
Abstract
Objective
Using the systematic review method, (1) to identify the investigations of the parental dentocraniofacial phenotype in orofacial clefting, (2) synthesize the data to derive a model of the phenotypic features that will assist in the identification of cleft morphogenes, and (3) make recommendations for the future global strategy for researching the parental craniofacial phenotype in orofacial clefting.
Search Strategy
The Cochrane, Medline (via PubMed and OVID platforms [1966 to December 2006]), Embase, CINAHL, and ASKSAM Orthodontic Reference Database (1950–1997) databases were searched using a combination of the following keywords: microform, parent, craniofacial, dental, and cleft. All published articles were reviewed. There were no exclusions of non-English reports. Of the 36 studies identified using this strategy, 26 met the inclusion criteria.
Data Abstraction/Synthesis
The statistically significant data were abstracted using a pro forma, and the methodological quality of the selected studies was evaluated using a checklist. There was considerable heterogeneity among the studies, and therefore it was not possible to synthesize the data. We were, however, able to collate the data.
Results/Conclusions
(1) The craniofacial phenotype possessed by parents of children with orofacial clefting is distinctive when compared with that of the noncleft population. (2) There is insufficient evidence to produce a model of the phenotypic features to assist in the search for orofacial clefting morphogenes. (3) The pattern of expression of the phenotypic features identified to date supports the contention that there are differences in the inheritance of cleft lip with or without cleft palate and isolated cleft palate. Progress in this field is affected by extreme heterogeneity in etiology of cleft lip with or without cleft palate, as well as heterogeneity in study design. (4) Subphenotyping using features such as microforms should be employed to reduce the heterogeneity and to improve the power of future genetic investigations and will also assist in clinical management and genetic counseling for families.
Many investigators over the years have reported that the dentocraniofacial phenotype in cleft lip and/or cleft palate (CL/P) is different from that of noncleft individuals (Bonn, 1963; da Silva Filho et al., 1998; Foster and Lavelle, 1971; Suzuki et al., 1999). The specific phenotypic features include variations in both the craniofacial morphology and the dentition in both the cleft and noncleft regions of the oral cavity. Cleft phenotypes are compounded by disordered muscle insertions, functional disturbances, and the various surgical and nonsurgical manipulations (Liao and Mars, 2006), but they also demonstrate cleft-specific phenotypic features in regions of the craniofacial complex that are remote from the cleft site. In addition, abnormalities of number, size, shape, development, eruption, and enamel of teeth are present more frequently in children affected with cleft lip with or without cleft palate (CL±P) or cleft palate (CP) than in the general population (Kraus et al., 1966; Ranta, 1986), and some of these features may be inherited.
Soft tissue microforms (a minimal manifestation or subclinical sign that is detected in noncleft subjects, indicating a greater propensity to clefting in their offspring [Huston et al., 1985]) also may manifest in either the lip or palate. Bifid uvula (Shapiro et al., 1971), submucous clefts, and notches in the vermilion border (Eppley et al., 2005) are seen more often in families where an overt cleft of the lip and palate has occurred. Subepithelial defects of the orbicularis oris muscle have been described by Martin et al. (2000) and Neiswanger et al. (2007). The latter group reported that in the Pittsburgh orofacial cleft study consisting of 525 cleft family members and 257 controls, the proportion of subepithelial orbicularis oris defects was significantly increased in noncleft relatives compared with controls. This study also observed sex differences in the occurrence of orbicularis oris muscle defects, with an increased predilection in male relatives compared with male controls.
It has been suggested that these skeletal, dental, and soft tissue abnormalities could represent an incomplete manifestation of the clefting process (Ranta, 1986; Tolarová, 1969; Weinberg et al., 2006). Schroeder and Green (1975) evaluated the dentition of cleft probands, normal siblings of their cleft probands, and noncleft controls, and the incidence of dental anomalies per individual was found to be higher in the siblings of cleft probands than in the noncleft controls. The multifactorial threshold model (Fraser, 1970) based on the theory of a genetic susceptibility toward the particular defect, coupled with a threshold determined by an admixture of genetic and environmental factors, remains plausible but does not fit all typical orofacial clefts. The alternative is the etiologic heterogeneity model, where there are relative contributions from both genetic and environmental sources (Blanton et al., 2004). The genetic contribution will be minimal in some cases, heavily weighted to one parent in other cases, and approximately equal in those instances where, by chance, each parent happens to possess the same degree of predisposing factors (Ward et al., 1989). As a result, cleft-predisposing features could be specified by the parental genome in CL/P and therefore demonstrated by the parental dentocraniofacial morphology.
Microforms Proposed for Orofacial Clefting
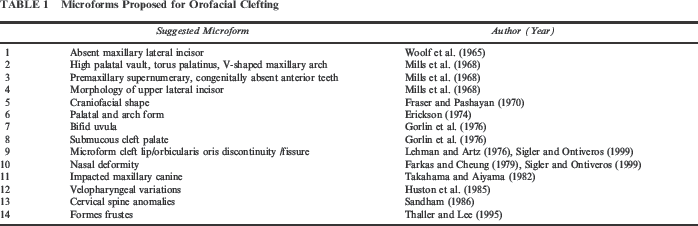
Indeed, microforms result from expression of the orofacial cleft genes, producing an underlying disturbance in several tissues, perhaps as a result of a malfunction of the neural crest cells (Sharma and Kharbanda, 1991). Thus, the orofacial cleft genes produce a variety of subtly different parental phenotypes, some of which may not be closely related anatomically or functionally to the oronasal region.
Identification of the cleft microforms will improve the prediction of recurrence risks (Huston et al., 1985) and will assist in the efforts to identify individual cleft type etiopathogenesis, in particular the genetic contribution to orofacial clefts (Mossey et al., 1998a). Clearly, the identification of microforms of orofacial clefting should be aimed primarily at searching for distinctive phenotypic features that are clearly identifiable in individuals with different types of orofacial cleft and their families.
Study Aims
The aims of this study, therefore, were to (1) identify the published data relating to the parental dentocraniofacial morphology in orofacial clefting, (2) synthesize the data to derive a model of the phenotypic features that will assist in the identification of cleft morphogenes, and (3) make recommendations for the future global strategy for researching the parental craniofacial phenotype in orofacial clefting.
Methods
We conducted a systematic review to identify all possible studies of parental orofacial clefting microforms according to the definition by Huston et al. (1985). However, many studies of the noncleft relatives of children with orofacial clefting have not investigated the craniofacial phenotype as a microform per se. Therefore, this study was designed to identify reports of investigations of the parental craniofacial phenotype as well as investigations of parental orofacial clefting microforms. Institutional review board/research ethics committee approval was not required for this study because no individual subject data were examined.
Search Strategy
The search strategy was formulated to identify any previous systematic reviews and meta-analyses in addition to all the published cohort studies (with appropriate comparison groups), case-control studies, and case reports investigating the parental dentocraniofacial phenotype in CL/P. The Cochrane, Medline (via PubMed and OVID platforms [1966 to December 2006]), Embase, CINAHL, and ASKSAM Orthodontic Reference Database (1950–1997, European Orthodontic Society, London) databases were searched using a combination of the following keywords: parent, craniofacial, cleft, microform, and dentition. A “grey literature” search was carried out using Google (http://www.google.com) to identify potentially forthcoming publications and those that may not have been identified already using the formal search strategy. The Cleft Palate-Craniofacial Journal (formerly The Cleft Palate Journal) was hand searched, and the reference lists and bibliographies of all previous publications were consulted to identify any publications not already identified using the electronic search strategy.
Selection Criteria
Search Results
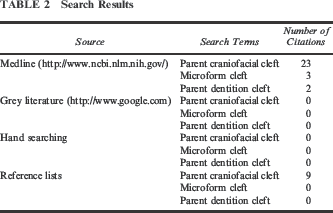
Results of the Search Strategy
Studies of the Craniofacial Phenotype in Parents of Children With Orofacial Clefting
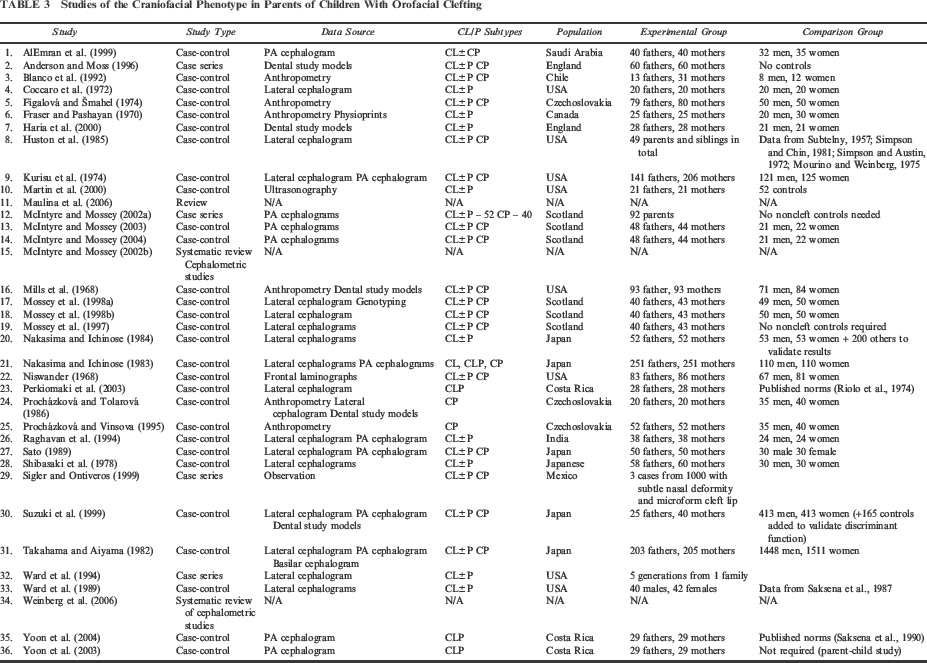
Of the remaining 26 original articles included in this review, five studies derived anthropometric data from direct measurements or photography (Figalová and Šmahel, 1974; Procházková and Tolarová, 1986; Procházková and Vinsova, 1995; Perkiomaki et al., 2003); one investigation used anthropometry, photographs, and physioprints (Fraser and Pashayan, 1970); and four studies used dental study models (Haria et al., 2000; Mills et al., 1968; Procházková and Tolarová, 1986; Suzuki et al., 1999). Niswander (1968) used frontal laminographs to allow the craniofacial complex to be studied in sections; whereas, Martin et al. (2000) used ultrasonography to study the continuity of the orbicularis oris musculature in the parents and siblings of children with clefts.
The majority of the included studies have used cephalometry (AlEmran et al., 1999; Coccaro et al., 1972; Huston et al., 1985; Kurisu et al., 1974; McIntyre and Mossey, 2003, 2004; Mossey et al., 1998a; Mossey et al., 1998b; Nakasima and Ichinose, 1983, 1984; Perkiomaki et al., 2003; Procházková and Tolarová, 1986; Procházková and Vinsova, 1995; Raghavan et al., 1994; Sato, 1989; Shibasaki et al., 1978; Suzuki et al., 1999; Takahama and Aiyama, 1982; Ward et al., 1989; Yoon et al., 2003, 2004).
The details of each of the included studies are summarized in Table 3. All the included study reports were reports of case-comparison group studies and were published in peer-reviewed journals.
Data Abstraction
The statistically significant data were abstracted from individual study reports using a standard pro forma completed for each study report, and the methodological quality of the selected studies was then evaluated using a checklist. The criteria in this checklist were as follows: (1) study of typical (nonsyndromic or isolated) clefts of the lip and/or palate; (2) comparison group or controls from the same population; (3) age and gender profiles of cases and controls reported; (4) error analysis reported for cephalometric or anthropometric studies; and (5) description of the statistical methods used.
Data Synthesis
A meta-analysis could not be carried out using the data from previous studies of the parental dentocraniofacial phenotype in CL/P due to the following factors: variable study methods (i.e., differing inclusion and exclusion criteria, encompassing a range of cleft types [CL, CL±P, CP, familial, sporadic]); differing ethnic and geographic background of experimental subjects; cephalometric data produced using variable image capture techniques; and variable formats of quantitative data output and the use of a variety of statistical tests.
We therefore collated the statistically significant dental study model data, craniofacial anthropometric data, ultrasonographic data, and radiographic data determined using univariate statistical tests, and we collated and tabulated the statistically significant cephalometric data. We also collated the statistically significant data obtained from the reports of studies using multivariate statistical techniques.
Results
Dental Study Models
The results from the investigations using dental study models by Procházková and Tolarová (1986), Suzuki et al. (1999), and Haria et al. (2000) were not consistent. Whereas Procházková and Tolarová (1986) found that parents of children with CP were more likely to have Class II malocclusions (as a result of mandibular retrusion), this was not found in other studies. Procházková and Tolarová (1986) also found the maxillary intercanine width to be statistically significantly greater in the mothers of children with CP compared with their female controls. However, Procházková and Tolarová (1986) did not find any other width measurements that statistically significantly differed between the mothers of CP children and the controls nor were any of the palatal dimensions in the paternal group statistically different from those of the male controls. Conversely, no statistically significant differences were found by Haria et al. (2000) in the incisor relationship, overjet, overbite, and intercanine widths for either the fathers or mothers of cleft children when compared with the fathers and mothers of noncleft children.
Furthermore, whereas Haria et al. (2000) observed that the dentition of parents of subjects with orofacial clefts was “inferior” to that of their control group as judged by the number of teeth that were extensively restored or extracted, the studies by Suzuki et al. (1999) and Haria et al. (2000) both found that the prevalence of abnormalities of tooth number, tooth, and the mesiodistal tooth diameters in parents of children with CL±P did not show any statistically significant differences from those in parents of children without CL±P.
Craniofacial Anthropometric Data
Craniofacial anthropometric data have been derived using direct measurements (Figalová and Šmahel, 1974; Fraser and Pashayan, 1970; Perkiomaki et al., 2003; Procházková and Tolarová, 1986; Procházková and Vinsova, 1995); although, Fraser and Pashayan (1970) also used physioprints (a lateral photograph of the subject, onto which a grid had been projected) in addition to photographs to study the parental craniofacial phenotype in CL/P.
In the landmark study reported by Fraser and Pashayan (1970), the parents of children with CL±P were found to have underdeveloped maxillae, wider bizygomatic diameters, more rectangular or trapezoidal facial shapes, and thinner upper lips compared with the control group. The researchers believed that these deviations were more pronounced in parents who had more than one affected child. Their hypothesis served as a premise for a number of subsequent studies. However, Figalová and Šmahel (1974) found the length and width of the neurocranium, the width of the skull base, and the bigonial width to be statistically significantly smaller in the mothers than in their controls; whereas, the height of the upper face and the intercanthal distance was statistically significantly larger when compared with controls. For their paternal group, the length and width of the neurocranium, the width of the skull base, the width of the face, and the width of the nose were statistically significantly smaller; whereas, the height of the upper face and the length of the nasal base were statistically significantly larger.
Procházková and Vinsova (1995) found parental head width, cephalic index, and facial index to be statistically significantly greater; whereas, head length, biocular distance, and head circumference were statistically significantly smaller in fathers of children with CP. On the other hand, interocular distance, cephalic index, and facial index were statistically significantly greater; whereas, head length, face width, biocular distance, and head circumference were statistically significantly smaller in mothers of children with CP. Both fathers and mothers had increased total face height. It is interesting that Perkiomaki et al. (2003) corroborated the finding of the shortened head length in mothers of daughters with CL±P in their Costa Rican population. Although Procházková and Tolarová (1986) used anthropometric measurements to classify head shape according to cephalic and facial indices, they did not compare their data with those of their comparison group. As a result, the data from this part of the study are not considered here.
Orbicularis Oris Morphology
In their investigation of the morphology of the orbicularis oris musculature, Martin et al. (2000) admixed siblings and index cases with their parental group, and they found that the vast majority of children with overt clefts had at least one parent demonstrating positive ultrasonographic findings of orbicularis oris discontinuity (although the actual numbers were not specified). However, in some cases of overt lip clefts in this study, neither parent possessed any orbicularis oris abnormalities.
Radiographs (Lateral and Posteroanterior Cephalograms and Dental Radiographs)
Of the 22 radiographic studies of the parental dentocraniofacial morphology in CL/P, only that by Niswander (1968) used frontal laminographs to study 10 slices (5 mm apart) of the parental craniofacial complex in CL/P. He found that of the 56 mothers of children with CL/P, four had “positive” radiographic findings of nasal septal abnormalities, asymmetry of the nasal cavity and/or palatal shelves, thinning or discontinuities of the nasal floor, and any other abnormalities or unusual configuration; whereas, of the 54 fathers of subjects with CL/P, six had positive radiographic findings. For the parents of children with CP, positive findings were identified in 10 of the 30 mothers examined and in 1 of the 29 fathers examined. It is intriguing that 9 of the 81 control group mothers and 10 of the 67 control group fathers also demonstrated positive radiographic findings.
Coccaro et al. (1972), Shibasaki et al. (1978), Takahama and Aiyama (1982), Huston et al. (1985), Nakasima and Ichinose (1984), Procházková and Tolarová (1986), Sato (1989), Ward et al. (1989), Raghavan et al. (1994), Procházková and Vinsova (1995), Mossey et al. (1998a), Mossey et al. (1998b), Suzuki et al. (1999), and Perkiomaki et al. (2003) used lateral cephalometry; whereas, AlEmran et al. (1999), McIntyre and Mossey (2003, 2004), and Yoon et al. (2003, 2004) used posteroanterior cephalometry to compare the parental craniofacial dentocraniofacial morphology with that of a comparison group. Kurisu et al. (1974), Sato (1989), Nakasima and Ichinose (1983), Raghavan et al. (1994), and Suzuki et al. (1999) used a combination of lateral and posteroanterior cephalometry to compare the parental dentocraniofacial morphology in orofacial clefting with that of a comparison group; whereas, Takahama and Aiyama (1982) examined lateral, posteroanterior, and basilar cephalograms of their parental group to determine the proportion that had impacted permanent maxillary canine teeth. Table 2 includes details of these studies.
Synthesis of Univariate and Multivariate Statistical Testing Data
Univariate Statistical Testing Data
Results From Lateral Cephalogram Data on Parental Findings *
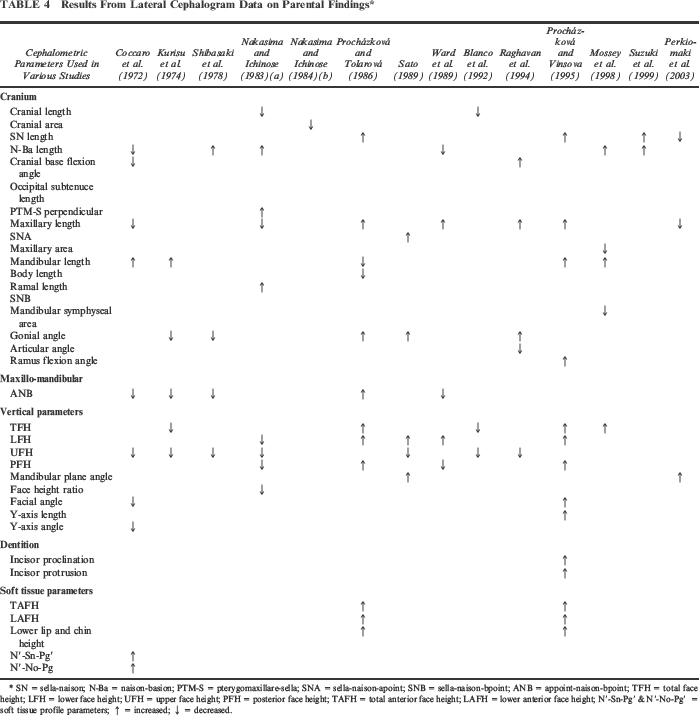
SN = sella-naison; N-Ba = naison-basion; PTM-S = pterygomaxillare-sella; SNA = sella-naison-apoint; SNB = sella-naison-bpoint; ANB = appoint-naison-bpoint; TFH = total face height; LFH = lower face height; UFH = upper face height; PFH = posterior face height; TAFH = total anterior face height; LAFH = lower anterior face height; N′-Sn-Pg′ & N′-No-Pg′ = soft tissue profile parameters; ↑ = increased; ↓ = decreased.
Results From PA Cephalogram Data on Parental Findings *
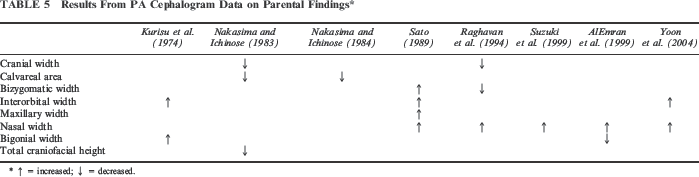
↑ = increased; ↓ = decreased.
Multivariate Statistical Testing Data
Because the geometric, morphometric techniques used by McIntyre and Mossey (2004) evaluate craniofacial shape based on a series of coordinate data, these data are reported along with those data from the reports of studies using “traditional” multivariate statistical tests. We therefore found that four different multivariate techniques had been used to evaluate the parental craniofacial morphology. Due to methodological differences among the various studies, the data from multivariate analyses could not be synthesized.
Cluster Analysis.
Cluster analysis was used by Ward et al. (1989) to identify groups of subjects demonstrating similar cephalometric features in their sample of parents of children with clefts. They identified three major clusters, two demonstrating cephalometric similarities to individuals with clefts and one having similar dimensions to published cephalometric values.
Factor Analysis.
Kurisu et al. (1974) carried out a factor analysis and Q-mode similarity correlation combined with principal component analysis. This procedure determined that the correlations between the groups were higher for mothers of children with CL±P than for fathers of children with CL±P, confirming the greater heterogeneity within the fathers as identified using univariate statistical tests. For the mothers, 92.1% of the variance was accounted for by the first two principal components, as opposed to 86.5% for the fathers.
Discriminant Analysis.
Discriminant function analysis (DFA) has been used to identify the parameters that could be used to classify an individual into the correct experimental group. Nakasima and Ichinose (1983) identified seven ratios that played an important role in the discrimination between parents and controls, all from posteroanterior cephalograms. In their study, the probabilities of misdiscrimination ranged from 13.0% to 17.4%. However, they were unable to distinguish parents of CLP children and parents of CP children according to their craniofacial morphology. Procházková and Vinsova (1995) claimed to use cluster analysis to determine the anthropometric and cephalometric parameters that determine the “at risk” parents, but they only reported discriminant function analyses in their results.
Mahalanobis distance2 analysis measures the degree of deviation of an individual from the mean of the group when multiple variables are evaluated simultaneously and are part of the DFA output. Using this technique, Nakasima and Ichinose (1983) found that the face shape of the parents of children with CLP, CL, or CP and the combined experimental group were highly distinguishable from the control group. Similarly, Mossey et al. (1998b) identified a highly significant difference between the craniofacial morphology of their parental sample and controls; one significantly different parameter between the paternal and control groups was mandibular length (Condylion-Gnathion). The Mahalanobis distance was greater for women than men.
Mossey et al. (1997) investigated the morphometric features that indicate a predisposition to CL/P (among parents of children with CL, CLP, and CP) and found no significant differences between CL and CLP, and only a few parameters differed between CL±P and CP. Their discriminant analysis indicated that for the maternal group, ramus height and cranial height are reliable discriminators for CLP (80%) and CP (75%). Mossey et al. (1998b) compared parents and controls and found that for male parents, the useful discriminators were cranial area, parietal chord length, cranial base length, total anterior facial height, ramus length, and the horizontal distance between condylesella. A jack-knifed classification found that 83.3% of parents and 82.6% of controls were classified correctly. For women, the useful discriminators were cranial area, cranial height, parietal chord length, and parietal and occipital subtenuce measurements. A jack-knifed classification found that 92.7% of parents and 98% of controls were classified correctly.
Suzuki et al. (1999) identified the features that classified parent participants in comparison to the control group as follows: a larger interorbital distance; larger nasal cavity width and larger intercoronoid distance relative to the maximum head width; and shorter mandibular length relative to the anterior cranial base length. This correctly classified the pooled experimental and control subjects in 67.9% of cases and the pooled test group in 61.8%.
Shape Analyses.
McIntyre and Mossey (2004) employed three morphometric techniques to localize the craniofacial skeletal shape differences between the parents of children with CL/P and a comparison group, the parents of children with CLP and CP, and the male and female parents of children with CL/P. The parental craniofacial shape had statistically significant differences from that of the comparison group when researchers used discriminant analysis of the principal components of shape (PCS) and Euclidean distance matrix analysis (EDMA). However, PCS, EDMA, and thin-plate spline analysis (TPS) differed in their localization of the shape differences, explainable by the different mathematical methods used by the individual techniques. It is interesting that the parental craniofacial shapes in CL±P and CP were morphologically similar when tested using PCS and EDMA. However, there was no shape-related sexual dimorphism in parental craniofacial morphology in CL/P when tested using PCS and EDMA. The conclusion was that, as viewed on posteroanterior cephalograms, although the parental craniofacial shape in CL/P differs from that of the noncleft population, the parental craniofacial shape does not differ between CL±P and CP, and there is no sexual dimorphism in the parental craniofacial morphology in CL/P.
The parameters used for measuring different aspects of facial morphology differed among studies, and therefore it was not logical to conduct a meta-analysis of these data. Cranium length was found to be decreased in the parental group by Nakasima and Ichinose (1983). Maxillary length was noted to be decreased in the experimental group by Coccaro et al. (1972), Nakasima and Ichinose (1983), and Perkiomaki et al. (2003); whereas, Procházková and Tolarová (1986), Ward et al. (1989), Raghavan et al. (1994), and Procházková and Vinsova (1995) found maxillary length to be increased in the parental group. Mandibular length was reduced in the parental groups studied by Kurisu et al. (1974) and Shibasaki and Ohtsuka (1978); whereas Procházková and Tolarová (1986), Sato (1989), and Raghavan et al. (1994) found mandibular length to be increased. Similarly, variations have been found in gonial angle. Kurisu et al. (1974) and Shibasaki and Ohtsuka (1978) found the gonial angle to be reduced; whereas, Procházková and Tolarová (1986), Sato (1989), and Raghavan et al. (1994) all found the gonial angle to be increased in their respective parental groups. Total face height has been shown to be decreased by Kurisu et al. (1974), yet increased by Procházková and Tolarová (1986), Procházková and Vinsova (1995), and Mossey et al. (1998a). Variations also have been found in lower face height. Nakasima and Ichinose (1983) found this dimension to be reduced in their parental group; whereas, Procházková and Tolarová (1986), Sato (1989), Ward et al. (1989), and Procházková and Vinsova (1995) all found lower face height to be increased in their parental groups. Upper face height has been noted to be decreased universally across the parental groups in the studies by Coccaro et al. (1972), Kurisu et al. (1974), Shibasaki and Ohtsuka (1978), Nakasima and Ichinose (1983), Sato (1989), and Raghavan et al. (1994). However, variability has been demonstrated in the posterior face height within parental groups: Nakasima and Ichinose (1983) and Ward et al. (1989) found this dimension to be reduced; whereas, Procházková and Tolarová (1986) and Procházková and Vinsova (1995) found it to be increased. Interorbital width has consistently been shown to be increased in the parental groups in the studies by Kurisu et al. (1974), Sato (1989), and Yoon et al. (2003).
Analysis of Synthesized Data
The parental dentocraniofacial morphology in CL/P is distinctive compared with noncleft populations. There is, however, a lack of consistency in the dental and skeletal soft tissue evidence to accurately identify the anatomical regions that distinguish the parents of children with CL/P from the population; although, greater lower facial height, increased interorbital distances, rotated mandibular position, and reduced head length (in mothers) may identify parents at risk of producing children with orofacial clefting. Furthermore, there is insufficient evidence to accurately determine whether the parental craniofacial morphology in CL±P differs from that of CP.
Discussion
In this study we identified that the dentocraniofacial morphology of the parents of children with orofacial clefting is distinctive in comparison to the noncleft population. However, there is insufficient evidence to produce a model of the phenotypic features to assist in the search for orofacial clefting morphogenes. The pattern of expression of the phenotypic features identified to date supports the contention that there are differences in the inheritance of CL±P and isolated CP. Progress in this field is affected by extreme heterogeneity in etiology of CL/P as well as heterogeneity in study design (Gritli-Linde, 2007). Subphenotyping using features such as microforms should be employed to reduce the heterogeneity and improve the power of future genetic investigations and to assist in clinical management and genetic counseling for families.
Strengths and Weaknesses
We used the systematic review method to minimize bias within the identification of relevant studies. We followed the Meta-analysis of Observational Studies in Epidemiology group guidelines (Stroup et al., 2000), which integrated the specifications for reporting of such studies, including background, search strategy, methods, results, discussion, and conclusion. By using wide search criteria including a grey literature search, we aimed to identify all possible sources of craniofacial phenotypic data in advance of abstracting the relevant clinical information. Specifically, we did not exclude non-English studies.
We critically appraised each study report to determine the type of study (mainly case-control studies) and subsequently synthesized the relevant data. Although a meta-analysis of the abstracted data was desirable, there were substantial methodological differences among the included studies. The most significant is the variability in parameters evaluated within different studies. Some of the observed differences, therefore, may be attributed to methodological variations among different studies, and for this reason, producing a unified model of the “characteristic” parental cleft phenotype is not yet possible.
One potential solution to this problem would be to weight the abstracted data prior to synthesizing the data, according to the grade of evidence, but this actually could introduce further bias due to the other methodological, qualitative differences among the various studies (Table 2). We therefore tabulated the data obtained using univariate statistical techniques and collated those data obtained using multivariate statistical techniques.
Discussion of Results
From this systematic review, we found that specific regions of the dentocraniofacial morphology were distinctive in comparison to the noncleft population. These included the dentition, the craniofacial skeleton, and the craniofacial soft tissues. However, not all the studies produced corroborative evidence and indeed, some studies reported conflicting results. The specific phenotypic features exhibited by the parents of children with oral clefts are quite similar to those shown by individuals with oral clefts (as demonstrated by Ward et al., 1989). The repeated finding of excess interorbital width in both affected individuals and noncleft parents of children with CL/P suggests increased facial width as a heritable trait that predisposes one to an oral cleft by reducing the threshold for its occurrence. Hypertelorism (and in some cases other, wider regions of the midface) may indicate a general disturbance in growth, perhaps caused by a major gene operating in the craniofacial development pathway. In this case, altered facial form could be seen as a forme fruste of the full-blown cleft.
The primary defect in some forms of CLP could be an abnormally wide but short cranial base. This would account for the greater facial widths, as well as abnormal midfacial depths (retruded maxilla), in the parent and the affected child and could lower the threshold for expression of the cleft. The mandible also tends to be posteriorly rotated both in CL±P and otherwise normal parents of these individuals. This rotation gives rise to either an increased total facial height or lower facial height and often associated decrease in facial convexity. Mossey et al. (1997) suggested that mandibular abnormalities may reflect functional adaptation to midfacial deficiency. The differences in mandibular growth might interact with embryonic tongue positioning in a susceptible proband and subsequently interfere with lip or palatal closure. However, the fact that increased interorbital width and a posterior rotation of the mandible occur together in otherwise normal parents of children with CL±P argues for a more generalized disturbance in craniofacial growth.
It is interesting that in most studies of parents of children with CP, the differences from the control population are less pronounced and seldom include significant differences in facial width or cranial size. However, variations in mandibular morphology may be more common in some relatives of children with isolated CP. There appears to be a stronger correlation between facial morphology and parental gender in children with CP.
These differences suggest that heritable differences in facial form may be less important in producing a child with CP than some as yet unspecified influence of sex or imprinting coming from the parents. From the results of this study, it can be deduced that there are no CL/P microforms at the dental hard tissue level. Indeed, it is claimed that an anomalous or missing permanent maxillary lateral incisor tooth (Woolf et al., 1965) has no relevance to predisposition to CL/P within a family pedigree.
The parental craniofacial phenotype, therefore, reflects the possible genetic information that may be conferred upon their offspring via the parental genotype irrespective of CL/P. It should be noted that CL/P predisposing facial factors are unlikely to be the sole determinants of the susceptibility to the condition (Ward et al., 1989). Moreover, the CL/P genetic influences may be possessed by one parent, with the other parent contributing relatively little. In other cases, almost equal contributions of predisposing factors may be made by both parents (Mossey et al., 1998a). Ward et al. (1989) found that eight pairs of parents were in the phenotypically normal cluster, suggesting that a different etiology may be responsible for the cleft offspring in these parents when compared with the cases where one parent displays unusual craniofacial findings. Therefore, in the etiopathogenesis of CL/P, the parental genetic contribution may not split equally between the father and mother, and etiologic heterogeneity allows for this. Recent genetic findings confirm the hypothesis that certain single genetic mutations (e.g., in TBX22, PVRL1, MSX1, IRF6, and FGFR1) can produce phenocopies of isolated clefts (Murray and Schutte, 2004; Riley et al., 2007; WHO, 2002).
Previous studies have estimated the heritability of different cephalometric parameters, according to lateral cephalograms, between parents and their normal offspring. Johannsdottir et al. (2005) observed that daughters had more variables that reached the level of significance than did sons. Daughters showed similar heritability to both parents at both age levels, but more variables were highly significant in the daughter-father groups. Sons showed stronger heritability to their mothers at both age levels. The variables showing the greatest heritability were those representing the position of the lower jaw, the anterior and posterior face heights, and the cranial base dimensions. Heritability was notably low for the dental variables. Thus they concluded that genetic aberrations can be detected for complex polygenetic, multifactorial traits.
Genetics of Craniofacial Morphogenesis and of Orofacial Clefts
Aberrant embryonic craniofacial morphology predisposes an embryo to CL/P, with discrepancies between the size of the embryonic facial processes and the craniofacial complex preventing the contact and/or subsequent fusion of the facial processes during the critical physiological period of primary and secondary palatal development. Homeotic genes such as morphoregulatory genes (Slavkin, 2000) are known to specify the “geometry” of orofacial form, and this group of genes could be of crucial significance in the development of CL/P by patterning an aberration in the embryonic craniofacial morphology.
In the field of orofacial clefting research, it has proven difficult to identify the genetic component in the etiology. There are many reasons for this, one of which is that the etiology is polygenic and multifactorial, and epidemiologic and genetic investigations indicate a great deal of heterogeneity. Others are the lack of genotype-phenotype correlation, a problem even in single gene craniofacial abnormalities, and the variation in penetrance and expressivity. In polygenic defects this is further complicated by gene-gene and gene-environment interactions.
Studies that seek to differentiate genetic predisposition on the basis of observable and measurable phenotype also are inevitably complicated by such problems, and one method of reducing the heterogeneity is to subdivide cleft types on the basis of phenotype. Distinctions between CP and CL±P are well documented, but there is also epidemiological evidence to support differences between CL and CLP (Mossey and Little, 2002); although, a twinning study in Norway has revealed that consanguinity and family history appear to be greater risk factors for CL than CLP (Harville et al., 2005). It is therefore logical to split nonsyndromic cleft lip and palate into subgroups such as CL and CLP and also subdivide complete and incomplete clefts both for CL and CLP (Oostrom et al., 1996).
Likewise, CP should be subphenotyped into soft palate, soft and hard palates, and Pierre Robin cases. Also chromosomal and single gene etiologies, if known, should be removed, and in the future, molecular diagnosis and comparative genomic hybridization will assist in the differentiation.
The recent observation that variants of genes involved in syndromic forms of CL/P with a Mendelian mode of inheritance also can produce phenocopies of nonsyndromic CL/P (Murray, 2002) suggests that a strategy of choosing variants of genes involved in Mendelian forms of clefting as candidates for investigations of the etiology of nonsyndromic CL/P may be productive. For example, the identification of MSX1, IRF6, and FGFR1 gene variants in population-based genotyping studies can be used in future studies to improve the homogeneity of subgroups of nonsyndromic clefts.
Because there is such heterogeneity in the etiopathogenesis of CL±P and CP (Gritli-Linde, 2007) and evidence for genetic differences between cleft subgroups, it would be logical to attempt subphenotyping the clefts in each group before searching for genotype-phenotype correlation. Likewise with microform research, it would be logical to seek retrospective associations taking into account parental phenotype such as hypodontia, orbicularis oris morphology, and the range of other recognized craniofacial microforms on the basis of the child's cleft type. There are several plausible CL/P candidate morphogenes such as the bone morphogenetic proteins (BMPs), homeobox genes, and growth factors, but to date, only a few studies have sought to combine genetic and parental craniofacial morphometric data (Mossey et al., 1998a; Neiswanger et al., 2006). Both of these studies demonstrated improved predictability of predisposition to both CP and CLP, and such parental phenotype-genotype studies are required to improve understanding in this field.
Subdivision of data, however, has drawbacks such as the requirement for much larger numbers overall, and in order to overcome this, multicenter collaboration is becoming increasingly necessary. Carrying out subset analyses does not rule out doing lumped analysis between seemingly different phenotypes to search for commonality between different subgroups. Multicenter studies also enable an exploration of consistency of association between CL/P in different ethnic groups and diverse gene pools, which would be an important component in providing proof of causality.
The development of the face and the development of the brain are intimately related, and defects in craniofacial development are most likely associated with defects in brain development. Nopoulos et al. (2001) demonstrated that men with CLP have an increased prevalence of enlarged cavum septi pellucidi, which is directly related to cognitive deficits. Nopoulos et al. (2005) observed that compared with healthy controls, subjects with nonsyndromic clefts of the lip and/or palate showed morphologic abnormalities in the cortical surface anatomy of a brain region known to govern social function, the orbitofrontal cortex. It may well be that neuroanatomical studies in parents of cleft children may provide further microforms for clefting in future studies.
Conclusions and Recommendations
Most studies imply that deviations from normal or control craniofacial morphology may represent extreme limits of normal variability and that genes responsible for the deviation from normal contribute to the manifestations of clefting in offspring. It is feasible, therefore, that craniofacial features could enable the identification of a phenotype that could be used to identify individuals who possess the CL/P genotype.
The reasons for conflicting results from the previous studies investigating the parental craniofacial complex in CL/P include (1) methodological differences between the various studies, (2) ethnic differences in craniofacial morphology, (3) the lumping of all clefts and variation in the ratios of different cleft types in these aggregate data, (4) the failure to account for sexual dimorphism in the craniofacial complex, and (5) the inappropriate use of conventional cephalometric analyses in the assessment of shape. Moreover, etiologic heterogeneity means that cases of CL/P involve one or more major genes, a range of genes in a polygenic model, and gene-environment interactions according to the multifactorial threshold model.
The etiological heterogeneity in both CP and CLP implies there will be different genetic predispositions. Assuming that these same genes may confer some influence on facial shape, there will be a range of facial morphologies in any group of CP or CL±P patients lumped together for analysis. Even in a discordant monozygotic twin study (Chatzistavrou et al., 2004), where there is an assumption that the noncleft twin will have a predisposing genotype, the phenotype was found to be not consistently different when the data were pooled for analysis, suggesting genotypic heterogeneity.
This study has identified that there is enough consistency in the studies investigating the craniofacial morphology of the parents of children with CL/P to conclude the differences do exist, but confounders in the data due to heterogeneity in samples and methods, as well as a failure to subphenotype, have masked these differences. We believe that splitting CP and CLP cases into more homogeneous groups according to both phenotype and genotype is necessary in future studies. Craniofacial, dental, and oral features can be measured, particularly if one knows where to look, which features/phenotype to examine, and which tools to use. To compensate for numbers, intercenter collaborative studies with previously agreed protocols will be necessary to make further progress in this field.
Recommendations for Future Studies
The rationale for persisting with morphometric research is that (1) there is a genetic predisposition to many craniofacial anomalies and specifically to nonsyndromic orofacial clefts, which is the most common of all craniofacial anomalies; and (2) the heritability of craniofacial, dental, and oral features undoubtedly holds a key to our understanding of the concept of genotype-phenotype correlation. One of the fundamental problems surrounding nonsyndromic orofacial clefting research is the accompanying heterogeneity of the phenotype and undoubtedly the genotype as well; yet in research there is a persistence with the categorization of clefts into two subgroups, CL±P and CP. Within each of these subgroups there is a range of different morphologies and etiologies, and therefore, the lumping of these is likely to confound attempts to decipher genetic and environmental causes.
The understanding of the genetics of orofacial clefting is improving steadily, thanks to a number of recent significant breakthroughs. As the genetic etiology gradually emerges, so also will the improvement in understanding of genotype-phenotype correlation. The recent discovery by Marazita (personal communication) that the possession of a mutation in the IRF6 gene results in distinctive whorls in lip print pattern of otherwise unaffected parents is an example of subtle phenotypic expression of a gene defect.
Ongoing research in this field promises to elaborate further on identification of genetic predisposition to exposures/environmental factors with public health implications, including prevention. Such research also will facilitate the understanding of the heterogeneity of nonsyndromic orofacial clefts and the possibility that subtle but measurable phenotypes (microforms) will be characteristic of underlying genetic traits. This has significant implications for diagnosis, clinical management, and genetic counseling for families, as well as for improving the power of genetic studies of nonsyndromic clefts in the research arena.
Future studies, therefore, should seek to subset clefts on the basis of phenotypic and genetic features, to standardize methodology, and to compensate for the splitting of numbers via multicenter collaboration.
Conclusions
The craniofacial phenotype possessed by parents of children with orofacial clefting is distinctive when compared with that of the noncleft population.
There is still insufficient consistency of evidence to produce a model of the specific phenotypic features to assist in the search for orofacial clefting morphogenes.
The pattern of expression of the phenotypic features identified to date supports the contention that there are differences in the inheritance of CL±P and isolated CP. Progress in this field is affected by extreme heterogeneity in the etiology of CL/P as well as heterogeneity in study design.
Subphenotyping in both major cleft groups using features such as microforms should be employed to reduce the heterogeneity and improve the power of future genetic investigations and to assist in clinical management and genetic counseling for families.