcified ground sections were obtained. Histomorphometric measurements were performed using the same measurement area described in the pQCT section. An image analysis system (KS-400, Carl Zeiss, Jena, Germany) was used to measure the regenerated bone area, which required the ratio of calcified area to total measured area (Noji et al., 2000). Regenerated bone thickness, regenerated bone number, and regenerated bone separation were calculated in the same way as trabecular thickness, trabecular number, and trabecular separation for the 6-mm and 10-mm groups (Parfitt et al., 1987).
Statistical Analyses
All data from pulpal blood flow measurements, radiography, BMD by pQCT, and bone histomorphometry for the 6-mm and 10-mm groups are presented as means ± SD and were analyzed using the Mann-Whitney rank sum test with Stat View software (SAS Institute Inc., Cary, NC). The difference was considered significant when p < .05.
Results
Operative Procedure
No significant differences in body weight were noted between the 6-mm group and the 10-mm group at the beginning of the experimental period (6-mm: 10.6 kg, 0.3, 10.1 to 11.5 [mean, SD, range]; 10-mm: 10.1 kg, 0.4, 9.7 to 10.8) or at the end of the experiment (6-mm: 10.8 kg, 0.5, 10.0 to 11.9; 10-mm: 10.5 kg, 0.4, 10.0 to 11.2). A series that included extraction, defect making, and device attachment was successful in all 10 beagle dogs, and the intended lengthening was obtained without major complications or relapse.
Pulpal Blood Flow Measurements
In both groups, mean blood flow (% of preoperative) demonstrated a steep decrease immediately after osteotomy and a gradual increase to the original level over time on the distracted side, where osteotomy was performed. Mean blood flow in the 6-mm group increased from day 30 and recovered to the original level within 90 days. On the other hand, it took 100 days to recover to the original level in the 10-mm group. Significant differences were noted between values for the two groups on days 60, 70, 80, and 90 (Fig. 3). On the control side, average blood flow was stable around the original level from the preoperative day until the end of the experiment in both groups.
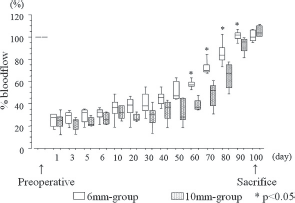
Measurements of blood flow recovery obtained by laser Doppler flowmetry (distracted side).
Radiographic Observations
On x-ray images captured on day 10, no callus seemed to have formed on the distracted site in animals in either group. On day 40, slightly radio-opaque lines appeared in animals in the 6-mm group, no calluses were apparent in the 6-mm group, and no callus had formed in the 10-mm group. On day 100, a more radio-opaque area at the DOG site was seen on x-ray images of animals in the 6-mm group, qualitatively illustrating more bone formation than had occurred in the 10-mm group (Fig. 4).
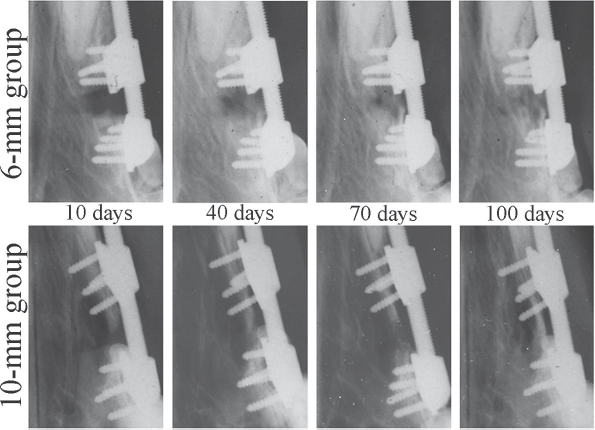
Radiographic images of the distracted area during the consolidation period.
The percentage gray level in the 6-mm group was significantly higher on days 40, 70, and 100 than in the 10-mm group (p < .05) (Fig. 5). On the control side, the percentage gray level did not show significant differences in both groups.
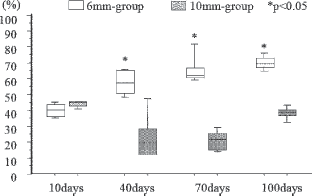
Radiographic evaluation of bone formation as percentage of the gray level.
BMD Measurement by pQCT
The radiologic profile obtained by pQCT at the site of the median slice at the distracted area (Fig. 6) revealed that the mineralized area at the site of distraction in the 6-mm group was much larger than in the 10-mm group, and bone mineralization on the control side in the 6-mm group was almost the same as in the 10-mm group (Fig. 7). Quantitative analyses showed that average BMD, bone area, and BMC in the cortical range were significantly higher in the 6-mm group than in the 10-mm group (p < .05), and mean BMD, bone area, and BMC in the subcortical and trabecular range were not significantly increased in the 6-mm group (Fig. 8). On the control side, BMD, bone area, and BMC did not show significant differences in either group.
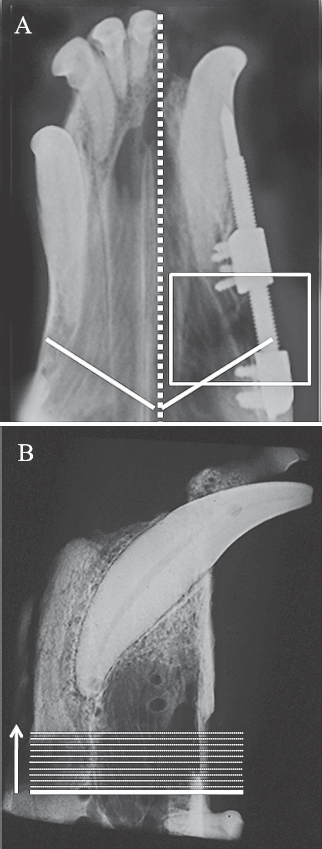
Sequential CT slices with a 1-mm scanning distance in a mesial direction from this reference line, the proximal site of the third premolars. Three median slices representing the central area were selected for analysis. (A) Occlusal x-ray with a reference line (dotted line; sagittal plane). (B) Lateral x-ray of a specimen with a reference line and slices with the distracted side after the sacrifice.
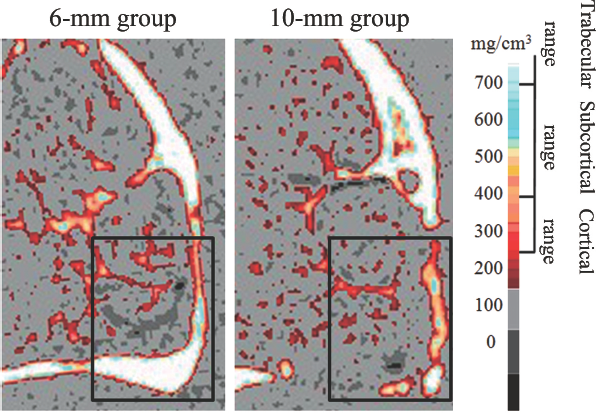
Digitized BMD image of representative slices from the distracted side by pQCT and ROI, 100 days after the operation. The color code bar on the right shows BMD gradient levels: The cortical range is represented by blue to white levels (>690 mg/cm3); the subcortical range by orange to light blue (395 to 690 mg/cm3); and the trabecular range by red to orange levels (230 to 395 mg/cm3).
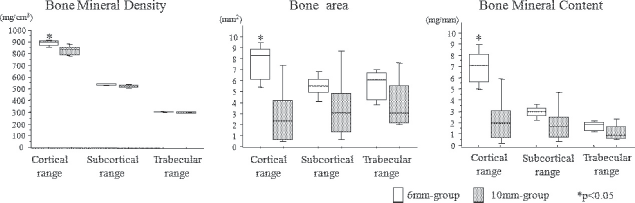
Measurements of bone mineral density, bone area, and bone mineral content by pQCT on the distracted side, 100 days after the operations.
Bone Histomorphometry
As is shown by the arrow in Figure 9, a larger amount of regenerated bone was apparent in the 6-mm group and several bony islets were observed in the 10-mm group. Histomorphometric measurement showed that the regenerated bone area and the regenerated bone thickness were significantly increased in the 6-mm group (p < .05) (Fig. 10). On the other hand, no significant difference in regenerated bone number and regenerated bone separation was noted between the 6– and 10-mm groups. These data indicate a significant increase in bone volume at the site of DOG in the 6-mm group compared with the 10-mm group. With regard to bone formation on the control side, no significant differences were observed between the two groups.
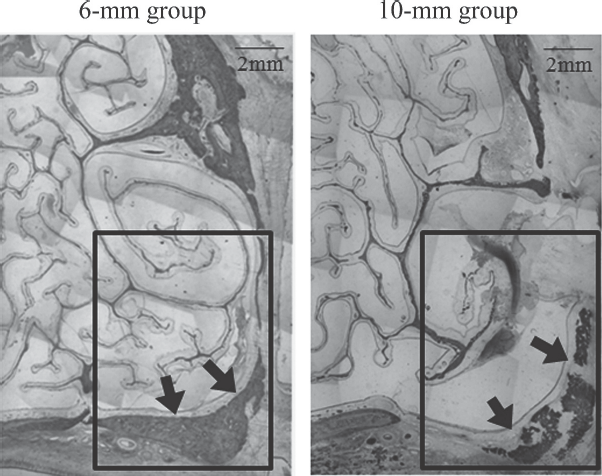
Histologic images from the distracted side, 100 days after the operation. Representative histologic images from both groups and the measured ROI. Arrows = regenerated bone area.
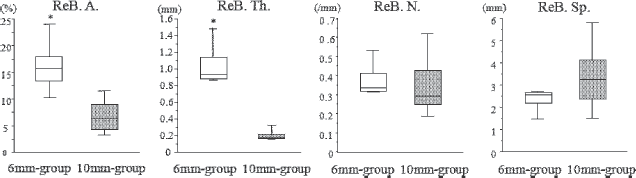
Histomorphometric analysis of regenerated bone on the distracted side, 100 days after the operations. ReB A = regenerated bone area; ReB Th = regenerated bone thickness; ReB N = regenerated bone number; ReB Sp = regenerated bone separation.
Discussion
Distraction osteogenesis has been regarded as a promising method for reconstruction of the craniofacial area since it was first introduced for human patients more than 10 years ago (McCarthy et al., 1992). Since then, a vast number of reports on DOG in the craniofacial area have been published (Cohen et al., 1995; Polley and Figueroa, 1997; Molina et al., 1998; Mommaerts, 1999).
Previous research using several models has emphasized the importance of latency (days), rate of distraction (mm/d), rhythm (times/24 h), and consolidation length, but not the importance of the amount of lengthening. Therefore, in the present study, we investigated the influence of the extent of DOG in the maxillofacial area in a beagle dog cleft palate model.
Aseptic necrosis of maxillary dental pulp, periodontal tissue, and dentoalveolar segment following maxillary osteotomies was reported (Lanigan et al., 1990). Because pulpal vascularization originates from surrounding bone vascularization, tooth blood flow recovery was considered to be a reliable parameter with which to evaluate the regenerated site (Emshoff et al., 2008). In this investigation, recovery of blood flow was not different between the 6-mm and 10-mm groups in the early phase until day 10. However, from day 10, the percentage blood flow in the 6-mm group presented an early rising curve and recovered to original levels earlier than in the 10-mm group. The results of this investigation show that the extent of DOG is correlated with time to recovery of the regenerated site.
To gain insight into the mineralization process after DOG, we used pQCT, a widely used imaging technique in animal experiments and clinical diagnosis (Nonaka et al., 2006). For all evaluated parameters, including volumetric BMD (g/mm3), which is used to predict the mechanical properties of bone material (Ferretti et al., 1995; Wachter et al., 2002), the bone mineral content, and the bone area in the same ROI, values in the cortical range were significantly higher in the 6-mm group than in the 10-mm group. In the subcortical and trabecular ranges, no significant differences were noted between the two groups.
Structural changes in bones at the regenerated site were illustrated by histomorphometry. These histomorphometric data showed significant increases in bone volume and bone connectivity at the site of DOG in the 6-mm group compared with the 10-mm group. A faster increase in mineralization in the 6-mm group was also evident on x-ray analysis after day 40.
The distraction process diminishes the supply of essential nutrients and gaseous exchange in cells close to the operated site. This supply is necessary for cell division, mineralization, and tissue formation in general. Cells in bone tissue are accessible only via micrometer-sized channels that enable nutrient transport in the interstitial fluid. Although diffusion is supposed to be the main process for the transport of nutrients, convection might support the movement of fluids (Knothe et al., 1998; Wang et al., 2005). In a fixed bone, these convective forces are limited and thus further limit oxygenation and nutrient transport.
Generally, mineralization begins at the host bone margins by the end of the distraction period; this is followed by a gradual increase in the mineralization of trabecular bone (Cope and Samchukov, 2000). The preserved periosteum provides the blood supply, which is critical to successful callous formation (Ilizarov, 1989). Because a smaller portion of bone marrow tissue is present in the craniofacial region compared with the long bones, the periosteum is thought to be a major source of blood supply at the site of DOG. The amount of DOG also affects the periosteum and therefore has an impact on mineralization. As would be expected from the bigger gap created in the tissue in the 10-mm group, regeneration and mineralization take longer and the bone in this group is less mature than in the 6-mm group. The difference between 6-and 10-mm groups becomes more readily visible in the cortical range, as this tissue is naturally sensitive to defects because of slower healing. This sensitivity is due to limited diffusion processes resulting from the isolated locations of osteoblasts and osteoclasts, which are embedded in a mineralized extracellular matrix that acts as a diffusion barrier, and the overall lower vascularization in hard bone. By contrast, subcortical bone and trabecular bone contain a higher percentage of nonmineralized extracellular matrix and higher vascularization and thus appear to be less sensitive to tissue destruction. Our previous report also showed the emergence of trabecular-like bone tissue in the long bones during the early phase after DOG (Noji et al., 2000). Thus, DOG has less impact in these less mineralized tissues. Because the main limitation for new tissue formation is the oxygen supply, a possible intervention could be hyperbaric oxygen treatment, which has been shown to improve the healing process in the alveolar region (Kudoh, 2008).
According to the results of the present study, the limitation of distraction lengthening can be one of the key considerations for the healing process. A shorter distraction length leads to more advanced healing progress, as could be seen when 6-mm distractions were compared with 10-mm distractions in the present study. This is true for vascularization as well as for bone mineral density, for which it is important to have enduring stability at the treated site. The data from this model experiment should therefore be considered when DOG is established for clinical treatment. However, despite the fact that canine blood flow recovered after 100 days, the design of our study did not allow us to investigate how bone mineral density is affected after 100 days. The absence of long-term data is the limitation of this study. Nevertheless, even if the 10-mm group recovered to the same level as the 6-mm group long after our original time frame, it would not be suitable in a clinical situation to have such extended recovery periods. If the distractor has to be installed for extended periods of time, hygienic issues, as well as psychological problems, could arise (Kanellopoulos and Soucacos, 2006). Low bone mineral density with an insufficient consolidation period may promote refracture at the distracted site. Besides, most experiments investigating the results of distraction osteogenesis (Swennen, 2001, 2002; Djasim, 2007) used a period of 4 to 8 weeks to draw conclusions; our study is thus within commonly assessed time frames.
Distractions of 6 mm and 10 mm resemble a premolar or molar, respectively. These teeth are often moved into the distracted site in patients with cleft palate after maxillary alveolar bone displacement during the course of treatment (Suzuki et al., 2006). In such cases, bones are distracted to different extents, depending on specific needs at a certain site, to close existing gaps or widen interdental areas to provide space for implants, or to further move existing, formerly displaced teeth. Alternatively, a corresponding implant could be inserted into the newly reconstructed space. Therefore, our study gives some insight into expected mineral densities at the distracted site in relation to the extent of DOG, which is important for the prediction of consolidation periods and subsequent therapeutic strategies. It remains to be seen what will be the long-term effects of distraction of different lengths. In clinical practice, it will be of importance to determine whether vascularization and mineralization also return to preoperative values in maximally distracted bones.
However, limiting distraction is not always possible. In such cases, additional precautions might be considered to shorten the consolidation time as much as possible to achieve proper healing. Such precautions may include application of tissue and bone formation-promoting factors, such as tissue growth factors like osteogenic protein 1 (Mandu-Hrit et al., 2006) and recombinant human fibroblast growth factor-2 (Abbaspour et al., 2008), or treatment with parathyroid hormone (Andreassen and Cacciafesta, 2004). At present, however, no trials have investigated the effects of these treatments on human fracture healing. By contrast, application of recombinant bone morphogenic protein could be considered an optional treatment, with human trials in progress (Giannoudis and Tzioupis, 2005). Hyperbaric oxygen treatment has also been shown to influence healing positively (Muhonen et al., 2002; Clark et al., 2006) and has been applied as a treatment for challenging clinical conditions (Atesalp et al., 2002).
In conclusion, the present study showed that shorter distraction length leads to more advanced healing progress, as was shown for 6-mm distractions compared with 10-mm distractions. Such morphologic data showing the natural limits of the tissue will support successful operations in the alveolar region. On the other hand, investigation of mineralizing phases over an extended time frame should be advocated to qualify any conclusions. Moreover, exploration should evaluate the background of vascularization and ossification in the maxillofacial area to improve treatments that involve distraction techniques. Basic research that elucidates the physiologic and biochemical processes of wound healing and bone mineralization will further stretch the given limits of distraction. To apply knowledge of basic science in clinical cases, a detailed analysis of morphologic and surgical constraints is indispensable.
Footnotes
Acknowledgments
This study was supported by Grants-in-Aid for Scientific Research (16592040, 17592131, 19592347, and 19791567) from the Japanese Ministry of Education, Science, Culture, and Sports, and by a grant from the Japanese Ministry of Education, Global Center of Excellence (GCOE) program, “International Research Center for Molecular Science in Tooth and Bone Diseases.”