Abstract
Objective
A meta-analytic study was conducted to examine the cross-cultural psychosocial impact of cleft lip and/or palate in non-Anglo populations.
Design
A total of 333 citations were initially identified for review using electronic and hand-search strategies. Of the six studies that met inclusion criteria, two were later excluded due to insufficient data. The four remaining studies represented a combined sample size of 2276 adolescents and adults with cleft lip and/or palate from China, Hong Kong, Taiwan, and Norway.
Main outcome Measures
Effect size using Cohen's d and confidence intervals were estimated using data from four studies of empirical, controlled study designs.
Results
The magnitude of effect sizes indicated that men (d = −0.75) with cleft lip and/or palate in non-Anglo cultures are more prone to psychosocial issues than women (d = −0.33). Adults (d = −0.50) are more impacted than adolescents (d = −0.04). Overall, regardless of age, gender, or culture, individuals with cleft lip and/or palate have lower psychosocial development than individuals without cleft lip and/or palate (d = −0.42).
Conclusion
The effects for the cross-cultural comparisons were moderated by the age group and gender of the participants; however, most studies resulted in negative effect sizes. Health care teams for cleft lip and/or palate should recognize the importance of psychological intervention and family support in the treatment of all patients with cleft lip and/or palate throughout the life span.
Because physical attractiveness plays a major role in social interactions, individuals with cleft lip and/or cleft palate (CL/P) may be perceived and treated differently from individuals who have “normal” facial features. Cleft lip (failure of closure of the lip) and cleft palate (failure of closure of the palatal shelves) occur during the first trimester and are two separate anomalies that may occur simultaneously. With an overall incidence of about 1 in 700 live births, the presence of a CL/P may lead to discriminatory and prejudicial practices by nonaffected individuals. Human communication generally requires face-to-face communication in which individuals continually exchange looks, stares, and environmental feedback. This feedback is internalized, thereby affecting the individuals' self-perceptions (Bjornsson and Augustsdottier, 1987). Individuals with CL/P are particularly vulnerable to the perception of others because facial disfigurement cannot be easily disguised and can produce aversive reactions. MacGregor (1974), in his studies of aberrant visual characteristics, describes “facial disfigurement” as the “most devastating of social handicaps” (pp. 55–56). However, results from previous studies investigating the association between cleft lip and palate (CLP) and psychosocial problems stemming from CLP vary depending on the assessment methods used by the researcher (Slifer et al., 2004).
Social and emotional adjustments of an individual with CL/P are viewed as a developmental process that changes with family environment, school success, and the person's ability to cope with the stress of growing up with the condition. At first, parents of a newborn with CL/P experience adjustment difficulties as they move through initial feelings of shock, anger, and ultimately, integration of the child into the family. The child's psychosocial adjustment and growth is affected by factors including personal temperament, reactions to surgeries, and societal and peer interactions (Kapp-Simon and McGuire, 1997).
Psychosocial and cognitive function of individuals with CL/P can be viewed as a complex interaction between genetic and environmental factors. Objective measures of social skills, interaction interchange, and psychological development must include domains of emotional well-being, self-confidence, and self-esteem to properly assess a child's position in his or her environment. Although previous reviews describe the psychological status of individuals with CL/P, some studies point out that research efforts lack the necessary consistency to evaluate psychosocial functioning among people with the condition (Berk et al., 2001; Thompson and Kent, 2001; Lockhart, 2003; Slifer et al., 2004; Chung et al., 2007). Hunt et al. (2005) reviewed 117 full-text publications to identify factors associated with risk of psychosocial problems among individuals with CL/P. Although no conclusions could be confirmed regarding difficulties related to behavioral problems, satisfaction with facial appearance, depression, and anxiety, many individuals with CL/P experience psychosocial adjustment difficulties resulting from their facial appearance (Kelton, 2001).
Population demographics of nations worldwide have changed dramatically since the year 2000. Diversity in culture, language, and ethnicity has become a hallmark of global landscapes, with multicultural sensitivity acting as a driving force for change. Research paradigms for studying patients with CL/P are influenced by a multitude of attitudes and behaviors unfamiliar to investigators. For example, practitioners employed in urban environments may encounter as many as 10 different cultures in a given week. In a large school district in California, more than 50 languages may be spoken (Lynch and Hanson, 1998). Increasing culture heterogeneity and subsequent diversity of practitioners' caseloads mandate social communities to develop skills that facilitate effective cross-cultural interactions with patients and families. By being cognizant of the cultural differences in the CL/P population, personnel will be better equipped to effectively communicate with the patient and to treat the medical and psychosocial effects of CL/P (Lynch and Hanson, 1998).
Cross-Cultural Historical Change
Records of attempts to modify the appearance of individuals with cleft lip have existed since 390 A.D., when an unknown surgeon successfully closed the cleft lip of an 18-year-old patient named Wei Yang-Chi. Wei subsequently became the governor general of six Chinese provinces (Rogers, 1971). In 1904, an English medical correspondent stationed in China reported a high incidence of cleft lip in the country and noted that the Chinese were indifferent toward the facial anomaly.
Reports of negative sociocultural development in individuals with CL/P began to appear in the literature in 1951 when MacGregor reported that individuals with facial abnormalities experienced more social stress and difficulties in their lifetimes (Ramstad et al., 1995a). Studies from Norway, France, the United States, the U.K., and China have similarly concluded that individuals with CL/P are less likely to marry, marry later in life when they do, have fewer children, and are paid significantly less than those with equitable jobs (McWilliams and Paradise, 1973; Bjornsson and Augustsdottier, 1987; Ramstad et al., 1995a; Danino et al., 2005; Chan et al., 2006). People with CL/P in the 21st century are less likely to hold high-profile jobs, rather seeking positions in professional and skilled trade occupations (Danino et al., 2005). In comparing the leadership role of the Chinese general in 390 A.D. to present-day jobs of individuals with CL/P in China, it appears that a metamorphosis has occurred in the postindustrialized society. Preindustrialized China favored physical strength over physical appearance, hence the public placement of an individual with CL/P; centuries later, China employs few people with CL/P in public roles. As exemplified by China, societies and the perceptions of its individuals tend to evolve in tandem (Harper, 1995).
Culture
Despite educational advances in many parts of the world, cultural prejudices remain and many beliefs persist, with a number steeped in superstition and folk beliefs (Cheng, 1990).
In India, the etiology of CL/P has been attributed to solar eclipses during pregnancy, starvation in the village, a previous miscarriage, or prematurity. Indians influenced by the Hindu religion, which teaches the belief of reincarnation, believed that sins from a past life caused the malformation. Therefore, shame was brought upon the family of a child with CL/P, and public presentation of the child was avoided (Weatherly-White et al., 2005).
The Nuer tribe of Central Africa referred to an anomalous child as a “hippopotamus,” and returned the “amphibious creature” to the water from whence it came (Evans-Pritchard, 1956). Other cultures believed CL/P to be the result of a pregnant woman consuming rabbit meat, transgressions of the individual's ancestors, or the father slaughtering chickens or fishing while his wife was pregnant (associating the fish hook and the mutilating of the fish's mouth) (Cheng, 1990; Schreiber-Willcox, 1994; Sailer and Kolb, 1995). Developing countries, including China and the Philippines, reportedly perceive facial disfigurement as a curse and often ostracize the person from the community (Scheper-Hughes, 1990).
Whereas infanticide continues to be a common practice in some cultures (e.g., the Mehinaku Indians of the Brazilian Amazon), other cultures view facial anomalies as a source of pride. In a Brazilian shanty town, individuals with CL/P are seen as survivors, individuals who have “avenged fate” and overcome obstacles (Scheper-Hughes, 1990; Reeve et al., 2004). The Chamorro culture of the Mariana Islands views someone with CL/P as a “gift from God,” an individual who “belongs to everyone and is protected and sheltered” (Cheng, 1990).
Western and Non-Western Societies
Psychosocial issues have been documented across cultures, but few studies have investigated the psychosocial implications of CL/P between Western and non-Western societies. In developed countries, perceptions of individuals with CL/P are influenced by the “Western outlook”—a body-conscious culture emphasizing a perfect, unblemished cosmetic appearance (Scheper-Hughes, 1990; Harper, 1995). In contrast, Chinese culture stresses integrity of interpersonal relationships. Lai (1995) hypothesized that the integral role of interpersonal harmony may lead to more aversive responses to negative social interactions. In researching the social interactions of children with children who have physical disabilities in Nepalese and Filipino populations, Harper collectively noted that children are less likely to engage with children presenting with CL/P than with children who have other physical disabilities (Harper, 1997; Harper and Peterson, 2001). Only in more physically laborious societies, in which physical health is a necessity for survival, are facial anomalies overlooked more than other physical abnormalities (Strauss, 1985; Scheper-Hughes, 1990; Harper, 1995, 1997).
Current research data on CL/P raises some intriguing questions regarding the way in which cultural beliefs have influenced cultural perceptions, as well as how those perceptions affect the psychosocial adjustment of individuals with CL/P.
Psychosocial Factors
Cleft lip and/or cleft palate can have profound effects on the person and their response to others (Clare, 2003), such as impaired social adjustment, lowered self-esteem, and social anxiety. Results of studies focusing on the psychosocial adjustment of individuals with CL/P appear to be contradictory. Noar (1991) correlated significant adjustment issues in individuals with CL/P relative to their appearance and speech. In contrast, Endriga and Kapp-Simon (1999) found that adults with CL/P did not seem prone to psychological disturbances, although frustration with facial appearance led to self-doubt and distress in interpersonal relationships. As noted earlier, individuals with CL/P are less likely to cohabitate and tend to marry later in life (Bjornsson and Augustsdottier, 1987; Ramstad et al., 1995a; Danino et al., 2005; Chan et al., 2006). However, far more disconcerting data surfaced with the study by Herskina et al. (1993), which indicated that the suicide rate among individuals with CL/P was twice that of the general population. Yet a Danish study noted that although there is an increased risk of hospitalized mental disorders among patients with CL/P, the risk for schizophrenia or bipolar illness was not statistically significantly higher compared with the general population (Christensen and Mortensen, 2002). Recent studies have alluded to gender, age, and culture as predictive factors in the psychological adjustment of individuals with CL/P.
Gender
Broder and Strauss (1992) found that men and women with CL/P have equitable levels of acceptance concerning their facial appearance. However, two studies demonstrated that women with CL/P were less accepting of their own physical appearance than were men with CL/P (Berscheid and Gangestad, 1982; Broder and Strauss, 1991). Women have commonly used cosmetics to conceal scars and accentuate their good features; whereas, men have admittedly grown a moustache, beard, or both (Patel and Ross, 2003).
Age
Age has a varying effect on how individuals cope with the effects of CL/P. Children, regardless of the culture, are less likely to interact socially with a peer who has a craniofacial anomaly (Harper and Peterson, 2001; Chan et al., 2006). Such negative social feedback affects the self-esteem of the child who has the anomaly and decreases his or her likelihood of approaching peers in succeeding interactions. The cyclical series of negative interactions experienced by children with CL/P renders them more prone for social failure and psychosocial adjustment tribulations than their peers (Tyl et al., 1990; Harper, 1995; Diaz de Leon, 1997; Pope and Ward, 1997; Patel and Ross, 2003). As adolescents, individuals with CL/P tend to display poor pragmatics; their psychosocial issues are then internalized as adults, and episodes of depression and anxiety become more prevalent (Pillemer and Cook, 1989).
A meta-analysis review can quantitatively summarize the relationship between variables across different studies. Identifying perceptions and psychosocial impacts through a meta-analytic review is particularly important. Research informed by multiple investigations allows health care professionals to approach culturally diverse patients more sensitively and competently, to better communicate with the patients and their families, and to advocate for their needs.
The attitude of the individual with CL/P impacts his or her social and emotional development, as do the attitudes of health care and education specialists toward the etiology, effects, and treatment of the facial anomaly (Patel and Ross, 2003). For this reason, a culturally sensitive review and meta-analysis of the literature on CL/P was completed to examine cross-cultural conclusions on the psychosocial adjustment of individuals with CL/P. A systematic meta-analysis provides quantitative examination of scientific evidence on the cultural implications of CL/P to implement evidence-based practice.
Research Aims and Hypotheses
Although a number of studies have investigated the psychosocial adjustment of CL/P, including a systematic literature review by Hunt et al. (2005), no research has specifically examined the influence of culture across studies. Evidence provided by investigators in India, Nepal, South Africa, the Czech Republic, and China indicates that culture in Western, so-called developed countries bears a different connotation regarding physical impairment than in the so-called developing countries (Tyl et al., 1990; Harper, 1995; Patel and Ross, 2003; Rankin and Borah, 2003; Reeve et al., 2004). The array of perceptions among countries elicits questions regarding the relevancy of cultural specificity of physical disparities across cultures (Harper, 1995). Furthermore, most of the psychosocial studies on CL/P were conducted in the United States and the U.K. Few studies have examined the perspectives of individuals with CL/P from countries with primarily non-Anglo populations. Because present studies may inaccurately portray the psychosocial perceptions of non-Western cultures, a cross-cultural study is integral to determine whether the response to CL/P can be generalized. In several ways, the meta-analysis extends previous qualitative and quantitative analyses of the literature on the culture-psychosocial relationship.
The overall aim was to investigate the scientific evidence linking CL/P with an increased risk of psychosocial problems in non-Anglo cultures. The analyses addressed a number of specific questions:
Do individuals with CL/P differ in overall psychosocial adjustment within and between cultures?
What is the effect of developmental stages (adolescent versus adults) on psychosocial adjustment?
Is there a difference between men and women with CL/P in terms of psychosocial adjustment patterns?
Materials and Methods
Meta-Analytic Approach
The present study used a meta-analytic approach to gain a holistic perspective of current empirical research in CL/P and to critically analyze the results. A meta-analysis is a summary of previous research that uses quantitative methods to compare outcomes across a wide range of studies. Because the results from different studies use different scales to calculate outcome variables, results from one study cannot be easily compared with the results of another without further statistical calculations. A meta-analytic statistic, used to synthesize the data, produces an average effect size across a range of studies. The effect size serves as a common denominator, allowing for the comparison of studies. More specifically, the effect size represents the magnitude of the treatment effect or the difference between two groups. A commonly used effect size in meta-analyses is Cohen's d because it has shown to be a robust measure (Higgins et al., 2003; Nye and Harvey, 2006).
Incorporating meta-analysis into a study shifts the focus from single studies to multiple studies. The different statistical perspective emphasizes the importance of effect size over the statistical significance of individual studies. For the purpose of this meta-analysis examining general psychosocial issues in control group comparison, the psychosocial effects of CL/P encompassed the following: (1) psychological problems (anxiety and depression), (2) general and social self-esteem, and (3) attitudes toward appearance and treatment.
Inclusion Criteria for Studies
Criteria for inclusion in this review included studies with the following elements:
The participants were diagnosed with CL/P.
The study examined the psychosocial adjustment of individuals with CL/P.
Psychosocial qualities were assessed quantitatively through the use of questionnaires.
Administration of questionnaires had to meet the following criteria:
Questionnaire was administered in the native language of the participant. The interviewer was fluent in the native language of the participant.
Studies assessed the perspectives of individuals from non-Anglo cultures.
Exclusion Criteria for Studies
Criteria for exclusion in this review included studies with the following elements:
Studies lacked a control or comparison group.
Studies only surveyed individuals of Anglo descent (e.g., U.K., Ireland, United States, Australia, Canada)
Studies of poor quantitative design (e.g., based on observation and/or unstructured questionnaires/interviews)
Studies dating back further than 20 years (published before 1987).
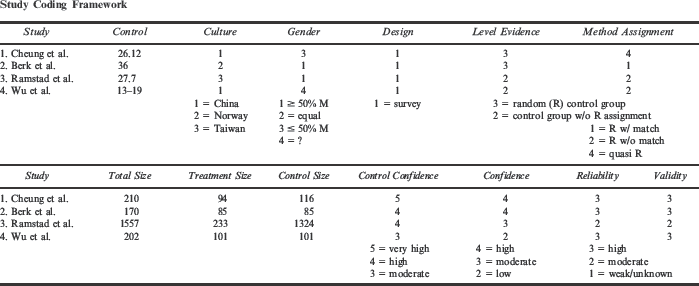
The authors established study date criteria to examine current terminology and research methods; the last 20 years have brought significant changes in diagnostic and therapeutic management of the child with craniofacial anomalies in several professional fields. Some of the examined studies investigated a single psychological or social construct; whereas, others addressed a range of psychological issues (Table 1).
Literature Review List
Information Retrieval
To retrieve as many relevant studies as possible, hand and electronic searches were conducted. Hand searches of bibliographic references were conducted in the following books:
Battle DE. Communication Disorders in Multicultural Population. Boston: Butterworth-Heinemann; 2002.
Lynch EW, Hanson MJ. Developing Cross-Cultural Competence. Baltimore: Brookes Publishing; 1998.
Peterson-Falzone SJ, Hardin-Jones MA, Karnell MP. Cleft Palate Speech. St. Louis: Mosby; 2001.
Wyszynski DF. Cleft Lip and Palate: From Origin to Treatment. New York: Oxford University Press; 2002.
For electronic searches, the following databases were searched: MEDLINE (117 relevant), PsychINFO (90 relevant), PubMed (112 relevant), OhioLink Theses & Dissertations (zero relevant), Networked Digital Library of Theses and Dissertations (two relevant), and Web of Science (five relevant). The bibliographies of relevant studies were perused for further suitable sources. Attempts were made to locate studies written in languages other than English.
During the search, the thesaurus was used to expand and focus keywords. Keywords were combined and narrowed using the Boolean operator “AND.” The following key words were used to locate relevant studies in each database: cleft lip and palate, oral cleft, craniofacial anomalies/condition, facial deformity I disfigurement, congenital deformity/malformation, fetal condition, multicultural, cultural factors, cultural perceptions/sensitivity I diversity, self-concept, social perception, psychosocial, social value, sociocultural, genetic/syndrome, genetic counseling.
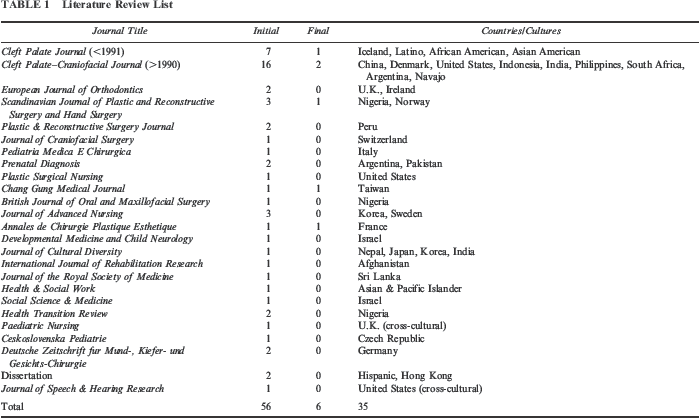
The key words used in the literature search were selected to identify the unique concepts associated with cultural comparisons of psychosocial effects of CL/P yet maintain a broad conceptual framework. A total of 333 abstracts were initially identified through database and other searches. Of these, only 56 appeared relevant. The full text of these papers was analyzed, including five foreign-language papers for which English translations were obtained. One author (M.A.W.) conducted the literature search. A second author (K.H.) was given a random sample of 10 of these abstracts to determine their suitability for inclusion in the review. At this point, there was good agreement (90%) between the two reviewers; the full-text article in which there was disagreement was obtained and jointly reviewed for inclusion. A total of six papers were finally identified as suitable for inclusion in the meta-analysis.
The original 56 studies (Table 1) represented 35 different cultures; the selected six studies represented five different cultures: Chinese (Hong Kong and Shanghai regions), Norwegian, French, Czech, and Taiwanese. The studies were cross-sectional or retrospective in nature and all included a control group. Review of the full texts revealed that 46 were narratives, observational studies, or qualitative studies. Of the remaining 10 studies, six met the inclusion criteria. Three of the studies required further translation (Cantonese, Czech, and French); the latter two were later excluded due to lack of quantitative data. Studies meeting initial inclusion criteria were coded for information regarding the participants, the design, and reliability (see Appendix 1). In the remaining four studies, participants were adolescents or adults with CL/P residing in China, Hong Kong, Taiwan, or Norway.
Publication Bias
Despite the best effort to find all relevant studies on the psychosocial effects of CL/P in non-Anglo populations, some studies may have been overlooked in the process. Two dissertation/thesis search engines were used to identify nonpublished works, and although three were initially identified, they were later excluded due to lack of data or exclusion/inclusion criteria. The aggregate effect size for the selected groups may have been affected by additional, identified control group investigations.
Participant Characteristics
The participants for the study were those who had been diagnosed with CL/P. No age limits were imposed.
Design Characteristics
Randomized controlled trials, longitudinal studies, cross-sectional investigations, and retrospective studies with control groups were considered appropriate for inclusion. All studies had to be of empirical design. The searches were not restricted to English-language journals. Dissertations and unpublished theses were included for review to prevent publication bias.
Results
Four studies representing a combined sample size of 2276 adolescents and adults with CL/P from China, Hong Kong, Taiwan, and Norway were identified to investigate the psychosocial effects of CL/P. The number of experimental subjects included ranged from 51 to 225, with control groups varying in size from 43 to 1323 subjects. One study (Cheung et al., 2007) compared adult and adolescent responses. The three remaining studies examined psychosocial adjustment differences between genders (Ramstad et al., 1995b; Wu et al., 2000; Berk et al., 2001).
Each study was statistically analyzed to determine effect size, standard error, and confidence intervals for each variable. An overall weighted mean effect size for all studies was calculated using a Microsoft Excel spreadsheet. From this calculation, a Q value, critical value, and I2 value were calculated. Based on these values, either a random-model mean effect size or a fixed-model mean effect size was determined. The overall effect size statistic for individual study values was expected to be smaller than group statistics because studies comparing experimental and control groups will typically find a larger difference than studies comparing multiple variables (age and gender).
A confidence interval (CI) was calculated around the effect size to determine how accurate the meta-analysis effect size was as an estimate of the effect size of a broad population. A wide CI indicates a less precise estimate of what would be the effect size of the general population; a narrow CI suggests a more precise measurement. If the CI contains zero within its limits (e.g., −0.6 to 3.4), then the effect size is considered statistically nonsignificant. A CI without zero within its limits (e.g., 0.09 to 4.3) indicates that the effect size is statistically significant. A CI containing only negative values (e.g., −3.7 to −1.2) would indicate that the treatment group was more negatively impacted than the control group (Law et al., 2004).
Meta-Analysis of Included Studies
Prior to meta-analysis, studies were further delineated into two groups, where possible: (1) results that compared the psychosocial effects of CL/P between genders (male versus female) and (2) results that compared psychosocial effects between age groups (adolescents versus adults). At the most global level, the outcomes of each study were summarized using a single Cohen's d effect size. Outcomes for gender, age, and overall psychosocial effects were analyzed within and across studies by comparing effect sizes.
Effect Size
The effect size is a standardized, scale-free measure representing the relative magnitude of an intervention's effect. In the present study, the effect size measured the degree to which CL/P affected an individual's psychosocial adjustment. The greater the effect size, the greater the impact. The significance of effect sizes is measured along a scale, with 0.0 representing no effect. As the effect size shifts toward the positive side of the scale (>0.0), the more beneficial the intervention is interpreted to be. In the present study, a positive effect size would indicate that CL/P has a positive effect on an individual's psychosocial adjustment. In contrast, a negative effect size (<0.0) would be interpreted to mean that CL/P has a negative psychosocial effect on persons with CL/P. The larger the negative number (e.g., −1.0 compared with −0.2), the greater the magnitude of negative impact (Nye and Harvey, 2006).
A commonly used formula for effect size in behavioral science is Cohen's d, which uses the weighted average of the standard deviation of the treatment group (e.g., group with CL/P) and the control group (e.g., group without CL/P) to standardize the mean difference between the two groups, as demonstrated in the following equation (Turner and Bernard, 2006).
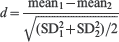
Within studies, a simple average of the multiple effect sizes is appropriate. However to average the effect sizes across the distribution of studies, a weighted mean statistic is used to account for stronger studies. Studies with a large sample size are considered stronger due to the more precise effect size they provide (i.e., lower standard error, thus a smaller confidence interval) (Turner and Bernard, 2006).
Psychosocial Effect
Individuals with CLIP and Individuals Without CLIP
The initial analysis assessed the effects of psychosocial adjustment of individuals with CL/P and unaffected individuals using a Cohen's d effect size. To account for cultural biases, outcomes within studies were calculated comparing the psychosocial adjustment of individuals with CL/P with a control group of citizens from their native country without CL/P. Table 2 shows the overall average effect for the CL/P group compared with the control group in individual studies. Two of the 95% CIs contained zero, thus indicating that a statistically significant treatment effect was not present in these two studies. Table 2 lists the countries in order from most to least negatively impacted by CL/P: China (d = −0.82, SE = 0.15), Norway (d = −0.60, SE = 0.07), Taiwan (d = −0.22, SE = 0.14), and Hong Kong (d = −0.06, SE = 0.11). Taiwan and Hong Kong have nonsignificant effect sizes.
Overall Psychosocial Effect of CL/P by Country †
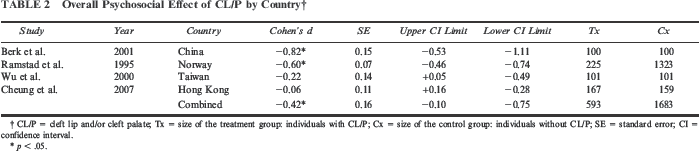
CL/P = cleft lip and/or cleft palate; Tx = size of the treatment group: individuals with CL/P; Cx = size of the control group; individuals without CL/P; SE = standard error; CI = confidence interval.
p < .05.
These effect sizes were aggregated to calculate an effect size and CI for overall psychosocial effect across the distribution of studies. The overall effect of psychosocial adjustment in correlation with CL/P is −0.42, indicating that CL/P has a negative impact on an individual's psychosocial adjustment. The 95% CI for the overall effect size in the population ranged from −0.10 to −0.75. The CI is interpreted to mean that the negative psychosocial effect of CL/P is statistically significant. The effect size and standard error in all aggregate data tables are based on the random effects model; tested measures of heterogeneity require use of the random versus fixed effects model.
Gender Differences
Table 3 demonstrates significant differences in the psychosocial adjustment between genders. The table outlines the three studies analyzed for gender differences (the fourth study, by Cheung, did not investigate gender differences). Regardless of the culture, greater negative effect sizes were notable in the male population. Two of the three confidence intervals were statistically significant for female participants, and all were statistically significant for male participants. The two bottom rows of Table 3 display aggregated effect sizes, statistically signifying that males are more likely to be negatively affected by CL/P (d = −0.75) than females (d = −0.33), with confidence intervals statistically significant for only the male individuals. Although the effect size and strength appear to individually verify differences of psychosocial impact between males and females, the difference in effect size (d = −0.42) between the two gender groups is significant at the 85% CI, not at the 95% CI.
Psychosocial Effect of CL/P by Gender †
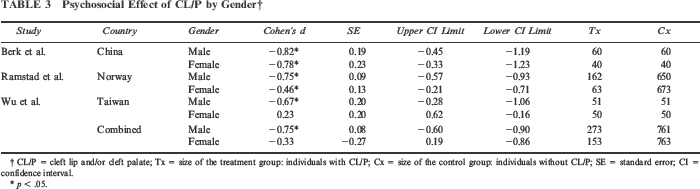
CL/P = cleft lip and/or cleft palate; Tx = size of the treatment group: individuals with CL/P; Cx = size of the control group; individuals without CL/P; SE = standard error; CI = confidence interval.
p < .05.
Age Differences
Regardless of the country, results indicate that adults (d = −0.05, −0.80, −0.60) are more negatively impacted by CL/P than adolescents (d = 0.17, −0.05) (refer to Table 4). Cheung et al. (2007) specifically compared the two age groups. Effect sizes and CIs from Cheung's study indicated that CL/P had a nonsignificant impact on adolescents in Hong Kong yet negatively impacted adults. In contrast, Wu et al. (2000) only investigated the psychosocial effects on adolescents.
Overall Psychosocial Effect of CL/P by Country: Adults and Adolescents †
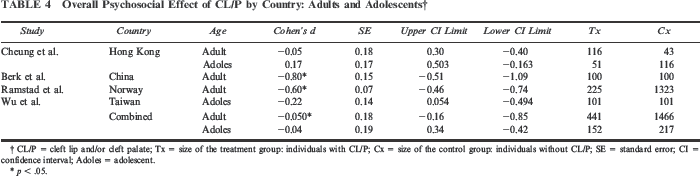
CL/P = cleft lip and/or cleft palate; Tx = size of the treatment group: individuals with CL/P; Cx = size of the control group: individuals without CL/P; SE = standard error; CI = confidence interval; Adoles = adolescent.
p < .05.
The studies completed by Berk et al. (2001) and Ramstad et al. (1995b) did not include adolescent participants; therefore, only the adult outcomes from the Cheung et al. (2007) and Wu et al. (2000) studies are represented in Table 4. Aggregated effect sizes indicated that adults are more negatively impacted (d = −0.50) by CL/P than adolescents (d = −0.04). Confidence intervals are statistically significant for only the adult groups at the 95% interval estimate. Calculations for effect size difference (d = 0.47) between adolescent and adult participants resulted in significant positive effect for adolescents at the 90% confidence level.
Homogeneity in Effect Sizes
Meta-analysis typically sets out to obtain a global index about the effect size magnitude of the studied relations and also to test whether the results are homogeneous. Basically, there can be two sources of variability that contribute to the homogeneity of the effect size distribution among a collection of studies (Higgins et al., 2003). One source is the variability due to sampling error, or within-study variability, which is always present because every individual study uses different samples. The other source of heterogeneity is the between-studies variability, which appears in a meta-analysis when there is a true difference among the population effect sizes calculated by the component studies. In other words, there may be differences due to the influences of undetermined characteristics that vary among the studies other than subject-level sampling errors. As shown in Tables 2 through 4, many studies produced statistically significant results (i.e., the CI does not include zero). Confidence intervals were calculated within each study for overall psychosocial effect and for gender and age differences where applicable. Aggregated effect sizes were calculated across studies to determine significance of overall CL/P psychosocial adjustment, as well as differences among genders, ages, and cultures.
When effect size distributions are found to be heterogeneous, several assessment methods can be applied. The Q statistic assesses whether the effect sizes of the meta-analysis estimated the same effect size in the population. Due to the variability in effect sizes, tests of homogeneity were necessary, which calculated Q and I2 statistics. Table 5 shows that the Q value for the homogeneity test for the effect of psychosocial adjustment in the female, adult, and overall populations was higher than the critical value, indicating that the effect size varied beyond what was expected from sampling error. The Q value for the effect of psychosocial adjustment in the male and adolescent populations was lower than the critical value, indicating that variation in findings was due to chance and results can be generalized to the general population. However, given the small number of studies available for the meta-analysis, the apparent lack of heterogeneity in the male and adolescent groups could have been due to lack of statistical power, as sometimes evident in the Q statistic for studies with small sample sizes (Higgins et al., 2003).
Test of Homogeneity of Effect Sizes
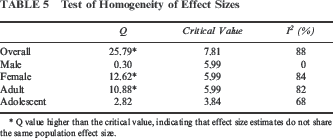
Q value higher than the critical value, indicating that effect size estimates do not share the same population effect size.
Because the Q statistic often exhibits low power in meta-analyses with few component studies, we also examined the more informative I2 statistic. The I2 statistic estimates the amount of variation in effect sizes beyond the sampling error. Unlike Q it does not inherently depend upon the number of studies considered. A common rule of thumb indicates that values of the I2 statistic above 75% are considered high, necessitating the use of a random effects model to calculate weighted overall effect sizes (Higgins et al., 2003). Table 5 demonstrates that the I2 statistic for the male population was low (0%), indicating little variation in the effect size beyond what would have been expected from sampling error. The I2 statistics for the female, adult, adolescent, and overall populations were high (84%, 82%, 68%, and 91%, respectively), indicative of greater variation beyond what would have been expected from sampling error; random effects model calculations were then used to calculate weighted overall effect sizes (Tables 2 through 4).
Discussion
In an effort to identify psychosocial patterns in non-Anglo cultures, a meta-analysis was conducted examining the outcomes of four studies relevant to the topic of psychosocial adjustment in the CL/P population. The present meta-analysis specifically investigated the influence of age, gender, and culture on psychosocial adjustment in individuals with CL/P. The overall effect size estimate (d = −0.42) suggests that an individual's psychosocial well-being is generally affected by having a CL/P. Further analyses tended to support findings that males and adults are more at risk of impaired psychosocial functioning than females and adolescents.
Although the overall effect size for psychological adjustment of adults represented a significant effect, the overall I2 and Q values tested with the adult and female values were high. An unusually large I2 value implies substantial heterogeneity among the studies. Because the studies are representative of diverse countries, significant cultural variation could be expected within gender and age groups. Therefore, it cannot be assumed that all age groups and genders of non-Anglo cultures are negatively impacted by CL/P to the same degree.
Conversely, the overall effect size for psychosocial adjustment for males represented a large effect and maintained a low I2 value. Therefore, this value is statistically significant in favor of the gender differences for males, and sample groups are representative of a homogeneous group of studies. Although social models and intervention methods have increasingly improved children's access to services and education, additional support and attention should be given in the transition from school to work and dependence to independence for young boys with CL/P.
The literature describing psychosocial functioning of CL/P individuals tends to report individual empirical data in a general way without reference to culture, age, and gender issues. Although the compilation of studies to gather a mean effect size did not produce statistically significant results in several analyses, the effects of the individual studies should not be overlooked.
Age
In a study of young adults with CL/P, Heller et al. (1981) reported that 56% of them experienced social life dissatisfaction, with a further 50% indicating that their facial disfigurement had negatively impacted their social life. Results from the present meta-analysis indicated that adults with CL/P have a significantly lower self-reported response to psychosocial adjustment compared with unaffected peers. When comparing adolescents and adults with CL/P across cultures (Taiwan, Norway, Hong Kong, and Shanghai, China), adults are likely to experience a more aversive reaction to CL/P than their younger counterparts.
In their questionnaire-based study, Cheung et al. (2007) compared responses between adolescents and adults and between women and men in Hong Kong. Their research concluded that adolescents tend to have higher self-esteem than adults, reinforcing that strong parental support contributes to stronger psychosocial health. In contrast, Wu et al. (2000), who investigated Taiwanese adolescents, noted that family support does not influence social or life adjustment of adolescents with CL/P. Chinese parents, according to Coy et al. (2002), react to their child's facial disfigurement by being overprotective, their protectiveness thus aiding in the deflection of some of the negative effects of CL/P in adolescent patients. Due to the interpersonal focus of the Chinese culture, a focus that makes one more susceptible to another's feedback, parental encouragement and acceptance serves as an essential component to the healthy psychosocial development of the adolescent (Suh et al., 1998; Suh, 2002). When parental support exists as in the Chinese culture, it appears to alleviate the negative psychosocial effects of a craniofacial anomaly, thus explaining the generally higher self-perceptions of adolescents relative to adults.
Gender
In many non-Western cultures, marital prospects, more so for girls than boys, have reportedly served as significant reason for surgical intervention. In India, it is considered more important to intervene on the behalf of girls with CL/P than boys because a girl's facial anomaly would likely prevent her from finding a husband; she would then remain the responsibility of her family for life (Weatherly-White et al., 2005). In reality, according to present meta-analysis results, men are more negatively impacted by CL/P than women (using an 85% CI), which held true across and within cultures. Ramstad et al. (1995b) reported that men with CL/P do not adjust as well as women and are socially less confident than their female counterparts. The discrepancy between genders may be explained by the more public role expected of men in society; individuals with CL/P are less inclined to take jobs with public exposure, and given that men are generally the head of the household in most cultures, they are often placed in necessarily social positions. In China, Chan (2006) reported that employers consider individuals with CL/P to be less employable, less trustworthy, and less honest, and as evidenced in many cultures, employees with CL/P receive a significantly lower pay rate than their unaffected coworkers, further contributing to their greater negative response (Bjornsson and Augustsdottier, 1987; Ramstad et al., 1995a; Danino et al., 2005; Chan et al., 2006). For this reason, men, due to their familial responsibilities, are prone to receiving more negative feedback than women, thus accounting for their overall lower psychosocial adjustment.
Culture
As evidenced by the meta-analysis values, individuals with CL/P, regardless of their culture, have a higher chance of lower psychosocial adjustment than their unaffected peers. The magnitude of the psychosocial effect can be further analyzed by comparing effect sizes, a lower number indicating a more negative effect. From the present study, individuals with CL/P in Shanghai, China, appeared to be most negatively affected (d = −0.8); whereas, individuals in Hong Kong appeared to be least affected (d = −0.06). The calculations for Norway (–0.6) and Taiwan (–0.2) ranged between those of the other two countries. Before one infers that individuals in Shanghai are less content than their peers in Hong Kong, one should first consider factors affecting the difference. Cheung and colleagues' (2007) study, based in Hong Kong, investigated psychosocial outcomes of adolescents and adults; whereas, Berk et al. (2001), from Shanghai, China, strictly investigated the adult population. As noted earlier, in the societies studied, adolescents tend to have higher self-esteems than adults. Of the four studies included in the meta-analysis, the Hong Kong and Taiwan studies were ranked the highest in psychosocial adjustment with nonsignificant effect sizes, but in actuality, they were the only two studies that included adolescent patients. Similarly, the male to female ratio of subjects in the studies affected the overall psychosocial outcomes. In addition to the lack of adolescent subjects, the lower effect size studies (i.e., China and Norway) also had a greater male to female ratio, further lowering the effect of CL/P conditions. Due to adolescent-adult and male-female ratio differences, comparisons between individual countries and Western/non-Western cultures can be made only with qualifications with current analyses. However, regardless of the country, all corresponding effects sizes were negative, suggesting that overall, CL/P negatively affects psychosocial adjustment across non-Anglo cultures.
In addition, one needs to be mindful of the cultural variability within a country. For example, the United States is a conglomerate of cultures, with citizens of Asian, Latino, and Native American descent following philosophical beliefs ranging from Judaism to atheism. Similarly, Asian/Pacific populations have a kaleidoscope of religious beliefs ranging from Buddhism to Animism. Buddhists view a deformity as the result of karma versus the Animists who believe that a deformity originates from spirits in the body (Cheng, 1990). Animists associate guilt and shame with craniofacial anomalies; whereas, Buddhists have a more indifferent outlook. Although interventions designed to bring functional and cosmetic benefits to individuals with CL/P are “objectively” in the person's best interests and are an integral part of a long-term treatment plan, it is important that the intervention team facilitate decision making without prejudice; exploration of fears and expectations of treatment should be done within the culture of the family context. Due to the variety of beliefs within a country, some variability in behaviors and perspectives are expected within a nation composed of strong religious and ethnographic groups.
Lack of Appropriate Controls
Due to the nature of meta-analysis requirements, a number of studies and cultures were excluded from the present study. Within the field of craniofacial anomalies, a number of qualitative studies have investigated the psychosocial effects of CL/P in countries where surgical intervention is rare and have provided valuable insight into non-Western beliefs. Because these studies were not of controlled designs, they were exempt from the meta-analysis. Therefore, the studies included provided only a sliver of non-Anglo psychosocial attitudes and only included the perceptions of individuals with repaired CL/P. Because the participants had access to adequate health care, their self-perceptions may have differed from individuals in more developing countries like Nigeria (Strauss, 1985). Additionally, because the investigated individuals sought surgical intervention, they may already have a more Western mindset. In contrast, some cultures do not believe in CL/P operations for fear that the spirits in the body may leave during surgery, lacking knowledge of possible functional problems (Lewis et al., 1989). Thus, more empirical data should be sought through randomized control trials to support the claims of qualitative, interview-oriented studies. The goal of synthesis research and meta-analysis is to determine accurately if the null hypothesis can be discarded in favor of the alternative. Statistical errors occur when analyses fail to detect differences in measurements due to poor sensitivity of questionnaires, lack of uniform methodology, and low number of comparable studies.
Future studies should investigate the influence of socioeconomic status on CL/P perceptions. In her dissertation research with Hispanic children with CL/P, Diaz de Leon (1997) reported that the socioeconomic status of an individual's family is a greater predictor of psychosocial adjustment than are cultural factors. Class privilege and position has the potential to dilute discrimination, both economically and socially. Similar to the Chinese adolescent population, parental support and acceptance plays a key role in the psychosocial development of the child with CL/P (Suh et al., 1998; Wu et al., 2000; Suh, 2002). The parent-child relationship should be further investigated in a longitudinal format to determine developmental and cultural responses.
Conclusion
The findings of significant effects indicated that men and adults with CL/P in non-Anglo cultures are more prone to psychosocial issues than women and adolescents. Regardless of age, gender, or culture, individuals with CL/P have lower psychosocial adjustment than individuals without CL/P, as evidenced by negative effect size estimates. The relatively small number of published studies with control groups prevents closer examination of the moderating effects of individual psychosocial distress resulting from specific variables.
In many parts of the world, intervention for CL/P is based on an interdisciplinary team approach comprising multiple health care professionals including, but not limited to, pediatric dentists, plastic surgeons, geneticists, speech-language pathologists, otolaryngologists, orthodontists, and audiologists. Despite the litany of studies citing the psychosocial effects of CL/P, some craniofacial-anomaly teams do not address the importance of psychological intervention. Broder and Richman (1987) noted that of the 195 CL/P teams investigated, only 14% had psychiatry represented, 40% had psychology represented, and 20% of team directors felt that mental health services were not necessary in the intervention of patients with CL/P. Societal hostilities, ridicule, and differential treatment among peers and authority figures undermine the psychological and emotional well-being of people with CL/P. As evidenced by the present study, individuals with CL/P, especially males and adults from lesser-developed countries, experience psychosocial issues. Despite their differences, patients with CL/P are similar in the inevitability of social exclusion in any society. Parental influence and peer relationships continue to be associated with adolescent social and behavioral adjustment (Snyder and Pope, 2009). Hearst (2007) reported positive results in the U.K. with family collaboration and teaching the young child coping skills in public social situations where comments or teasing about appearances occurred. Due to the lack of psychological support in some environments, it is imperative that CL/P teams support and bolster psychological strengths and coping strategies in young persons and their families while remaining particularly mindful of individuals more prone to psychosocial problems and cultural misinterpretations.
Study Coding Framework