
Abstract
Objective
To describe the effect of time after velopharyngoplasty on outcome and to search for preoperative prognostic factors for residual hypernasality in patients with 22q11.2 deletion syndrome.
Design
Retrospective chart review.
Setting
Tertiary hospital.
Patients
Patients with 22q11.2 deletion syndrome and velopharyngeal dysfunction who underwent a primary (modified) Honig velopharyngoplasty between 1989 and 2009.
Main Outcome Measures
Clinically obtained perceptual and instrumental measurements of resonance, nasalance, and understandability before and after velopharyngoplasty.
Results
Data were available for 44 of 54 patients (81% follow-up), with a mean follow-up time of 7.0 years (range, 1.0 to 19.4 years). During follow-up, 24 (55%) patients attained normal resonance and 20 (45%) had residual hypernasality or underwent revision surgery. Mean postoperative nasalance and understandability scores were closer to the norm than mean preoperative scores were (2.0 versus 5.5 standard deviations for the normal passage, 1.3 versus 8.1 standard deviations for the nonnasal passage, and score 2.3 versus 4.1 understandability). Serial measurements revealed that hypernasality only resolved an average of 5 years after surgery, and three patients whose resonance initially normalized later relapsed to hypernasality. Gender, age at surgery, lateral pharyngeal wall adduction, velar elevation, presence of a palatal defect, previous intravelar veloplasty, nasalance, understandability, adenoidectomy, hearing loss, and IQ were not able to predict poor outcome following primary velopharyngoplasty (all p > .05).
Conclusions
In this chart review of patients with 22q11.2 deletion syndrome and velopharyngeal dysfunction, residual hypernasality persisted in many patients after velopharyngoplasty. None of the preoperative factors that were studied had prognostic value for the outcome.
The 22q11.2 deletion syndrome (22q11.2DS) is the most frequent human microdeletion syndrome (Saitta et al., 2004). The frequency is estimated around 1 in 4000 (Devriendt et al., 1998) but may be as high as 1 in 2000 surviving newborns (Shprintzen, 2008). More than 180 clinical features, including every organ system, have been associated with the deletion (Robin and Shprintzen, 2005).
One of the most common clinical features is velopharyngeal dysfunction (VPD), affecting 27% to 92% of children with 22q11.2DS (Kobrynski and Sullivan, 2007). The 22q11.2DS is the most common diagnosis in patients with VPD of unknown cause (Zori et al., 1998). Velopharyngeal dysfunction is the incomplete closure of the velopharyngeal valve that normally separates the oral and nasal cavities, resulting in nasal regurgitation during feeding, frequent otitis media, and hypernasal speech (McDonald-McGinn et al., 1999). In 22q11.2DS, the etiology is related to structural abnormalities such as palatal anomalies in 34% of patients (McDonald-McGinn et al., 1999) but may also be the corollary of cranial nerve dysfunction (Hultman et al., 2000). Surgeons aim to correct VPD by improving the velopharyngeal closure. This can be done by lengthening the palate, mobilizing a pharyngeal flap that spans the center of the gap but retains lateral ports, or rotating lateral flaps to augment the sphincter (Sie and Chen, 2007). In general, the speech outcome after surgery has been reported to be worse in patients with 22q11.2DS than in patients without the syndrome (Sie et al., 1998; D'Antonio et al., 2001a, 2001b; Sie et al., 2001; Losken et al., 2003, 2006; Widdershoven et al., 2008b), but some patients with 22q11.2DS fare as well as those without the deletion after surgery (Argamaso et al., 1994; Meek et al., 2003; Perkins et al., 2005, 2006; Milczuk et al., 2007; Rouillon et al., 2009). Naturally, parents are interested to know whether their child will benefit from surgery. However, prognostic factors remain elusive (Losken et al., 2003).
All postoperative outcome studies to date have mean follow-up periods of less than 5 years. This report includes an analysis of the functional outcome after a follow-up of up to 19 years after primary velopharyngoplasty in patients with 22q11.2DS. To do this, a group of patients previously reported on (Widdershoven et al., 2008b) was augmented with more recent patients. The purpose of this study was to describe the effect of time on functional outcome and search for preoperative prognostic factors for residual perceptual hypernasality or the need for surgical revision following velopharyngoplasty.
Methods
In accordance with the Health Code of 2005 based on the Code of Good Conduct 1995, our institutional review board grants a universal waiver for retrospective chart reviews, such as this study, in which patient data is completely anonymous and not identifiable.
Patients
Postoperative functional outcome was inventoried from the medical records of patients with fluorescence in situ hybridization–confirmed 22q11.2DS who underwent a primary (modified) Honig velopharyngoplasty for VPD between 1989 and 2009 in our tertiary hospital. These surgeries include both palatal lengthening by push-back and raising a superiorly based pharyngeal flap from the posterior pharyngeal wall. The lateral edges of the flap curl under, causing it to become tubular. Whereas the conventional Honig velopharyngoplasty uses full-thickness mucoperiosteal flaps for the oral lining of the defect, the modified technique uses only mucosal flaps (Mink van der Molen et al., 2009). Only patients for whom resonance was measured preoperatively and at least 1 year postoperatively were included because resonance takes at least a year to stabilize after surgery (Conley et al., 1997; Tatum et al., 2002; Arneja et al., 2008; Widdershoven et al., 2008b; Rouillon et al., 2009). The outcome of a subgroup of 25 patients, invited to return for long-term follow-up assessment at the outpatient clinic, was previously reported after a mean follow-up time of 5 years (Widdershoven et al., 2008b).
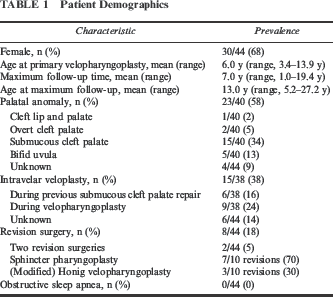
Between 1989 and 2009, a total of 54 patients with 22q11.2DS underwent a primary (modified) Honig velopharyngoplasty at our institution. All patients had intensive speech therapy before and after surgery. Assessments of resonance both preoperatively and at least 1 year after primary velopharyngoplasty were available for 44 of these patients (81% follow-up). One patient was excluded because she did not speak preoperatively, precluding preoperative resonance assessment. Another nine patients were excluded because they only returned for follow-up assessments within 1 year after primary velopharyngoplasty. No reasons were recorded for discontinued follow-up. Patient demographics are listed in Table 1. As indicated by the inclusion criteria, the minimum postoperative follow-up time to speech assessment was 1 year. The maximum follow-up time was 19.4 years after primary velopharyngoplasty, with a mean of 7.0 years. Intravelar veloplasty constitutes the anatomic dissection and repositioning of the velar muscles. On all but one occasion when revision surgery was performed, this was for residual hypernasal speech. The exception was one patient without residual hypernasality whose speech continued to be perceptually bothersome after more than 8 years of speech therapy after primary pharyngeal flap surgery. The first and second revisions were performed an average of 6.2 years (range, 1.5 to 11.0 years) and 8.6 years (range, 5.1 to 12.1 years), respectively, after primary velopharyngoplasty. Based on patient histories, no patients suffered from obstructive sleep apnea postoperatively.
Patient Demographics
Outcome Measures
Resonance was tested during live assessment preoperatively and postoperatively at varying follow-up times by reading or repeating standardized passages. The “normal” passage has a proportion of nasal sounds representative of the Dutch language similar to that of the Rainbow passage. The “nonnasal” passage is similar to the Zoo passage in that it has no nasal sounds (van der Weijer and Slis, 1991).
Perception is the criterion standard of speech assessment (Kuehn and Moller, 2000). Speech pathologists graded hypernasality using the 3-point scale used by the Dutch Association for Cleft and Craniofacial Anomalies (Meijer, 2003; Meijer and Reijman Hinze, 2008). A score of 1 denotes normal resonance on vowels, a score of 2 denotes hypernasality on vowels, and a score of 3 denotes hypernasality on vowels and approximants. Documentation in patient charts, however, was inconsistent, often only stating whether resonance was normal or hypernasal. Therefore, only normal and hypernasal resonance were inventoried for this chart review.
Although the perceptual speech test used by the Dutch Association for Cleft and Craniofacial Anomalies has not officially been tested for validity, some believe there is poor interrater and intrarater reliability for the perceptual assessment of hypernasality. Therefore, the speech pathologists at our center frequently measured nasalance instrumentally with the Nasometer 6200 (Kay Elemetrics, Lincoln Park, NJ) until 1999 and the NasalView (Tiger DRS Electronics, Seattle, WA) from 2000 onward. These measurements were inventoried as secondary outcome measures. Because these machines have different calibrations (van der Weijer and Slis, 1991; Hogen Esch and Dejonckere, 2004), the nasalance percentage scores could not be compared directly. Instead, the standard deviations were calculated for the percentage scores. Values within two standard deviations (SDs) greater than or less than the normal score were considered to be within the normal range (van der Weijer and Slis, 1991; Hogen Esch and Dejonckere, 2004). Occasionally, when perceptual resonance was normal, speech pathologists did not perform instrumental measurements.
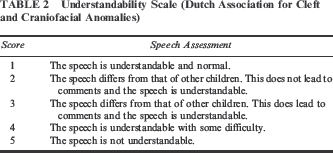
Speech understandability is less directly influenced by surgery because it is a sum of many speech components besides resonance, including articulation and voice quality. It was inventoried for this study due to its social importance (Lipson et al., 1991). Based on live conversational speech, a speech pathologist graded the understandability together with the patients and their parents using the 5-point scale used by the Dutch Association for Cleft and Craniofacial Anomalies (Meijer, 2003; Meijer and Reijman Hinze, 2008) (Table 2). A score of 1 indicated normal speech, and a score of 4 or 5 indicated poor speech understandability.
Understandability Scale (Dutch Association for Cleft and Craniofacial Anomalies)
As aforementioned, resonance takes at least a year to stabilize after surgery (Conley et al., 1997; Tatum et al., 2002; Arneja et al., 2008; Widdershoven et al., 2008b; Rouillon et al., 2009). Lipson et al. (1991) found improvement occurred up to 4 years after surgery. To examine whether speech continues to change, serial assessments in patients with multiple assessments were compared. Given this was a retrospective study, patients had not been invited for measurements at regular intervals. Limited data precluded statistical analysis; descriptive analyses are presented.
Poor outcome after primary pharyngeal flap surgery was defined as residual perceptual hypernasality or the need for surgical revision. Based on studies including both syndromic and nonsyndromic patients with VPD, the following potential preoperative prognostic factors for poor postoperative outcome were analyzed in the 22q11.2DS population: male gender (Kasten et al., 1997), age >7 years at surgery (Riski, 1979), poor or moderate lateral pharyngeal wall adduction (Argamaso et al., 1980; Schmelzeisen et al., 1992; Armour et al., 2005; Lam et al., 2007), poor or moderate velar elevation, presence of a palatal defect (de Buys Roessingh et al., 2006), previous intravelar veloplasty, adenoidectomy, hearing loss of at least 40 dB in both ears, IQ <70 (Moll et al., 1963), poor understandability, and high nasalance scores (Losken et al., 2006). Lateral pharyngeal wall adduction and velar elevation had been assessed during nasal endoscopy with a Pentax 2.3-mm flexible endoscope (FNL7RP3, Tokyo). Motion had been categorized as either poor, moderate, or good. IQ was measured using the age-appropriate WPPSI-R (Weschsler Preschool and Primary Scale of Intelligence Revised), SON-R (Snijders-Oomen Nonverbal Intelligence Test), or WISC-III (Wechsler Intelligence Scale for Children) scales.
Statistical Analysis
An independent t test was used to compare the mean follow-up time until resolution of hypernasality, mean age at primary velopharyngoplasty, mean preoperative nasalance, and mean preoperative understandability between the group that attained normal resonance and the group that had residual hypernasality or underwent revision surgery. A two-tailed Spearman correlation was used to quantify the correlations between resonance and nasalance and between resonance and understandability. The values of the potential prognostic factors for predicting poor outcome were tested using the Fisher exact test. Only complete data pairs were used.
Results
Preoperative and Postoperative Speech Assessments
Hypernasal resonance is the indication for velopharyngoplasty. After primary velopharyngoplasty, 24 (55%) patients attained normal resonance, and 20 (45%) had residual hypernasality or underwent revision surgery (Fig. 1). The follow-up time to either outcome did not differ significantly between the groups (5.2 years [range, 1.1 to 17.4 years] versus 4.9 years [range, 1.0 to 15.5 years]; p = .80), nor did the age at primary velopharyngoplasty (5.9 years [range, 3.4 to 10.0 years] versus 6.0 years [range, 3.4 to 13.9 years]; p = .88). Normal resonance was not limited to those who had been followed for at least 5 years. Three of the patients who attained normal resonance relapsed to hypernasality an average of 2.0 years after achieving normal resonance. Of the eight who underwent revision surgery, two went on to attain normal resonance. At maximum follow-up, 21 (48%) had residual hypernasality, including six who remained hypernasal after revision surgery.
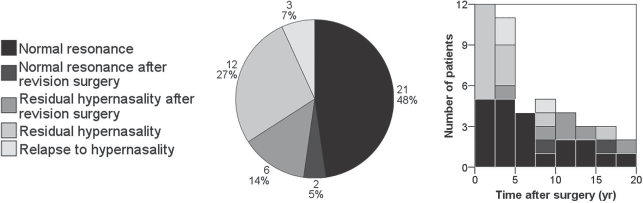
Resonance at maximum follow-up, including the total number of patients with each outcome and stratification by follow-up time.
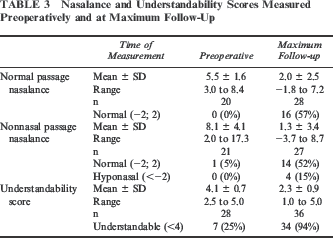
Given the retrospective nature of this cohort study, although resonance assessments were available for all patients based on the inclusion criteria, nasalance and understandability scores were not. The mean nasalance and understandability scores at maximum follow-up showed an improvement relative to the mean preoperative scores (Table 3). Resonance was more highly correlated to the nasalance scores (.67 for the normal passage and .71 for the nonnasal passage) than to understandability (.48) (Fig. 2).
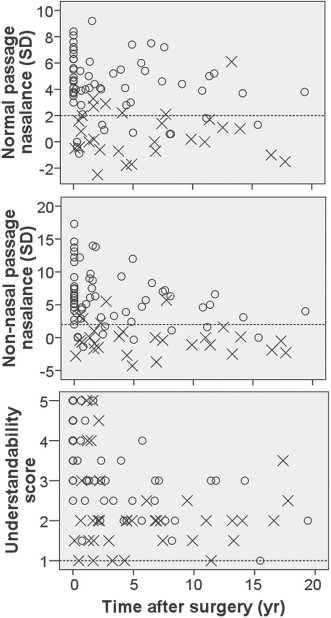
Nasalance, understandability, and resonance measured preoperatively (time after surgery = 0) and at varying times after velopharyngoplasty. Dashed lines indicate upper limits of normal nasalance and understandability scores. × = normal resonance; ○ = hypernasal.
Nasalance and Understandability Scores Measured Preoperatively and at Maximum Follow-Up
Prognostic Factors
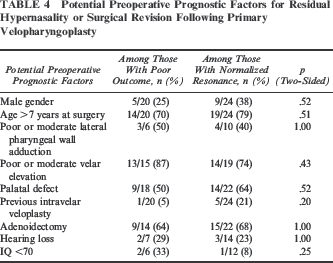
Again, because this was a retrospective study, not all of the potential preoperative prognostic factors had been measured or recorded for all patients. None of the factors tested were prognostic for poor outcome following primary velopharyngoplasty (Table 4). The group of patients with poor outcomes did not differ from the group that attained normal resonance regarding the preoperative nasalance while reading or repeating the normal passage (5.9 versus 5.0 SD; p = .24) or the nonnasal passage (9.1 versus 6.9 SD; p = .23) or in understandability (4.0 versus 4.1; p = .55).
Potential Preoperative Prognostic Factors for Residua] Hypernasality or Surgical Revision Following Primary Velopharyngoplasty
Discussion
Speech generation and perception are complex, involving cognition, language, and voice. Understanding and managing speech problems in patients with 22q11.2DS is especially challenging due to the gamut of clinical findings associated with the syndrome and the heterogeneous presentation among patients (Widdershoven et al., 2008a). Anatomically, palatal defects, adenoid hypoplasia (Havkin et al., 2000), and platybasia (Ricchetti et al., 2004) enlarge the pharyngeal gap, and medially placed internal carotid arteries call for extra caution during surgery (Mehendale and Sommerlad, 2004). Comorbidities such as cardiac anomalies and immune deficiencies may delay or preclude surgery. Additionally, muscle hypotonia (Gerdes et al., 1999; Kitsiou-Tzeli et al., 2004; Oskarsdottir et al., 2005), asymmetric palatal elevation (Solot et al., 2000; Tatum et al., 2002; Chegar et al., 2006; Cheng et al., 2006), hearing disorders (Solot et al., 2000), schizophrenia (Debbane et al., 2009), and learning disabilities (Gerdes et al., 2001; Kobrynski and Sullivan, 2007; Van Aken et al., 2007) may hamper speech therapy.
The Effect of Time on Functional Outcome
Rouillon et al. (2009) showed that postoperative speech in patients with 22q11.2DS was inferior to that of patients without 22q11.2DS at 9 months but was equal at 24 months. The authors postulated that this delayed improvement could be attributed to psychomotor retardation or acquisition difficulties that are common in 22q11.2DS (Gerdes et al., 2001; Kobrynski and Sullivan, 2007; Van Aken et al., 2007). As was described by Widdershoven et al. (2008b), our experience confirms that the adjustment to the new anatomic situation after surgery is markedly slower in patients with 22q11.2DS than in patients without 22q11.2DS. Witt et al. (1999b) found that perceptual speech scores at ages 6 and 12 years after cleft palate repair are stable in children without 22q11.2DS. Following pharyngeal flap surgery in children without 22q11.2DS, Riski (1979) reported that the percentage of patients with acceptable resonance remained consistent 2 and 5 years after, and Cable et al. (2004) found that overall resonance continued to be adequate up to 14 years after pharyngeal flap surgery. Given the complex nature of the speech problems in 22q11.2DS, we were curious whether postoperative speech outcome changes over time in this population. All postoperative outcome studies in patients with 22q11.2DS to date have mean follow-up periods of less than 5 years. In this report, we present the functional outcome up to 19 years after primary pharyngeal flap velopharyngoplasty.
Previous studies only note that resonance takes at least a year to stabilize after surgery (Conley et al., 1997; Tatum et al., 2002; Widdershoven et al., 2008b). In this study we showed that speech continues to evolve as patients age. In patients whose resonance normalized, this only occurred an average of 5 years after primary velopharyngoplasty. Perhaps the patients with residual hypernasality who were followed for fewer than 5 years will eventually attain normal resonance and therefore have been erroneously categorized as having a poor outcome. Once normal resonance was attained, some patients relapsed to hypernasal speech. These continuing changes in resonance make conclusions about postoperative outcome questionable.
The upper limits of the ranges of follow-up times until normalization of resonance may illustrate the marked phenotypic heterogeneity in 22q11.2DS, or they could be artifacts of this retrospective study in which patients had not been assessed at regular intervals after surgery. For example, the patient who attained normal resonance 17.4 years after primary velopharyngoplasty had been dismissed from clinical follow-up 5.7 years after surgery, at which point his resonance was still hypernasal. When he was invited to return for reassessment, his resonance was normal. It is unclear when his resonance normalized. Patients with poorer speech return more frequently for follow-up consultations and measurements, introducing a selection bias. A prospective study where all patients are measured at regular intervals would avoid selection bias and would ensure sufficient data pairs for statistical analysis.
Outcome Measures
Whereas perceptual speech is the criterion standard for assessing the success of a velopharyngoplasty (Kuehn and Moller, 2000), there is no standardized reporting system. Henningsson et al. (2008) have suggested a system that includes the parameters hypernasality, hyponasality, audible nasal air emission and/or nasal turbulence, voice disorder, consonant production errors, understandability, and acceptance. They suggested continued usage of local measures with mapping to a universal scale to allow comparison of outcomes between centers. The speech test developed and used by the Dutch Association for Cleft and Craniofacial Anomalies measures all parameters except voice disorder but has not officially been tested for validity or reliability. The speech test uses a 3-point scale to rate resonance, differentiating between hypernasality on vowels or consonants. However, due to inconsistent reporting in the charts, in this study resonance was recorded as either normal or hypernasal. Dichotomous scales generally yield higher agreement and reliability, but this made it impossible to grade improvements in resonance other than complete normalization, underestimating the effect of velopharyngoplasty in partially correcting hypernasal resonance.
Along with perceptual speech rated by a speech pathologist, various surrogate outcome measures are used to assess speech and the success of a velopharyngoplasty. For example, revision rates are easy to measure. However, they are not always indicative of success (Losken et al., 2006): Sometimes the surgeon gauges that further surgery will not be beneficial, and sometimes patients are satisfied with improved speech and therefore do not opt for further surgery to optimize speech. Patient satisfaction, another outcome measure, is more subjective than perceptual speech assessed by a speech pathologist. Some find that hyponasality causes less social stigmatization than hypernasality (Witt et al., 1999a). Nasendoscopic velopharyngeal closure is difficult to assess objectively (Pigott, 2002; Paal et al., 2005; Sie et al., 2008). Objective measures such as nasalance measured with the Nasometer (Kay Elemetrics) or NasalView (Tiger DRS Electronics) are often reported; however, the correlation with perceptual resonance varies from .31 to .74, limiting its use to measuring the degree of hypernasality once hypernasality has been diagnosed perceptually (Keuning et al., 2002; Sweeney and Sell, 2008) (Fig. 2).
Understandability, which is perhaps the most important outcome measure for social interaction, is only partially affected by resonance, as is illustrated by the poor correlation (.48; Fig. 2). Normalized resonance may not lead to improved understandability if articulation does not improve (Meek et al., 2003). Compensatory articulation is common among patients with 22q11.2DS.
Prognostic Factors
Nearly half of our patients had residual hypernasality following velopharyngoplasty. Given the costs and potential complications associated with this procedure, can we identify this subset before subjecting them to surgery? As suggested by Witt et al. (1995a), suboptimal postoperative functional outcome may represent errors in patient selection rather than errors in operative technique. At our center, all children with 22q11.2DS and residual speech problems following intensive speech therapy undergo velopharyngoplasty. Preoperative prognostic factors have been sought to determine whether it can be predicted which patients are less likely to benefit from surgery. Studies in the larger VPD population including those with 22q11.2DS and nonsyndromic cleft palate present conflicting results regarding the predictive value of the preoperative factors we tested.
Like Losken et al. (2006), who are the only previous group to have reported on prognostic factors for postoperative outcome in patients with 22q11.2DS, we did not find gender to be a predictive factor. In the larger VPD population including nonsyndromic patients, Kasten et al. (1997) found that males had worse postoperative speech scores than females. Sie et al. (2001) found that females had worse scores; whereas, four larger studies showed that gender was not a predictor for outcome (Riski et al., 1992; Losken et al., 2003; Perkins et al., 2005; Pryor et al., 2006).
One may postulate that those undergoing surgery at an older age may be disadvantaged because compensations are more ingrained and their brains have less plasticity to relearn speaking techniques. However, neither we nor Losken et al. (2006) found age to be an outcome predictor. In the larger VPD population including nonsyndromic patients, some studies found that an older age at surgery led to worse postoperative results (Moll et al., 1963; Riski et al., 1992; Schmelzeisen et al., 1992; Peat et al., 1994; Meek et al., 2003); whereas, others found that older patients did not have a poorer outcome (Albery et al., 1982; Van Demark and Hardin, 1985; Seyfer et al., 1988; Sie et al., 1998; Sie et al., 2001; Losken et al., 2003; Becker et al., 2004; Armour et al., 2005; Perkins et al., 2005; Pryor et al., 2006) but in fact had a better outcome (Kasten et al., 1997). It is impossible to draw a general conclusion because these studies used different methods: Some studies compared the mean ages of patients with successful outcome to those without; whereas, others, like ours, tested the success rate above and below a cutoff age.
The murine model for 22q11.2DS has hypoplastic branchiomeric muscles (Kelly et al., 2004; Xu et al., 2005) and aberrant cranial nerves (Vitelli et al., 2002). The clinically hypodynamic pharynx in patients with 22q11.2DS (Witt et al., 1999a; Milczuk et al., 2007; Rouillon et al., 2009) echoes a neuromuscular component in the etiology of VPD. We expected to find that patients without good lateral pharyngeal wall adduction would be less likely to attain normal resonance following a (modified) Honig velopharyngoplasty, but we failed to find a significant relationship. This may be explained by the presence of a pharyngeal flap changing the postoperative lateral pharyngeal wall adduction (Karling et al., 1999). In the larger VPD population including nonsyndromic patients, Sie et al. (1998) did not find worse postoperative outcomes among patients with less lateral wall movement, but larger studies did (Argamaso et al., 1980; Schmelzeisen et al., 1992; Armour et al., 2005; Lam et al., 2007). Likewise, in our study, patients with poor or moderate velar elevation were not more likely to remain hypernasal than their counterparts with good velar elevation. Witt et al. (1995a) also did not find a correlation between velar activity and postoperative speech outcome in a VPD population including nonsyndromic patients.
We did not find preoperative nasalance or understandability to be predictive for residual hypernasality after surgery. In the larger VPD population including nonsyndromic patients, preoperative speech scores have been predictive for postoperative speech scores (Riski et al., 1992; Schmelzeisen et al., 1992; Losken et al., 2003). In patients with 22q11.2DS, Losken et al. (2006) found that lower preoperative nasalance scores correlated with a decreased need for surgical revision.
In our study population, patients with a palatal defect were not more likely to remain hypernasal. Likewise, those who underwent intravelar veloplasty prior to pharyngeal flap surgery did not fare worse than those who did not. This may affirm the adequacy of the (modified) Honig velopharyngoplasty technique for correcting anatomical aberrations. In the larger VPD population including nonsyndromic patients, only de Buys Roessingh et al. (2006) found that patients with palatal defects who underwent velopharyngoplasty had worse postoperative speech outcomes; all other studies found no predictive value (Seyfer et al., 1988; Riski et al., 1992; Schmelzeisen et al., 1992; Sie et al., 2001; Perkins et al., 2005; Pryor et al., 2006).
Although adenoidectomy predisposes an individual to VPD (Conley et al., 1997; Ford et al., 2000; Saunders et al., 2004), in our study prior adenoidectomy was not predictive for outcome. Likewise, Witt et al. (1995b) found no overt correlation between removal of lymphoid tissue and outcome in the larger VPD population including nonsyndromic patients. Given that the adenoids are often hypoplastic in 22q11.2DS (Williams et al., 1987; Havkin et al., 2000; Mehendale et al., 2004), there may not be a real difference between the groups who did and did not undergo adenoidectomy.
Hearing loss in 22q11.2DS can be sensorineuronal (Reyes et al., 1999) or conductive following recurrent otitis media (Solot et al., 2000). As postulated by Willging (1999), hearing loss hampers VPD resolution because it reduces the patient's ability to self-correct the problem. Albery et al. (1982) did not find hearing to be prognostic in the larger VPD population including nonsyndromic patients, and we did not find a correlation between preoperative hearing loss and postoperative resolution of hypernasal resonance in patients with 22q11.2DS.
Those with a higher IQ may more readily learn to use the new anatomical situation after surgery for understandable speech. In the larger VPD population including nonsyndromic patients, Moll et al. (1963) found that IQ is prognostic for postoperative speech outcome; whereas, Albery et al. (1982) did not find intelligence to be prognostic. We did not find IQ to be prognostic in our 22q11.2DS population. All our patients had speech therapy before and after surgery; however, the amount was not documented in the charts and therefore was unavailable for testing as a prognostic factor. Speech therapy is essential in learning to speak understandably (Wang et al., 2009).
Major weaknesses of this study include that speech had not been evaluated by speech therapists who were blinded to the study, that previous live assessments by speech therapists preclude controlling the data, and that much data are missing. Admittedly, being able to review recordings and having more complete data would be preferred, but these ideals are impossible to realize in a retrospective study. Yet, a retrospective design was necessary to yield the largest number of patients.
Although our center is a referral center, and we inventoried data from the past 20 years, we did not have a large enough population to definitively refute the null hypothesis. Performing a sample-size calculation with our ratio of patients with poor outcome to those who attained normal resonance (1:1) to find a prognostic factor that is deemed clinically significant when 70% of the patients with poor outcome have the factor but only 40% of patients with normalized resonance do, using an alpha of .05, a power of 0.8, and a continuity correction yields a necessary sample size of 96 patients (48 per group). With those assumptions, even with complete data for all the 22q11.2DS patients treated at our center in the past 20 years, we would not have enough patients. A multicenter cohort study, therefore, will be necessary to get sufficient numbers to find prognostic factors for postoperative resonance in 22q11.2DS and inform parents whether their child is expected to benefit from surgery.
Conclusion
This chart review shows that residual hypernasality persisted after primary velopharyngoplasty in many patients with 22q11.2DS and VPD. Resonance continued to change years after surgery, making conclusions about postoperative outcome questionable. No preoperative prognostic factors were found for residual hypernasality and/or undergoing revision surgery. A prospective study or a meta-analysis of current data from multiple centers is needed to elucidate prognostic factors.
Footnotes
Acknowledgment
The authors would like to thank Ellen Tromp for giving expert advice regarding statistical calculations.